Original Article 5, Issue 8.1
Comparing Anterior Protrusive With Sibilant Phoneme Mandibular Positioning Techniques for Dental Sleep Appliances in Managing Obstructive Sleep Apnea: A Retrospective Study
http://dx.doi.org/10.15331/jdsm.7178Enoch T. Ng, DDS1; Pedro Mayoral DDS, MSc, PhD2; Ivonne A. Hernandez, DDS, MSc3; Manuel O. Lagravère, DDS, MSc, PhD3
1Graduate Student, School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada; 2University Católica de Murcia UCAM, Faculty of Medicine and Dentistry, School of Dentistry , Madrid, Spain;3School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada
ABSTRACT
Study Objectives:
The objective of this study is to compare the differences in mandibular protrusion between anterior protrusive and sibilant phoneme mandibular positioning techniques for dental sleep appliance therapy.
Methods:
Three clinics in the United States and one clinic in Spain provided retrospective data from dental records on patients treated with either the anterior protrusive or sibilant phoneme technique for dental sleep appliances. Only patients with an apnea-hypopnea index (AHI) reduction to fewer than 10 events per hour and greater than 50% were included. Patient data from those treated with the sibilant phoneme technique were assigned to one group, whereas patient data from those treated with the anterior protrusive technique were assigned to another group.
Results:
The two groups were statistically different in pretreatment (Pre-Tx) AHI. Because of the number of patients with severe obstructive sleep apnea (OSA) in the anterior protrusive group, subgroup analysis was used to compare only those patients with mild and moderate OSA. The sample size met the minimum requirements by power calculation. Patients treated with the sibilant phoneme technique had less mandibular protrusion from habitual position compared to those treated with the anterior protrusive technique.
Conclusions:
The study results suggest that the use of a sibilant phoneme technique is an alternative to an anterior protrusive technique for determining mandibular position due to decreased protrusion necessary to reach the same reduction in the AHI of patients with OSA.
Keywords:
anterior protrusive; dental appliance; obstructive sleep apnea; sibilant phoneme
Citation:
Ng ET, Mayoral P, Hernandez IA, Lagravère MO. Comparing anterior protrusive with sibilant phoneme mandibular positioning techniques for dental sleep appliances in managing obstructive sleep apnea: A retrospective study. J Dent Sleep Med. 2021;8(1)
INTRODUCTION
Obstructive sleep apnea (OSA) is a medical condition characterized by the repetitive loss of upper airway patency via collapse of the pharyngeal segment while maintaining thoracic respiratory effort.1 Although multifactorial, an essential component of this collapsibility revolves around anatomic impairment. Components involved in this impairment include the tongue, soft palate, pharyngeal walls, airway length and shape, craniofacial morphology, and hyoid bone position.2 Other factors involved in airway collapse include ineffective upper airway dilator muscles, unstable ventilator control, and low respiratory arousal threshold.3 For this reason the American Academy of Sleep Medicine (AASM) advocates for several different treatment options including weight loss, positive airway pressure, pharmacotherapy, dental sleep appliances, and surgical intervention.4
Although sleep physicians make diagnoses and direct treatment for OSA, dentists play a vital role due to expertise in the fabrication and treatment protocols related to dental sleep appliances.5,6 These appliances work by advancing the mandible and tongue anteriorly and widening the velopharynx along the lateral walls, thereby working on the pharyngeal anatomic components in OSA.7-13 However, there are a number of generally accepted adverse effects associated with the use of dental sleep appliances and mandibular protrusion. These include dental occlusal changes, temporomandibular joint (TMJ) dysfunction, and craniofacial changes.5,14-18 The risk and magnitude of these side effects usually increase with increased apnea-hypopnea index (AHI) and increased mandibular protrusion, with protrusion beyond 50% of maximum generally correlating with significantly greater risks of side effects.13,16-21 As well, craniofacial and occlusal changes continue over time with no defined endpoint independent of the type of dental sleep appliance used.22
Normal mandibular protrusion is, on average, between 9.86 to 13.09 mm with overjet being the primary method of measurement.23,24 This would imply that protruding the mandible greater than 4.93 to 6.55 mm would greatly increase the risk of side effects occurring with any dental sleep appliance. For dental sleep appliances, mandibular protrusion is generally accepted to start at 50% to 70% of maximum protrusion, where the higher the AHI value of the patient, the greater the mandibular advancement/protrusion generally necessary for treatment.17,18,25-27 However, recent research indicates that minimal protrusion may be sufficient for treatment of OSA by dental sleep appliances.7,27-29
Phonetics and the sibilant phoneme have been used in prosthodontics for removable dentures since before the 1970s. The sibilant phoneme provides a reproducible position in three dimensions regardless of whether dentition is present or absent.30 This position also happens to be the most anterior superior position beyond which would interfere with speech and function.30,31 To date, minimal research has been done to determine whether the sibilant phoneme would provide a meaningfully position for dental sleep appliance therapy.
The purpose of this study is to compare two different mandibular positioning techniques for dental sleep appliance therapy. It was hypothesized that the sibilant phoneme technique will require less mandibular advancement compared with the current anterior protrusive technique, which uses 50% to 70% initial protrusion. The significance of this research involves minimizing the risk of dental sleep appliance side effects to patients including craniofacial changes, TMJ dysfunction, and progressive occlusal changes.
MATERIALS AND METHODS
This study was approved by Alberta Research Information Services: Human Research Ethics Board (Pro00088954).
Data Collection
Any patient not treated in accordance with AASM and American Academy of Dental Sleep Medicine (AADSM) guidelines was excluded from the study.5 All patients must have had OSA diagnosed by a physician, been treated with a custom and titratable dental sleep appliance, and have had pretreatment (pre-Tx) and posttreatment (post-Tx) sleep studies of level 3 or higher.1,32
For the study the definition of successful treatment for OSA was an AHI reduction of at least 50% and fewer than 10 events per hour.33 Inclusion criteria required successful treatment of the patient’s OSA by a dental sleep appliance and pre-Tx and post-Tx overjet and overbite positions or total change in overjet and overbite as measured by the treating clinical team. Other data collected included sex, age, body mass index (BMI), height, weight, ethnicity, other medical conditions, current medications, allergies, and signs and symptoms of pre-existing TMJ dysfunction and any changes to those conditions.
Based on the exclusion criteria and definition of successful treatment three practices providing dental sleep medicine treatment in the United States and one university/hospital research team in Spain agreed to participate. Retrospective data were collected during 2019 for patients previously treated by the clinicians for use in this project.
