Review Article 1, Issue 7.1
Sleep-Disordered Breathing: The Dentists’ Role – A Systematic Review
http://dx.doi.org/10.15331/jdsm.7108
Silvia Gianoni-Capenakas, DDS, MSc, PhD1, Andre Chiconelli Gomes, DDS2, Pedro Mayoral, DDS, MSc, PhD3, Manuel Miguez, DDS, MSc, PhD4,5, Benjamin Pliska, DDS, MSc, PhD6, Manuel Lagravere, DDS, MSc, PhD7
1Student Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, 2Orthodontist, Private Clinic, São Paulo, Brazil, 3Professor of Dentistry, Director Dental Sleep Medicine Program, Catholic University of Murcia UCAM, Madrid, Spain, 4Professor of Dentistry, Orthodontics Department, Catholic University of Murcia UCAM and Universidad de Salamanca (USAL), 5co-Director Dental Sleep Medicine at Universidad Católica de San Antonio de Murcia (UCAM), Madrid, Spain, 6Assistant Professor, Department of Oral Health Sciences, Faculty of Dentistry, University of British Columbia, Vancouver, Canada, 7Associate Professor Orthodontics Department. School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Canada
ABSTRACT
Study Objectives:
Although dentists have an important role related to sleep disorders, there is a concern about how far dentists can go when screening or treating these patients. The objective of this systematic review is to present guidelines, recommendations, and studies designed with the intention to describe and guide the role of dentists in sleep-disordered breathing (SDB)–related issues.1
Methods:
The eligibility criteria were guidelines, protocols, and recommendations focused on determining the role of dentists in the sleep disorders topic. The search was conducted through the databases Cochrane, EMBASE, Medline, LILACS, PubMed, and Web of Science. This systematic review was reported according to the preferred reporting items for systematic review and meta-analysis protocols (PRISMA).1
Results:
Overall, a total of 1,432 studies were found in the 6 databases searched. After removing duplicates, the studies were evaluated by title and abstract. In the second phase, 231 studies were evaluated by reading their full text. Twenty-two studies matched the inclusion criteria.
Conclusions:
Through this systematic review it is possible to conclude that the guidelines describe the role of dentists in screening patients for SDB/obstructive sleep apnea (OSA) as follows: refer the patients suspected of SDB/OSA to sleep physicians; apply, manage, and follow up the use of oral appliances.
Clinical significance:
All dentists should screen for SDB/OSA; however, only well-trained dentists with good knowledge of dental sleep medicine should be part of the multidisciplinary team to treat patients with SBD/OSA.
Keywords:
dentists’ role; guidelines; sleep-disordered breathing; sleep medicine
Citation:
Gianoni-Capenakas S, Gomes AC, Mayoral P, Miguez M, Pliska B, Lagravere M. Sleep-Disordered Breathing: The dentists’ role – A systematic review. J Dent Sleep Med. 2020;7(1)
INTRODUCTION
Sleep-disordered breathing (SDB) affects adults and children worldwide.2 SDB can reach high prevalence as shown by the HypnoLaus study, which found rates of 49.7% for men and 23% for women.3 It is estimated that approximately 23 million adults in the United States have undiagnosed or untreated moderate to severe obstructive sleep apnea (OSA).4,5 The main problem in patients with SDB/OSA is the pharyngeal collapse occurring in hypopnea (reduction in ventilation) or apnea (complete respiratory cessation).6 According to Guillerminault and Huang “the upper airway is a collapsible tube, and its collapsibility increases during sleep”.7 The increased levels of carbon dioxide (hypercapnia) and the low concentration of oxygen (hypoxemia) in the blood in these patients may lead to hypertension, cardiac diseases, and even premature death.4,6 SDB is also related to snoring, mood disorder, disruptive behavior, and depletion of quality of life.2,4,8,9 Some oral anatomic features associated with SDB may include high arched or narrow hard palate and retrognathia.2,8
The most common risk factor for sleep apnea in children is the airway constriction associated with enlarged tonsils and/or adenoids.10 Additionally, the atypical orofacial growing pattern of “adenoid facies” has been associated with SDB, and may lead to a reduced size of the upper airway; causing not just sleep breathing-related problems but also a constricted maxilla, usually causing posterior crossbites and crowded teeth.11 Impaired growth, cardiovascular problems, and learning and behavioral problems are also linked to SDB.5,12 Because these problems are critical and are related to craniofacial proportions, the dentist is the first person to recognize these issues.
