Original Article 1, Issue 4.2
A Descriptive Report of Combination Therapy (Custom Face Mask for CPAP Integrated With a Mandibular Advancement Splint) for Long-Term Treatment of OSA With Literature Review
http://dx.doi.org/10.15331/jdsm.6522
Ronald S. Prehn, DDS, Diplomate, ABDSM1 ; Todd Swick, MD2
1University of Texas School of Dentistry, Houston, Texas; 2University of Texas School of Medicine, Houston, Texas
ABSTRACT
Study Objectives:
This is a descriptive retrospective study about the efficacy of combination therapy using the TAP-PAP custom face mask (CFM) interface, with a literature review of combination therapy. The purpose of this study is to determine which group of failed obstructive sleep apnea (OSA) therapies would benefit from combination therapy with the CFM. The three failed therapies are mandibular advancement splint (MAS) monotherapy, continuous positive airway pressure (CPAP) monotherapy, and TAP-PAP CS (nasal pillows) combination therapy. Clinically, this will assist the clinician to understand the benefit of the CFM when the patient’s current therapy fails.
Methods:
There was a retrospective chart review of patients on combination therapy from 2006–2012. The 75 patients who underwent combination therapy with the CFM were categorized into the three failed groups. OSA severity was compared between groups. CPAP and compliance were compared before and after CFM use. A 6-year follow-up was conducted.
Results:
A total of 220 charts of patients undergoing combination therapy were reviewed; 75 patients were in combination therapy with a CFM. The populations of the three groups were as follows: MAS monotherapy failed in 11 (11%), TAP-PAP CS failed in 21 (27%), and CPAP failed in 43 (57%) before the CFM was used. These patients had severe OSA with mean CPAP 14 cm H2O. At 6-year followup, a 78% compliance rate and average CPAP of 13 cm H2O were reported.
Conclusions:
This study suggests that patients in whom CPAP monotherapy failed would benefit the most from the CFM. The application of the CFM is for patients with more severe OSA and is well tolerated with improved compliance. The CFM should be considered when other therapeutic methods of treating OSA have failed or when CPAP or the CPAP mask are intolerable to the patient.
Keywords:
combination therapy, CPAP, custom face mask, MAS, TAP-PAP
Citation:
Prehn RS, Swick T. A descriptive report of combination therapy (custom face mask for CPAP integrated with a mandibular advancement splint) for long-term treatment of OSA with literature review. Journal of Dental Sleep Medicine. 2017;4(2):29–36.
INTRODUCTION
Obstructive sleep apnea (OSA) is a common sleep disorder manifested by repetitive closure or partial closure of the upper airway causing hypoxemia, hypercapnia, and increased sympathetic activity resulting in sleep fragmentation. The natural history of untreated OSA has been well described, including but not limited to daytime sleepiness, hypertension, cognitive impairment, metabolic syndrome, and obesity. In patients who are symptomatic (presence of excessive daytime sleepiness, cognitive dysfunction, mood disorders, insomnia, hypertension, ischemic heart disease, or cerebrovascular accident) the diagnosis is established if there are five or more sleepdisordered respiratory events/h of sleep (apneas, hypopneas, or respiratory effort related arousals). If the patient does not exhibit the previously noted symptoms, the presence of 15 or more events/h is sufficient to make the diagnosis.1 The severity of OSA varies from mild to severe based on a combination of clinical and polysomnographic determinants.
Oral appliance therapy, specifically mandibular advancement splint (MAS) monotherapy and continuous positive airway pressure (CPAP), are indicated for the treatment of mild to moderate OSA.2 Oral appliance therapy and CPAP are equally effective for mild to moderate OSA,3 however for patients with severe OSA, the use of MAS monotherapy is generally not recommended; instead, CPAP is typically the preferred method of treatment because of its effectiveness for treating severe OSA.4 It is generally thought that as the number of apneas/hypopneas increase, the pressure required to maintain upper airway patency also typically increases. As the pressure increases, so do the challenges of CPAP acceptance and/or compliance. With increased pressure, there is increased mask leakage, air leakage out of the mouth, and patient discomfort.5 Standard off-the-shelf noncustom masks often are not effective in these severe cases.
