Special Article 3, Issue 1.1
Sleep Medicine Education in US and Canadian Dental Schools: A Report of the Inaugural Dental Educators Conference at the University of North Carolina School of Dentistry
http://dx.doi.org/10.15331/jdsm.3742
Rose D. Sheats, DMD, MPH1 ; Gregory K. Essick, DDS, PhD2
1Department of Orthodontics, and 2 Department of Prosthodontics and Regional Center for Neurosensory Disorders, University of North Carolina School of Dentistry, Chapel Hill, NC
EXECUTIVE SUMMARY
The University of North Carolina School of Dentistry hosted the first ever national dental educators conference to gain an understanding of the current status of sleep medicine education in US and Canadian dental schools. “Sleep Disordered Breathing in Dental School Education: Past, Present, and Future” took place in Chapel Hill, NC, on August 24-25, 2013, and was partially supported by the American Academy of Dental Sleep Medicine, the Dean of the University of North Carolina School of Dentistry, and the Dental Foundation of North Carolina. Commercial vendors with an interest in sleep medicine provided support via educational grants or exhibitor fees.
The objectives of the conference were to:
- Describe the need to provide education in sleep disordered breathing to predoctoral and advanced dental education students, dental hygiene students, and other health care providers;
- Compare and contrast models currently used in US or Canadian dental schools that provide education in sleep disordered breathing;
- Provide recommendations for educational content of sleep disordered breathing curricular initiatives;
- Discuss strategies for implementation of clinical training in provision of oral appliances for patients with sleep disordered breathing;
- Develop lists of available teaching materials to assist with curriculum development in dental sleep medicine.
CONFERENCE STRUCTURE
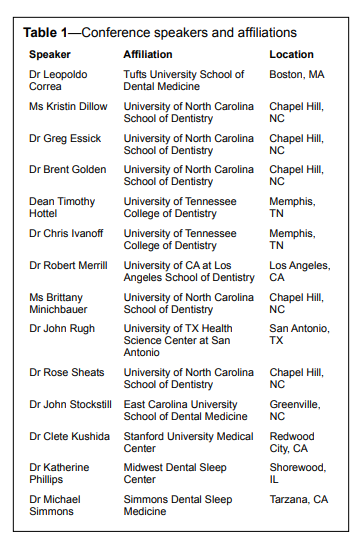
While conference promotion was targeted to dental school administrators and faculty of all 57 public and private US and 10 Canadian dental schools, it was nonetheless open to private dental practitioners and other health care providers with an interest in the education of dental students and dental hygienists in sleep medicine. A total of 70 attendees participated, with over half representing 21 dental schools in the US, 3 in Canada, and 1 in India. Other attendees included 4 physicians as well as dentists in private practice, including one from Spain. Five dental school deans attended, including one dean each from Canada and India. Some dental schools sent more than one representative.
The format of the conference consisted of 1.5 days of invited speakers who presented information on sleep medicine education in 1 of 3 half-day sessions each: predoctoral education, advanced dental education programs, and integration of oral health care providers and medicine. Speakers were mainly from academia and included 2 dental school deans and one physician. At the conclusion of each session, open floor discussions were held to solicit comments from conference participants. Open floor discussions were recorded in their entirety but are presented in a summary format below.
KEY FINDINGS AND RECOMMENDATIONS
It was widely recognized that dental schools currently are not meeting the educational needs of their students with respect to education in sleep medicine. Although most dental schools provide a few hours of instruction in sleep medicine to predoctoral and/or postdoctoral students, only a few dental schools at present have an established curriculum. A few schools have, or are, developing programs that aim to teach predoctoral students the pathophysiology and epidemiology of sleep disorders; how to screen, advise and refer patients at risk for SDB to sleep physicians for evaluation; and how to refer patients who are candidates for oral appliance therapy to dental clinicians with advanced training in sleep medicine. Some schools additionally offer clinical training in oral appliance therapy to select advanced education in general dentistry students, particularly those training in orofacial pain programs. There was no report of predoctoral students currently being trained to a level of competency in oral appliance therapy for sleep disordered breathing. Residency training in oral and maxillofacial surgery includes soft and hard tissue procedures to improve airway patency.Considerable discussion centered around both the feasibility and desirability of providing sufficient didactic and clinical experience in the predoctoral curriculum to enable a dental graduate to participate collaboratively with their medical colleagues in providing oral appliance therapy. There was no consensus about the extent of sleep medicine education that should be provided in predoctoral dental education curricula, especially with respect to clinical experiences and level of competency. Some participants expressed the opinion that oral appliance therapy should be limited to individuals with advanced training in orofacial pain.
Only a few schools appear to have dedicated resources for sleep medicine education. Presenters from these schools described laudable established or developing programs that included continuing education for dentists in practice as well as training for pre- and postdoctoral students. However, in other schools represented, time constraints within the predoctoral curriculum, lack of administrative support, and insufficient faculty expertise were identified as the most significant challenges to the implementation of education programs in sleep medicine. It was argued that individual faculty in these schools must initiate efforts to establish programs in sleep medicine, but these were unlikely to succeed without the full endorsement and financial and administrative support from the dean.
Strong support was voiced for planning follow-up conferences to focus on unresolved issues. Some participants recommended inclusion of even more stakeholders, such as representatives of the American Dental Education Association, the Commission on Dental Accreditation, and the Joint Commission on National Dental Examinations in decisions regarding sleep medicine education in our dental schools. Although the University of North Carolina was urged to plan the next conference, UNC organizers encouraged other dental schools to share leadership in this regard as well.
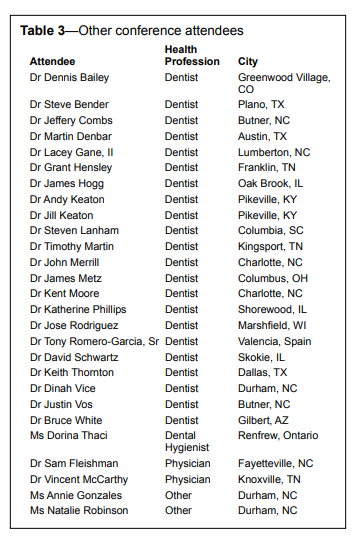
Table 1 lists the speakers who presented at this conference. Table 2 tabulates the dental schools that were represented and the attending faculty who had full- or part-time appointments. Table 3 lists remaining attendees and their expertise to provide insight into the breadth of interest in this important conference.
