Special Article 2, Issue 7.4
Identifying the Appropriate Therapeutic Position of an Oral Appliance
http://dx.doi.org/10.15331/jdsm.7158
Rose Sheats, DMD, MPH1; Gregory Essick, DDS, PhD2; Jarrett Grosdidier, DDS3; Sheri Katz, DDS4; Chun Kim, DDS5; Mitchell Levine, DMD6; Imran Patel, DMD7
1Chair, Adams School of Dentistry, University of North Carolina, Chapel Hill, North Carolina (Retired); 2Comprehensive Oral Health, Adams School of Dentistry, University of North Carolina, Chapel Hill, North Carolina; 3S&G Family Dentistry, Leawood, Kansas; 4Oral Appliance Therapy, Atlanta, Georgia; 5TMJ Head & Neck Pain Center, Rancho Mirage, California; 6Board Liaison, Department of Orthodontics, University of Tennessee Health Science Center, Memphis, Tennessee; 7Department of Medicine, University of Arizona, Tucson, Arizona
*This paper was updated November 29, 2023.
INTRODUCTION
Customized, adjustable oral appliances stabilize and protrude the mandible to effectively treat sleep-related breathing disorders (SRBDs) by reducing respiratory events.1
Recognizing that the appropriate therapeutic position of mandibular advancement varies from patient to patient,2 an American Academy of Dental Sleep Medicine (AADSM) task force evaluated a variety of methods for identifying the therapeutic position of an oral appliance. The task force determined the most clinically useful methods and provided a protocol on how to use each method. These protocols cover the following methods: initial mandibular position, symptom review, pulse oximetry (PO) or home sleep apnea tests (HSATs) administered by qualified dentists, and HSATs or polysomnography (PSG) ordered by physicians. A qualified dentist includes American Board of Dental Sleep Medicine (ABDSM) diplomates, AADSM qualified dentists, and ABDSM international certificants. In order to receive one of the above designations, at a minimum, a dentist must successfully complete all or specific components of the AADSM Mastery Program.3,4
For the protocols, the appropriate therapeutic position of an oral appliance is defined as:
A position of the mandible that achieves improvement of signs, symptoms, or objective indices of sleep-related breathing disorders. The determination of improvement is agreed upon by the patient, dentist, and medical provider using clinical experience and, when available, evidence-based approaches. At this position, the appliance can be used comfortably, on a nightly basis.
METHODS SUPPORTED BY EVIDENCE
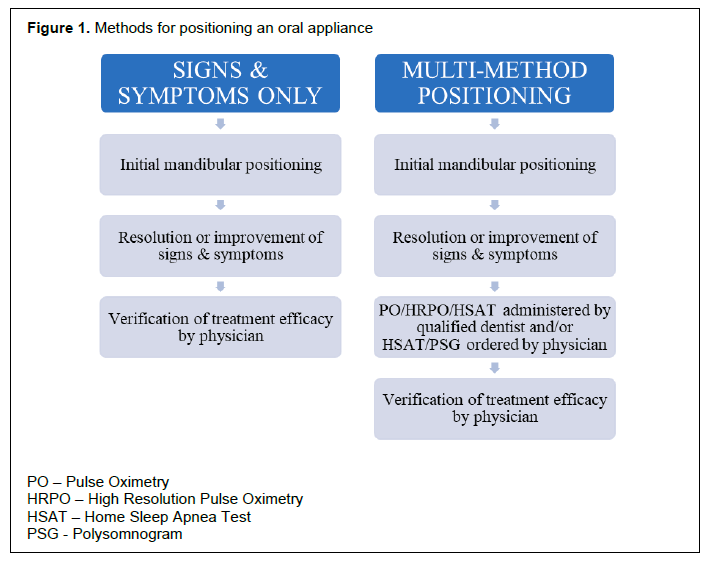
Although each of the methods for therapeutic positioning presented in this article was evaluated separately, they are often used in combination. Figure 1 describes potential combinations of the methods described in the following paragraphs.