Combining CPAP therapy and oral appliance therapy with MAS monotherapy has been shown to be a tolerable and effective therapeutic option. With combination therapy, many of the challenges of CPAP intolerance can be overcome, resulting in improved therapeutic outcomes. Combination therapy utilizes a standard CPAP machine to deliver positive air pressure through a standard nasal and/or oronasal interface in conjunction with MAS monotherapy.6,7
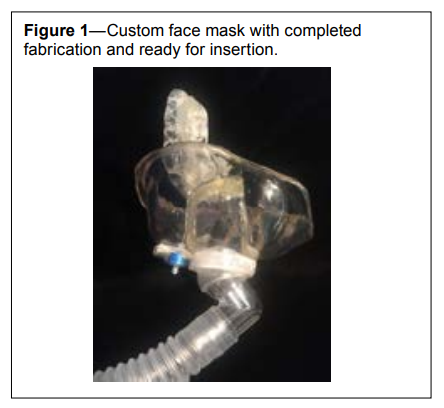
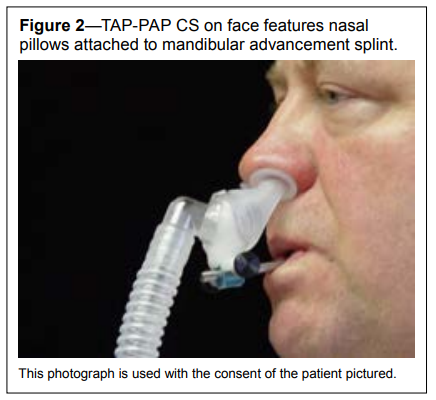
Combination therapy is categorized into two types. Type 1 is CPAP therapy used with MAS monotherapy. There is no integration of the two therapies other than both are applied to the patient at the same time. Type 2 involves connecting the CPAP device directly to the MAS. The TAP-PAP CS (nasal pillows) is one application of type 2 combination therapy (Figure 1); and the TAP-PAP CM (custom face mask, CFM) is another application of type 2 combination therapy (Figure 2).
Figure 1Custom face mask with completed fabrication and ready for insertion. |
{kind=link}
Figure 2TAP-PAP CS on face features nasal pillows attached to mandibular advancement splint. |
{kind=link}
The CFM for combination therapy was developed by W. Keith Thornton, DDS in 1993.8 Since then, there have been limited reports (case reports and small proof-of-concept studies) that have utilized combination therapy for the treatment of OSA.
As an interesting historical side note, the CFM for combination therapy was developed by a dentist in response to a critical need of postpolio patients. In 1993, Sue Sorter, a respiratory therapist, under the direction of Dr. Joseph Viraslav of the Dallas Rehabilitation Institute, was using a modification of a mask developed in Lyon, France called the “Lyon mask” on postpolio patients with severe OSA. She constructed an oral appliance along with an acrylic mask for her patient. She then used an acrylic post to attach the separate components together (personal communication, Dr. Keith Thornton, January 14, 2011). Dr. Thornton perfected this idea with a custom oral device from dental impressions, and a CFM from an impression of the face, connected by a stainless steel post.
In 2002 Dr. Thornton reported the successful use of combination therapy in a patient who was intolerant of auto-set positive airway pressure (APAP).9
In 2015, Upadhyay et al.10 reported on the use of a custommade mandibular advancement device with concomitant use of APAP (the devices were separate without structural integration) in a patient who could not tolerate CPAP at 12.7 cm H2O and was deemed to be “unfit” for palatal surgery. The initial use of MAS monotherapy elicited complaints of excessive salivation and jaw pain, which were temporary. The APAP was applied and on day 1 of combined treatment the pressure was reduced to 8.5 cm H2O and at day 90 it was 6.5 cm H2O.10
In 2011 El-Solh et al.7 performed a multipatient study that assessed the efficacy and tolerability of using a custom-made MAS in combination with a standard positive airway pressure (APAP) system compared to CPAP alone. Of note was that the MAS lacked mechanical integration of the intraoral device with the nasal mask. The MAS device was fabricated using the Herbst attachment to bring the mandible to at least 65% of the patient’s maximal protrusion in combination with a standard nasal CPAP mask. After 3 days of treatment the combination approach allowed for a significant reduction in the pressure necessary to maintain upper airway patency as well as reduction of residual apnea-hypopnea index (AHI). CPAP pressures were reduced from 9.4 ± 2.3 cm H2O to 7.3 ± 1.4 cm H2O, and residual AHI was reduced from 11.2 ± 3.9 to 3.4 ± 1.5 respiratory events/h of sleep.7
In another study that assessed patient comfort, compliance, and preference between standard CPAP and “hybrid therapy,” de Vries et al.11 chose seven patients with moderate to severe OSA who tolerated their “high” CPAP pressures (> 10 cm H2O) who were then fitted with the TAP 3 type MAS with an integrated set of nasal pillows. The mandible was set at 70% of the patient’s maximum protrusion and CPAP was set at 6 cm H2O. If OSA symptoms persisted or worsened the pressure was increased. Patients filled out questionnaires at baseline (CPAP treatment alone) assessing comfort, compliance, and satisfaction with treatment and again after 3 months of treatment with the hybrid system. After 3 months a polysomnographic study was performed. Four of seven patients reported hybrid therapy to be more comfortable and effective and preferred it over conventional CPAP. There were no differences between baseline (conventional CPAP) and follow-up (hybrid therapy) scores in compliance, satisfaction, daytime sleepiness, and quality of life. Effectiveness of hybrid therapy was good as AHI significantly decreased from median AHI at diagnosis (64.6 events/h; range, 31.0–81.0) to median AHI with hybrid therapy (1.5 events/h). There was no statistical difference in effectiveness between conventional CPAP and hybrid therapy (median AHI with conventional CPAP was 2.4 events/h. It was concluded that although pressure could be lowered, hybrid therapy was perceived as a comfortable alternative to conventional CPAP. There were no differences between both therapies regarding compliance, satisfaction, and effectiveness.11
The purpose of this study was to review and summarize the characteristics of patients who had undergone combination therapy with a MAS secured to a CFM. Failure of three common therapeutic options, MAS monotherapy, CPAP monotherapy, and TAP-PAP CS (nasal pillows) combination therapy, were considered for this study. The application of the results of this study in a clinical setting would help the clinician to understand the benefit of the CFM when the patient’s current therapy fails. The decision to move into type 2 combination therapy with the CFM will depend on which current therapy is failing. This study will help clarify that decision process for the clinician. This study will also determine the efficacy and tolerability of type 2 combination therapy with the CFM as a therapeutic option in patients with all degrees of OSA who presented to a dental sleep center.