Table 1Conference speakers and affiliations |
{kind=link}
Table 2Academic centers represented |
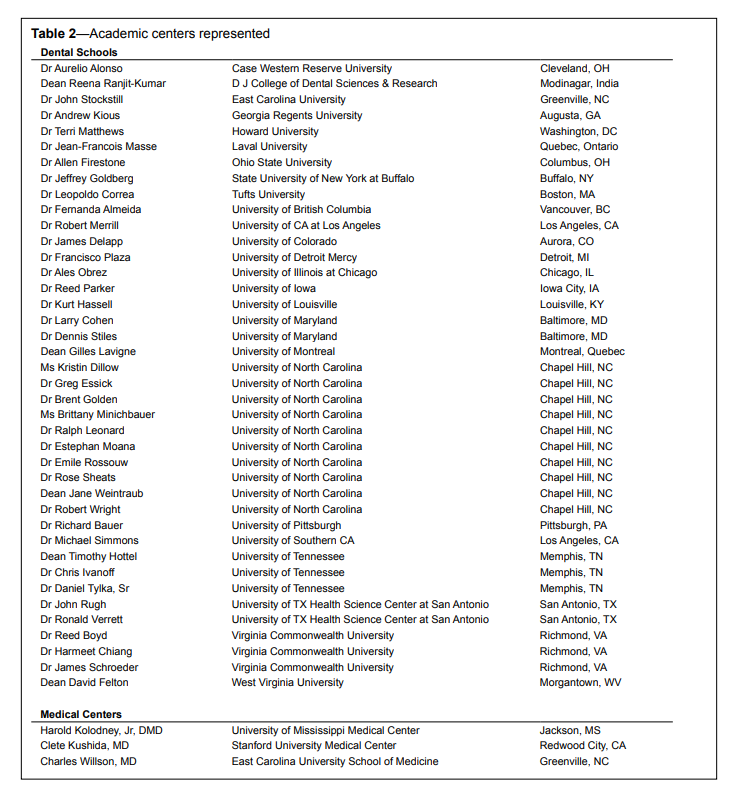{kind=link}
Table 3Other conference attendees |
{kind=link}
SUMMARY OF SESSION PRESENTATIONS
Saturday Aug 24, 2013 – Morning Session: Dental Sleep Medicine in Predoctoral Programs
Historical Perspective and Current Status of Dental Sleep Medicine Education in US Dental Schools
Michael Simmons, DMD, Lecturer, University of California at Los Angeles; Clinical Assistant Professor, Ostrow School of Dentistry; Director, Simmons Dental Sleep Medicine, Tarzana, CAA broad overview of the need for, and evolution of, sleep medicine care in the United States, including the emerging role of dental professionals was provided. To summarize the current status of dental sleep education in US dental schools, four questions were posed and evidence was offered to answer them:
- How has dental sleep medicine (DSM) evolved in the past? (see Endnote 1)
- Where is DSM at present both in numbers of experts and education provided in the DDS programs as compared to our medical peers’ training?
- Who are the DSM experts and educators at this time?
- Why should dentistry care about sleep medicine?
Additional unanswered questions for conference consideration were also proposed, including:
- Who should teach DSM?
- What should be taught?
- Who should it be taught to?
- How should teaching be tested, validated, and credentialed?
- What is to be the legacy of DSM teaching?
Subsequent to a 1988 Congressional investigation into the impact of sleep disorders in the US, both medicine and dentistry have grappled for 25 years with the challenges issued to health care professionals. The report ensuing from that landmark investigation exhorted health care professionals to increase the number of sleep medicine experts; to validate experts via training, testing, credentialing, and accreditation of their facilities; and to increase predoctoral university educational hours in topics of sleep.
Currently both medicine and dentistry include approximately 3 hours of sleep medicine education in predoctoral university programs. Dentistry is increasing these educational hours more rapidly than medicine and focuses on sleep disordered breathing and the sleep related movement disorder of sleep bruxism. The growth in membership rosters in dental sleep medicine groups has been catching up with their medical counterparts, such that over the past 15 years, the ratios of dental to medical sleep academy members have evolved from 1:10 to the current ratio of 1:3.
Several groups that have potential to impact the teaching of DSM in dental schools include the American Dental Education Association (ADEA), the Commission on Dental Accreditation (CODA), General Practice Residencies, Advanced Education Programs in General Dentistry, university pre- and postdoctoral programs, non-profit and for-profit academies including industry sponsored courses, and even massive open online courses (MOOCs). ADEA’s Commission on Change and Innovation appears to be an appropriate access point for encouraging or supporting the incorporation of DSM into dental school curricula, as such an agenda is consistent with this Commission’s goals and objectives.
Clarifications of specific terms in evolving DSM documents were discussed. Because of the different ramifications of various terms, careful consideration must be given to the use of such terms as “accreditation” compared to “credentialing,” “protocols” compared to “guidelines” or “recommendations,” “novice” versus “advanced beginner,” “competent,” “proficient” or “expert” practitioner, and finally “policy statements” versus “white papers.”
Proposed reasons that the field of dental sleep medicine should be actively engaged in the educational process included the ongoing and still unaddressed findings of the 1988 Congressional investigation, an obligation as health care professionals, and especially because currently dentists have some of the best solutions to the ongoing challenges. A model was suggested, based on Alan Pack’s 2011 editorial on a similar topic (Sleep Medicine: Strategies for change. Journal of Clinical Sleep Medicine: Vol. 7, No. 6), that described the 8 steps required to transform the current model of limited dental school education devoted to DSM. The 8 steps progressed from establishing a sense of urgency → forming a powerful guiding coalition → creating a vision → communicating the vision → empowering others to act on the vision → planning and creating short-term wins → consolidating improvements and producing more change → institutionalizing new approaches.
Conference participants were exhorted to focus on “asking the right questions” in order to ensure the future of dental sleep medicine.
University of Tennessee College of Dentistry Vision and Model for Dental Sleep Medicine Education
Chris S. Ivanoff, DDS, Associate Professor, and Timothy L. Hottel, DDS, MS, MBA, Dean, University of Tennessee College of Dentistry, Memphis, TN
A review of protocols and practices at the University of Tennessee College of Dentistry revealed that dental patients were not being queried about sleep disorders, screened for sleep disordered breathing, or treated with oral appliances that improve sleep respiration. This recognition led to a progressive plan of dental sleep medicine education that includes: the institution of a school-wide sleep disorders screening program, changes in the predoctoral curriculum during all 4 years of predoctoral education, establishment of research protocols and continuing education for practicing dentists, recruitment of new faculty trained in dental sleep medicine, and remodeling of space for dedication to the treatment of patients with sleep disordered breathing.
The mission to increase student competency in dental sleep medicine begins during Phase I of the predoctoral program. By providing basic knowledge and skills during the early basic science, occlusion, and TMD/Sleep Medicine courses, students are enabled by traditional didactics (6 h) to screen for OSA more effectively when taking patients’ medical history. Lessons include basic concepts, terminology, the pathophysiology of sleep medicine as it relates to dentistry, and understanding of screening tools such as the Epworth Sleepiness Scale.