All clinicians who contributed data were either published researchers or board certified in dental sleep medicine. Detailed discussions with the individual clinicians indicated that all clinicians who provided patient data on the sibilant phoneme mandibular (SPM) technique followed the protocol published by Singh and Olmos whereas all clinicians who provided patient data on the anterior protrusive mandibular (APM) technique followed the protocol published by Mayoral et al.24,31 Although there were other clinicians who volunteered to provide patient data, their participation was declined due to either inability to confirm specific details on their SPM or APM technique or missing data points required for this project that they did not routinely collect or record into patient charts (including not recording pre-Tx or post-Tx AHI interpreted by a sleep physician (or equivalent) in the patient charts and keeping copies of the sleep reports where appropriate). All clinicians who contributed data to the project were provided with detailed instructions on the specific data points to extract from patient charts and a database into which to input the data points. All data provided were reviewed and patients that did not meet inclusion criteria (specifically, patients that did not have an AHI reduction of at least 50% and fewer than 10 events per hour) were removed. Because of the retrospective nature of this study, requiring consecutive patient data from the participating clinics was not possible. General inclusion criteria for treatment included any patient that could be treated within AASM and AADSM treatment parameters. Dental measurements within each clinic were taken by a single clinician per clinic.
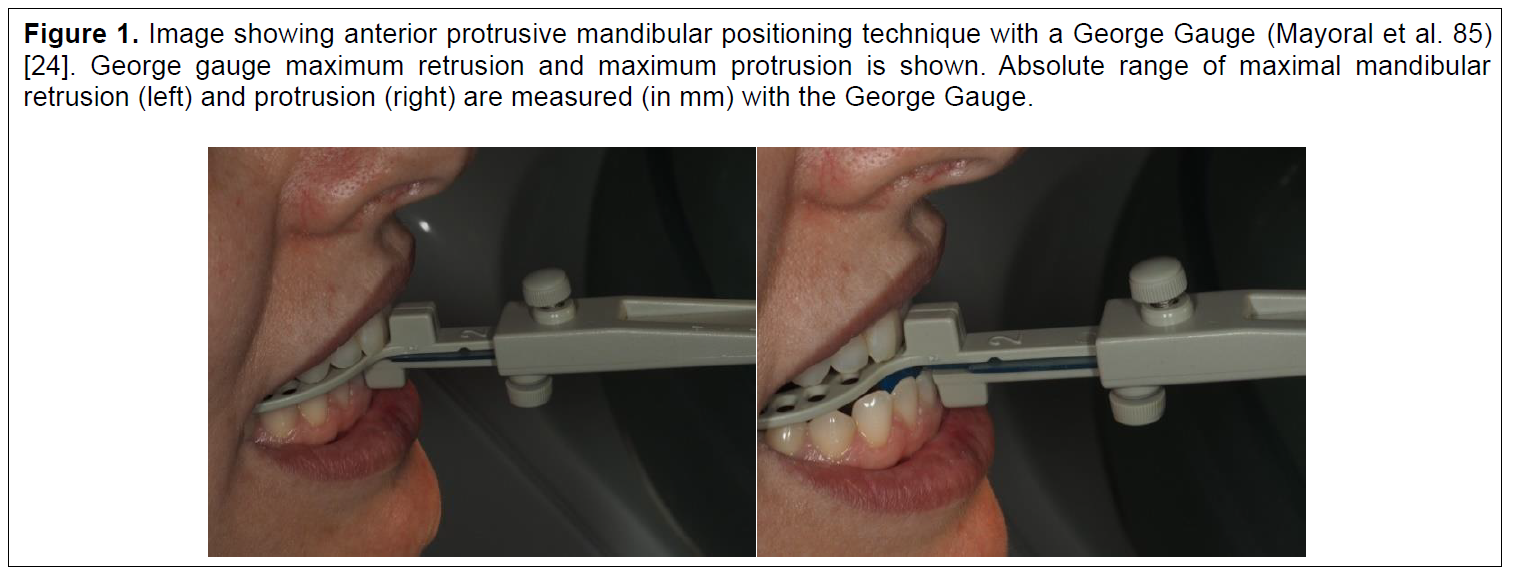
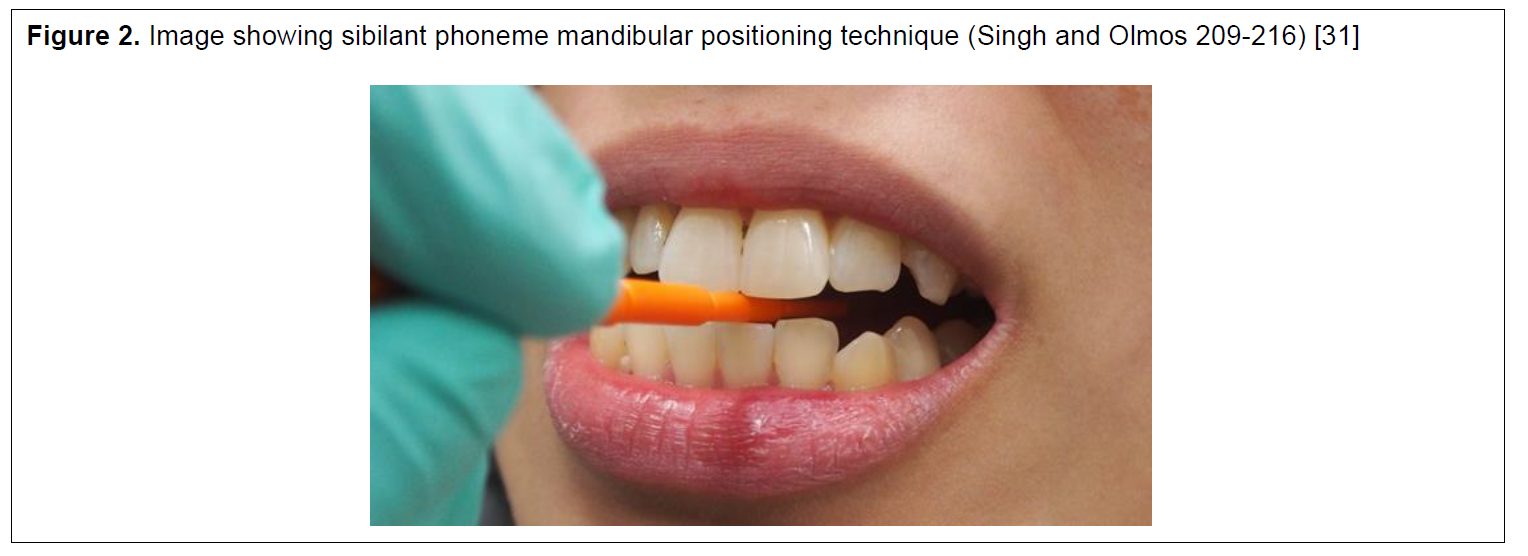
A total of 19 patients with SPM positioning were collected from the clinical teams in the United States and a total of 44 patients with APM positioning were collected from the research team in Spain that fell within the inclusion criteria. Based on discussions with the clinicians who provided their data for analysis, the APM position was obtained in accordance with previous research done by Mayoral et al.24 (Figure 1) whereas the SPM position was obtained in accordance with previous research done by Singh and Olmos31 (Figure 2). From data collected and discussions with the clinicians who provided data for analysis, patients were primarily treated with OrthoApnea (https://www.orthoapnea.com/en/) and Diamond Digital Sleep Orthotic (https://diamondorthoticlab.com/) dental sleep appliances.