METHODS
A retrospective chart review (evaluation of quality of care) of all the combination therapy patients was conducted to determine who had underwent CFM treatment and what therapies had been attempted prior to the CFM. All patients who had been provided combination therapy from 2008 to 2012 at the Center for Facial Pain and Dental Sleep Medicine in The Woodlands, Texas were included in the review.
The CFM (Figure 1) fabrication process has been well described.12 It should be noted that every patient fitted with a CFM underwent an in-laboratory titration to determine the therapeutic pressure for the CPAP aspect of the therapy.
Patient Selection
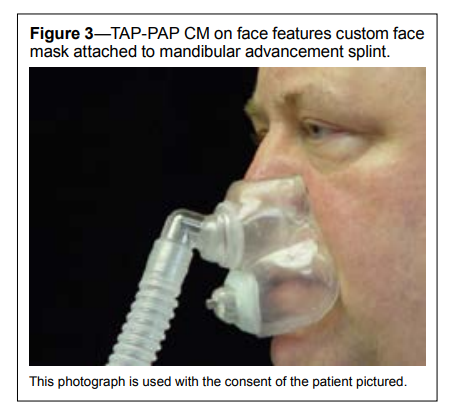
CPAP monotherapy and MAS monotherapy typically failed in patients in this study before they were considered for combination therapy. All patients underwent a diagnostic nocturnal polysomnogram and all underwent a CPAP titration study prior to institution of combination therapy. The dental sleep center used two types of combination therapy; both utilize the basic TAP3 MAS (Airway Management, Inc., Dallas, Texas). The first type 2 device is the TAP-PAP CS (chair side TAP3 with post and nasal pillows) (Figure 2). The second type 2 device is the TAP-PAP CM (TAP3 with post and CFM) (Figure 3).
Figure 3TAP-PAP CM on face features custom face mask attached to mandibular advancement splint. |
{kind=link}
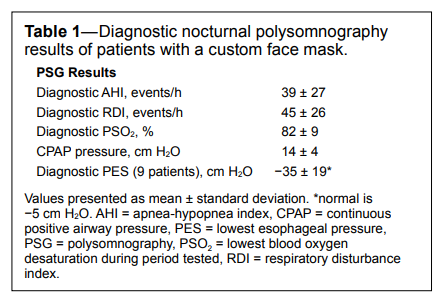
Table 1Diagnostic nocturnal polysomnography results of patients with a custom face mask. |
{kind=link}
Two hundred twenty consecutive charts of patients who underwent type 2 combination therapy were analyzed for this study. Of these 220 patients, 145 were excluded because they had a successful outcome utilizing the TAP-PAP CS (nasal pillows) device. This left 75 patients who were prescribed the TAP-PAP CM (CFM).
Patients who were included in this study were those for whom a sequence of previous treatments failed. There were three groups comprising failed therapy. Group 1 included those for whom MAS monotherapy failed; group 2 included those for whom combination therapy with the MAS attached to nasal pillows (TAP-PAP CS) failed; and group 3 included those for whom CPAP monotherapy failed. Charts were reviewed and patients were placed into one of these three groups based on the type of failed therapy used before the CFM was used. Original diagnostic nocturnal polysomnography and CPAP titration results were recorded. Many patients had undergone esophageal pressure monitoring (PES studies) as part of their nocturnal polysomnography; as a result, those pressures were recorded as well.
RESULTS
The charts of the 75 patients who were prescribed the TAP-PAP CM (CFM) were surveyed and the type of previously failed therapies were determined. The nocturnal polysomnography results of the 75 CFM patients were determined along with the results of the previous CPAP titration studies that were accomplished with a stock non-custom CPAP mask (Table 1).The level of severity of this group (Table 1) reflects the type of patient who would benefit from combination therapy with the CFM. These patients represent individuals on the moderate to severe end of the spectrum of OSA.
