Special Article 4, Issue 1.1
History of Dental Sleep Medicine
http://dx.doi.org/10.15331/jdsm.3744
Robert R. Rogers, DMD, DABDSM1 ; John Remmers, MD2 ; Alan A. Lowe, DMD, PhD, ABDSM3 ; Peter A. Cistulli, MD, PhD4 ; Jeff Prinsell, DMD, MD, DABDSM5 ; Donald Pantino, DDS, ABDSM6
1Pittsburgh Dental Sleep Medicine, Wexford, PA; 2 Sedona, AZ; 3 Department of Oral Health Sciences, University of British Columbia, Vancouver, BC, Canada; 4 Department of Respiratory Medicine, Royal North Shore Hospital, Saint Leonard’s, NSW, Australia; 5 Marietta, GA; 6 Islip, NY
As this inaugural issue of The Journal of Dental Sleep Medicine debuts, it is my pleasure to recount the historical highlights of the development of Dental Sleep Medicine over the past 25 years. The youthfulness of this nascent field allows us the luxury of calling on some of the original pioneers for their direct recollection and comment in this regard. I have chosen to let each submission stand essentially on its own to reflect the individual author’s unique, personal take on the subject. As such, there may be some redundancies in the content and a difference in writing style. I am hoping this adds to the depth and texture of the presentation.
The basic underpinnings of Dental Sleep Medicine are the critical roles sleep and breathing play in the maintenance of overall health and well-being and indeed, life itself. Presently, it is well known that sleep deprivation and sleep disorders are highly prevalent and are intimately related to adverse social, health, and occupational problems. Snoring is no longer thought to be benign, and obstructive sleep apnea is viewed in epidemic proportion worldwide. Fortunately, continuous positive airway pressure (CPAP) has been found to prevent upper airway collapse, normalize nocturnal sleep and breathing, alleviate daytime hypersomnolence, and decrease associated medical comorbidity. However, despite the benefits positive airway pressure intervention can provide, adherence remains a significant issue and effective treatment options are needed.
The impact of tongue and mandibular positioning on upper airway patency has been well known for over 100 years and remains the functional basis of the “jaw thrust” during CPR maneuvers. In the early 1900s, surgeons occasionally treated micrognathic infants by suturing the tongue to the lower lip in a forward position attempting to open and stabilize the upper airway during sleep. By 1930, helmets and chin straps were utilized by physicians for mandibular repositioning in an effort to accomplish the same goal. The first described use of an intra-oral mandibular repositioning device is generally attributed to Pierre Robin, a French pediatrician, in 1923.1 Since then, surgical advancement of the maxilla and mandible has been reported and, in 1982, Charles Samuelson, a Chicago psychiatrist, designed a tongue retaining device that was shown to be effective.2
Substantial progress has been documented in the expanding literature. A milestone review appeared in the 1995 literature summarizing the efficacy of oral appliance therapy (OAT) for the first time and suggested clinical practice parameters.3,4 In 2005, these two documents were revised to reflect the newer data in this growing field,5,6 and the scientific literature is replete today with investigations supporting OAT. Most recently, the American Academy of Sleep Medicine has, for the first time, published guidelines for the evaluation, management, and long-term care of obstructive sleep apnea in adults that cites OAT as an effective option for management of sleep disordered breathing.7
Today, Dental Sleep Medicine represents a synergistic blend of medicine and dentistry as dentists bring their unique skills associated with the stomatognathic system to bear on the problems that physicians face attempting to create and maintain a patent airway during sleep.
—Robert R. Rogers
DENTISTS, DENTISTRY, AND SLEEP APNEA: AN UNINHIBITED HISTORY AND PERSONAL PERSPECTIVE
For a physician and non-historian to write on the historical role of dentists in sleep science might be presumptuous or folly depending on your viewpoint. I will attempt to mitigate concerns by restricting my comments to sleep apnea.
Dentistry was pivotal in the earliest elucidation of sleep apnea. In 1932 the well-known French dental surgeon, Pierre Robin, described a breathing impairment during sleep caused by pharyngeal obstruction in children with micrognathia and glossoptosis.1 This was the first clear demonstration that oralpharyngeal anatomic abnormalities can induce a narrowing of the pharyngeal airway that obstructs breathing during sleep. In this seminal contribution, Robin laid the groundwork for understanding the role of pharyngeal obstruction in the pathogenesis of sleep apnea. Arguably, the entire field of sleep disordered breathing was founded by a dentist who discovered that anatomic abnormalities of the pharynx lead to obstruction of breathing during sleep.
Thirty-eight years later, another dental scientist, Eberhart Sauerland, provided a complimentary insight to Robin’s when he discovered the respiratory action of pharyngeal muscles. While not formally educated as a dentist, “Ebo” was a dental academician at the UCLA Dental School. In 1970, he reported that during inspiration, humans displayed a burst of EMG activity in the genioglossus muscle, thereby dilating and stiffening the pharynx when subatmospheric intraluminal pressure acts to narrow it.8 In 1976 with Ron Harper, he extended this finding by showing that the rhythmic respiratory bursting of the genioglossus is exhibited by normal humans during sleep.9 Thus, the contributions of two dental scientists, Robin and Sauerland, laid the foundation for our understanding of that pharyngeal structure and function engage in a complex neural-anatomical interaction that maintains pharyngeal airway during wakefulness and sleep.