Power Calculation
To determine the minimum per group sample size, we used the Massachusetts General Hospital Biostatistics sample size calculator (http://hedwig.mgh.harvard.edu/biostatistics/). The parameters were a quantitative parallel study with a two-tailed significance of 5%, power of 0.8, and difference in means of one standard deviation.34 The sample size necessary with these parameters was 34 (17 per group).
Statistical Tests
In analyzing the data, the Pearson correlation was used to test for correlations between continuous variables (for example, AHI and age). The Welch t-test was used to compare between groups due to group size differences and the inability to assume equal variances between groups. Descriptive statistics are provided, and subgroup analysis was also performed to separate patients with mild and moderate apnea from those with severe apnea within groups.
Figure 1Image showing anterior protrusive mandibular positioning technique with a George Gauge (Mayoral et al. 85) [24]. George gauge maximum retrusion and maximum protrusion is shown. Absolute range of maximal mandibular retrusion (left) and protrusion (right) are measured (in mm) with the George Gauge. |
{kind=link}
Figure 2Image showing sibilant phoneme mandibular positioning technique (Singh and Olmos 209-216) [31] |
{kind=link}
RESULTS
Hypothesis
The primary comparative value in the study is the total change in overjet between the two treatment interventions. Therefore, the null hypothesis is that there is no difference in total change in overjet between the SPM and APM techniques for mandibular positioning. Total change was understood to be the difference between pre-Tx overjet and post-Tx overjet.Descriptive Data
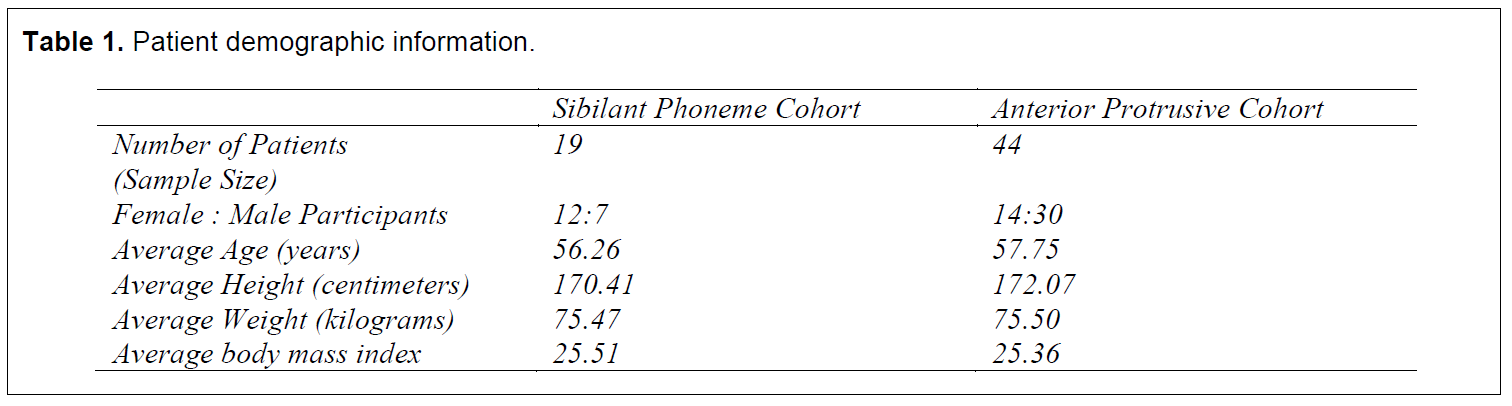
Patient demographic information is provided in Table 1.On average, patients were middle aged (45 to 65 years old) and overweight (BMI of 25 to 29 kg/m2).