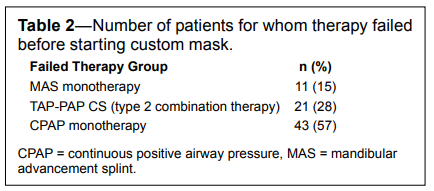
These patients were then grouped into three categories: the first group involved failed MAS monotherapy; the second, failed combination therapy with the TAP-PAP CS (nasal pillows), and the third, failed CPAP monotherapy (Table 2).
Table 2Number of patients for whom therapy failed before starting custom mask. |
{kind=link}
Previous MAS Monotherapy Failures
In 15% of patients using a CFM, MAS monotherapy failed (Table 2). The most frequent reason for MAS monotherapy failure was the inability to tolerate advancement of the mandible. These patients all had a history of recent temporomandibular joint (TMJ) therapy and the forward movement of the mandible resulted in pain. The most cited reason for the desire to discontinue MAS monotherapy in this group was continued daytime fatigue. Because CPAP in many of these patients had previously failed, they were willing to abandon all types of therapy at this point. However, when presented with the description of combination therapy, they were willing to try the CFM. The acceptance rate of this group of patients for combination therapy was 98%. There was one patient who could not tolerate the CPAP even with the CFM.Previous TAP-PAP CS (Nasal Pillow) Failures
In 28% of patients, type 2 combination therapy using the TAP-PAP CS failed (Table 2). The TAP-PAP CS device utilizes the MAS as its foundation with a blue swivel nut secured to the post to allow direct integration of the nasal pillows into the MAS (Figure 1). The main reason given for failure of this therapy was discomfort due to the flow of air directly into the nares; this in turn led to mouth leakage and fluttering of the cheeks. The net result, as in the MAS monotherapy failure group, was persistent daytime fatigue. There were also some mouth breathers in this group. These patients required a CFM in order to seal the mouth.Previous CPAP Monotherapy Failures
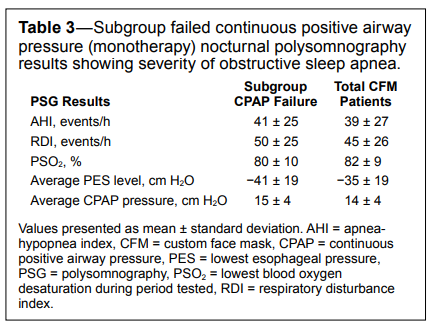
In 57% of patients undergoing combination therapy with the CFM, CPAP monotherapy failed (Table 2). The reason for failure of CPAP was mask and/or headgear discomfort. Leakage around the mask was also cited as an unacceptable side effect. These patients were willing to abandon therapy despite the severity of their OSA. Although the nocturnal polysomnography results for all groups have been outlined (Table 1), a subgroup analysis was determined to understand the severity of this CPAP monotherapy failure group, when compared to the entire CFM group (Table 3). The largest group of CFM patients experienced CPAP monotherapy failure (57%, 95% confidence interval: 46% to 69%).
Table 3Subgroup failed continuous positive airway pressure (monotherapy) nocturnal polysomnography results showing severity of obstructive sleep apnea. |
{kind=link}
The severity of OSA in the subgroup of CPAP monotherapy failure reflects a group of patients on the more severe end of the spectrum of OSA (Table 3). For each indicator of severity, the patients for whom CPAP monotherapy failed had more severe OSA than the average of the entire group.
Follow-Up Survey
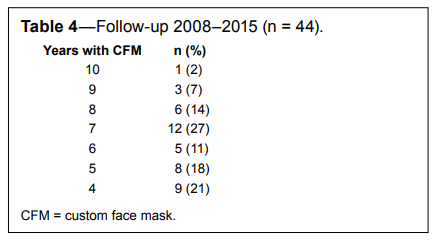
All patients included in this follow-up survey (seen in the Dental Sleep Clinic from 2006–2012) were followed up with a phone call in June 2015 to determine if they were still wearing the CFM (Table 4). Of the original 75 patients, only 56 were able to be contacted. Of those 56 patients, 44 were still wearing the CFM.
Table 4 demonstrates the longevity of the CFM. Approximately 61% of patients who received the CFM had it for more than 6 years.
Table 4Follow-up 2008–2015 (n = 44). |
{kind=link}
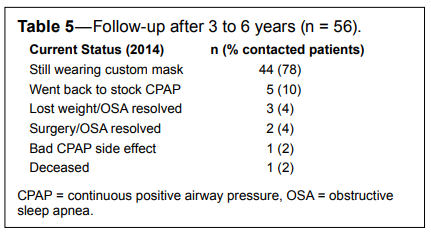
Included in the telephone survey was a question concerning patients’ current status with the CFM regarding combination therapy for OSA (Table 5).
Table 5Follow-up after 3 to 6 years (n = 56). |
{kind=link}
Table 5 demonstrates that 78% of the patients contacted were still wearing the CFM in 2015. After attempts were made to contact all patients in the study, 19 patients were unable to be contacted, which left 56 participating in the telephone survey.