In the early 1970s, Sauerland and I serendipitously moved to the same institution, the University of Texas Medical Branch, met, and collaborated. Two kinds of creation myths are told: one where life arises from the mud and another where it falls from the sky. Both sources of creativity contributed to our research collaboration. Wallowing in the mud, I was trying to comprehend why some people stop breathing when they sleep. Sadly, I found that the culprit was the pharynx, an area of total ignorance for me. Ebo, a preeminent expert on pharynx, appeared from the sky, illuminating the relevant anatomy and the respiratory actions of the pharyngeal muscles. Our collaboration was magical; we arrived at the first comprehensive understanding of sleep apnea, showing that it originates from chemoreceptordriven, cyclic variation in the activity of the genioglossus, which in turn, causes repetitive opening and closure of the pharyngeal airway.10
The need for convenient methods of treating sleep apnea has stimulated advances in dental sleep science. The rather barbaric features of standard medical therapy, continuous positive airway pressure (CPAP), spurred dentists to invent dental appliances that might relieve pharyngeal obstruction during sleep by protruding the mandible. The specifics of this development are related elsewhere in this issue. The point to be emphasized here, however, is that dental scientists developed a novel therapy and carried out appropriate validation research. Noteworthy in this regard is the pioneering study of Clark,11 providing clear evidence that mandibular protruding dental appliances can be efficacious in eliminating OSA, and, hence, may constitute an alternative CPAP therapy. Thus, the problematic aspects of the medical treatment of OSA set the stage for advances in dental sleep science.
The relative efficaciousness of oral appliances therapies has been evaluated by clinical trials involving the collaboration of dental and medical investigators. Three will be mentioned here. Lowe collaborated with medical colleagues in a crossover comparison of nasal CPAP and oral appliance therapy. The results revealed that oral appliance therapy, while preferred by patients, had lower efficaciousness rate than CPAP.5 A randomized clinical trial with long-term follow-up, involving the Swedish dentists Tegelberg and Ringqvist, compared oral appliance therapy to pharyngeal surgery and showed that oral appliance therapy has superior effectiveness to surgery in the long term.12 Hoekema carried out a large randomized trial comparing CPAP with oral appliance therapy in treating OSA.13 This study showed that the two therapies are comparably effective in treating OSA when adherence and symptomatic improvement are taken into account.
That sleep apnea conveys significant cardiovascular risk implies that any successful therapy for this disease must be highly effective. This has particular significance for oral appliance therapy, as it is efficacious in only half of all apneics.14 In other words, for oral appliances to become a front-line therapeutic option for sleep apnea, methods for selecting favorable candidates for this therapy must be developed. Such predictive methods are being actively explored, and dentists have participated in this search. Marklund and Tsuiki have described promising clinical features that may be helpful in this regard.15,16 Dort and Charkhandeh have shown that a remotely controlled mandibular positioner used in a polysomnographic setting provides an accurate selection method.17,18 While the search is far from over, there is ample reason to be optimistic about the advent of methods that will allow selection of patients for oral appliance therapy.
This brief historical review highlights the resonance, collaboration, and mutual reinforcement that have occurred between the two fields—sleep medicine and dental sleep medicine. Current and anticipated technological advances suggest that we are now embarking on a new phase of this relationship, one where the sleep dentist and physician will collaborate efficiently in widespread use of oral appliances to manage OSA. In other words, we may be entering a new era of sleep medicine, one where dental sleep medicine plays a central role: A perfect time to launch a new journal.
—John E. Remmers
EVOLUTION OF ORAL APPLIANCES
Oral appliances (OAs) have evolved in the treatment of sleep disordered breathing as an increasingly popular alternative to more established therapies, including continuous positive airway pressure. Although the early literature consisted of case reports and a number of small case series, a significant number of randomized controlled studies have been reported in the last decade, which clearly document the efficacy of both preformed and custom-made appliances. The concept of moving the tongue and jaw forward to correct a compromised airway has been effectively used for many decades in anesthesiology and orthodontics and is now being applied to OSA.Each of the more than 100 currently available OAs has a primary effect on either the tongue or the tongue and mandible together. Several appliances move the mandible anteriorly. The tongue is affected by all the appliances either by direct forward movement of the muscle itself or by changes secondary to an altered mandibular position. In 1923, Pierre Robin described glossoptosis (tongue obstruction) due to mandibular hypotrophy and used a monobloc functional appliance to move the mandible forward. Since then, many variations in mandibular repositioning appliances have been used to affect growth, change airway size, and alter the dentition. A maxillary appliance with an attached esophageal tube has been used to open and advance the mandible. Meier-Ewert was the first to describe a rigid mandibular repositioning appliance to move the mandible forward that was effective in reducing OSA. Numerous reports based on single case studies also documented the use of similar appliances.