The approach most often indicated to treat SDB in adults is the oral appliance (OA). The OA can be categorized into two types: mandibular advancement device (MAD),13 which aims to protrude the mandible and associated soft tissues to open the airway and reduce the apnea-hypopnea index (AHI)14; or the less frequently used tongue retaining device where the objective is to maintain the tongue in a forward position, to avoid obstruction of the airway.15 However, continuous positive airway pressure (CPAP) therapy is mostly used by sleep physicians and remains the gold standard for OSA treatment.2 More recently, several studies reported upper airway dimensional changes and AHI decrease in children and adolescents with posterior crossbites/maxillary constriction and retrognathia treated for maxillary expansion and mandibular advancement, respectively.16–18 In general, those studies, albeit lacking control groups, have encountered positive results in regard to an increase in upper airway dimension and breathing capacity.16–18
Although it is evident that dentists can have an important role related to SDB/OSA, the exact position of the dentist in the overall evaluation and treatment paradigm for patients with SDB/OSA continues to be debated. The objective of this systematic review is to summarize existing guidelines, recommendations, and studies designed with the intention to describe and guide the role of dentists in SDB- related issues.
METHODS
Protocol and Registration
This systematic review was reported according to the preferred reporting items for systematic review and meta-analysis protocols, or PRISMA.19
Eligibility Criteria
Guidelines, protocols, and recommendations focused on determining the role of dentists in SDB/OSA were included in this study. No limits in year or language were applied.
Information Sources-Search strategy
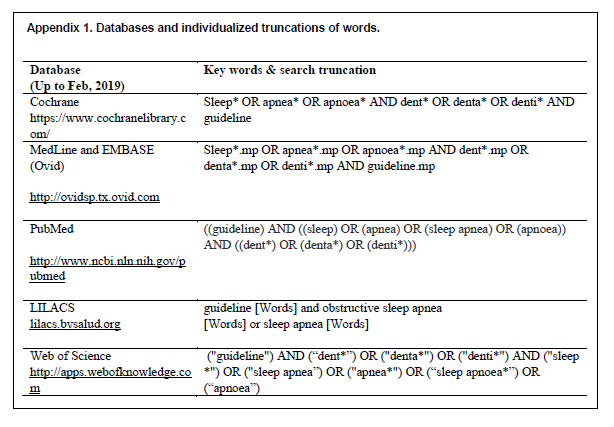
The following databases were included in the search strategy: Cochrane, EMBASE, Medline, LILACS, PubMed, and Web of Science. The search strategy used in this review is available in Appendix 1. All searches were conducted in February 2018 and updated in February 2019. The references were managed, and the duplicates were removed using the RefWorks software (ExLibris a ProQuest LCC Company- Jerusalem, Israel).
Two independent reviewers (SG-C and ACG) proceeded with the search on the selected databases.
Study Selection
The study selection was conducted in two phases. In the first phase, two reviewers (SG-C and ACG) independently checked the titles and abstracts of all studies identified. In the second phase, the same two reviewers evaluated the remaining articles, analyzing the full text to include only those that fulfilled the eligibility criteria.
Data Collection Process
The data collection was extracted by two authors (SG-C and ACG). Table 1 displays the following information extracted from the studies: authors, country, year, objective, methods, the role of dentists, dental clinical procedures, additional information, results, and conclusions.
Studies Design and Detail |
Summary Measures
The main outcome was to determine the role of dentists in patients with SDB.Synthesis of Results
A list of the possible role of dentists in view of the SDB problems was made from each article.
RESULTS
Selection of Studies
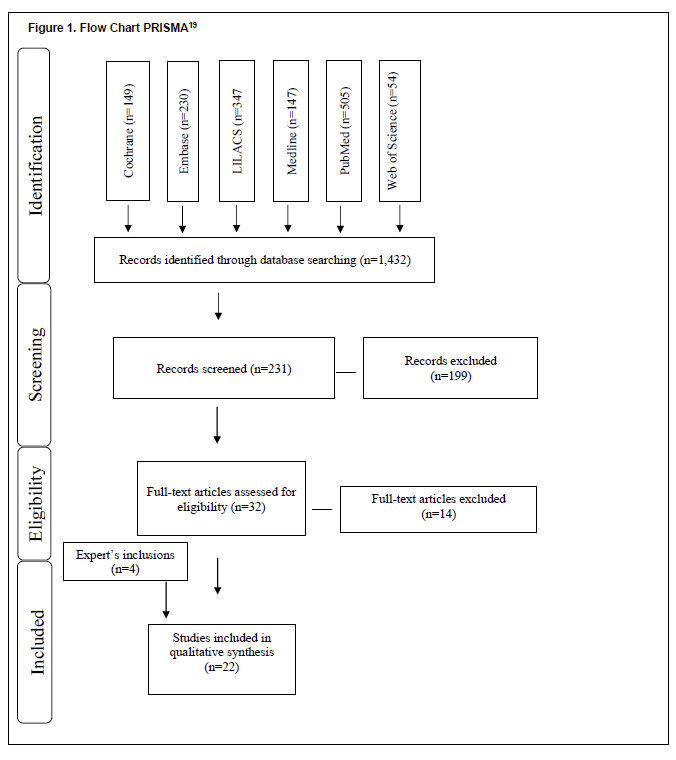
Overall 1,432 studies were found in the six databases searched: Cochrane, Embase, Lilacs, Medline, PubMed, and Web of Science. After removing duplicates, the studies were evaluated by title and abstract. In the second phase, 231 studies were evaluated by reading their full text. Eighteen studies matched the inclusion criteria. Four studies were included by the experts, for a total of 22 included studies. Figure 1 maps the selection process.