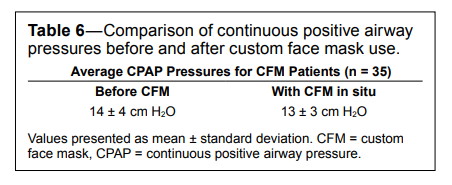
As a part of this follow-up, records were reviewed to determine the CPAP pressures before and after CFM fabrication (Table 6).
Table 6Comparison of continuous positive airway pressures before and after custom face mask use. |
{kind=link}
Table 6 revealed that the average CPAP pressures were reduced after the fabrication of the CFM. Post-CFM fabrication CPAP titrations of 35 patients were obtained. Most patients (n = 23) in this follow-up survey who had any post-CFM insertion reduction of CPAP pressures had significant reduction of pressures. Twelve patients had increased CPAP after the fabrication of the CFM. These pressures were mostly raised by just a few points. These patients had an increased body mass index.
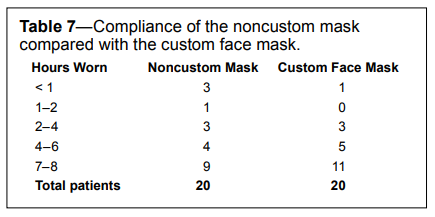
A subgroup analysis (Table 7) by separate telephone survey of the CPAP monotherapy failure group was performed (n = 20) to determine compliance and satisfaction with the CFM. These patients presented to the dental sleep center and were ready to abandon CPAP monotherapy.
Table 7Compliance of the noncustom mask compared with the custom face mask. |
{kind=link}
Table 7 demonstrates that this population represented those on the severe end of the CPAP failure subgroup. The average respiratory disturbance index of 48, AHI of 42, PSO2 of 77% and average CPAP pressures was 15 cm H2O (compare Table 3). The top two noncustom stock mask complaints were leakage (80%) and strap discomfort (40%). With the CFM there was 100% compliance. The top features of the CFM revealed by the patients were comfort (40%) and absence of straps (20%).
These results demonstrate the significant increase in compliance to the CPAP interface with the CFM. The number of patients wearing the stock mask 4 hours or more was 13 (65%); whereas the number of patients wearing the CFM 4 hours or more was 16 (80%).
DISCUSSION
The MAS is clinically accepted as a safe and effective treatment for mild to moderate OSA. From a historical clinical standpoint, they have been used primarily as second-line treatment for patients who are CPAP intolerant for many reasons (mask discomfort, leakage, claustrophobia, skin irritation) in patients with mild to moderate OSA. This retrospective review of patients seen in a single dental sleep clinic is important in demonstrating that combination therapy can be used successfully in patients who have failed the more traditional forms of therapy (MAS or CPAP as monotherapy) in all ranges of OSA severity.
In patients for whom CPAP monotherapy has failed and who subsequently used MAS monotherapy, combination therapy provides a therapeutic option for those who cannot tolerate MAS monotherapy. The most common reason for failure of MAS monotherapy for patients in this study were TMJ symptoms. The next most common side effect of MAS monotherapy for patients in this study was a change in the alignment of the teeth. Both of these side effects increase in frequency, as the mandible is advanced to stabilize the airway.13,14 In utilizing combination therapy, the oral aspect of the device can be set to minimize the advancement of the mandible, thereby reducing these side effects. The chief clinical advantage of combination therapy is its ability to reduce the pressure from the CPAP machine necessary to maintain upper airway patency (particularly in those patients with moderate to severe OSA) as well as the reduction in the degree of advancement of the mandible to lessen the TMJ discomfort and tooth movement that typically accompanies the use of MAS monotherapy. Some of the failures involved the inability of MAS monotherapy to resolve daytime sleepiness. Even if the patients in the MAS monotherapy group showed resolution of OSA on a polysomnogram, respiratory effort related arousals may still be present, resulting in fragmented sleep and continued daytime sleepiness.15
Along with the development of the TAP-PAP CM (CFM) (Figure 3), the TAP-PAP CS with nasal pillows (Figure 2) was available. However, many patients who elected to use CFM either knew they did not want the nasal pillows, or were at the “end of their rope” and just wanted to try one more therapy. In the patients for whom TAP-PAP CS failed, the most common residual sleep symptom was fatigue. The failures of the TAP-PAP CS (nasal pillows) were most often due to intolerance of the high pressures applied through the nasal pillows. The clinical experience of the authors and others who provide this combination therapy with the TAP-PAP CS have observed that the combination system is effective with CPAP less than 15 cm H2O.16 Leakage from or around the mouth was the most common side effect. Even though the intraoral component of the device was the same as the CFM, the leakage occurred between the MAS and the cheeks, resulting in a fluttering or leakage out the mouth that resulted in a loss of effectiveness. In our series, two patients reported discomfort that they attributed to the nasal pillows. The most common negative issue reported was fatigue. Fragmented sleep may have resulted from persistence of the OSA, discomfort of the nasal pillows, the noise of leakage or other factors including residual excessive daytime sleepiness in patients in whom OSA is adequately treated. CFM appears to have resolved many of these issues for those who could not tolerate TAP-PAP CS (nasal pillows).