Phase II strategizes to prepare students to respond more effectively after OSA patients have been screened. Building on basic knowledge acquired during Phase I, the aim of Phase II is to prepare students with better multidisciplinary communication skills to effectively conduct a professional consultation with medical reviewers and polysomnography technicians for appropriate referral. Proposed additions to the curriculum that are expected to be implemented soon include (1) one 3-h shadowing rotation in a sleep clinic; (2) one 3-h lab in which students pair up to take protrusive records and fabricate a sleep appliance on each other; and (3) one 3-h problem-based learning session led by a multidisciplinary group to review sample cases or summary reports by a medical reviewer. The expectation is that these curriculum enhancements will reinforce all the principles learned in the TMD/Sleep Medicine Course.
Phase III aims to engage students after referral, by shadowing credentialed faculty in the Craniofacial Pain/Sleep Disordered Breathing Clinic, adding depth to student understanding of the clinical features and diagnosis of OSA as well as current dental and medical therapies.
Phase IV presses further by extending continued education to practicing dentists through symposia that bring together dental and medical sleep experts, e.g., “The Meeting of the Minds” Symposium held on June 7-8, 2013. By providing opportunities to discuss topics ranging from screening to complex patient cases, Phase IV aims to build bridges between dentists and their medical colleagues.
An underlying premise of the University of Tennessee model is that basic acquisition of the language of polysomnography will enable students to screen for OSA better and to participate as functioning members of a multidisciplinary team to diagnose and treatment plan OSA patients. Increased research opportunities are also anticipated to provide another dimension to actively engage students in dental sleep medicine. It is important to note that the proposed strategies will allow students to become involved in the treatment of OSA in a manner that does not violate AASM and AADSM standards of care.
Dean Hottel challenged dental school leadership, especially Deans, to recognize that they must make the commitment to sleep medicine education in the dental school environment if the field is to flourish and remain within control of the dental community. Such leadership however obligates them to dedicate faculty resources and clinical space to enable appropriate didactic and clinical education for students. His boldness has led to hiring 2 full-time dental faculty members dedicated to this vision who have expertise in sleep medicine and board certification in TMD/orofacial pain. He is also renovating 1,300 sq ft of clinical space to tailor to the practice of dental sleep medicine. When a new 40,000 sq ft clinical addition to the dental school is completed, more space will be devoted to dental sleep medicine. The College of Dentistry is anticipating developing a postgraduate program in orofacial pain in the future.
The College is reaching out to its medical sleep colleagues and establishing interactions with the medical sleep fellowship program, developing research protocols, and providing continuing education opportunities for dentists. These actions have clearly reinforced the need for a strong presence in dental sleep medicine education in dental schools, and have set a standard of commitment for other schools to follow.
Physicians realize that oral appliance therapy is a viable therapeutic option for patients diagnosed with sleep disordered breathing. The Dean reported being warned that if dentists do not provide this treatment modality, physicians will. It is incumbent on dental school educators to ensure that their graduates are provided the foundation in sleep medicine to become competent to meet the growing demand for oral appliance therapy.
Dental Sleep Medicine at the University of North Carolina School of Dentistry
Rose D. Sheats, DMD, MPH, Affiliate Associate Professor, University of North Carolina School of Dentistry, Chapel Hill, NCInterest in sleep medicine education, research and patient care at the University of North Carolina School of Dentistry has grown greatly over the past 5 years, providing in part the motivation for this conference. Strategies to respond to the increasing number of inquiries and requests by students, faculty, patients and practicing dentists in NC have been proposed and are under administrative review. Present activities depend largely on innovative use of existing resources allocated to other programs at the school.
Currently, sleep medicine teaching encompasses a total of about 16 hours, more than half of which is provided in advanced dental education programs in orthodontics, pediatric dentistry, and oral and maxillofacial surgery. Occasional lectures are provided to students in advanced education in general dentistry and the prosthodontics residency programs. Despite providing educational hours in sleep medicine greater than the average of all US dental schools, the teaching at UNC is fragmented, overlapping, and not coordinated among the 3 faculty members from different departments who provide this education. Predoctoral dental and dental hygiene students receive 3 and 2 hours, respectively, of didactic education in separate offerings. No clinical or laboratory experience is provided in any pre- or postdoctoral program. An increasing number of graduate students are requesting research opportunities in sleep medicine in fulfillment of their thesis requirements. These requests are being met. Patients from students and residents who seek oral appliances, or are referred for oral appliance therapy by their physicians, are transferred for treatment in the faculty practice. Continuing education lectures in sleep medicine to dentists in practice in North Carolina are provided by the same faculty.
Dental students and directors of advanced education programs desire an opportunity for clinical experience in providing oral appliance therapy for their patients diagnosed with sleep disordered breathing. However, the lack of clinical faculty charged with didactic and clinical education responsibilities in dental sleep medicine, the absence of administrative expertise/support for medical insurance billing, administrative policy that prevents resident training in the dental faculty sleep medicine practice, and insufficient clinical resources including dedicated space for the practice of dental sleep medicine constitute current barriers to expanding this aspect of dental education in the UNC curriculum. Emerging programs in sleep medicine at other dental schools likely face very similar barriers, and solutions are sorely needed.
Recommendations to prepare graduates of the UNC School of Dentistry with a foundation in sleep medicine and clinical experience in provision of oral appliance therapy (OAT) include:
- Establishment of an administrative home for dental sleep medicine that will facilitate:
- Coordination of didactic teaching to increase the amount of information provided, to minimize redundancies, and to more equitably distribute the burden on the limited number of faculty experts currently available at the School;
- Creation of a didactic and clinical curriculum in sleep medicine for fellows in the orofacial pain program that would be available on an elective basis to residents in other advanced dental education programs
- Development of a predoctoral, one-hour weekly didactic elective as a prerequisite to obtaining clinical experience in OAT;
- Dedication of clinical space and equipment to evaluate and treat patients referred for OAT by medical colleagues;
- Administrative support of faculty experts to supervise predoctoral and advanced education student clinics devoted to OAT;
- Development and implementation of a financial model based in part on medical insurance reimbursement that covers the cost of care delivery and enables the educational program to grow; and
- Encouragement of faculty and students at all levels to explore research opportunities in sleep medicine at the School of Dentistry or adjacent health professional schools.
Surgical Aspects of Sleep Medicine in Dental School Curriculum
Brent Golden, DDS, MD, Clinical Assistant Professor, University of North Carolina School of Dentistry, Chapel Hill, NCSurgical treatment of sleep apnea is a key component of board certification for American oral and maxillofacial surgeons, and is therefore a core component of resident education throughout their training. On the other hand, predoctoral students are educated by surgery faculty only to a level of exposure with very little expanded discussion of surgical therapy.
Oral and maxillofacial surgeons are highly experienced in the diagnosis and surgical management of skeletal and soft tissue disproportion in the face and neck. These principles and surgical techniques have been demonstrated to be effective in modifying anatomic abnormalities that contribute to narrowing or obstruction of the airway at multiple levels.