SPM Position
From data reported by the clinicians, no patients developed any symptoms of TMJ dysfunction (joint noises, myalgia/muscle pain), nor any post-Tx limitations to mandibular range of motion. No patients found it necessary to temporarily halt treatment for any reason. One patient treated with the sibilant phoneme technique required jaw relaxation exercises (jaw opening exercises to stretch mandibular muscles).35, 36 Several patients had increased mandibular range of motion and/or reported reduced facial myalgia post-Tx.APM Position
From data reported by the clinicians, three patients reported transient temporal myalgia, one patient reported transient masseteric myalgia, and two patients reported transient joint noises during treatment. All of these reported transient symptoms were resolved within 3 months of the start of treatment. In another two patients, prolonged masseteric myalgia developed that did not resolve within 3 months. Six patients reported pre-Tx temporal and/or masseteric myalgia that resolved during their treatment whereas one patient’s reported temporal and masseteric myalgia did not resolve during treatment. In no patients did any post-Tx limitations to mandibular range of motion develop. Ten patients treated with the anterior protrusive technique required jaw relaxation exercises. Two patients temporarily halted treatment because of the development of symptoms. Several patients had increased mandibular range of motion and/or reported reduced facial myalgia post-Tx.Statistical Analytics
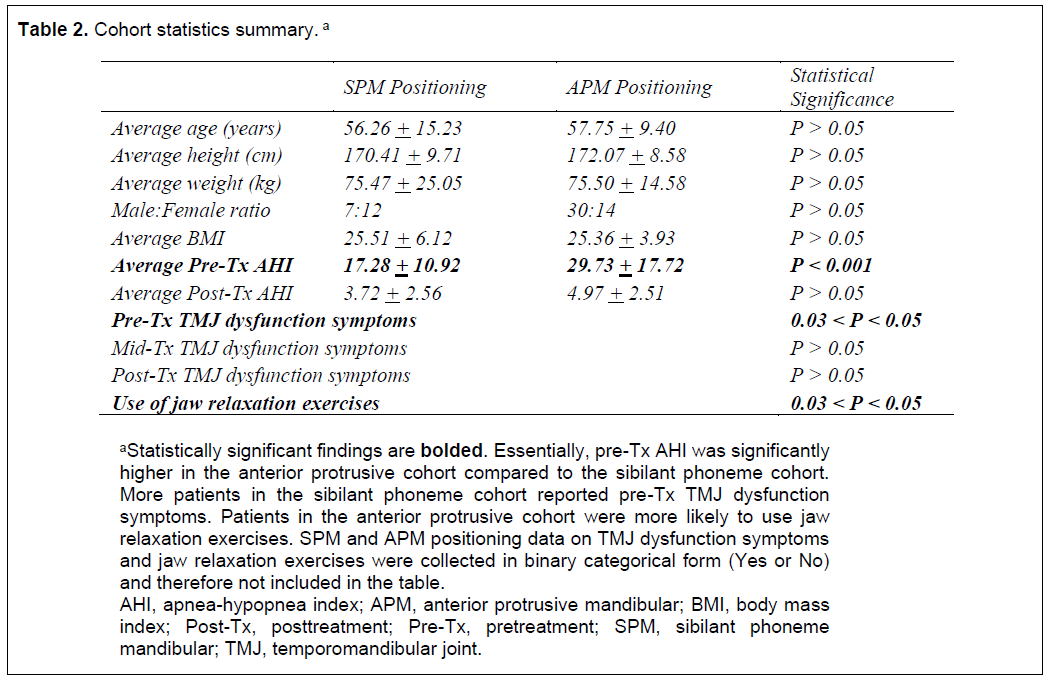
Pearson’s Correlation analysis was run across all patients to determine if pre-Tx AHI, change in AHI, and post-Tx AHI were significantly associated with age, gender, height, weight, and BMI as well as with pre-, mid-, and post-Tx TMJ dysfunction symptoms. Statistically significant associations were found between pre-Tx AHI and age (r = 0.25, P < 0.05) and BMI (r = 0.25, P < 0.05). Statistically significant associations were found between AHI reduction and BMI (r = 0.26, P < 0.05). No statistically significant associations were found between post-Tx AHI and age, sex, height, weight, BMI, and pre-, mid-, and post-Tx TMJ dysfunction symptoms. All statistically significant Pearson correlations were positive and moderate in value (0.2 < P < 0.04).To determine whether the two samples were comparable, Welch’s t-test was performed to compare pre-Tx and post-Tx AHI between the two cohorts, respectively. Pre-Tx AHI was significantly different (P < 0.001), whereas post-Tx AHI was not statistically different (P > 0.05).
Review of the cohorts showed that although the SPM group had only two patients with an AHI within the severe criteria, the APM group had 15 patients with an AHI within the severe criteria. In accordance with AASM guidelines, the criterion for determining severe sleep apnea was an AHI > 30 events per hour. Therefore, subgroup analysis was performed excluding all patients with an AHI > 30 events per hour.
Subgroup Differences
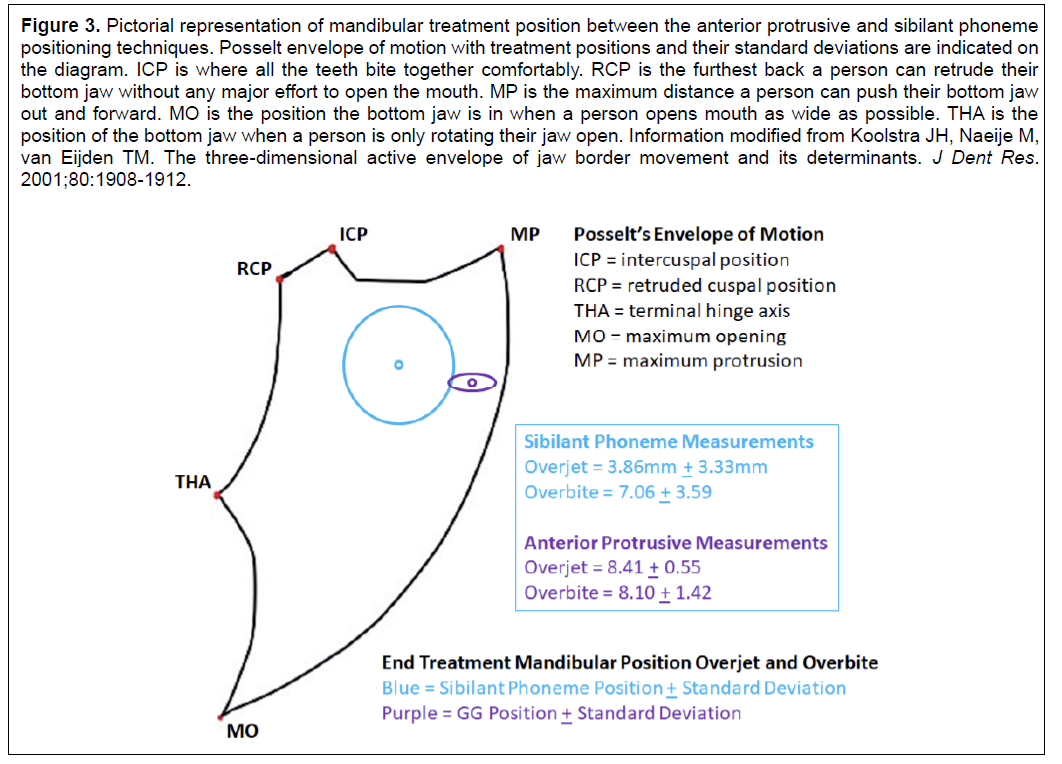
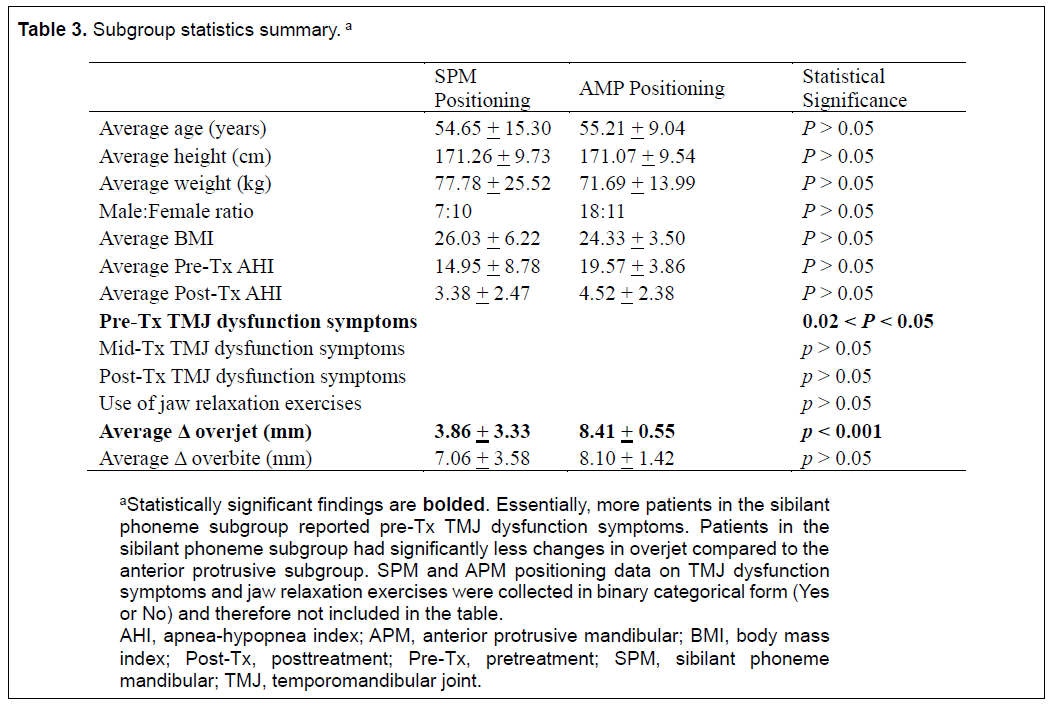