Methods for positioning an oral appliance |
{kind=link}
Initial Mandibular Positioning
The term initial mandibular position is defined as the starting position of the mandible when an oral appliance is delivered at initiation of therapy. The initial mandibular position may be recorded as a millimeter measurement or as a percentage of maximum mandibular excursion from the posterior reference point to maximal protrusion. The initial mandibular position is recorded with a construction bite by the qualified dentist. It is important to note that the initial mandibular protrusion differs based on which oral appliance is fabricated – the ideal bite gauge varies based on appliance type.
Multiple studies have attempted to determine the most effective initial mandibular position, balancing adverse effects against the time required to reach an appropriate therapeutic position.5–9 However, past studies do not consistently indicate whether the posterior reference for the construction bite refers to maximal mandibular retrusion or habitual occlusion and other studies have not indicated the posterior reference at all. The task force recommends that the posterior reference point be standardized to the most retruded position.
Studies vary considerably on a recommended initial mandibular position. Starting positions ranged from 25% to 75%.5,7–9 In a meta-analysis of 13 randomized controlled trials, data analysis suggested that advancements greater than 50% did not influence the success rate.7 Although most evidence indicates that an initial mandibular position of 50% advancement may both minimize side effects and improve respiratory indices, there are studies indicating that starting treatment at the patient’s habitual occlusion without any additional advancement can significantly reduce the apnea-hypopnea index.6 Clinicians should recognize that 50% advancement may be greater than necessary for any individual patient and may consider decreasing the amount of advancement as long as subjective and/or objective assessments do not worsen.
Data can be derived from motorized systems that are used either at home or in the sleep laboratory while a temporary appliance is in situ. These data are termed theragnostic sleep data. In the case of oral appliance therapy (OAT), these data can be used to both identify the apnea-hypopnea index and suggest an appropriate therapeutic position, thus, expediting the positioning process.10 One advantage of using such systems in a sleep laboratory is that they enable a sleep technologist to adjust the position of the mandible without removing the appliance from the patient’s mouth.11,12 In one test of such a system, the predicted target protrusion was effective in 87% of patients.12 In another study, a home version of this technology successfully predicted the appropriate therapeutic position in 85% of cases.13
Protocol
The qualified dentist will deliver the appliance with a predetermined initial starting position captured by an interocclusal record that defines the construction bite. The qualified dentist must assess the patient’s curve of Spee and include adequate vertical dimension in the construction bite to allow for device advancement.
Different protocols may be used to obtain the construction bite. These may include:
- A percentage of maximum protrusion, relative to maximum retrusion, determined without theragnostic sleep data.
- A percentage of maximum protrusion, relative to maximum retrusion, determined by theragnostic sleep data.
- Other methods as determined by the qualified dentist.
Note that the initial starting position may also be the appropriate therapeutic position. In this instance, no further subsequent advancement is needed.
Review of Signs and Symptoms
Signs and symptoms reported by the patient or the bed partner is a clinically useful method for determining the appropriate therapeutic position of an oral appliance. After the appliance is delivered, the patient uses it nightly for a period of time to acclimatize to the initial mandibular position. Subsequently, the oral appliance may be advanced in small increments by the patient or qualified dentist.14–16 Within the literature reviewed, there is no consensus regarding the duration of the initial acclimatization period, the increment of advancement or the time between adjustments. However, with few exceptions,17–19 the studies reported increasing the advancement no more than 1 mm at a time.
Research studies using this method have defined signs and symptoms differently. In some research, the targeted signs and symptoms include snoring, witnessed apneas and/or excessive daytime sleepiness .15,17, 19–26,27–30 Snoring can be assessed by informal questioning or the use of the visual analog scale score. Excessive daytime sleepiness can be assessed by informal questioning, use of the visual analog scale score or use of the Epworth Sleepiness Scale or other standardized sleep assessment.
Some studies have considered positioning based on symptomatic improvement alone to be insufficient.27,28,31 In these studies, the authors demonstrate that better resolution can be obtained by combining reduction of signs and symptoms with results of objective data. Some studies suggest a position that balances the risk of additional advancement, such as temporomandibular joint discomfort, with the benefit of better symptomatic improvement.14,32–34
Nevertheless, the task force agreed that the appropriate therapeutic position can be achieved by using signs and symptoms alone in some cases, or by combining this method with other methods.