Maxillomandibular advancement (MMA) surgery can address anatomic abnormalities in all the anatomic regions of the head and neck; only tracheostomy is more comprehensive. MMA surgery can have a direct or indirect effect on the nasal valve, nasal septum, nasal turbinates, palate, tongue, tonsillar pillar region, hyoid bone, and pharynx.
Maxillomandibular advancement as a primary or secondary treatment is a successful, safe, single-stage surgical intervention for clinically significant OSA with a therapeutic efficacy comparable to nasal CPAP. Oral and maxillofacial surgeons are uniquely qualified to provide this safe and effective option and should be a part of any comprehensive, multidisciplinary sleep disorder team.
Dental education should provide predoctoral dental students exposure to surgical aspects of treatment for sleep disordered breathing, such that they understand the indications for referral.
What I Wish Dental School Had Taught Me about Dental Sleep Medicine
Katherine S. Phillips, DDS, Dental Director, Midwest Dental Sleep Center, Chicago, ILOn the heels of graduating from dental school in 2008, this speaker was invited to join a dental practice which limited its practice to the provision of oral appliance therapy for sleep disordered breathing. She was ignorant of the fundamentals of sleep medicine and noted with regret that her dental education did not prepare her with an understanding of the medical significance of this condition and the role that dentists can play in its management.
In recognition of the paradigm shift in dentistry away from cottage industry to integration with medicine, sleep medicine in dentistry is well positioned to exploit this growing trend. Parallels can be drawn to the role of dentists in screening and referring for oral cancer, hypertension, diabetes, the effect of medications on the stomatognathic system, and a host of other medical conditions. With a prevalence as great as asthma and type 2 diabetes, dentists are in a unique position not only to screen for patients with sleep disordered breathing but also to provide first- and second-line therapy in collaboration with their medical colleagues whose role is to diagnose the condition and provide or refer for appropriate treatment.
Dental disciplines which overlap fundamentals of sleep medicine in dentistry include but are not limited to Physiology, Pathology, Temporomandibular Joint Disorders, Pharmacology, Oral Medicine/Oral Diagnosis, Physical Assessment, Pediatric Dentistry, Orthodontics, and Human Growth and Development.
Graduates of dental school predoctoral programs would be well served if they were educated in the following areas of sleep medicine:
- medical history and screening for risk for sleep disordered breathing (SDB);
- extra- and intra-oral clinical findings strongly associated with risk for SDB, including jaw relationships, soft tissue and dental findings, and temporomandibular joint findings;
- education in the specific examination of pediatric, TMD, and pain patients who may be at risk for SDB;
- the fundamentals of oral appliance therapy and its side effects and management;
- appropriate appliance selection, differences in design features, and rationale for selecting design features; and
- appliance delivery, adjustment, and troubleshooting issues with oral appliances.
Open Floor Discussion: How Much Dental Sleep Medicine Should Be Taught To Predoctoral Dental Students?
Discussion was initiated with the exhortation that predoctoral dental students be educated minimally in the medical significance of untreated sleep disordered breathing, the benefits of oral appliance therapy (OAT), and the certainty that occlusal and skeletal changes will occur from treatment. In some instances, dentists are our own worst enemy when, in their lack of an overall understanding of this medical condition, they advise that OAT be discontinued due to unfavorable changes in the occlusion.
Recurrent themes of the Predoctoral Education Open Floor Discussion included the following:
- At minimum predoctoral dental students should be educated in the screening for and understanding of consequences of untreated sleep disordered breathing in their patients.
- Rather than creating separate courses in sleep medicine, predoctoral dental students should be introduced to the condition across several dental disciplines, including but not limited to anatomy, physiology, pathology, oral maxillofacial surgery, oral medicine/oral pathology, and temporomandibular disorders. Even modest curricular modifications, however, require that individual course directors understand the need to educate students in sleep disordered breathing and coordinate efforts to make these changes across multiple courses.
- Dental educators must alter their thinking about “treatment” versus “management”. Many classic dental conditions such as caries can be “treated,” however chronic medical conditions such as sleep disordered breathing are not “treated” but rather “managed.”
- Appropriately educated dentists in sleep medicine have the skills to make a significant impact on the interdisciplinary management with their physician colleagues of affected patients.
- The American Dental Education Association (ADEA), as the “Voice” of dental education, should be included in the discussion of curricular modifications or transformations. Such involvement encompasses establishment of an ADEA Special Interest Group in sleep disordered breathing and creation of awareness of this ubiquitous condition at the dean’s level by the ADEA Council of Deans.
- The Joint Commission on National Dental Examinations is creating a new examination to replace Parts I and II. The Integrated National Board Dental Examination will seek to assess dental graduates’ ability to integrate the basic, behavioral, and clinical sciences to judge entry level competency in dentistry. As such, it will behoove dental school educators to provide a more integrated approach to teaching fundamental principles of dentistry. Sleep disordered breathing offers an ideal model for across-the-board blending of classic dental courses and clinical relevance.
- Sleep disordered breathing is a chronic and costly medical condition with significant public health ramifications. It affects 1 in 5 Americans with burdensome social, economic and health impacts. As such, it creates an extraordinary opportunity to integrate dentistry and oral health into a primary health care model that is increasingly focusing on the integration of all health care professional education. Team-based and collaborative approaches to health care delivery with emphasis on fiscal responsibility and outcomes assessments are becoming the cornerstone of the future of health care.
- Dental school based sleep medicine research should be strongly encouraged to:
- demonstrate the engagement of dentists in the field of sleep medicine beyond the delivery of care;
- provide greater awareness to the dental and medical community of the role and responsibility of dentists to more actively participate in the management of patients with sleep disordered breathing; and
- emphasize to students in all dental programs the importance of sleep medicine to the overall health of patients.
Saturday Aug 24, 2013 – Afternoon: Integrating Oral Health Providers and Medicine
Sleep Bruxism and Sleep Disordered Breathing: What and Why We Should Teach to Undergraduate Dental Students?
Gilles Lavigne, DMD, FRCD (Oral medicine), PhD, hc (U Zurich) Professor and Dean, Faculty of Dental Medicine, Universite de Montreal Canada Research Chair in pain, sleep and traumaAt the Faculty of Dental Medicine of the University of Montreal, sleep and pain dental medicine have been integrated into the education of undergraduate dental students in every year. Relevant material is included in basic science (physiology and neuroscience, psychology), oral medicine, occlusion splints, and orthodontics courses. In the final year, a 15-h series of lectures provides a foundation in sleep medicine by covering the following topics:
- Review of sleep physiology, the neuroscience of pain and behavioral components related to both
- Definitions, classification, and epidemiology of sleep disorders including: sleep disordered breathing, sleep bruxism, gastroesophageal reflux disease and xerostomia during sleep, insomnia, periodic limb movements, REM behavior disorders (RBD), sleep and pain (TMD, neuropathic pain)
- Risk factors and psychosocial causes
- Patient interview and clinical examination
- Differential diagnosis (before and after tests)
- Tools and tests (validity, sensitivity, specificity): including imaging studies and polysomnography (home or in-lab; full or limited number of channels)
- Who is conducting the sleep studies: technician under medical supervision?