Flow Chart PRISMA19 |
{kind=link}
Study Characteristics
The selected studies were published between 1999 and 2019. One was published in Italian,20 and the others were published in English.4,11,13,15,20-37 Recommendations made by the studies included in this systematic review were for the dentists’ clinical practice in patients with OSA, SDB or snoring. Most of the included studies were based on or were the guideline itself from an accredited dental or medical association as follows: American Association of Orthodontics (AAO)33; American Academy of Dental Sleep Medicine (AADSM)4,21; American Academy of Sleep Medicine (AASM)22,23; AADSM + AASM24; AASM + German Sleep Society25; American Academy of Craniofacial Pain;26 Canadian Sleep Society;27 American College of Prosthodontists;15 American Dental Association (ADA);11 German Society of Otorhinolaryngology, Head and Neck Surgery + Association of Scientific Medical Societies in Germany.28 A group of Italian dental societies also involved with the Italian Association of Sleep Medicine13; and British Society of Dental Sleep Medicine.29 Nonetheless, the statements regarding the role of dentists when treating SDB/OSA made by the studies not linked to a medical or dental association are basically the same.
Results of Individual Studies
Studies’ recommendations for ALL dentists:
Dentists/orthodontists/prosthodontists should screen for potential patients with SDB/OSA.4,9,29–33,11,13,15,20,22,24,27,28
Screening could include questionnaires, such as the validated tool for OSA risk assessment STOP-Bang questionnaire, the Epworth Sleepiness Scale, Friedman Tongue Classification System, Kushida Index, or Berlin Questionnaire for Sleep Apnea; evaluation of neck size and body mass index; modified Mallampati classification to describe the patency of oral airway.33
Refer to the sleep physician or otolaryngologist when SDB/OSA is suspected.9,11,15,20,24,27,29,31,32,33
Studies’ recommendations for OA:
- OA is an effective therapy for OSA.15,21,33
- OA is indicated for patients with mild to moderate OSA who prefer OAs to CPAP therapy or who do not respond to CPAP therapy or have contraindications for the use of CPAP therapy, although the sleep physicians are responsible for prescribing the most appropriate or acceptable treatment option.11,13,30,31,34,35,15,20,22–25,27,29
- OA can significantly decrease the AHI, respiratory disturbance index, and respiratory event index, independently of OSA severity.15,21
- Reduction in AHI before and after treatment with OAs versus CPAP has no statistically significant differences (P = 0.44). 21
- The sleep physician should prescribe OA rather than no treatment for adult patients who request treatment of primary snoring and also for patients with OSA who do not tolerate CPAP therapy.21,23
- The evaluation of OA treatment efficacy should be done by the sleep physician with sleep testing.4,11,32,33
Studies recommendations for the management/treatment of SDB by qualified dentists:
- Only qualified dentists should manage SDB/OSA and snoring screening and therapy.4,9,15,21–23,25–28,32,33,34,35
- When an OA is prescribed, the qualified dentist should use a custom, titratable appliance over noncustom oral devices.4,11,21,24,33,32
- The dentist should instruct patients with OA to return for follow-up, and evaluate possible dental-related side effects such as occlusal changes and long-term effects.4,15,34,21–24,26,31–33
- The dentist can acquire objective information with a portable monitor for purposes of titration only; the diagnosis and follow-up assessment are the sleep physician’s role.32,33
Studies’ recommendations for multidisciplinary approach:
The final diagnosis of SDB or OSA should be made by a physician or sleep physician.4,11,15,22,24,25,27,32,33,35
The evaluation of OA treatment efficacy should be done by the sleep physician with sleep testing.4,11,32,33
The dentist must collaborate with the surgeon in case of maxillofacial surgery.20
Two orthodontic treatments in children may change airway dimension: rapid maxillary expansion in patients with a constricted maxilla and mandibular advancement for class II malocclusion correction; however, the orthodontic treatment in children in whom OSA is diagnosed should be planned based on the same principles for correction of dental and skeletal malocclusion.33
The management of OSA in children is different from that in adults, with tonsillectomy and adenoidectomy usually considered the first-line treatment.33
Additional findings within studies about SDB:
The grade of severity of OSA is classified as mild (5-14 AHI); moderate (15-30 AHI), and severe (+30 AHI).20 However, for children the threshold is lower: mild (1-5 AHI), moderate (5-10 AHI), and severe (+10 AHI).9,23,33,34
Usually, the reduction in the AHI, respiratory disturbance index, and respiratory event index must be less than 5 and greater than 50% reduction in these indexes to be classified as successful.21
Snoring patients without features of OSA should undergo treatment to reduce snoring to a subjective reasonable level.23
Age 12 years is the cutoff point for childhood SDB.9
DISCUSSION