A significant number of “boil and bite” appliances have been developed over the years. They are very easy to fit and adjust directly on the patient and appear to be well tolerated, but retention issues may appear in the long term. Failure rates with thermoplastic appliances appear to be higher than with custom-made appliances. Based on their low success rates, it has also been suggested that they not be used as screening tools for custom-made appliances. The overall amount of mandibular protrusion is not controlled and is not reproducible in the absence of study models and an accurate bite registration.
Preformed and custom-made appliances have also been designed to hold the tongue forward during sleep. One custom-made appliance has an anterior bulb which, by means of negative pressure, holds the tongue forward during sleep. For those patients with blocked nasal passages, a modified appliance with lateral airway tubes is also available. Tongue appliances have been studied in various body positions and in conjunction with other forms of therapy.
Over time, the concept of an adjustable appliance to allow titration of the mandibular position over time was developed. Dentists realized early on that determining the correct jaw position to fully open the airway was the most difficult step to use OAs successfully. Considerable variations in the initial comfortable range of the anteroposterior movement of the mandible and differences in the speed and the amount of forward jaw position that any given patient could tolerate were found. Single jaw position appliances often needed to be remade if the initial jaw position proved to be inadequate. Gradual titration forward of the mandible without the necessity of making a new appliance each time became the objective, and numerous adjustable mandibular repositioning appliances were invented and marketed. It was also observed that a subgroup of patients, particularly those who suffered from sleep bruxism, often experienced a considerable amount of jaw discomfort in the morning after wearing a rigid hard acrylic single jaw position OA. A need to develop OAs that could allow for lateral jaw movement as well as some degree of vertical jaw opening was addressed.
At the same time, retention issues were identified as a major concern, since if the mandible drops out of the appliance, effectiveness is significantly reduced. In addition, major advances in dental materials significantly improved the flexibility and strength of thermosensitive acrylic resin materials. Appliances made of temperature-sensitive material that the patient could heat in hot water before insertion that would cool and harden somewhat intraorally were found to have better retention than traditionally designed cold cure acrylic appliances. Techniques for the determination of the correct jaw position that can be obtained during sleep studies have been developed. The combination of adjustability, lateral and vertical jaw movement, increased retention, and better defined titration protocols all significantly improved the effectiveness of OAs, and a myriad of appliances have been designed and marketed.
As OAs continue to evolve over time, several questions require further study. How can one easily identify the obstruction site in a cost-effective way so as to utilize the most effective OA? Which patients are ideally suited for an OA? Which appliance will be most effective in any one patient? What is the long-term compliance with these appliances? What are the long-term periodontal implications? Are there any long-term deleterious effects?
Unfortunately, aggressive marketing of specific appliances together with professional disagreements as to the snoring/ OSA caseload distribution have slowed down the acceptance of this treatment modality. The efficacy of OAs for the effective treatment of snoring and/or OSA is no longer in question. Only their correct management and supervision require clarification. However, the issue of patient compliance with OAs does need to be evaluated further. Recent compliance monitor developments suggest that a randomized clinical trial with an accurate monitor embedded directly into the OA can now be undertaken. As the field exists today, if the initial assessment is coordinated by the attending physician and good communication is established with the dentist involved, a significant number of subjects with snoring and/or OSA can be effectively treated with a variety of currently available OAs. The evolution of these appliances over time has been rapid and successful in providing effective management of OSA.
INDICATIONS/EFFICACY OF OAT
Pierre Robin is generally credited with the earliest clinical work on OAT, when in 1902 he described a “monoblock” device for the treatment of glossoptosis.19 He subsequently used an oral appliance to reposition the mandible.20 A further 50 years elapsed before the earliest reports of the use of oral appliances for the treatment of snoring and obstructive sleep apnea (OSA), involving a tongue retaining device2 or a mandibular advancement device.21 The evidence base supporting the role of OAT in the management of OSA has gradually evolved over the last 30 years, reaching the point today where OAT is increasingly recognized as a viable and effective treatment option for many patients.The last decade in particular has witnessed substantial advances in the field through rigorous research evaluating the efficacy and effectiveness of OA therapy, and particularly mandibular advancement devices. The earliest randomized controlled trials of OAT were published in 1996 by Clark et al.22 and Ferguson et al.14 In 2001, Mehta at al. published the first placebo-controlled study in the field, and advocated for a stringent definition of treatment outcome that is on par with CPAP treatment.23 This spawned a series of important studies, and the strengths of these newer studies include rigorous clinical trial designs, further comparisons to placebo treatment (e.g., inactive oral devices or tablet placebo), adoption of more stringent definitions of treatment outcome, direct comparisons to the gold standard therapy (i.e., CPAP), and an increasing focus on health outcomes.