- Interpretation and limitation of sleep studies
- If insomnia, sleep disordered breathing, or sleep movement disorders are suspected, need for appropriate referral to medical sleep clinics, ENT, neurology and/or psychology
- Pathophysiology overview
- “Management” of sleep disordered breathing with clarification that the term “treatment” is a misnomer since it suggests “curing” the condition. Students are educated in the following sequential approach to management:
- Counseling (sleep habits, sleep schedule, sleep position, time of food intake, time of exercise)
- Cognitive behavioral treatment (CBT) and physical/psychotherapy referrals
- Prescription (start with simple over-the-counter medication to more powerful medications/RISK assessments and medical partnership)
- Overview of various oral appliances, sleep aids (sleep positioning device/back cushion, sleep position alerting devices, etc.)
- Surgical and orthodontics treatment options
- Follow-up protocol: 1 to 6 months with emphasis that medical collaboration is mandatory if diagnosis of obstructive sleep apnea was made
In summary, the dental school curriculum of one Canadian dental school provides a foundation in sleep medicine education that enables its graduates to participate in screening, recognition of risk factors, and collaboration with a sleep team to diagnose and manage their patients with obstructive sleep apnea.
Teaching Dental Sleep Medicine in an Evidence Based Practice and Research Methods Course
John D. Rugh, PhD, Professor, University of Texas Health Sciences Center Dental School at San Antonio, TXDental sleep medicine was introduced into the dental predoctoral, residency, and faculty development programs at San Antonio in the context of an Evidence-Based Practice (EBP) and Clinical Research Elective Course. The inspiration for the course came from a grant funded by PHS/HRSA D86HP24480.
Forty-eight participants applied newly learned evidencebased practice, research, and critical thinking skills to the epidemiology, etiology, diagnosis, and management of obstructive sleep apnea. This one-semester, 32-h course employed teambased learning strategies. Dental students (n = 12), dental residents (n = 13), dental faculty (n = 13), dental hygiene faculty (n = 3), and dental practitioners (n = 7) were assigned to 7 teams. During the semester these 7 teams engaged in multiple team problem-solving exercises and projects including: (1) the design of a National Practice-Based Research Network research protocol on extraction orthodontics and OSA; (2) an OSA screening program for dental continuing education courses; and (3) the writing and publication of 36 critically appraised topics (CATs) related to OSA in the UTHSCSA CATs Online Library (https://cats.uthscsa.edu/). These CATs have now been indexed on the British Trip Database (http://www.tripdatabase. com/). Course activities included students recording their sleep O2 values with wrist oximeters. Thirteen faculty from dentistry, medicine, basic sciences, and the library provided instruction and mentoring of the team projects.
Course evaluations and learning outcome measures were extremely positive. Participants were particularly pleased to be able to apply their newly learned EBP and research skills to the exciting new clinical area of sleep apnea. The team-based learning methods were very popular with the students and faculty but were found to be labor intensive for the faculty in comparison to the traditional lecture format. However, given the course’s popularity and very positive evaluations, the course is scheduled again next year using the same focus on OSA and team-based learning methodology.
What Role Can Dental Hygienists Play?
Kristin Dillow, BSDH; Brittany Minichbauer, BSDH, Master’s Candidates in Dental Hygiene Education, University of North Carolina School of Dentistry, Chapel Hill, NCDental hygienists are on the front line regarding prevention and counseling. They perform patient oral cancer screenings, tobacco cessation guidance, nutritional counseling and extraoral examinations. While dental hygienists focus on oral health, they also assess and advise on the patient’s overall health.
Acutely aware of the detrimental effects of periodontitis, dental hygienists focus most of their daily clinical activities on preventing and treating this disease. Current research, albeit limited to only a few studies since 2009, suggests an association between periodontitis and obstructive sleep apnea (OSA). With this recognition, treating periodontal disease is not limited to the oral cavity alone as it is important to consider also the possible presence of sleep related breathing disorders affecting the patient’s overall health.
Ideally, education in sleep medicine should be offered in the dental hygiene curriculum; however, it is unknown to what extent sleep medicine is being taught in these programs. To address this question, the presenter (B.M.) conducted a survey to assess sleep medicine education in dental hygiene programs nationwide (over 300 programs). Preliminary results from the survey indicate a lack of formal sleep medicine education in most dental hygiene curriculums. Sleep bruxism was the most commonly reported topic covered. However, dental hygiene faculty expressed an interest in learning more about sleep medicine, which is encouraging for future integration of sleep medicine into the curriculum.
It was argued that dental hygienists in clinical practice can play an important role in evaluating patients periodically for risk factors associated with sleep related breathing disorders such as OSA. However, there are presently no widely accepted algorithms for screening patients in the dental office, nor is it known how patients who screen at high risk will use this information. The presenter (K.D.) described a well-planned clinical study in which she is assessing how patients in a communitybased dental practice in Raleigh, NC, respond to OSA screening based on questionnaire and pulse oximetry, and whether those patients who screen at high risk for OSA follow up with their physician as recommended in the study.
The types of research described represent a first step in recognizing the dental hygienist’s role in a health care team dedicated to the identification and management of patients with sleep related breathing disorders.
Care Under One Roof Model
Gregory K. Essick, DDS, PhD, Professor, University of North Carolina School of Dentistry, Chapel Hill, NCIntegrating oral appliance therapy into the delivery of care for sleep related breathing disorders has been a challenge for dental and medical professionals alike. Because of separate offices with inadequate channels of between-office communication, different record keeping systems, different financial models, and different modes of care delivery, treatment is often fragmented with the possibility of the patient remaining untreated for long periods of time after diagnosis. A multidisciplinary care delivery model that integrates dental sleep medicine and sleep medicine under the same roof with educational and research components was proposed. In addition to providing a venue for the clinical cross-training of both dental and medical students and residents, the model offers distinct advantages to improved patient care, continuity of treatment, and the central coordination of clinical and insurance-related benefits.
The care-under-one-roof concept entails the co-treatment of patients with sleep disordered breathing in the same facility, by which sleep physicians and team are in face-to-face-contact with dental sleep faculty and team (assistants, residents, and dental and dental hygiene students) during diagnostic, treatment, and follow-up procedures. Working under the same roof guarantees continuity of care and facilitates protocols involving both medical and dental personnel that are presently difficult to implement from separate offices, e.g., adjustment of an oral appliance during a PSG sleep study or implementation of CPAP combined with oral appliance therapy.