Statistically significant differences were found between the two subgroups in pre-Tx TMJ dysfunction symptoms (0.02 < P < 0.05) and change in overjet (P < 0.001). SPM change in overjet averaged 3.86 mm whereas APM change in overjet averaged 8.41 mm. There were no other statistically significant differences between the two subgroups.Summary of Statistics
Findings are summarized in Table 2. Subgroup findings are summarized in Table 3.Figure 3 depicts mandibular treatment position between the APM and SPM positioning techniques within the Posselt envelope of motion.
Figure 3Pictorial representation of mandibular treatment position between the anterior protrusive and sibilant phoneme positioning techniques. Posselt envelope of motion with treatment positions and their standard deviations are indicated on the diagram. ICP is where all the teeth bite together comfortably. RCP is the furthest back a person can retrude their bottom jaw without any major effort to open the mouth. MP is the maximum distance a person can push their bottom jaw out and forward. MO is the position the bottom jaw is in when a person opens mouth as wide as possible. THA is the position of the bottom jaw when a person is only rotating their jaw open. Information modified from Koolstra JH, Naeije M, van Eijden TM. The three-dimensional active envelope of jaw border movement and its determinants. J Dent Res. 2001;80:1908-1912. |
{kind=link}
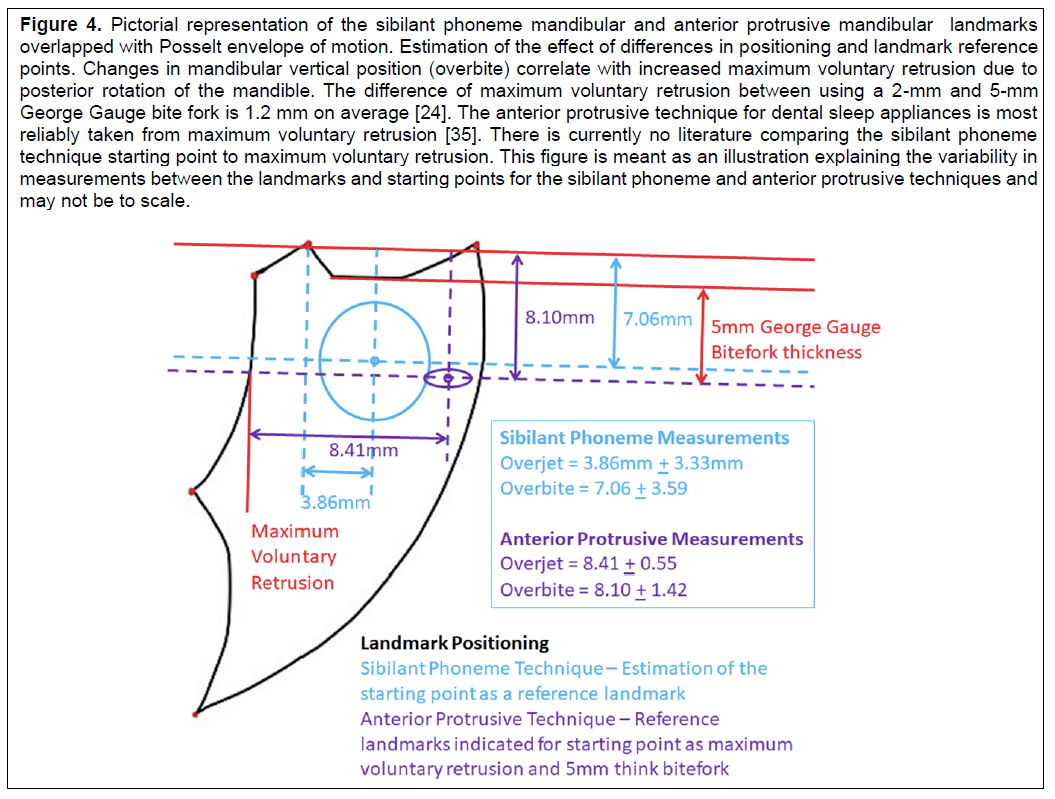
Figure 4Pictorial representation of the sibilant phoneme mandibular and anterior protrusive mandibular landmarks overlapped with Posselt envelope of motion. Estimation of the effect of differences in positioning and landmark reference points. Changes in mandibular vertical position (overbite) correlate with increased maximum voluntary retrusion due to posterior rotation of the mandible. The difference of maximum voluntary retrusion between using a 2-mm and 5-mm George Gauge bite fork is 1.2 mm on average [24]. The anterior protrusive technique for dental sleep appliances is most reliably taken from maximum voluntary retrusion [35]. There is currently no literature comparing the sibilant phoneme technique starting point to maximum voluntary retrusion. This figure is meant as an illustration explaining the variability in measurements between the landmarks and starting points for the sibilant phoneme and anterior protrusive techniques and may not be to scale. |
{kind=link}
Table 1Patient demographic information. |
{kind=link}
Table 2Cohort statistics summary. a |
{kind=link}
Table 3Subgroup statistics summary. a |
{kind=link}
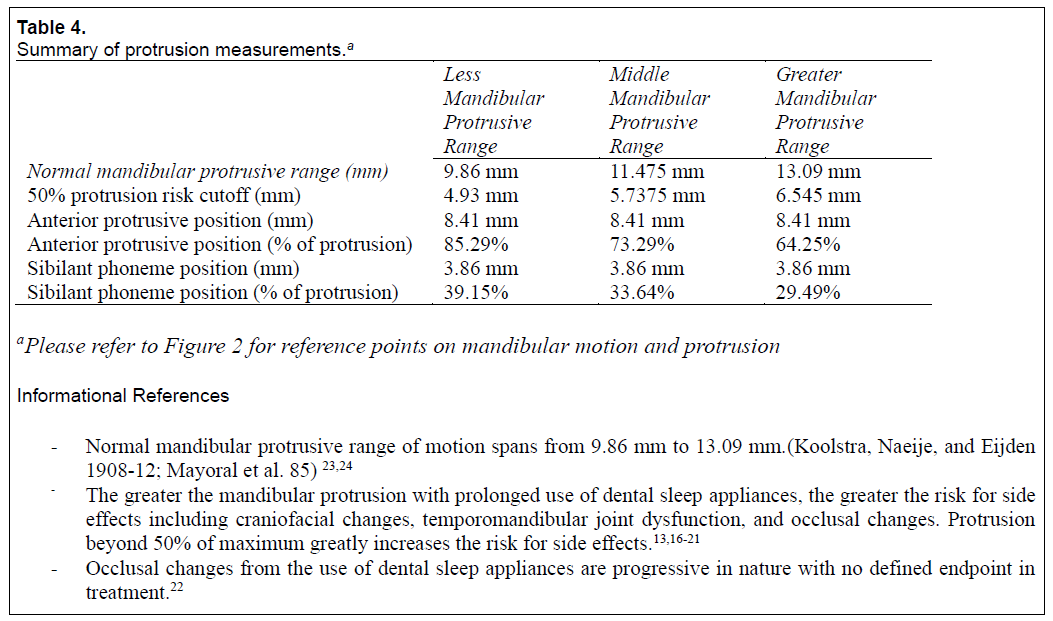
Table 4Summary of protrusion measurements.a |
{kind=link}
DISCUSSION
Although the APM method has been taught and used extensively in dentistry for determining initial mandibular position for dental sleep appliances, recently published literature indicates other methods may provide similar clinical outcomes while potentially decreasing the risk of side effects associated with dental sleep appliances.28,29 We designed this study to investigate whether commonly used prosthodontic methods for determining mandibular position by use of an SPM technique would yield results similar to those of the APM method. Specifically, one goal of the study was to determine whether the SPM technique would provide for a smaller change in overjet and overbite in comparison with the APM technique for mandibular positioning.