The noncompliance rate with the CPAP machine (35% to 85%) as defined by nightly use of fewer than 4 h/night and less than 70% of all nights is well documented in the literature.17–20 In our study, the most common reasons for patients to seek alternative treatment options for CPAP machine usage were mask leakage and discomfort related to the elastic headgear (mask straps) (Table 7). The patients electing to use a CFM generally had more severe OSA. The patients in this group required pressure from the CPAP mask (on average) of 15 cm H2O (Table 3), and exhibited greater breathing effort as demonstrated by esophageal pressures of less than −35 cm H2O (Table 1). One of the significant problems with stock noncustom CPAP masks is their inability to work well under high pressures with high amounts of leakage. This has led to the empirical use of full-face masks. However, there is literature to suggest that full-face masks have a higher noncompliance rate compared with nasal masks and can increase the AHI just by the use of an oronasal interface.21,22 If air leakage occurs, then a chin strap is commonly prescribed with or without tightening the headgear/ mask straps. Unfortunately, addition of a chin strap tends to have significant negative effects on the size of the oropharyngeal airway because of the vector force placed on the mandible causing distalization (posterior movement of the mandible back toward the airway), which results in a greater degree of airway obstruction.23 Combination therapy addresses these issues by increasing the retrolingual space by moving the mandible (and the tongue base) anteriorly while stabilizing the mandible. It eliminates the straps by connecting the CPAP airflow interface directly to the oral device and it decreases leakage by means of a customized fit of the facial/nasal interface.
There are circumstances where the delivery of airway pressure through the nose is not effective because of nasal pathology (mouth breathers) and it is desirable to have CPAP delivered orally. Both are effective in therapeutic outcomes.24 With this in mind, the CFM can be modified to create a communication port between the nasal vestibule and the mouth vestibule to allow airflow from the CPAP mask to enter the mouth and nose simultaneously. This was done in four patients in this study. One patient had Graves disease and had undergone an infraorbital decompression that caused her to be intolerant of nasal pressure as it put outward stress on her eyes. The CFM was further customized by adding a communication between the nasal vestibule and the oral vestibule to resolve these issues.
The follow-up telephone survey (Table 5) revealed another aspect of combination therapy with the CFM that has not been considered until now. This survey suggests that the CFM has a longer clinical shelf life when compared to a stock noncustom CPAP mask, raising the possibility that this is a cost-effective therapeutic option. The longevity of this device affects its costeffectiveness. Sixty-one percent of patients were still wearing their CFM after more than 6 years.
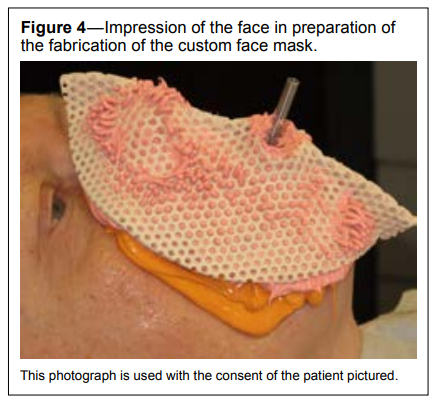
In the analysis of the average CPAP pressure before and after CFM use (Table 6), it was shown that the average pressure was reduced by 1 cm H2O. When there was a reduction in CPAP pressure (for 23 patients) the reduction was significant. This speaks to the efficacy of the seal of the mask and the efficiency of the interface as a whole. The other 12 had an increase in CPAP pressures after the fabrication of the CFM. The reason is probably because the OSA disorder may have actually become worse (nothing to do with the CFM) and the CFM is helping to keep these patients in effective therapy with the higher pressures; or perhaps these patients were undertitrated to begin with (intolerance of high pressures) and now they are able to tolerate these higher pressures with the CFM. A unique aspect of the CFM is that leakage around the mask is significantly reduced by providing an improved seal of the mask against the face. The design of the mask by virtue of the way it is fabricated from an accurate impression of the face (Figure 4), specifically in line with facial and nasal contours, enables the pressure of the PAP to expand the facial skin outward towards the mask, creating a more secure seal.
Figure 4Impression of the face in preparation of the fabrication of the custom face mask. |
{kind=link}
A subgroup analysis of the failed CPAP monotherapy group (Group 3) regarding compliance and comfort (Table 7) revealed that the CFM had a higher compliance and satisfaction when compared to the stock CPAP mask. We hypothesize the reasons for increased compliance and comfort are the elimination of the headgear straps and the stability of the mask. In a study by Prehn,25 there was an unanticipated benefit accorded to the bed partner, with greater satisfaction of the bedroom ambiance with this far quieter therapeutic option.