The academic care-under-one-roof model is envisioned as a partnership between a university-based American Academy of Sleep Medicine (AASM)-accredited sleep disorders center and the dental school associated with the university. The center would be accredited by the AASM and would be supervised by a board certified sleep specialist, who would adhere to AASM practice parameters in the diagnosis and management of sleep disorders. The dental sleep medicine (DSM) program would be directed by a DSM trained dental faculty member, who would adhere to AASM practice parameters, American Academy of Dental Sleep Medicine (AADSM) protocols and evidence-based practices, all of which the trainees would experience and learn through their participation. The importance of periodic follow-up, compliance, side effects monitoring, and longitudinal outcomes assessment would be emphasized.
Educational opportunities associated with the care-under-oneroof model are envisioned to include:
- Weekly multidisciplinary conferences, a forum for cross-training of medical and dental personnel.
- (Hands-on) Rotations for dental residents, enabling practice of skills taught by dental and medical faculty.
- Grand rounds presentations by sleep physician fellows and dental residents, demonstrating their mastery of clinical care and supporting literature.
- Development of an education framework, for eventual extension into the predoctoral DDS and MD curricula of the schools and allied health professional curricula.
- Development of CE opportunities for physicians and dentists in private practice, sleep technologists, respiratory therapists, and other allied professionals.
A Role for Oral Appliance Therapy and Practice Parameters Update
Clete Kushida, MD, PhD, Professor, Stanford University Medical Center Medical Director, Stanford Sleep Medicine Center, Director, Stanford Center for Human Sleep ResearchThe predisposing factors and anatomic determinants of upper airway collapse in obstructive sleep apnea (OSA) patients were discussed. In particular, the contributions of obesity, neck girth, and craniofacial dysmorphism to the pathogenesis of OSA were described, including hereditary factors and candidate genes for both OSA and craniofacial dysmorphism. The contributions of bony and soft tissue structures to an abnormal upper airway were highlighted, as well as changes to the airway that occur with oral appliances.
Recent studies on oral appliances were summarized, such as airway imaging studies before and after use of oral appliances and patient preferences, expectations, and factors impacting OSA treatment choice. The current AASM oral appliance (OA) practice parameters were reviewed and questions such as oral appliances as second-line therapy to CPAP and upper airway surgery, OA indications for only mild-to-moderate OSA patients, and OA outcomes management were explored beyond the current OA practice parameters.
OSA mortality and cardiovascular risk were described, including studies that indicated changes in blood pressure with CPAP, upper airway surgery, and OAs. Other changes with OA treatment, such as sleepiness and cognition were discussed.
The Agency for Healthcare Research and Quality (AHRQ)- supported Comparative Outcomes Management with Electronic Data Technology (COMET) Study was described, particularly with respect to its comparative effectiveness trial comparing cardiovascular risk in patients with OSA randomized to CPAP or OAs. The Patient-Centered Outcomes Research Institute (PCORI)- supported Sustainable Methods, Algorithms, and Research Tools for Delivering Optimal Care Study (SMART DOCS) was also discussed, with relevance to its use of new technology, such as OA titration and adherence monitoring. Lastly, future directions and needs for research on oral appliances were considered.
Open Floor Discussion: How Can We Integrate Sleep Medicine/Professionals into Dental Sleep Medicine Training Programs?
While the original focus of the afternoon sessions was to examine opportunities or models to integrate dental and medical education in the management of sleep disordered breathing, the open floor discussion tended to be narrower in its breadth. The following points were made:- The “Care Under One Roof ” model still poses significant challenges because of the barriers to accessing or sharing a clinical record, whether dental or medical.
- Much support was expressed for the utilization of dental hygienists to participate in or assume the role of identifying patients at risk for sleep disordered breathing in private dental practices. Distinction was made between “identification” of at risk patients versus “screening” for at-risk patients as the latter implies use of a screening instrument (e.g., questionnaire, pulse oximeter).
- The pilot program at the University of Texas Health Sciences Center at San Antonio described by Dr. Rugh demonstrated potential demand for education in sleep medicine when an elective course that was offered at 7 AM on Monday mornings for an entire semester reached its registration limit before all demand was met. Although the course was billed as a research methodology course, it was advertised as using the model of sleep disordered breathing to teach research principles.
- One strategy to address the shortage of faculty with expertise in sleep disordered breathing included sharing of successful educational models from other institutions. Possibilities suggested were online learning modules or exchange of curricular content.
- Patient-centered care will mandate that more effective interactions be developed among medical sleep specialists, primary care physicians, and dentists in the realm of diagnosing and managing patients with sleep disordered breathing.
Sunday Aug 25, 2013 – Dental Sleep Medicine in Advanced Dental
Education Programs
Tufts School of Dental Medicine Model of Dental Sleep Medicine Education
Leopoldo P. Correa, BDS, MS, Associate Professor and Head of Dental Sleep Medicine Division, Department of Oral and Maxillofacial Pathology, Oral Medicine and Craniofacial Pain, Tufts University School of Dental Medicine, Boston, MAUnder the direction of Dr. Correa, a diplomate of the American Board of Dental Sleep Medicine, Tufts University School of Dental Medicine provides a comprehensive education program in dental sleep medicine that includes the following components:
- Predoctoral education of dental students
- Postdoctoral education of students in advanced education programs
- Education of dental hygiene students
- Mini-residency for dentists (Continuing Education)
- International training of dental students at their home schools
- Sleep fellowship collaboration with Tufts Medical Center
- Dental sleep medicine fellowship
Postdoctoral education is offered as an elective to the advanced dental education students. The elective course consists of 10 lecture sessions of 1.5 h each with rotations of a half-day in each of the Dental Sleep Clinic, the sleep laboratory, and the Department of Pulmonary, Critical Care and Sleep Medicine at Tufts Medical Center. Lecture sessions address the following topics:
Session 2: Psychiatric Disorders and Sleep Disturbances
Session 3: Medical Conditions Affecting Sleep
Session 4: Sleep Disorders Part I
Session 5: Sleep Disorders Part II
Session 6: Screening and Diagnosis of Sleep Disordered Breathing
Session 7: Assessment of Sleep Patients
Session 8: Sleep Bruxism
Session 9: Temporomandibular Disorder (TMD) and Sleep Disordered Breathing (SDB)
Session 10: Review of the Program and Final Written Examination
Education of students in the School of Dental Hygiene consists of one 2-h lecture on dental sleep medicine.
Tufts University School of Dental Medicine provides many continuing educational opportunities for dentists in private practice, the most extensive of which is the Mini-Residency Program. This program consists of 3 modules of on-site lecture and handson instruction over a period of 6 months. Each module provides 3 days of instruction, for a total of 9 days of training. The participants complete assignments between the modules.
As part of the dental sleep medicine teaching mission of Tufts University School of Dental Medicine, Dr. Correa frequently travels to Mexico to teach. Students in Monterrey follow a similar curriculum to what is offered to dental students at Tufts University.