Protocol
Goal of the therapeutic positioning method: to achieve reduction/elimination of signs and symptoms consistent with untreated SRBDs.
Parameters typical of patient-specific signs and symptoms may include: snoring, witnessed apneas, nocturnal polyuria, gasping, restless sleep, mood disorders, excessive daytime sleepiness, unrefreshed sleep, cognitive impairment, morning headaches, and memory impairment.
- Prior to delivery of the oral appliance, ensure there has been a recent assessment of signs and symptoms. Use standardized assessments when possible.
- A period of acclimatization to the appliance at its initial starting position is advisable. Following a 1 to 4 week acclimatization, if signs and symptoms persist and patient comfort permits, the device may now be advanced in 0.25 to 1mm increments.
- Advancement can be done by the qualified dentist or by the patient at home.
- Within 30 days post insertion and on regular intervals as needed, the patient should be followed up for evaluation and reassessment of signs and symptoms with the same questionnaires used at initial assessment.
- Advancement should continue, patient comfort permitting, until signs and symptoms resolve. Frequency of advancements should be determined by the qualified dentist based on the amount of advancement, the patient response, and device features.
- When signs and symptoms are sufficiently resolved or the maximum comfortable position is reached, the qualified dentist may choose to proceed with another method to further improve the therapeutic position or the patient should return to the referring provider to verify treatment efficacy.
PO, HSATs, or PSG
Pulse Oximetry
The task force determined that PO, including high-resolution pulse oximetry (HRPO), administered by dentists is a supported strategy for identifying the appropriate therapeutic position. PO measures a patient’s oxygen levels during sleep and is a type 4 sleep study.35 The position of the oral appliance is typically adjusted until the frequency of oxygen desaturations (oxygen desaturation index [ODI]) of a given magnitude (often 3% or 4%) is reduced to a target level or further advancement is uncomfortable. Unlike traditional PO, HRPO measures oxygen levels and incorporates a sampling rate at least every second.36
Studies have determined that PO may be useful in identifying the appropriate therapeutic position of an appliance.8,36,37 Adjustment based on reduction in both symptoms and the frequency of oxygen desaturations resulted in better resolution of the patients’ SRBD than either method alone.37 The task force concluded that PO may be relatively easy to use and may be more beneficial than frequent HSATs in certain clinical settings.
Home Sleep Apnea Tests
The task force determined that HSATs are a supported method for identifying the appropriate therapeutic position. HSATs are unattended sleep studies that measure a variety of sleep parameters (for example, respiratory event index [REI], ODI, oxygen nadir, oxygen saturation [SpO2], body position). Most HSATs are classified as type 3 or type 4 sleep studies. In 2017, the American Dental Association endorsed home sleep apnea testing as a method that dentists may use “to help define the optimal target position of the mandible”.38 It is important for the clinician to recognize that education on use of HSATs is indicated.
HSATs were described as helping to identify the appropriate therapeutic position of an oral appliance.39,40 HSAT was used in a number of studies in combination with resolution of signs and symptoms to position appliances.41–44
Limitations of HSAT include its diminished accuracy in patients with comorbid medical conditions such as moderate to severe pulmonary disease, neuromuscular disease, or congestive heart failure.35 HSAT is also contraindicated in patients in whom other sleep disorders such as central sleep apnea, periodic limb movement disorder, insomnia, or narcolepsy are suspected or have been diagnosed.45 It is also important to understand that because HSAT does not measure electroencephalographic activity, it may underestimate the severity of OSA due to inability to differentiate between total sleep time and time in bed.45,46
Polysomnography
The task force determined that PSG is a supported method for identifying the appropriate therapeutic position of an appliance. Adjustment of the oral appliance to achieve the best improvement of signs and symptoms usually precedes the PSG. PSG involves a continuous, simultaneous recording of a number of sleep parameters (electroencephalography, electro-oculography, airflow respiratory effort, oximetry, sleep duration). PSG is performed overnight and is typically attended by a sleep technologist. PSG is useful to clarify whether patients need additional advancement despite symptomatic relief, but the data may also be used by the medical provider to verify treatment efficacy.