A definition given by the AADSM in 2008 states that the dentists’ role in dental sleep medicine “focuses on the management of sleep-related breathing disorders (SDB), which includes snoring and obstructive sleep apnea (OSA), with oral appliance therapy (OAT) and upper airway surgery.”37 With a broader definition, Lobbezoo et al.38 proposed that “Dental Sleep Medicine is the discipline concerned with the study of the oral and maxillofacial causes and consequences of sleep-related problems.” From this perspective, the role of dentists would go farther, including the management of orofacial pain, oral moistening disorders (including oral dryness and hypersalivation), gastroesophageal reflux disorder, SDB (including snoring and OSA), and mandibular movement disorders (including dyskinesia, dystonia, and sleep bruxism). According to the studies included in this systematic review, screening SDB, OA treatment, and follow-up are the major roles for dentists working in dental sleep medicine.
Screening for SDB
Dentists have an important role in the early screening of patients with SDB/OSA because the dentist usually has regular contact with patients.29,30,33 The anatomic determinant factors attributed to the development of SDB/OSA are micrognathia, retrognathia, macroglossia, adenotonsillar hypertrophy, and nasal septum deviation.20 Additionally, some genetic confounders can also be related to SDB/OSA such as jaw position, tonsillar tissue, and tongue size that may affect the size of the pharyngeal airway.6 Therefore, indications of the presence of SDB/OSA might be evident in the oral cavity such as high-arched or narrow hard palate and retrognathia.2,8 With that being said, the dentist has a responsibility for the evaluation of the determinant factors attributed to the development of SDB/OSA previously described. Moreover, dentists have radiographic examinations that might help to evaluate the upper airway, such as cephalometric tomography and cone-beam computed tomography.20 According to the Guide for Radiation Health and Safety Program of the Alberta Dental Association and College, dentists should review and provide a report about the entire data volume generated by cone-beam computed tomography.39 However, the cephalometric images do not define mediolateral information in the oropharyngeal airway and may lead to inaccurate information regarding volume and minimal cross-sectional area.33 According to the AAO, orthodontists also should assess the patient’s height, weight, and neck size to screen for SDB/OSA.33 An important screening tool is the questionnaire; AAO recommends the use of the STOP-Bang questionnaire, which is a validated tool for OSA risk assessment in adults, and the Pediatric Sleep Questionnaire or the Epworth Sleepiness Scale in children.33 The STOP-Bang questionnaire includes questions on snoring, tiredness, observed pauses in breathing, high blood pressure, and body mass index (BMI). A BMI higher than 35 kg/m2, age older than 50 years, neck circumference of 17 inches or larger in males and 16 inches or larger in females, and male sex are confounders for the development of SDB/OSA.33 The scores in this questionnaire gives the predisposition for OSA: for 2 or fewer “yes” answers, indicative of low risk for OSA; for 3 to 4 “yes” answers, indicative of moderate risk for OSA; for more than 5 “yes” answers, suggestive high risk for OSA.33 The Modified Mallampati Classification for patency of oral airway can be done by the orthodontists and would be helpful to evaluate patients at risk for upper airway obstruction during sleep.33 The Brodsky tonsil classification grades the tonsil hypertrophy when analyzing the oropharyngeal airway space taken up by the two tonsils; the Friedman Tonsil Grading System gives information on the size of the tonsil.33 Caution should be taken when using the tonsils’ size evaluation because they do not give a correlation to OSA severity; an otolaryngologist will best evaluate and correlate the size of the tonsils to clinical symptoms.33 In addition, according to the International Classification of Sleep Disorders, there are some sleep breathing-related symptoms classified as borderline abnormal/normal sleep such as snoring.40 Yet snoring can also be related to OSA,28 and dentists have a duty to manage OSA.21,26,31 Developing a model where the dentist, the family physician, and the sleep physician are in the loop to take care of patients, each one playing a particular role involved in the care of SDB/OSA: screening for the dentist, diagnosis for the sleep physician, and global health (hypertension, obesity, following up) for the family physician, would improve the quality of care for the patient.14
Diagnosis
There is consensus among the studies that the final diagnosis of OSA should be done by a physician or a sleep physician.4,11,14 Masse pointed out an important concern that the comorbidities associated with OSA such as hypertension are not within the scope of a dentist’s care.14
Treatment