This is a new therapy for OSA that integrates MAS monotherapy and CPAP. The success of this therapy involves the collaboration of a qualified sleep physician and a qualified sleep dentist. As the technology of combination therapy improves, so will the need for further research. With the modifications available to this mask system, the applications will be expanded as well.
As noted previously, the ability of this combination therapy system to improve treatment effectiveness is accomplished via two mechanisms. The first is the protrusion of the mandible. This physical advancement allows the physical space of airway to increase the lateral dimension of the velopharynx region of the oropharynx.26–28 There is also an increase in tone of the genioglossus muscle.29,30 Both of these mechanisms provide the foundation of the mechanism of action of MAS monotherapy for the treatment of OSA.31 In addition, the combination of effective airflow through the nasal passage32 along with mandibular stabilization offers a potentially superior method of treating OSA.
As more qualified dentists are trained in utilizing the CFM as a therapeutic option in their practice to treat OSA, the data for its application will also expand. It is difficult to deny that for those with severe OSA, this retrospective study of the CFM suggests there may be increased therapeutic success.
Terminology
As we carried out this study and as we prepared the manuscript for publication, we have been engaged in an ongoing discussion about the terminology used to describe the types of combination therapy that are the focus of this study. There is no consistency in the literature to date, and even in discussions with medical/dental professionals there is little clarity about the preferred nomenclature. Since this is an emerging therapeutic option, we suggest that consistent terminology be used going forward. In this study, the term “type 1 combination therapy” refers to therapy that combines MAS and CPAP. We suggest that the term “dual therapy” be used henceforth since it describes two distinct monotherapies that are applied to the patient at the same time. We suggest that the term “type 2 combination therapy,” as used in this study, should instead be “integrated therapy” because it describes two therapies that are integrated into one therapy. Following this terminology, treatment using the CFM would be called integrated therapy.CONCLUSIONS
This retrospective study suggests that patients for whom CPAP monotherapy fails comprise the group that would benefit the most from type 2 combination therapy with the CFM. Although the patients who experienced failure of the other two types of OSA therapy (MAS monotherapy and TAP-PAP CS nasal pillows combination therapy) did benefit from the CFM, the majority of patients (57%) who underwent type 2 combination therapy with the CFM were from the CPAP monotherapy group. This suggests that the CFM should be high on the therapeutic options considered by the clinician when CPAP monotherapy fails.This study suggests that the application of the integrated TAP-PAP CM (CFM) in type 2 combination therapy for patients with more severe OSA is well tolerated with improved compliance. The CFM appears to enable patients to tolerate higher CPAP pressures. The CFM should be considered when other therapeutic methods of treating OSA have failed or when pressures or the CPAP mask are intolerable to the patient.
Because of the cost of the mask (including the hours of labor involved in fabricating and fitting), it is currently not well suited as a first-line therapeutic option. However, we think the cost should decrease over time as more cost-efficient systems to create custom hardware (for example, face scanners, threedimensional printers) become available. Furthermore, the longevity of the CFM may prove that it is a cost-effective option in the long-term.
REFERENCES
2. Ramar, K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: an update for 2015. J Clin Sleep Med. 2015;11(7):773–827.
3. Phillips C, Grunstein RR, Darendeliler MA, et al. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea: a randomized controlled trial. Am J Respir Crit Care Med. 2013;187(8):879–887.
4. Hoekema A, Stegenga B, Wijkstra PJ, van der Hoeven JH, Meinesz AF, de Bont LG. Obstructive sleep apnea therapy. J Dent Res. 2008;87(9):882–887.
5. Oksenberg A, Arons E, Froom P. Does the severity of obstructive sleep apnea predict patients requiring high continuous positive airway pressure? Laryngoscope. 2006;116(6):951–955.
6. Denbar MA. A case study involving the combination treatment of an oral appliance and auto-titrating CPAP unit. Sleep Breath. 2002;6(3):125–128.
7. El-Solh AA, Moitheennazima B, Akinnusi ME, Churder PM, Lafornara AM. Combined oral appliance and positive airway pressure therapy for obstructive sleep apnea: a pilot study. Sleep Breath. 2011;15(2):203–208.
8. Thornton WK, inventor; Thornton WK, assignee. Combination face mask and dental device for improved breathing during sleep. US patent 6,209,542. January 31, 1996.
9. Thornton WK. Case report-combined CPAP-oral appliance therapy. Sleep Review Web site. http://www.sleepreviewmag.com/2002/01/ news-story-29. Published January 9, 2002. Accessed January 11, 2017.
10. Upadhyay R, Dubey A, Kant S, Singh BP. Management of severe obstructive sleep apnea using mandibular advancement devices with auto continuous positive airway pressures. Lung India. 2015;32(2):158–161.