In a number of studies, appliances were first positioned using signs and symptoms, and then later, PSG was also used for additional positioning. One study achieved treatment success in almost 74% of patients using this method.47 Other studies showed an increased number of treatment successes when adding PSG to their positioning method following sign and symptom relief.48,49 Some studies have initially used PSG to position the appliance. Pételle et al. concluded that single-night PSG is a suitable solution to identify the appropriate therapeutic position or to conclude that OAT is not efficacious.50
The qualified dentist should provide the sleep facility with instructions for positioning during the PSG and provide training for the appliances delivered by that dentist. It should be noted that patient preference and lack of access may impede use of this method.
Protocols
PO or HSAT Administered by a Qualified Dentist
The respiratory parameters in this protocol were defined according to the American Academy of Sleep Medicine’s scoring manual.51
Goal of the therapeutic positioning method: to achieve a reduction in or normalization of PO or HSAT parameters and resolution of SRBD after signs and symptoms have been addressed.
Parameters typically considered with use of PO include: ODI, percentage of time spent at peripheral SpO2 less than 90% (CT 90), and oxygen nadir (LSAT). Other parameters are available from use of proprietary software and HRPO.
Additional parameters typically considered only with use of HSAT include: respiratory event index [REI], sleep position, and snoring index.
NOTE: This protocol includes positioning with signs and symptoms first.
- PO or HSAT (unless prohibited by the qualified dentist’s state dental board) is administered by the qualified dentist. The qualified dentist should ensure that a written advancement protocol is provided to the patient.
- Prior to the delivery of an oral appliance, the qualified dentist should obtain baseline parameter values using the same type of monitoring device which will then be used during interim adjustments.
- The oral appliance device is advanced by the qualified dentist or patient at home to reduce or eliminate signs and symptoms (see previous section on Review of Signs and Symptoms).
- Once resolution of signs and symptoms has been addressed, PO or HSAT is repeated to determine whether an appropriate therapeutic position has been achieved. If the target parameter values have not been met, oral appliance advancement should continue.
- Oral appliance advancement should continue until target parameter values are attained, can no longer be improved, or the maximum comfortable position is reached. The patient should return to the referring provider to verify treatment efficacy. The PO /HSAT data should be provided to the referring medical provider; they may use it to verify treatment efficacy.
HSAT or PSG Ordered by the Physician
The respiratory parameters in these protocols were defined according to the American Academy of Sleep Medicine’s scoring manual.51Goal of the therapeutic positioning method: to achieve a reduction in or normalization of HSAT parameters or in-laboratory PSG parameters and resolution of SRBDs after signs and symptoms and any home testing (PO or HSAT) administered by the dental office have been addressed.
Parameters typically considered with use of either HSAT and PSG include: ODI, percentage of time spent at peripheral oxygen saturation (SpO2) less than 90% (CT 90), and oxygen nadir (LSAT), sleep position, and snoring index.
Parameters typically considered with use of HSAT only include: REI.
Parameters typically considered with use of PSG only include: apnea-hypopnea index (AHI) and respiratory disturbance index (RDI).
- Initially, the oral appliance is advanced by the qualified dentist or patient at home to reduce or eliminate signs and symptoms (see previous section on Review of Signs and Symptoms).
- Objective methods may subsequently be used to adjust the oral appliance after resolution of signs and symptoms (see previous section on PO or HSAT).
- The qualified dentist then refers the patient for a physician-ordered and -monitored multi-night HSAT or single-night PSG to identify the appropriate therapeutic position of the oral appliance.
- The qualified dentist provides a written advancement protocol to the patient and medical provider.
The intent is to allow for assessment of device efficacy at two or three different oral appliance positions as tested on different nights.
Elements of this protocol may include:
- Instructions for how to advance the appliance.
- Amount of additional advancement (the appliance setting) for each night.
- Instructions that following all testing, the patient should re-set the oral appliance to the pre-test setting.
Instructions for use during single-night PSG.
The intent is to allow assessment of device efficacy at several different positions during the single-night PSG.
Elements of this protocol to be sent to the sleep facility may include:
- Name of the oral appliance.
- Current level of advancement.
- The amount of sleep time before the first device advancement and the criteria for advancement.
- Instructions for how to advance the appliance.