Finally, 2 fellowship opportunities exist within the Dental Sleep Clinic at Tufts University School of Dental Medicine. One program enables physicians to rotate in the clinic and learn about dental sleep medicine (1 day per week for 3 months). The second program is a one-year full-time fellowship in Dental Sleep Medicine for dentists. This program focuses on the interactions of dental sleep medicine, sleep medicine, temporomandibular disorders, and the role of the dentist in the screening and treatment of sleep disorders. The clinical training includes performing a full dental, sleep, and TMD history including medical systems; examination of the head, face, and neck for assessing the anatomical and physiological structures related to airway; review and understanding of polysomnograms; and formulating and implementing an interdisciplinary treatment plan in conjunction with other medical providers.
The core of the teaching program at Tufts University School of Dental Medicine is the Dental Sleep Clinic, located in the Craniofacial Pain Center where approximately 30-35 patients are seen every week under Dr. Correa’s supervision. This clinic provides the opportunity to educate predoctoral dental and dental hygiene students, advanced dental education students, dentists and physicians in a collaborative and well-integrated environment.
American Academy of Oral Facial Pain Perspective: UCLA Program
Robert L. Merrill, DDS, MS, Clinical Professor and Director, Graduate Orofacial Pain Program, University of California at Los Angeles School of DentistryThe UCLA School of Dentistry Graduate Orofacial Pain Residency Program was the first orofacial pain program in the country to be accredited by the Commission on Dental Accreditation (CODA). This occurred in February and August of 2011. The Orofacial Pain (OFP) residency program was established in 1990 and now provides the home for training in sleep medicine in the dental school. The pain program first began receiving sleep referrals from UCLA Neurology and Pulmonary Medicine in 2004, and training of the residents in sleep medicine was expanded in 2006 under the direction of Dr. Dennis Bailey and Dr. Merrill. In 2008, a Sleep Mini-Residency program was developed to provide “in-depth and comprehensive training” in sleep medicine for dentists in practice (“Advanced Clinical Training” dentists). At the completion of the mini-residency, the dentist is prepared to competently treat patients with sleep related breathing disorders (SRBD).
The mini-residency consists of 5 Friday/Saturday sessions of on-site training over a period of 5 months. Physician colleagues from UCLA Neurology and Pulmonary Medicine provide lectures during the mini-residency, as well as referrals of patients to be treated in the OFP Clinic. OFP residents and Advanced Clinical Training (ACT) dentists attend all sessions of the Sleep Mini-Residency for the didactic aspect of their pain program (60 h). For the clinical phase of their training, the OFP residents and ACT dentists see SRBD patients in the OFP clinic under the guidance of the clinic attendings, including Drs. Bailey and Merrill.
Thirty percent (30%) of the patients treated in the OFP Clinic are sleep patients. The graduate training program is characterized by close collaboration with medical colleagues and is integrated into the medical center. The residents generate consultation letters and SOAP notes directly in the medical center’s EPIC medical record, as well as order and retrieve sleep studies, laboratory tests and imaging through the electronic medical record system. The sleep physicians support the use of home sleep testing devices for titrating the oral appliances when administered by the residents or ACT students prior to a followup PSG in the hospital’s sleep laboratory.
Dr. Merrill believes that education in oral appliance therapy as a component of sleep medicine education in dental schools should be (1) undertaken only by advanced general dentistry education programs in orofacial pain and (2) limited to advanced education residents and dentists trained to at least a minimum level of competency in orofacial pain and sleep medicine. He noted the commonly observed relationship between sleep and pain disorders and the responsibility of the dentist to refer patients with dual complaints of orofacial pain and poor sleep to a sleep center/laboratory for further evaluation for a sleep problem. Moreover, patients with SRBD who are referred to a dentist for management with an oral appliance should be expertly evaluated for orofacial pain prior to initiating treatment for the SRBD. The treating dentist must be capable of managing the temporomandibular pain that may result from progressive mandibular advancement.
At the present time sleep medicine is unlikely to be recognized by CODA as a specialty within general dentistry. However, CODA has set standards for training in sleep medicine within the standards for orofacial pain mandating education in sleep medicine as well as clinical experience in oral appliance therapy for SRBD. OFP programs are the logical place for sleep medicine because of the strong overlap between pain disorders and sleep disorders. Students of these programs are trained to perform complex head and neck neurological examinations, oropharyngeal/nasal airway examinations, and stomatognathic and musculoskeletal examinations, including a comprehensive evaluation of TMJ dysfunction.
Dr. Merrill argued that skills required for the treatment of sleep patients are not practical expectations for predoctoral dental students. He also noted that “CODA no longer requires TMD to be taught in dental schools…How can DDS students proceed to treat a sleep patient with an MAD that can complicate an existing TMD/OFP condition?” Additionally, treating SRBD patients with oral appliances requires close follow-up to manage problems that can occur with an appliance that advances the jaw. Undergraduate programs generally are not good at managing follow-up once the dental student has received credit for a procedure.
Predoctoral education in sleep medicine should follow the model used to expose predoctoral dental students to the OFP Clinic for care of complex TMD/orofacial pain disorders. Dental students whose patients are referred to them for oral appliance therapy should, in turn, refer the patient to the OFP/ oral medicine clinic for care and would benefit from observation of the management of and possibly limited participation in the patient’s care. Many aspects of patient care with oral appliance therapy do not fit well into a predoctoral dental program, e.g., home sleep test monitoring, appliance titration/adjustment over a 3-4 month period, and periodic follow-up visits for as long as the patient is being managed with OAT.
Dr. Merrill’s recommendation is that predoctoral programs include lectures on sleep medicine to broaden the awareness of the student regarding health issues of their patients. They should be educated to identify patients at risk for potential sleep disorders, know how to make an appropriate referral to a sleep clinic for further evaluation and care, and be able to shadow the OFP resident providing care for the student’s patient.
A Brief Summary of Temporomandibular Disorders/ Orofacial Pain and Dental Sleep Medicine: An Historical Perspective of Predoctoral and Postdoctoral Level Curriculum Development for Related Disciplines
John W. Stockstill, DDS, MS, Clinical Associate Professor, East Carolina University School of Dental Medicine, Greenville, NCPredoctoral and postdoctoral TMD/Orofacial Pain curricula in US and Canadian dental schools have evolved over the past 25 years yet remain a “work in progress.” Educational conferences for the development of the curriculum were held in 1990, 1992, and 2000, and as a result of these consensus-focused meetings, educational guidelines for teaching TMD/Orofacial Pain were proposed. Collaborative alliances between the American Academy of Orofacial Pain, the Association of University Temporomandibular Disorder/Orofacial Pain Programs (AUTOPP), academicians and clinicians were created, and numerous publications highlighted the effort of these groups to establish dental educational standards for TMD/Orofacial Pain teaching and clinical utilization.
In 2007, 2011, and 2012, the results of educationally based TMD/Orofacial Pain surveys were published, with these surveys highlighting the need for further calibration and renewed focus upon evidence-based curricula at the predoctoral and postdoctoral levels in this discipline. In conjunction with this recent renewal for curriculum updating came a simultaneous and similar need for the development of dental sleep medicine curriculum in US and Canadian schools. It is within the context and content of the previous TMD/Orofacial Pain conferences that a model or framework for developing a dental sleep medicine (DSM) curriculum was proposed.