11. de Vries GE, Doff MH, Hoekema A, Kerstjens HA, Wijkstra PJ. Continuous positive airway pressure and oral appliance hybrid therapy in obstructive sleep apnea: patient comfort, compliance, and preference: a pilot study. Journal of Dental Sleep Medicine. 2016;3(1):5–10.
12. Prehn R, Colquitt T. Fabrication technique for a custom face mask for the treatment of obstructive sleep apnea. J Prosthet Dent. 2016;115(5):551–555.
13. Doff MH, Finnema KJ, Hoekema A, Wijkstra PJ, de Bont LG, Stegenga B. Long-term oral appliance therapy in obstructive sleep apnea syndrome: a controlled study on dental side effects. Clin Oral Investig. 2013;17(2):475–482.
14. Doff MH, Hoekema A, Wijkstra PJ, et al. Oral appliance versus continuous positive airway pressure in obstructive sleep apnea syndrome: a 2-year follow-up. Sleep. 2013;36(9):1289–1296.
15. Savani A, Guilleminault C. Neurologic basis of sleep breathing disorders. Sleep Med Clin. 2012;7(3):555–562.
16. White J, et al. Efficacy and tolerance of combination therapy using MAS supported nasal pillows (abstract). 20th Anniversary Meeting of the American Academy of Dental Sleep Medicine, Minneapolis, Minnesota, USA, 10–12 June 2011. Sleep Breath. 2011;15(2):253–261.
17. Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc. 2008;5(2):173–178.
18. Gay P, Weaver T, Loube D, et al. Evaluation of positive airway pressure treatment for sleep related breathing disorders in adults. Sleep. 2006;29(3):381–401.
19. Boyaci H, Gacar K, Bar?? SA, Ba?yi?it I, Y?ld?z F. Positive airway pressure device compliance of the patients with obstructive sleep apnea syndrome. Adv Clin Exp Med. 2013;22(6):809–815.
20. Weaver TE. Don’t start celebrating--CPAP adherence remains a problem. J Clin Sleep Med. 2013;9(6):551–552.
21. Westhoff M, Litterst P. Obstructive sleep apnoea and non-restorative sleep induced by the interface. Sleep Breath. 2015;19(4):1317–1325.
22. Ebben MR, Narizhnaya M, Segal AZ, Barone D, Krieger AC. A randomised controlled trial on the effect of mask choice on residual respiratory events with continuous positive airway pressure treatment. Sleep Med. 2014;15(6):619–624.
23. Borel JC, Tamisier R, Dias-Domingos S, et al. Type of mask may impact on continuous positive airway pressure adherence in apneic patients. PLoS One. 2013;8(5):e64382.
24. Weaver TE, Sawyer A. Management of obstructive sleep apnea by continuous positive airway pressure. Oral Maxillofac Surg Clin North Am. 2009;21(4):403–412.
25. Prehn R. New applications for combination therapy (abstract). 22nd Annual Meeting of the American Academy of Dental Sleep Medicine, Baltimore, MD, USA May 30–June 1, 2013. Sleep Breath. 2013;17(2):888–889.
26. Brown EC, Cheng S, McKenzie DK, Butler JE, Gandevia SC, Bilston LE. Tongue and lateral upper airway movement with mandibular advancement. Sleep. 2013;36(3):397–404.
27. Chan A, Sutherland K, Schwab RJ, et al. The effect of mandibular advancement on upper airway structure in obstructive sleep apnoea. Thorax. 2010;65:726–732.
28. Sam K, Lam B, Ooi CG, Cooke M, Ip MS. Effect of a non-adjustable oral appliance on upper airway morphology in obstructive sleep apnoea. Respir Med. 2006;100(5):897–902.
29. Shinagawa H, Murano EZ, Zhuo J, et al. Effect of oral appliances on genioglossus muscle tonicity seen with diffusion tensor imaging: a pilot study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107(3):e57–e63.
30. Tsuiki S, Ono T, Kuroda T. Mandibular advancement modulates respiratory-related genioglossus electromyographic activity. Sleep Breath. 2000;4(2):53–58.
31. Scherr SC, Dort LC, Almeida FR, et al. Definition of an effective oral appliance for the treatment of obstructive sleep apnea and snoring: a report of the American Academy of Dental Sleep Medicine. Journal of Dental Sleep Medicine. 2014;1(1):39–50.
32. Sullivan CE, Issa FG, Berthon-Jones M, Eves L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet. 1981;1(8225):862–865.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication May 23, 2016
Submitted in final revised form November 22, 2016
Accepted for publication November 27, 2016
Address correspondence to: Ronald S. Prehn, DDS, 1001 Medical Plaza Drive, Suite 200, The Woodlands, TX 77380; Tel: (281) 296-6797; Fax: (281) 296-6778; Email: rprehn@tmjtexas.com
DISCLOSURE STATEMENT
This was not an industry supported study. Work for this study was done at a dental sleep center owned by the first author. The authors have indicated no financial conflicts of interest. The devices used in this study are FDA approved.