- The frequency of advancement, the maximum number of advancements, and the incremental amount of each advancement.
- Instruction to reset the oral appliance to the initial setting before the patient leaves the sleep laboratory.
- Instructions for the sleep technologist to note timing and amount of each advancement during the sleep study and to include in the report.
- The sleep technologist must be provided with the accessories necessary to advance the appliance.
Following HSAT or PSG scoring, the medical provider will determine which setting is the appropriate therapeutic position and relay this information to the qualified dentist. The qualified dentist should be sure to follow up with the patient regarding this information.
When using any of these methods, it is critical to take patient tolerance and comfort into account when identifying the appropriate therapeutic position. It is important not to over advance the appliance in order to avoid potential adverse effects. Although these methods are useful for identifying the appropriate therapeutic position of the appliance, the patient should be referred to a medical provider to verify treatment efficacy. In some cases, the method for final verification of efficacy may differ from the one used for positioning.
METHODS WITH UNCERTAIN EVIDENCE
Nasopharyngoscopy
Nasopharyngoscopy uses a scope to examine the airway and can be performed while the patient is either awake using topical anesthesia (awake endoscopy), or while the patient is asleep using agents such as propofol (drug-induced sleep endoscopy).
Several studies reviewed used nasopharyngoscopy to evaluate anatomic changes in the upper airway during mandibular advancement; however, most studies were focused on identification of potential OAT responders.8 The task force concluded that no study has demonstrated the usefulness of awake nasopharyngoscopy to determine the appropriate therapeutic position of an oral appliance, and awake nasopharyngoscopy may not accurately mimic the sleeping patient. With the use of sleep nasopharyngoscopy, it is unknown whether anatomic observations made with simulated bite registrations will translate to OAT efficacy or whether additional adjustment with another method (such as HSAT or PSG) will be required to normalize respiratory parameters. Additionally, the task force concluded that although nasopharyngoscopy with neuromuscular block, as used in one study, might prove useful in adjusting an oral appliance, the invasiveness and risk of the procedure precludes its clinical use.
The available evidence led the task force to conclude that the usefulness of nasopharyngoscopy for identifying the appropriate therapeutic position is uncertain at this time, although some studies are promising. For example, preliminary data from a pilot study suggest that drug-induced sleep endoscopy might be used to identify the appropriate therapeutic position for oral appliance success based on anatomic observations of the pharynx and that airway patency may not be optimal at the position of maximum advancement.52
METHODS NOT SUPPORTED BY EVIDENCE
The task force found inadequate evidence in support of the following methods for therapeutic positioning.
Maximum Comfortable Protrusion Without Other Information
Some studies advocate either initiating OAT at or advancing to the maximum comfortable protrusion without consideration of improvement of symptoms.53–57 However, most studies suggest that the maximum comfortable protrusion may result in unwanted dental adverse effects.58 Studies have demonstrated that some patients respond adequately to a nominal amount of mandibular advancement6 or that a small mandibular advancement may be more efficacious than a larger one.59
Rather than a specific therapeutic positioning method, the task force viewed the maximum comfortable protrusion as the upper limit of advancement for positioning based on other strategies (signs and symptoms, PO, etc.), and therefore did not consider maximum comfortable protrusion to be a method for identifying the appropriate therapeutic position of an oral appliance.
Imaging Techniques
Imaging techniques measure the upper airway while an oral appliance is adjusted either by horizontal advancement or vertical opening of the mandible.60–62 The imaging techniques in the literature reviewed included magnetic resonance imaging, lateral cephalometry, and pharyngometry. These studies did not assess airway parameters during appliance adjustments and thus did not directly lead to identification of the appropriate therapeutic position of an oral appliance. Furthermore, one study used nonapneic men as study subjects, leading the task force to question its applicability to patients with OSA.60
Pharyngometry uses sound waves to classify the site of airway collapse by recording the amplitude of the soundwaves as they reflect off the hypopharynx and oropharynx.63 It is accomplished in awake patients and thus may not be an accurate assessment of the behavior of the upper airway in sleeping patients. Most articles were either review articles or were focused on the deployment of the technique itself;64,65 no study reviewed demonstrated the effectiveness of pharyngometry in ascertaining the appropriate therapeutic position of OAT for symptom resolution or normalization/improvement in respiratory parameters.64-73
FORTHCOMING TECHNOLOGIES
Consumer sleep technology (CST) is a rapidly evolving field that has been enthusiastically embraced by patients.74 CST may include commercially available devices and apps that measure sleep parameters (snoring and sleep apps). The task force sought literature on the use of CST to identify the appropriate therapeutic position of oral appliances but did not identify any studies that evaluated the use of CST in this context. Evidence for the use of CST for early screening of sleep-disordered breathing, however,75 suggests that CST may extend in the future to dental sleep medicine for use in therapeutic positioning of oral appliances.