The main role of dentists when treating SDB/OSA patients is to evaluate, apply, and follow up OA use with the intention to increase respiratory capacity and decrease AHI episodes.21,23 The OA is used in patients with SDB/OSA and snoring with the aim to protrude the mandible, enlarging the pharynx.8 The mandibular protrusion allows greater breathing capacity, reducing the frequency and intensity of snoring, leading to an improvement in the quality of sleep and, consequently, in the quality of life.21 There are several types of OA available on the market; however, a study on the diagnosis and treatment of SDB/OSA in adults discouraged the use of premolded OA in which the use of warm water is required in order to fit the appliance in the patient’s mouth.41 A similar statement is suggested by several guidelines in which it is claimed that the customized OA is more effective than the premanufactured one.20, 21 Therefore, only custom-made, titratable OAs should be applied. 4,11,21,24,32 Furthermore, there are some contraindications for the use of OA that only the dentist has the knowledge to manage: insufficient teeth to support the device, periodontal problems inducing tooth mobility, active temporomandibular joint disorder, and limited maximum protrusive distance (6 mm).42,43 Cephalometric, tomographic, and videoendoscopic studies have revealed an increase in the velopharyngeal, nasopharyngeal, and anteroposterior dimension of the upper airway when using OA.44–46 With that in mind, the oral appliances for maxillary expansion and mandibular advancement treatments in cases of constricted maxilla or class II malocclusion might be beneficial for children and adolescents in whom SDB has been diagnosed; however, the primary goal in those cases remains correction of malocclusion.33 Upper airway dimensional changes and breathing capacity have been analyzed and several studies reported that those appliances effectively increase the upper airway and decrease AHI; however, randomized controlled trials are needed to ascertain in which children these forms of treatment will be of benefit for SDB.47 OAs have to be managed by a qualified dentist because technical skills and knowledge are required to reach a favorable outcome. 4,15,21–23,25–28,32,33,34 According to the AADSM, the dentist working with sleep apnea should have received specialized training with a duration of at least 25 hours.4 Despite the fact that the dentist is the only healthcare professional able to perform OA management, in cases of SDB/OSA, the sleep physician should indicate the therapy with OA and then the dentist will evaluate and confirm the indication to apply the therapy.
Follow-up
Nonetheless, it is of utmost importance that the dentist controls the management of the OA to minimize side effects such as occlusal interferences, pain in the masticatory muscles, temporomandibular joint pain, and discomfort with hypersalivation.21 The patients should be referred back to the sleep physician for the confirmation of OA therapy efficacy.4 The multidisciplinary teamwork is the key to success in the treatment for patients with SDB/OSA where the dentist following up on the OA, the family physician following up on global health, and the sleep physician following up on OSA/SDB treatment would lead to a favorable outcome.
Position Statements of Dental and Medical Associations
Overall, the position statements or guidelines of the various dental or medical associations agree that the dentist’s role in SDB is related to the screening for potential SDB/OSA9,13,20,22,24,27–31 and to refer to the sleep physicians when SDB or OSA is suspected11,15,24,27,29,31,32; only qualified dentists should manage SDB/ OSA and snoring therapies4,15,21–23,25–28,32; OAs are indicated for patients with mild to moderate OSA who prefer OA to CPAP therapy or who do not respond to CPAP or have contraindications for the use of CPAP11,13,15,22–26,27,29; when OA is prescribed, the qualified dentist should preferably use custom, titratable appliances over noncustom oral devices4,11,21,24,32; the dentists should provide follow-up of OA therapy to evaluate possible dental-related side effects such as occlusal changes11,15,22,24,26,32; and the final diagnosis of SBD/OSA should be done by the sleep physician4,11,15,22,24,25,27,32; however, a multidisciplinary teamwork is essential for a better outcome. 4,24,25
LIMITATIONS
Only AADSM has defined the skills necessary for a qualified dentist; other groups should develop their own definitions of the competencies for a qualified dentist.
A well-defined and established model of teamwork involving patient, dentist, family physician, and sleep physician should be developed and challenged by studies.
FUTURE CONSIDERATION
Better and further studies are needed on the role of dentists and effectiveness of maxillary expansion and mandibular advancement appliances in patients with OSA.41 The multidisciplinary approach for treating OSA is of great importance for better results, a model should be developed where dentist (screening and treatment), family physician (medical history and follow-up), and sleep physician (diagnosis of OSA) should be in a loop to give to the patients the best treatment against OSA. Dental and medical students should learn about dental sleep medicine.41 It is particularly relevant to improve and to align the curriculum guidelines for dental sleep medicine.