Because the two samples were not similar in pre-Tx AHI, likely due to the disparity in the number of patients with severe OSA, subgroup analysis to exclude patients with severe apnea was warranted. The reasoning for the subgroup analysis was that previous research has indicated that the more severe the AHI, the greater the protrusion necessary for treatment efficacy using the APM method.13,19-21 Therefore, any analyses run with unequal pre-Tx AHI would potentially compromise the purpose of the study.
Review of the subgroup analyses showed no statistical differences between the two subgroups in pre-Tx AHI and biographical data (age, sex, weight, height, BMI) and no difference in post-Tx AHI. This indicated that the subgroups were comparable, and that the two methods did not affect management of the patient’s AHI. Furthermore, the sample size for both the cohorts and the subgroups met the minimum threshold as set by the power analysis. Based on this understanding and in review of the data showing a strong statistical difference in total overjet change between subgroups of the two interventions, the null hypothesis that there is no difference in total change in overjet between the SPM and APM techniques for mandibular positioning was rejected. The SPM technique requires less total change in overjet compared to the APM technique.
Other findings indicate minimally significant differences in AHI reduction outcomes between the two subgroups, though the difference between the two subgroups in pre-Tx TMJ dysfunction symptoms may warrant further investigation. The differences in use of jaw relaxation exercises, combined with no difference in post-Tx TMJ dysfunction symptoms, suggests the APM method may lead to greater transient TMJ dysfunction symptoms. However, the lack of difference in midtreatment (mid-Tx) TMJ dysfunction symptoms potentially contradicts this theory. Further research into this area is warranted.
The average post-Tx overjet for the APM method was 8.41 mm, whereas the average post-Tx overjet for the SPM method was 3.86 mm. The difference in final mandibular position between the two methods was, on average, 4.56 mm. Conservatively, the average end of treatment protrusion using the APM method was 64% whereas for the SPM method it was 29%, a difference in protrusive range of 35%. Because protrusion beyond the range of 4.93-6.55 mm (beyond 50% of protrusive range) greatly increases the risk of the development of side effects such as occlusal changes and TMJ dysfunction symptoms, a difference of 4.56 mm in protrusion should be considered significant for dental sleep appliances. Table 4 explains these percentages.
Such a decrease in overjet could significantly decrease the risk of TMJ dysfunction side effects commonly associated with the use of dental sleep appliances. The study results suggest that the use of a SPM technique compared to the APM technique may be able to achieve similar clinical efficacy in managing the AHI in a patient with OSA while also potentially providing a mandibular position with decreased risk of the development of TMJ dysfunction symptoms and occlusal changes commonly associated with the use of dental sleep appliances.