The early focus of research was on polysomnographic and symptomatic outcomes, including snoring, daytime sleepiness and other major symptoms, and patient preference. More recently there has been an important and substantial shift to more relevant health outcomes, including neuropsychological and cardiovascular endpoints. There is now strong evidence from randomized controlled trials that OAT is effective in the prevention or significant reduction in the number of obstructive respiratory events and arousals and improvement in arterial oxygen saturation across the full spectrum of OSA severity.24
Ultimately the goal of any OSA treatment is to prevent the occurrence of complete or partial upper airway collapse during sleep. OAT has been associated with a reduction of the apneahypopnea index (AHI) to normal levels (< 5/h) in 36% to 50% of patients, and up to 70% of patients achieve an AHI < 10/h.24 Using the most liberal definition of treatment outcome, namely a > 50% reduction in AHI, an average of 65% of patients achieve this outcome.24 With regard to oxygen saturation parameters, the improvements noted with OAT is of smaller magnitude than the changes in AHI, and rarely to normal levels. Some studies have reported improved sleep architecture. Similarly, reductions in arousal index have been reported. It seems likely that differences in OAT designs have a major influence on the extent to which these parameters are improved, but research on this is lacking.
In terms of downstream health outcomes, OAT appears to lead to improvement in subjective daytime sleepiness, as measured by the Epworth Sleepiness Scale. A limited number of studies using objective tests of sleepiness and simulated driving performance report improvements equivalent to those with CPAP. General and disease-specific quality of life are improved with OAT. Reports on the effect of OAT on neurophysiological function are limited but show an improved performance in some neurocognitive assessments after oral device treatment. As OSA is associated with increased cardiovascular morbidity and mortality, modifying this risk is an important goal of treatment. Modest reductions in blood pressure (2 to 4 mm Hg) following treatment with OAT have been reported in both uncontrolled and randomized placebo-controlled trials.25 Currently longterm studies into the effect of OAT on cardiovascular endpoints are lacking. However, there is some evidence that OAT may improve intermediate endpoints such as oxidative stress, endothelial function, and arterial stiffness.26
Improvements in long-term adverse health consequences are of course dependent on sustained efficacy of the treatment over time. However, less is currently known about the effectiveness of OAT therapy long term. Studies reevaluating patients 1 to 5 years after treatment initiation indicate that there is a reasonably high rate of sustained control, even in cases of severe OSA.27 Reductions in efficacy can be attributed to issues such as weight gain or device wear and tear and highlight the need for long-term dental and medical follow-up to sustain effectiveness.
A meta-analysis of studies comparing OAT to CPAP found OAT less efficacious in improving polysomnographic measures of OSA (AHI, oxygen saturation). CPAP reduces the AHI, improves sleep efficiency, and attenuates oxyhemoglobin desaturation to a greater degree than OAT.28 However reports of similar improvements in health outcomes (e.g., blood pressure, sleepiness) suggest that there may not be such a discrepancy in clinical practice. Specifically, suboptimal compliance to CPAP reduces its clinical effectiveness, and recent research suggests that the health outcomes of CPAP and OAT are equivalent, at least in the short term.29 Among patients who responded to both therapies, there is strong preference for oral appliances.
The earliest clinical practice parameters on the use of OAT in OSA were produced by the American Academy of Sleep Medicine in 1995.4 The subsequent growth in robust evidence was incorporated in an updated comprehensive review of OA therapy published in 2006, along with updated practice parameters for their use.5,6 As of 2006, clinical practice parameters of the American Academy of Sleep Medicine (AASM) state that oral devices are indicated as a first-line therapy for patients with mild-to-moderate OSA who prefer an oral appliance over CPAP or who fail treatment attempts or are inappropriate candidates for CPAP.6 OAT can effectively treat OSA across a range of disease severity; however, it is currently recommended that patients with severe OSA initially try CPAP (due to its superior efficacy) before considering an oral device. Similarly, CPAP therapy is preferred in severely symptomatic patients who require urgent treatment (such as in cases of sleepy drivers) and those with medical comorbidities, as CPAP may be immediately effective, whereas oral device therapy requires an extended acclimatization period until optimal therapeutic benefit is achieved. Given the continuing growth in the evidence base, there is now a need to further update practice parameters to reflect an expanded role of OAT in the management of OSA.
Future comparative effectiveness studies are needed to assess long-term outcomes of OAT in comparison to CPAP. Such work will be enhanced by the ability to objectively monitor OAT use and emerging methods to reliably predict treatment outcome, using phenotypic approaches or single-night titration methods. Research is also needed to assess the influence of appliance design features on efficacy and compliance, as well as methods to optimize the titration process.
SURGICAL APPROACHES
OSA surgery is generally indicated when conservative treatments such as CPAP, oral appliances, weight reduction, positional, and other behavioral therapies are unsuccessful or intolerable. It can be safe and therapeutic if performed competently and on the correctly identified specific anatomic sites or levels that contribute to upper airway obstruction, which vary between patients. There are many surgical procedures30 and approaches that can be classified anatomically as upper airway bypass (e.g., tracheostomy), intrapharyngeal versus extrapharyngeal, and unilevel versus multilevel. For cases of multiple levels or diffusely complex sites of disproportionate upper airway anatomy, it is often difficult to decide when and how to prioritize and combine surgical procedures in one or more stages.One approach is to perform certain procedures in a stepwise fashion according to a methodical protocol,31 usually beginning with intrapharyngeal surgery on the soft palate (e.g., uvulopalatopharyngoplasty [UPPP]) and other anatomic structures such as the tonsils/adenoids or segmental soft tissues such as the tongue base that compromise or impinge upon the velo-orohypopharyngeal airway. However, this may result in unnecessary multiple operations that may be painful, dysfunctional, expensive, subtherapeutic, and, ultimately a deterrent for patients to pursue additional surgery.