CONCLUSION
Through this systematic review, it is possible to conclude that in general, the guidelines describe the role of the dentist in SDB/OSA as:- All dentists can prescreen patients through a clinical examination, patient history, and questionnaires to reduce undiagnosed SDB/OSA;
- Refer patients to the physician or sleep physician;
- A qualified dentist can apply, manage and follow up OA.
Additionally, OA therapy is an effective first-line treatment for patients suffering from primary snoring and in whom mild to moderate OSA has been diagnosed. OA therapy is a treatment option for patients with severe OSA who are, for whatever reason, unable to adhere to CPAP therapy. Dentists should screen for SDB/OSA; however, only dentists with good knowledge of dental sleep medicine or dentists who regularly update their knowledge and training in dental sleep medicine should be part of the multidisciplinary team to treat patients with SDB/OSA. It is important to know that there are more causes that affect sleep other than SDB that the dentist should be aware of.
ABBREVIATIONS
SDB: sleep-disordered breathing
OSA: obstructive sleep apnea
OA: oral appliance
MAD: mandibular advancement device
AHI: apnea-hypopnea index
CPAP: continuous positive airway pressure
AAO: American Association of Orthodontics
AADSM: American Academy of Dental Sleep Medicine
AASM: American Academy of Sleep Medicine (AASM)
RDI: respiratory disturbance index
REI: respiratory event index
REFERENCES
- Gianoni-Capenakas S, Gomes AC, Mayoral P, Miguez M, Lagravere M. Sleep-disordered breathing: A systematic review on the dentists’ role. J Dent Sleep Med. 2019; 6(3).
- Vuorjoki-Ranta TR, Lobbezoo F, Vehkalahti M, Tuomilehto H, Ahlberg J. Treatment of obstructive sleep apnoea patients in community dental care: knowledge and attitudes among general dental practitioners and specialist dentists. J Oral Rehabil. 2016;43(12):937-942. doi:10.1111/joor.12441
- Heinzer R, Vat S, Marques-Vidal P, et al. Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study. Lancet Respir Med. 2015;3:310-328. doi:10.1016/S2213-2600(15)00043-0
- Addy N, Bennett K, Blanton A, et al. Policy Statement on a Dentist’s Role in Treating Sleep-Related Breathing Disorders. J Dent Sleep Med. 2018;05(01):25-26. doi:10.15331/jdsm.6920
- AAPD Guideline. Policy on Obstructive Sleep Apnea. The Reference Manual of Pediatric Dentistry. 2016, 110-112. https://www.aapd.org/globalassets/media/policies_guidelines/p_sleepapnea.pdf. Accessed January 14, 2019.
- White DP. Sleep-related breathing disorder.2. Pathophysiology of obstructive sleep apnoea. Thorax. 1995;50(7):797-804. doi:10.1136/thx.50.7.797
- Guilleminault C, Huang YS. From oral facial dysfunction to dysmorphism and the onset of pediatric OSA. Sleep Med Rev. 2018;40:203-214. doi:10.1016/j.smrv.2017.06.008
- Stuck BA, Dreher A, Heiser C, et al. S2k-Leitlinie “Diagnostik und Therapie des Schnarchens des Erwachsenen”: Vorgelegt von der Arbeitsgemeinschaft Schlafmedizin der Deutschen Gesellschaft für Hals-Nasen-Ohren-Heilkunde, Kopf- und Hals-Chirurgie e. V. HNO. 2013;61(11):944-957. doi:10.1007/s00106-013-2775-3
- Leibovitz S, Haviv Y, Sharav Y, Almoznino G, Aframian D, Zilberman U. Pediatric sleep-disordered breathing: Role of the dentist. Quintessence Int (Berl). 2017;48(8):639-645. doi:10.3290/j.qi.a38554
- Perlis M L, Lichstein K. Treating Sleep Disorders - Principles and Practice of Behavioral Sleep Medicine. Publisher Wiley, 1st Edition. 2003.
- The Role of Dentistry in the Treatment of Sleep Related Breathing Disorders. https://www.ada.org/en/~/media/ADA/Member Center/FIles/The-Role-of-Dentistry-in-Sleep-Related-Breathing-Disorders. Accessed January 14, 2019.
- Huang Y-S, Guilleminault C. Pediatric Obstructive Sleep Apnea: Where Do We Stand? Adv Otorhinolaryngol. 2017;80:136-144. doi:10.1159/000470885
- Levrini L. Italian recommendations on dental support in the treatment of adult obstructive sleep apnea syndrome (OSAS). Ann Stomatol (Roma). 2015:81-86. doi:10.11138/ads/2015.6.3.081
- Masse J-F. On the role of dentists in the diagnosis and treatment of obstructive sleep apnea:controversy and Controversy. J Dent Sleep Med. 2018;5(2):29–30.