However, recently published literature also notes that there can be significant variability in overjet measurements when using different landmarks for starting position. A recent study has shown the difference between habitual bite position and maximum voluntary retrusion, as a starting point when assessing mandibular advancement when using the George Gauge, yields an overjet difference of 4.81 + 1.75 mm.37 This may explain discrepancies between the results of previous studies. Another recent study has indicated that the SPM technique uses different landmarks than the habitual bite position or maximum voluntary retrusion used with the APM technique.38 To date, no studies have directly compared the landmarks used for starting points neither between the techniques nor for their corresponding overjet and overbite measurements. Research on the effects of mandibular position and changes in landmarks may provide insight into some of this variability. Although changes in overbite in the study were not statistically significant, overbite with the SPM method was on average 1.04 mm smaller. Changes in mandibular vertical position (overbite) significantly affect landmark position, with a change of 3 mm in vertical position leading to a 2- to 3-mm change in horizontal (overjet) landmark location.24 An estimation of these effects on position between the two techniques is illustrated in Figure 4. This difference in reference landmarks may account for some of the variability found in the technique comparison outcomes. Further investigation is required to determine how much variability between the SPM and APM techniques and measurements may be from differences in landmarks.
There are significant differences in the effort and materials required between the APM and SPM techniques. Although the APM technique requires a protrusive gauge of some sort, the SPM method requires the use of a round bite stick or similar object (a microbrush, thin round wooden dowel, or tri-syringe/air-water syringe tip are all acceptable). The protrusive gauges necessary for the APM technique have a range of costs, some with an initial cost of $100 and a per-impression cost of $1.00 per bite fork, whereas other gauges are single use and cost approximately $100 each. For the APM technique, most protrusive gauges have set vertical (overbite) dimensions (George Gauge bite forks are 2 mm and 5 mm). For the SPM technique, vertical dimension can be set at whatever bite stick thickness the clinician has on hand. In both techniques, the accuracy of the bite registration is critical to successful treatment. However, the SPM technique has a greater learning curve and is more prone to error for the inexperienced clinician. These differences may explain why the APM method is much more popular and well known among dental practitioners.
The results of the current study should be viewed with caution because of several limitations. One of the primary limitations of the study was the large differences in sample size between the two samples. This difference was addressed as adequately as possible statistically and in subgroup analysis. Another significant limitation was the retrospective nature of the study, meaning no evaluation for both inter-operator and intraoperator primary data point measurement (in reference to overjet and overbite) variability was possible (as previously mentioned, intraoperator self-evaluation for measuring overjet and overbite is not routinely done in clinical private practice; this makes calculating intraoperator kappa impossible for this study). Other limitations include potential interoperator patient inclusion criteria variability, nonsequential nonrandomized patient selection, differences and variability between the sleep physicians who diagnose OSA and the AHI/respiratory disturbance index values, night-to-night variability in patient sleep testing, potential patient selection bias, limited prior published research with which to establish baseline protocols, differences in dental sleep appliances and patient variability and tolerance with different dental sleep appliances, differences in equipment, differences in treatment teams, and potentially the use of only 5-mm bite forks for the George Gauge. Any conclusions drawn from this study should account for these limitations and should be further investigated with future prospective randomized trials. However, the data and results in our study indicate that the sibilant phoneme method for mandibular positioning for dental sleep appliances warrants further study and that this study provides a foundational stepping stone upon which future research can be built. Future studies should investigate this relationship in a prospective fashion and the differences between the APM and SPM methods on total oral volume and on mandibular position using a three-dimensional approach.
CONCLUSIONS
The study results suggest that the use of a sibilant phoneme technique is an alternative to an anterior protrusive technique for determining mandibular position due to decreased protrusion necessary to reach the same reduction in the AHI of patients with OSA. This decreased protrusion necessary for treatment may decrease the risk of the development of TMJ dysfunction (facial myalgia/muscle pain, joint noises, and joint pain) and occlusal/bite changes, among other side effects, with the use of dental sleep appliances. Further research into the use of the sibilant phoneme technique for dental sleep appliances is warranted.
ABBREVIATIONS
AHI, apnea-hypopnea index
APM, anterior protrusive mandibular
AASM, American Academy of Sleep Medicine
AADSM, American Academy of Dental Sleep Medicine
BMI, body mass index
OSA, obstructive sleep apnea
Pre-Tx, pretreatment
Post-Tx, posttreatment
Mid-Tx, midtreatment
PVS, polyvinyl siloxane
SPM, sibilant phoneme mandibular
TMJ, temporomandibular joint
ACKNOWLEDGMENTS
This research was supported in part by the University of Alberta School of Dentistry and Faculty of Graduate Studies and Research.
The authors would like to thank Dr. David Shirazi, Dr. Michael Giesy, and Dr. Steven Olmos for their generosity in data collection and sharing information related to dental sleep appliances. Without their contribution this research would not have been possible.
REFERENCES
- Kapur VK, Auckley DH, Chowdhuri DC, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2017;13:479-504.
- Osman AM, Carter SG, Carberry JC, Eckert DJ. Obstructive sleep apnea: current perspectives. Nat Sci Sleep. 2018;10:21-34.
- Eckert DJ. Phenotypic approaches to obstructive sleep apnoea - new pathways for targeted therapy. Sleep Med Rev. 2018;37:45-59.
- American Academy of Sleep Medicine. Practice Guidelines 202.) Available at https://aasm.org/clinical-resources/practice-standards/practice-guidelines/. Accessed March 2020. (American Academy of Sleep Medicine )
- Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: an update for 2015. J Clin Sleep Med. 2015;11: 773-827.
- S. Gianoni-Capenakas S, Gomes AC, Mayoral P, Miguez M, Pliska B, , Lagravère M. Sleep-disordered breathing: the dentists’ role – a systematic review. J Dent Sleep Med. 2020;7:1. Available at: https://aadsm.org/journal/review_article_1_issue_71.php. Accessed March 2020.
- Ngiam J, Balasubramaniam R, Darendeliler MA, Cheng AT, Waters K, Sullivan CE. Clinical guidelines for oral appliance therapy in the treatment of snoring and obstructive sleep apnoea, Aust Dent J. 2013;58:408-419.
- Hoekema A, Stegenga B, de Bont LGM. Efficacy and co-morbidity of oral appliances in the treatment of obstructive sleep apnea-hypopnea: a systematic review. Crit Rev Oral Biol Med. 2004;15:137-155.
- Burke P, Knapman F, Tong B, et al. Effects of mandibular advancement splints on upper airway physiology in obstructive sleep apnoea [Abstract]. J Sleep Res. 2018;27:114.
- Brown L, Juge L, Burke P, Sutherland K, Cistulli P, Bilston L. How lateral airway tissues affect upper airway dimensions with mandibular advancement in obstructive sleep apnoea. Eur Respir J. 2018;52:OA5369.