Extrapharyngeal surgery such as maxillomandibular advancement (MMA) pulls forward the anterior pharyngeal soft tissues suspended from the maxilla, mandible, and hyoid to enlarge and stabilize the entire velo-orohypopharyngeal airway with minimal risks of airway embarrassment resulting from edema in the immediate postoperative period or recurrent OSA due to cicatricial scarring and stenosis, because the osteotomies are outside the pharyngeal airway lumen.32 Although highly therapeutic, telegnathic MMA, which can be a secondary or primary operation with or without adjunctive procedures such as an anterior inferior mandibular osteotomy, removal of anterior mandibular lingual tori, septoplasty with turbinate reduction, sinus curettage, and cervicofacial lipectomy,33 is a long and technically difficult surgery with risks of neurosensory deficits, malocclusion, and unavoidable changes in facial appearance that can be unesthetic.
The plethora of surgical procedures and approaches can be confusing and intimidating, the selection of which should not be industry-driven or specialty-specific, but rather based on the individual patient’s sites of disproportionate upper airway anatomy and stated preference following comprehensive informed consent that includes a discussion of the risks versus benefits and alternatives to treatment.34 Preoperative assessment involves integration of clinical and radiographic examination including multiple airway imaging modalities, as well as a thorough understanding of the patient’s OSA severity and other medical comorbidities that may require multidisciplinary management perioperatively.
Patients should be monitored closely, particularly for airway management with continuous pulse oximetry, in the immediate postoperative period. Repeat diagnostic PSG, usually obtained several months postoperatively, is necessary to document therapeutic efficacy. Based on percent reduction in AHI, multilevel approaches with MMA and adjunctive extrapharyngeal procedures are generally more therapeutic than multilevel combinations of intrapharyngeal procedures.33,34 However, long-term success of OSA surgery should be measured by a yet undefined comprehensive algorithm of standardized multiple weighted outcome parameters that includes PSG measurements, health, performance, and quality-of-life variables.
MULTIDISCIPLINARY APPROACH TO SLEEP DISORDERED BREATHING: THE ROLE OF THE DENTIST
Sleep impacts nearly every aspect of health, development, and well -being. The most common sleep disorder is sleep disordered breathing (SDB). The number of health concerns linked to SDB continues to increase. Most health care providers and safety and business leaders directly or indirectly deal with the consequences of SDB on a daily basis, presenting both a challenge and an opportunity.Twenty-five years ago, dentists would not have expected to develop clinical practices as exist today concentrated on caring for those with SDB. Because the dentist-patient relationship is long-term with regular follow-up, dentists are well positioned to participate in the recognition, prevention, and treatment of SDB.
Many dental practitioners can participate in the field of SDB. General practitioners, maxillofacial surgeons, and orthodontists can work together in a multidisciplinary approach to the prevention and treatment of SDB.
Dentists trained in dental sleep medicine can offer an evidence-based alternative therapy to those who have been diagnosed with SDB and are unable, unwilling, or simply unsuccessful with other therapeutic interventions. Most importantly every dentist through routine examination and history can help screen, refer, and care for these patients. These are but a few of the skills and abilities that allow us to work with and be an integral part of the SDB team. Once we understand the medical, cognitive, psychological, social, behavioral and subsequent economic consequences of SDB, the need for a multidisciplinary approach to SDB becomes clear.
Understanding the complex nature of SDB gives us the opportunity to seek out, educate, and work with other members of the healthcare and business communities to participate in a multidisciplinary approach to patient care. This relationship is very different depending geography, demographics, education, philosophy, and other factors. What we all have in common is caring for and treating the patient.
EVOLUTION OF THE AMERICAN ACADEMY OF DENTAL SLEEP MEDICINE (AADSM)
As sleep medicine and the therapeutic modalities to treat sleep disordered breathing evolved, it became apparent that an option to continuous positive airway pressure was sorely needed. Although oral appliances were first utilized in the early 1900s to stabilize the upper airway during sleep, the resurgence in their use did not occur until the 1980s. At this point in time, research supporting their use was scant and the number of practitioners utilizing oral appliances for this purpose was miniscule.Quite serendipitously in 1990, this author received a phone call from a dentist-friend (Arthur Strauss, DDS) inquiring as to whether or not I was aware of oral appliances being used to treat snoring and obstructive sleep apnea. I admitted that I was not and struggled to remember exactly what obstructive sleep apnea actually was since my academic dental school days were fading quickly into my past. As such, we decided to attend a continuing education course in San Antonio entitled, “Training in the Principles of the Snore Guard Dental Orthosis,” delivered by a dentist, Thomas E. Meade, DDS, who had done some seminal oral appliance research with his medical colleague, Wolfgang Schmidt-Nowara, MD. That weekend changed my life, the lives of many of our patients, and the course of dental sleep medicine. (see Box 1).