DEVELOPMENT OF RECOMMENDATIONS
Consensus Conference Process
The AADSM Board of Directors created a task force with seven members, all of whom have extensive experience in dental sleep medicine and reviewing literature. None of the task force members had any conflicts of interest relevant to this topic.
A modified RAND/UCLA Appropriateness Method76 was used to develop this article Task force members considered scholarly evidence, other clinical literature, their own clinical experience, and patient preferences to determine the most clinically useful methods for identifying the appropriate therapeutic position of an oral appliance. As indicated by RAND/UCLA rules, the inclusion or exclusion of methods did not include consideration of cost or insurance.
Literature Search
A literature search of PubMed and Google Scholar was performed using a combination of terms (see next paragraphs). Additionally, the bibliographies of pertinent review articles and dissertations were searched for relevant articles. Although comprehensive, this literature review was not conducted as a systematic review.
Search Terms
Search terms related to treatment: oral, intraoral, dental, orthodontic(s), mandibular, tongue retaining, tongue stabilizing, occlusal, titratable/titrated, appliance(s), splint(s), device(s).
Search terms related to disease: sleep apnea, sleep apnea syndromes, sleep-related breathing disorder(s), sleep-disordered breathing, snoring.
Search terms related to positioning of the oral appliance: titration, calibration, adjustment.
Literature Review
The final set of 133 articles was divided into categories based on the type of positioning method addressed in the article. An additional 21 articles were reviewed after collecting these 133 original articles, for a total of 154 articles. Task force members performed a detailed review of the literature and presented their evaluations to the full task force at their face-to-face meeting described below.
The task force eliminated literature on strategies used to identify treatment responders. Such methods are based on phenotyping or on evaluating patterns of airway collapse77,78 to predict which patients might respond to OAT. However, even after identifying probable or ideal candidates, the appliance must still be adjusted to ascertain the appropriate therapeutic position.
Voting on Strategies
Prior to the face-to-face consensus conference, task force members were sent an exhaustive list of methods for identifying the appropriate therapeutic position of an oral appliance. This list was compiled based on input from members of the AADSM and Diplomates of the American Board of Dental Sleep Medicine. For the first round of voting, task force members were asked to independently rate each method. The rating scale ranged from 1 to 9, with 1 indicating the lowest and 9 indicating the highest level of support by evidence and clinical experience.
Unanimous votes by the task force members are not required by the RAND/UCLA rules. Consensus among the task force members was achieved when at least four members agreed that the particular method was supported by the evidence, unsupported, or that the evidence was uncertain.
During the face-to-face conference on February 21-23, 2020, task force members presented their evaluation of the literature associated with each method. Following each presentation, a second round of voting occurred, using the same scale as the first round. Based on discussion of evidence presented, task force members were free to change their ratings of each method from their first vote. A third round of voting was held after additional discussion of any methods for which consensus was not reached after the second round of voting. After the voting was completed, the most clinically useful methods, supported by both strong levels of evidence and clinical experience, were identified.
LIMITATIONS AND RECOMMENDATIONS
Because no definition of treatment success exists, the task force did not specify the value of respiratory parameters to achieve when adjusting the oral appliance to therapeutic position using the methods described. OAT providers should collaborate with the patient and medical provider to individualize treatment goals for each patient before OAT is initiated.
The literature review for this article was thorough but was not conducted as a systematic review. The task force also acknowledged that the research could have had larger sample sizes, better control groups, and long-term follow-up. Additionally, many articles did not directly test the validity of the method and thus interpretations had to be inferred from indirect data.