- Juge L, Knapman F, Eckert D, et al. Tongue deformation during mandibular advancement may help to predict mandibular advancement treatment outcome in obese patients with obstructive sleep apnoea [Abstract]. J Sleep Res. 2018;27:0037.
- Chan ASL, Sutherland K, Schwab RJ, et al. The effect of mandibular advancement on upper airway structure in obstructive sleep apnoea. Thorax. 2019;65:726-732.
- Ferguson KA, Cartwright R, Rogers R, Schmidt-Nowara W. Oral appliances for snoring and obstructive sleep apnea: a review, Sleep. 2006;29:244-262.
- Marklund M, Franklin KA, Persson M. Orthodontic side-effects of mandibular advancement devices during treatment of snoring and sleep apnoea. Eur J Orthod. 2001;23:135-144.
- Giannasi LC, Almeida FR, Magini M, et al. Systematic assessment of the impact of oral appliance therapy on the temporomandibular joint during treatment of obstructive sleep apnea: long-term evaluation. Sleep Breath. 2009;13:375-381.
- Sheats RS, Schell TG, Blanton AO, et al. Management of side effects of oral appliance therapy for sleep-disordered breathing. J. Dent Sleep Med. 2017;4:111-125.
- de Almeida FR, Bittencourt LR, de Almeida CIR, Tsuiki S, Lowe AA, Tufik S. Effects of mandibular posture on obstructive sleep apnea severity and the temporomandibular joint in patients fitted with an oral appliance. Sleep. 2002;25:507-513.
- Minagi HO, Okuno K, Nohara K, Sakai T. Predictors of side effects with long-term oral appliance therapy for obstructive sleep apnea. J Clin Sleep Med. 2018;14:119-125.
- Kato J, Isono S, Tanaka A, Watanabe T, et al. Dose-dependent effects of mandibular advancement on pharyngeal mechanics and nocturnal oxygenation in patients with sleep-disordered breathing. Chest. 2000;117:1065-1072.
- Rose E, Staats R, Virchow C, Jonas IE. A comparative study of two mandibular advancement appliances for the treatment of obstructive sleep apnoea. Eur J Orthod. 2002;24:191-198.
- Walker-Engström ML, Ringqvist I, Vestling O, Wilhelmsson B, Tegelberg A. A prospective randomized study comparing two different degrees of mandibular advancement with a dental appliance in treatment of severe obstructive sleep apnea. Sleep Breath. 2003;7:119-130.
- Pliska BT, Nam H, Chen H, Lowe AA, Almeida FR. Obstructive sleep apnea and mandibular advancement splints: occlusal effects and progression of changes associated with a decade of treatment. J Clin Sleep Med. 2014;10:1285-1291.
- Koolstra JH, Naeije M, van Eijden TM. The three-dimensional active envelope of jaw border movement and its determinants. J Dent Res. 2001;80:1908-1912.
- Mayoral P, Lagravère MO, Míguez-Contreras M, Garcia M. Antero-posterior mandibular position at different vertical levels for mandibular advancing device design. BCM Oral Health. 2019;19:85.
- Gindre L, Gagnadoux F, Meslier N, Gustin JM, Racineux JL. Mandibular advancement for obstructive sleep apnea: dose effect on apnea, long-term use and tolerance. Respiration. 2008;76: 386-392.
- Gupta A, Tripathi A, Trivedi C, Sharma P, Mishra A. A study to evaluate the effect of different mandibular horizontal and vertical jaw positions on sleep parameters in patients with obstructive sleep apnea. Quintessence Int.2016;47:661-666.
- Aarab G, Lobbezoo F, Hamburger HL, Naeije M. Effects of an oral appliance with different mandibular protrusion positions at a constant vertical dimension on obstructive sleep apnea. Clin Oral Investig. 2010;14:339-345.
- Anitua E, Durán-Cantolla J, Almeida GZ, Alkhraisat MH. Minimizing the mandibular advancement in an oral appliance for the treatment of obstructive sleep apnea. Sleep Med. 2017;34:226-231.
- Bartolucci ML, Bortolotti F, Raffaelli E, D’Antò V, Michelotti A, Bonetti GA. The effectiveness of different mandibular advancement amounts in OSA patients: A systematic review and meta-regression analysis. Sleep Breath. 2016;20:911-919.
- 3Pound E. Let /S/ be your guide. J Prosthet Dent. 1977;38:482-489.
- Singh GD, Olmos S. Use of a sibilant phoneme registration protocol to prevent upper airway collapse in patients with TMD. Sleep Breath. 2007;11:209-216.
- Collop NA, Anderson WM, Boehlecke B, et al. Clinical guidelines for the use of unattended portable monitors in the diagnosis of obstructive sleep apnea in adult patients, Portable monitoring task force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2007;3:737-747.
- Mogell K, Blumenstock N, Mason E, RohatgI R, Shah S, Schwartz D. Definition of an effective oral appliance for the treatment of obstructive sleep apnea and snoring: an update for 2019. J Dent Sleep Med. 2019;6.
- Jain S, Gupta A, Jain D. Estimation of sample size in dental research. Int Dent Med J Adv Res. 2015;1:1-6.
- Ishiyama H, Inukai S, Nishiyama A, et al. Effect of jaw-opening exercise on prevention of temporomandibular disorders pain associated with oral appliance therapy in obstructive sleep apnea patients: A randomized, double-blind, placebo-controlled trial. J Prosthodont Res. 2017; 61(3):259-267.
- Cunali P, Almeida F, Santos C, et al. Mandibular exercises improve mandibular advancement device therapy for obstructive sleep apnea. Sleep Breath. 2010;15(4):717–727.
- Ippolito DR, Stipa C, Cameli M, Sorrenti G, Pelligra I, Alessandri-Bonetti G. Maximum voluntary retrusion or habitual bite position for mandibular advancement assessment in the treatment of obstructive sleep apnoea patients. J Oral Rehabil. 2020;47(3):301-306. [Epub ahead of print]
- Viviano J, Klauer D, Olmos S, Viviano JD. Retrospective comparison of the George GaugeTM registration and the sibilant phoneme registration for constructing OSA oral appliances. Cranio. 2019;26:1-9.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication June 9, 2020
Submitted in final revised form September 23, 2020
Accepted for publication October 1, 2020
Dr. Enoch Ng, DDS, Graduate Student, School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, 11405 - 87th Avenue, Edmonton, Alberta Canada, T6G 1C9; Email: enoch@ualberta.ca