Box 1AADSM Timeline |
{kind=link}
Upon returning from San Antonio, we convened a very informal telephone “study club,” comprising a handful of us who had placed a modest number of boil and bite Snore Guard appliances for the purposes of discussing our experiences. As memory serves, this small group included me, Arthur Strauss, DDS; Peter George, DDS; Alan Lowe, DMD, PhD; Michael Alvarez, DDS; Gary Johnson, DDS; Jeffery Hall, DDS; and Don Rosenbloom, DDS. A year into this, the bold step of creating a formal society was taken, so named the Sleep Disorder Dental Society (SDDS). These Founding Members placed a small ad in the Journal of the American Dental Association soliciting members. To our great surprise, a number of dentists responded and created a core group of Charter Members. In 1992, the first annual meeting was held in Phoenix, Arizona, with attendance of approximately 25 of our founding and charter members.
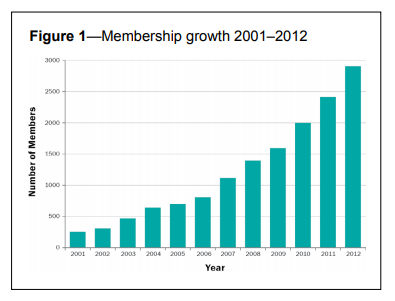
Renamed The Academy of Dental Sleep Medicine in 2000 and later the American Academy of Dental Sleep Medicine in 2006, the Academy today lists approximately 3,000 total members (Figure 1), with more than 230 being located outside the United States in 27 foreign countries. Instrumental in this impressive growth from the beginning, was Mary Beth Rogers, the Academy’s first Executive Director. She operated the Academy during its first decade from the den in our house and nurtured the fledgling organization during the delicate, formative years building it into a viable, credible organization. As the scope and magnitude increased, Jerry Barrett was asked to bring his special talent and sophisticated resources to bear upon the evolution of the society and bring it to the level it is today. Thanks to these two committed individuals, there are currently over 3,000 members with nearly 200 board-certified Diplomates and 5 International Certificants. The Academy is the leading professional organization promoting the special interest area of dental sleep medicine and advocates for excellence in clinical care, providing educational opportunities to its members and other health professionals.
Figure 1Membership growth 2001–2012 |
{kind=link}
Specifically, the purpose of the organization is to:
- establish, update and maintain standards for the treatment of sleep disordered breathing by dentists utilizing oral appliances and/or surgical techniques;
- establish an exam process for certification in dental sleep medicine (oral appliance track and surgical track);
- provide a forum for the exchange of information on dental sleep medicine;
- promote the role of a dentist in the treatment mix of sleep disordered breathing; and
- represent the discipline in relation to professional health organizations, federal/local regulatory bodies, and federal/private health insurers.
In 1998, through the tireless efforts of Harold Smith, DDS, the American Board of Dental Sleep Medicine (ABDSM) was established and created the first certification program in dental sleep medicine. This provided a means for dentists in the field of dental sleep medicine to be recognized as possessing the knowledge and skills necessary to interface with physicians and competently manage appropriate sleep disordered breathing patients. The ABDSM is an entity independent from the AADSM with input from a professional testing organization regarding test questions and analysis of results.
In 2012, Steven Scherr, DDS, guided a committee that created an AADSM Office Accreditation program which supports standards and requirements for billing Medicare and other insurers while identifying accredited dental offices as a highest level provider. The Office Accreditation program focuses on designated quality standards such as administration, financial management, human resource management, consumer services, performance management, product safety, information management, and supplier product-specific service requirements.
Practitioner education stands as an essential part of the Academy mission. Numerous courses have been developed and are continually offered including Essentials of Dental Sleep Medicine, Advanced Dental Sleep Medicine, Board Review Course, and Practical Demonstration to mention a few.
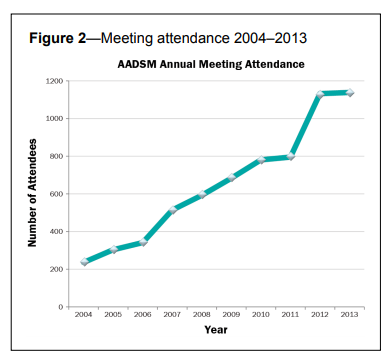
By the 12th annual meeting in 2003, attendance was at nearly 500. Attendance approached 800 people at the 20th anniversary meeting in 2011. Meet the Professor Sessions, introduced during the 17th annual meeting in 2008, steadily expanded from three the first year offered to the nine sessions currently available at the annual meeting. In Boston, 2012, the meeting expanded to a 2-track program for the first time, and the Academy saw record-breaking attendance with over 1,100 attendees at this 21st annual meeting (Figure 2).
Figure 2Meeting attendance 2004–2013 |
{kind=link}
FUTURE OF DENTAL SLEEP MEDICINE
This is been an overview highlighting the history of dental sleep medicine and the American Academy of Dental Sleep Medicine. As we look to the future, we must not lose sight of the innumerable contributions of the many researchers, educators, inventors, and practitioners whose collective efforts have given increasing credence to the role of the dentist in the management of sleep disordered breathing.The field of dental sleep medicine will undoubtedly continue to grow through advancing research and technology, allowing the role of the dentist to continually morph and expand. As a result, the relationship between the dentist and physician will become more finely tuned, to the benefit of all concerned. And as our younger colleagues enter the ranks of the dental profession, it will become critical that dental school curricula include meaningful courses in dental sleep medicine. The seeds have already germinated, as several leading universities already offer their students guidance in this area.