- Wu J, Dubois N. Role of Oral Devices in Managing Sleep-Disordered Breathing Patients. 2016. https://www.prosthodontics.org/assets/1/7/16.Role_of_Oral_Devices_in_Managing_Sleep-disordered_Breathing_Patients.pdf. Accessed January 14, 2019.
- Pirelli P, Saponara M, Guilleminault C. Rapid maxillary expansion in children with obstructive sleep apnea syndrome. Sleep. 2004;27(4):761-766.
- Mordente CM, Palomo JM, Horta MCR, Souki BQ, Oliveira DD, Andrade IJ. Upper airway assessment using four different maxillary expanders in cleft patients: A cone-beam computed tomography study. Angle Orthod. 2016;86(4):617-624. doi:10.2319/032015-174.1
- Villa MP, Rizzoli A, Miano S, Malagola C. Efficacy of rapid maxillary expansion in children with obstructive sleep apnea syndrome: 36 months of follow-up. Sleep Breath. 2011;15(2):179-184. doi:10.1007/s11325-011-0505-1
- Moher D et al. Preferred Reporting Items for Systematic review and Meta-Analysis Protocols: The PRISMA Statement. PLoS Med. 2009;6(6):e-10.
- Ranieri S, Lagana G, Lombardo EC, Cozza P. Le problematiche respiratorie nel sonno en eta adulta: il ruolo dell’ortodentista. Rassegna Ortognatodonzia. 2018;86(6):501-514. Doi: 10.19256/d.cadmos.06.2018.06
- Ramar K, Dort LC, Katz SG, et al. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015. J Clin Sleep Med. 2015;11(7):773-827. doi:10.5664/jcsm.4858
- Epstein L, Kristo D, Strollo P, Friedman N. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(3):263-276. http://jcsm.aasm.org/Articles/05_03_263_1.pdf. Accessed December 10, 2018.
- Kushida CA, Morgenthaler TI, Littner MR, et al. Practice parameters for the treatment of snoring and Obstructive Sleep Apnea with oral appliances: an update for 2005. Sleep. 2006;29(2):240-243. http://www.ncbi.nlm.nih.gov/pubmed/16494092. Accessed September 16, 2018.
- Quan SF, Schmidt-Nowara W. The role of dentists in the diagnosis and treatment of obstructive sleep apnea: Consensus and controversy. J Clin Sleep Med. 2017;13(10):1117-1119. doi:10.5664/jcsm.6748
- Schwarting S, Huebers U, Heise M, Schlieper J, Hauschild A. Position paper on the use of mandibular advancement devices in adults with sleep-related breathing disorders: A position paper of the German Society of Dental Sleep Medicine (Deutsche Gesellschaft Zahnaerztliche Schlafmedizin, DGZS). Sleep Breath. 2007;11(2):125-126. doi:10.1007/s11325-007-0116-z
- Spencer J, Patel M, Mehta N, et al. Special consideration regarding the assessment and management of patients being treated with mandibular advancement oral appliance therapy for snoring and obstructive sleep apnea. Cranio. 2013;31(1):10-13. doi:10.1179/crn.2013.002
- Gauthier L, Almeida F, Arcache PMP, et al. Position Paper by Canadian Dental Sleep Medicine Professionals Regarding the Role of Different Health Care Professionals in Managing Obstructive Sleep Apnea and Snoring with Oral Appliances. Can Respr J. 2012; 19(5):307-309.
- Stuck BA, Dreher A, Heiser C, et al. Diagnosis and treatment of snoring in adults–S2k Guideline of the German Society of Otorhinolaryngology, Head and Neck Surgery. Sleep Breath. 2015;19(1):135-148. doi:10.1007/s11325-014-0979-8
- Stradling J, Dookun R. Snoring and the role of the GDP: British Society of Dental Sleep Medicine (BSDSM) pre-treatment screening protocol. Br Dent J. 2009;206(6):307-312. doi:10.1038/sj.bdj.2009.214
- Masoud AI, Jackson GW, Carley DW. Sleep and airway assessment: A review for dentists. Cranio. 2017;35(4):206-222. doi:10.1080/08869634.2016.1228440
- Ngiam J, Balasubramaniam R, Darendeliler MA, Cheng AT, Waters K, Sullivan CE. Clinical guidelines for oral appliance therapy in the treatment of snoring and obstructive sleep apnoea. Aust Dent J. 2013;58(4):408-419. doi:10.1111/adj.12111
- Almeida FR, Lowe AA Gauthier L. The Role of Dentists in the Treatment of Snoring and Obstructive Sleep Apnea with Oral Appliances. Standards and Guidelines. College of Dental Surgeons of BC, British Columbia, Canada. 2014. https://www.cdsbc.org/CDSBCPublicLibrary/Obstructive-Sleep-Apnea.pdf
- Behrents RG, Shelgikar AV, Conley RS, Flores-Mir C, Hans M et al. White Paper: Obstructive Sleep Apnea and Orthodontics.; American Association of Orthodontics Task Force. 2019. www.aaoinfo.org.