In keeping with an overriding theme of “consensus building,” the proposed manner in which this DSM curriculum may be developed closely mimics the previous TMD conference models yet more efficiently supports the inclusion of administrative, educational, and clinical groups in an effort to maintain open channels of communication during this developmental process. This model for inclusion offers an equitable partnership to all interested groups in such a way as to ensure cooperation and collaboration in this new and equally evolving effort, the development of the curriculum in dental sleep medicine. In conclusion, it is recommended that “instead of reinventing the wheel, simply improve upon it”; that is, use the TMD conferences as a model for current and future DSM curriculum development.
Educational Materials
Rose D. Sheats, DMD, MPH, Affiliate Associate Professor, University of North Carolina School of Dentistry, Chapel Hill, NCDue to a desire to provide adequate time for the open floor discussion which was scheduled to follow, this presentation was canceled; however, course participants were advised that written materials for this presentation were included in the course handouts. The intent of the presentation was to assist faculty who sought guidance in developing a foundational curriculum in dental sleep medicine. The materials included a summary of the UNC School of Dentistry dental sleep medicine seminars and lectures with lecture objectives and reading lists, a list of recommended readings, and other resources for additional educational materials in the form of educational CDs, textbooks, journals, and professional organizations.
Open Floor Discussion: What Distinguishes Education in Dental Sleep Medicine in Advanced Education Programs from Education in Predoctoral Dental Programs?
Recurring themes of this discussion follow:- Agreement that predoctoral dental students should minimally be educated to a level of competency
- in the identification of patients at risk for sleep disordered breathing (SDB)
- in the ability to make appropriate referrals for management of SDB patients
- in the ability to explain the consequences of untreated SDB.
- Unless a process is developed in each dental school to ensure appropriate follow-up of patients treated with oral appliance therapy (OAT) consistent with practice guidelines, predoctoral dental students should not be providing oral appliance treatment.
- Restriction of OAT to graduates of advanced education programs, especially only orofacial pain graduates, will not solve the challenge of insufficient practitioners to meet health demand. To alleviate the burden, it may be appropriate for predoctoral students to be educated to competency in treating the “simple” cases of sleep disordered breathing. Clear guidelines must be developed to clarify which SDB patients are classified as “simple.”
- Insufficient faculty expertise in both predoctoral and advanced education programs limit the ability to adequately educate students in predoctoral or graduate programs. Recommendations to develop strategies to share resources among dental schools included:
- emulating the East Carolina University School of Dentistry educational model of electronic access to experts by remote practices by which ECU dental students obtain much of their clinical education at a distance from the source
- purchasing/selling/sharing sleep modules developed by other programs with established educational programs in dental sleep medicine in dental education
- implementing the UCLA model of an extended mini-residency program in sleep medicine at other schools.
Conference Summary: Detailed Recommendations and Follow-up
Drs. Rose Sheats/Greg EssickThe broad issues that emerged from this conference were that sleep disordered breathing, a major global public health burden that affects one in five Americans, provides an opportunity for dentists to make a significant impact on the overall health of the nation and the world. Dental schools are woefully unprepared to educate their graduates to offer appropriate treatment options to manage this condition in support of their medical colleagues. This void in education has permitted more nimble splinter groups and commercial entities to create educational niches which may not serve the best interests of patients.
Physicians express concern about identifying dentists competently trained in OAT. To ensure that oral health care providers are educationally qualified at a minimum to identify sleep disordered breathing, dental school leaders are urged to recognize the urgency of providing a foundation in sleep medicine for all dental graduates. Such education may entail a paradigm shift in dental education that will need to build on an interdependence with medical education and physician educators.
Specific recommendations of conference attendees included:
- Publication of proceedings of this inaugural dental educators conference
- Identification of a core group of educators interested in taking the next steps
- Development of an action plan with deadlines to address the educational challenges described. Plan may include:
- Establishment of a “Dental School Curriculum Committee” to propose educational guidelines for pre- and postdoctoral dental school programs
- Creation of an American Dental Education Association Special Interest Group in sleep medicine
- Creation of liaisons with other stakeholders such as the Commission on Dental Accreditation, the American Dental Education Association, the American Academy of Orofacial Pain, the American Academy of Dental Sleep Medicine, and the American Academy of Sleep Medicine.
CONFERENCE EVALUATIONS
At the conclusion of the conference, participants completed program evaluations to score program content, topic organization, and usefulness and relevance of the information. These three areas were judged favorably with scores of 4.55, 4.52, and 4.4, respectively (maximum score: 5.0). The response rate of 41% was partially influenced by the fact that many attendees had departed by the conclusion of the conference.Attendees observed that course objectives may have been too ambitious, noting that little was accomplished in the development of a strategy to implement teaching of dental sleep medicine in dental schools (score: 3.97) or in the creation of teaching materials to assist faculty who seek to initiate sleep education in their respective programs (score: 3.73). The other course objectives scored very favorably with the objective of describing the need to provide education in sleep disordered breathing in dental schools ranking highest (score: 4.40).
Recommendations for future meetings included:
- establishment of work groups to formulate specific recommendations for educational goals and objectives
- development of awareness campaigns among the public and health care providers to foster an understanding of oral appliance therapy
- strategies to improve interdisciplinary education among all health care providers
- creation of a formal position statement on the importance of sleep medicine education in dental school curricula.
ENDNOTE
1. Although not the intent of the conference, the use of the popular term “dental” sleep medicine, rather than, for example “sleep medicine in dental education or dentistry,” was discussed with the argument that it is inaccurate, confusing, and possibly minimizes the medical implications of sleep disorders or trivializes the dentist’s role in managing it. Sleep disorders comprise medical conditions, but the term “dental” may suggest that some other “sleep” conditions are affecting the dentition. Practitioners and leaders in the field were urged to consider abandoning the term “dental sleep medicine” in favor of “sleep medicine” and to recognize that dentists contribute to an interdisciplinary team of health care providers that seek to optimize the care for each patient.CITATION
Sheats RD, Essick GK. Sleep medicine education in US and Canadian dental schools: a report of the inaugural dental educators conference at the University of North Carolina School of Dentistry. Journal of Dental Sleep Medicine 2014;1(1):53–65.ACKNOWLEDGMENTS
The authors gratefully acknowledge partial support of this conference from the American Academy of Dental Sleep Medicine, Dean Jane Weintraub of the University of North Carolina School of Dentistry, the Dental Foundation of North Carolina, and Airway Management, Inc., Carrolton, TX.SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication February, 2014Accepted for publication February, 2014
Address correspondence to: Rose D. Sheats, DMD, MPH, University of North Carolina School of Dentistry, CB 7450, Chapel Hill, NC 27599; E-mail: rsheats1@nc.rr.com