Objective research supporting dental sleep medicine together with physician acceptance and increasing patient demand have influenced insurance carriers to offer benefits for oral appliance therapy and surgical procedures to manage sleep disordered breathing. Their focus on access to care, efficacy of treatment, and conservation of resources will challenge and guide us as our clinical protocols evolve. Likewise, the commercial interests of manufacturers may play some role as we blend their contribution into responsible clinical care.
Especially provocative is the evolution of the oral appliance itself and how it may affect creation and maintenance of a patent airway during sleep. How nice it would be to be able to identify good candidates for oral appliance therapy and to accurately pinpoint upper airway sites of obstruction. Our best and brightest thinkers and tinkerers are tasked with inventing and testing different methods to influence oral/ pharyngeal anatomy to prevent airway collapse. And as oral appliances and surgical procedures reach many millions of people, a better understanding of side effects and adherence loom as critical topics of study and investigation.
All told, the past 25 years have seen the creation and evolution of a unique, new branch of dentistry that now serves to offer physicians an effective option to manage a life-threatening malady. Indeed, millions of people worldwide have benefited from dental sleep medicine and will continue to do so in the years to come.
APPENDIX
Past Presidents of the American Academy of Dental Sleep Medicine
• Arthur M. Strauss, DDS—1992–1993
• R. Michael Alvarez, DDS—1993–1994
• Jeffrey R. Prinsell, DMD, MD—1994–1995
• Robert R. Rogers, DMD—1995–1996
• Lawrence I. Barsh, DMD—1996–1997
• Kenneth Hilsen, DDS—1997–1998
• Dennis R Bailey, DDS—1998–1999
• Robert R. Rogers, DMD—1999–2000
• Donald A. Pantino, DDS—2000–2002
• Harold A. Smith, DDS—2002–2004
• Kent E. Moore, DDS, MD—2004–2006
• Jeffrey R. Prinsell, DMD, MD—2006–2008
• Jeffrey P. Pancer, DDS—2008–2010
• Sheri Katz, DDS—2010–2012
• B. Gail Demko, DMD—2012–2014
CITATION
Rogers RR, Remmers J, Lowe AA, Cistulli PA, Prinsell J, Pantino D, Rogers MB. History of dental sleep medicine. Journal of Dental Sleep Medicine 2014;1(1):67–74.REFERENCES
2. Cartwright RD, Samelson CF. The effects of a nonsurgical treatment for obstructive sleep apnea. The tongue-retaining device. JAMA 1982;248:705-9.
3. Schmidt-Nowara W, Lowe A, Wiegand L, Cartwright R, Perez-Guerra F, Menn S. Oral appliances for the treatment of snoring and obstructive sleep apnea: a review. Sleep 1995;18:501-10.
4. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances. American Sleep Disorders Association. Sleep 1995;18:511-3.
5. Ferguson KA, Cartwright R, Rogers R, Schmidt-Nowara W. Oral appliances for snoring and obstructive sleep apnea: a review. Sleep 2006;29:244-62.
6. Kushida CA, Morgenthaler TI, Littner MR, et al. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances: an update for 2005. Sleep 2006;29:240-3.
7. Epstein LJ, Kristo D, Strollo PJ Jr., et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med 2009;5:263-76.
8. Sauerland EK, Mitchell SP. Electromyographic activity of the human Genioglossus muscle in response to respiration and to positional changes of the head. Bull Los Angeles Neurol Soc 1970;35:69-73.
9. Sauerland EK, Harper RM. The human tongue during sleep: electromyographic activity of the genioglossus muscle. Exp Neurol 1976;51:160-70.
10. Remmers JE, deGroot WJ, Sauerland EK, Anch AM. Pathogenesis of upper airway occlusion during sleep. J Appl Physiol Respir Environ Exerc Physiol 1978;44:931-8.
11. Clark GT, Arand D, Chung E, Tong D. Effect of anterior mandibular positioning on obstructive sleep apnea. Am Rev Respir Dis 1993;147:62Q.
12. Walker-Engstrom ML, Tegelberg A, Wilhelmsson B, Ringqvist I. 4-year follow-up of treatment with dental appliance or uvulopalatopharyngoplasty in patients with obstructive sleep apnea: a randomized study. Chest 2002;121:739-46.
13. Hoekema A, Stegenga B, Wijkstra PJ, van der Hoeven JH, Meinesz AF, de Bont LG. Obstructive sleep apnea therapy. J Dent Res 2008;87:882-7.
14. Ferguson KA, Ono T, Lowe AA, Keenan SP, Fleetham JA. A randomized crossover study of an oral appliance vs nasal-continuous positive airway pressure in the treatment of mild-moderate obstructive sleep apnea. Chest 1996;109:1269-75.