- Levine M, Bennett KM, Cantwell MK, Postol K, Schwartz DB. Dental Sleep Medicine Standards for Screening, Treating and Managing Adults with Sleep-Related Breathing Disorders Standards of Practice Committee of the American Academy of Dental Sleep Medicine. J Dent Sleep Med. 2018;5(3). doi:10.15331/jdsm.XXXX
- Lavigne GJ, Goulet J, Zuconni M, Morisson F. Sleep disorders and the dental patient. Oral Surg Oral Med Oral Pathol. 1999;88(3):2-6.
- Schmidt-Nowara W. A review of sleep disorders. The history and diagnosis of sleep disorders related to the dentist. Dent Clin North Am. 2001;45(4):631-642. http://www.ncbi.nlm.nih.gov/pubmed/11699233. Accessed December 10, 2018.
- Lavigne J, Cistulli P, Smith M. Sleep Medicine for Dentists: A Practical Overview. Quintessesce Publishing Co. 1st edition, 2009. http://quintessenz.de/PR/Lavigne_17681.pdf. Accessed November 21, 2018.
- Lobbezoo F, Aarab G, Wetselaar P, Hoekema A, de Lange J, de Vries N. A new definition of dental sleep medicine. J Oral Rehabil. 2016;43(10):786-790. doi:10.1111/joor.12421
- Alberta Dental Association and College. Guide for Radiation Health and Safety Program. 2015. https://www.dentalhealthalberta.ca/wp-content/uploads/2019/09/Guide-for-the-Radiation-Health-and-Safety-Program.pdf
- Sateia MJ. International Classification of Sleep Disorders-Third Edition: highlights and modifications. Chest. 2014;146(5):1387-1394. doi:10.1378/chest.14-0970
- Remmelink HJ, Hoeke A. [Dutch national guidelines for diagnosis and treatment of obstructive sleep apnea syndrome in adults]. Ned Tijdschr Tandheelkd. 2010;117(4):227-231. http://www.ncbi.nlm.nih.gov/pubmed/20446552. Accessed November 19, 2018.
- Clark GT. Mandibular advancement devices and seep disordered breathing. Sleep Med Rev. 1998;2(3):163-174. doi:10.1016/S1087-0792(98)90019-3
- Petit F-X, Pépin J-L, Bettega G, Sadek H, Raphaël B, Lévy P. Mandibular advancement devices: rate of contraindications in 100 consecutive obstructive sleep apnea patients. Am J Respir Crit Care Med. 2002;166(3):274-278. doi:10.1164/rccm.2008167
- Ryan CF, Love LL, Peat D, Fleetham JA, Lowe AA. Mandibular advancement oral appliance therapy for obstructive sleep apnoea: effect on awake calibre of the velopharynx. Thorax. 1999;54(11):972-977. http://www.ncbi.nlm.nih.gov/pubmed/10525554. Accessed November 20, 2018.
- Tsuiki S, Hiyama S, Ono T, et al. Effects of a titratable oral appliance on supine airway size in awake non-apneic individuals. Sleep. 2001;24(5):554-560. http://www.ncbi.nlm.nih.gov/pubmed/11480653. Accessed November 20, 2018.
- Cozza P, Ballanti F, Castellano M, Fanucci E. Role of computed tomography in the evaluation of orthodontic treatment in adult patients with obstructive sleep apnea syndrome (OSA). Prog Orthod. 2008;9(1):6-16. http://www.ncbi.nlm.nih.gov/pubmed/19294236. Accessed November 20, 2018.
- Caprioglio A, Meneghel M, Fastuca R, Zecca PA, Nucera R, Nosetti L. Rapid maxillary expansion in growing patients: Correspondence between 3-dimensional airway changes and polysomnography. Int J Pediatr Otorhinolaryngol. 2014;78(1):23-27. doi:10.1016/j.ijporl.2013.10.011
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication April 10, 2019
Submitted in final revised form July 2, 2019
Accepted for publication July 8, 2019
Address correspondence to: Silvia Gianoni-Capenakas, DDS, MSc, PhD, Student Faculty of Medicine and Dentistry, University of Alberta - Edmonton, Alberta, Canada, 11405 87 Ave 5th floor, T6G 2R3; Email: capenaka@ualberta.ca
DISCLOSURE STATEMENT
APPENDIX
Databases and individualized truncations of words. |
{kind=link}