15. Marklund M, Stenlund H, Franklin KA. Mandibular advancement devices in 630 men and women with obstructive sleep apnea and snoring: tolerability and predictors of treatment success. Chest 2004;125:1270-8.
16. Tsuiki S, Kobayashi M, Namba K, et al. Optimal positive airway pressure predicts oral appliance response to sleep apnoea. Eur Respir J 2010;35:1098-105.
17. Dort LC, Hadjuk E, Remmers JE. Mandibular advancement and obstructive sleep apnoea: a method for determining effective mandibular protrusion. Eur Respir J 2006;27:1003-9.
18. Remmers J, Charkhandeh S, Grosse J, et al. Remotely controlled mandibular protrusion during sleep predicts therapeutic success with oral appliances in patients with obstructive sleep apnea. Sleep 2013;36:1517-25, 25A.
19. Robin P. Demonstration pratique sur la construction et la mise enbouche d’un Nouvelle appareil de redressement. Revue de Stomatologie 1902;9:561-90.
20. Robin P. Glossoptosis due to atresia and hypotrophy of the mandible. Am J Dis Child 1934;48:541-47.
21. Meier-Ewert K, Brosig B. Treatment of sleep apnea by prosthetic mandibular advancement. In: Peter H, Podszus T, von Wichert P, eds. Sleep related disorders and internal diseases. Springer, 1987:341-45.
22. Clark GT, Blumenfeld I, Yoffe N, Peled E, Lavie P. A crossover study comparing the efficacy of continuous positive airway pressure with anterior mandibular positioning devices on patients with obstructive sleep apnea. Chest 1996;109:1477-83.
23. Mehta A, Qian J, Petocz P, Darendeliler MA, Cistulli PA. A randomized, controlled study of a mandibular advancement splint for obstructive sleep apnea. Am J Respir Crit Care Med 2001;163:1457-61.
24. Cistulli PA, Ferguson KA, Lowe A. Oral appliances for sleep-disordered breathing. In: Kryger MH, Roth T, Dement WC, eds. Principles and practice of sleep medicine. Elsevier Saunders, 2011:1261-77.
25. Gotsopoulos H, Kelly JJ, Cistulli PA. Oral appliance therapy reduces blood pressure in obstructive sleep apnea: a randomized, controlled trial. Sleep 2004;27:934-41.
26. Itzhaki S, Dorchin H, Clark G, Lavie L, Lavie P, Pillar G. The effects of 1-year treatment with a herbst mandibular advancement splint on obstructive sleep apnea, oxidative stress, and endothelial function. Chest 2007;131:740-9.
27. Marklund M, Sahlin C, Stenlund H, Persson M, Franklin KA. Mandibular advancement device in patients with obstructive sleep apnea: long-term effects on apnea and sleep. Chest 2001;120:162-9.
28. Lim J, Lasserson TJ, Fleetham J, Wright J. Oral appliances for obstructive sleep apnoea. Cochrane Database Syst Rev 2004:CD004435.
29. Phillips CL, Grunstein RR, Darendeliler MA, et al. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea: a randomized controlled trial. Am J Respir Crit Care Med 2013;187:879-87.
30. Aurora RN, Casey KR, Kristo D, et al. Practice parameters for the surgical modifications of the upper airway for obstructive sleep apnea in adults. Sleep 2010;33:1408-13.
31. Riley RW, Powell NB, Guilleminault C. Obstructive sleep apnea syndrome: a review of 306 consecutively treated surgical patients. Otolaryngol Head Neck Surg 1993;108:117-25.
32. Prinsell JR. Maxillomandibular advancement surgery in a site-specific treatment approach for obstructive sleep apnea in 50 consecutive patients. Chest 1999;116:1519-29.
33. Prinsell JR. Primary and secondary telegnathic maxillomandibular advancement, with or without adjunctive procedures, for obstructive sleep apnea in adults: a literature review and treatment recommendations. J Oral Maxillofac Surg 2012;70:1659-77.
34. Caples SM, Rowley JA, Prinsell JR, et al. Surgical modifications of the upper airway for obstructive sleep apnea in adults: a systematic review and meta-analysis. Sleep 2010;33:1396-407.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication February, 2014Accepted for publication February, 2014
Address correspondence to: Robert R Rogers, DMD, Pittsburgh Dental Sleep Medicine, PC, 11676 Perry Highway, Building III, Suite 3201, Wexford, PA 15090, Tel: (724) 935-6670; Fax: (724) 935-6758; E-mail: rrogers@pghdsm.com
DISCLOSURE STATEMENT
This was not an industry supported study. Dr. Cistulli is a chief investigator on sponsored clinical trials in obstructive sleep apnea for ResMed Inc and Exploramed Inc. His department receives equipment support for oral appliance research from SomnoMed Ltd, and he has a pecuniary interest in the company from previous involvement in product development. He is a medical advisor to Exploramed Inc (a US medical device incubator) and Zephyr Sleep Technologies. He has received speaker fees / travel support from ResMed Inc Fisher & Paykel Healthcare. The other authors have indicated no financial conflicts of interest.
PDF