The task force recommended that future research focus on how best to identify the appropriate therapeutic position of an oral appliance. Specifically, the following topics merit further investigation:
- Most of the research reviewed for this paper compared end-of-treatment outcome measures to those at baseline, rather than at initiation of treatment. In doing so, the efficacy of OAT is assessed but not the efficacy of the therapeutic positioning method itself. Final outcomes should be compared to those at initiation of therapy in future studies to elucidate the usefulness of the method used to determine the appropriate therapeutic position. Similarly, the posterior reference should be clearly indicated in future studies as well.
- More research should be conducted on whether nasopharyngoscopy can be used to determine the appropriate therapeutic position of an appliance.
- Robust studies should be conducted that compare the value of following symptom resolution with any of several objective methods. Study methodology should ensure that the same equipment and measurement tools are used throughout the study to make meaningful comparisons between treatment assessments. Additionally, therapeutic positioning via symptoms alone should be tested against using symptoms in conjunction with an objective therapeutic positioning method.
- As imaging techniques are refined, studies should test their effectiveness in simplifying the therapeutic positioning process.
- Although the field of CST is expanding, none of these technologies have been evaluated for their efficacy in identifying the appropriate therapeutic position of an oral appliance. As CSTs evolve, their potential should be scientifically tested.
ACKNOWLEDGEMENTS
The task force gratefully acknowledges the invaluable and patient support of Heather Montague, AADSM Research and Policy Development Manager, and appreciates the counsel of Becky Roberts, AADSM Executive Director, and Coreen Vick, AADSM Director of Clinical Services. The Chair is deeply indebted to the task force members for their selfless commitment to this project in support of the AADSM vision to be a leader in the field of dental sleep medicine.
CITATION
Sheats R, Essick G, Grosdidier J, Katz S, Kim C, Levine M, Patel I. Identifying the appropriate therapeutic position of an oral appliance. J Dent Sleep Med. 2020;7(4).
REFERENCES
- Scherr SC, Dort LC, Almeida F, et al. Definition of an effective oral appliance for the treatment of obstructive sleep apnea and snoring: A report of the American Academy of Dental Sleep Medicine consensus conference participants. J Dent Sleep Med. 2014;1(1). https://aadsm.org/docs/JDSM.1.1.39.pdf. Accessed December 28, 2018.
- Dieltjens M, Vanderveken OM, Van de Heyning PH, Braem MJ. Current opinions and clinical practice in the titration of oral appliances in the treatment of sleep-disordered breathing. Sleep Med Rev. 2012;16(2):177-185. doi:10.1016/j.smrv.2011.06.002
- Levine M, Bennett KM, Cantwell MK, Postol K, Schwartz DB. Dental sleep medicine standards for screening, treating, and managing adults with sleep-related breathing disorders. J Dent Sleep Med. 2018;5(3):61-68. doi:10.15331/jdsm.7030
- Levine M, Cantwell M, Postol K, Schwartz D. Dental sleep medicine standards for screening, treating, and management of sleep-related breathing disorders in adults using oral appliance therapy. J Dent Sleep Med. 2022;9(4)
- Aarab G, Lobbezoo F, Hamburger HL, Naeije M. Effects of an oral appliance with different mandibular protrusion positions at a constant vertical dimension on obstructive sleep apnea. Clin Oral Investig. 2010;14(3):339-345. doi:10.1007/s00784-009-0298-9
- Anitua E, Durán-Cantolla J, Almeida GZ, Alkhraisat MH. Minimizing the mandibular advancement in an oral appliance for the treatment of obstructive sleep apnea. Sleep Med. 2017;34:226-231. doi:10.1016/j.sleep.2016.12.019
- Bartolucci ML, Bortolotti F, Raffaelli E, D’Antò V, Michelotti A, Alessandri Bonetti G. The effectiveness of different mandibular advancement amounts in OSA patients: a systematic review and meta-regression analysis. Sleep Breath. 2016;20(3):911-919. doi:10.1007/s11325-015-1307-7
- Kato J, Isono S, Tanaka A, et al. Dose-dependent effects of mandibular advancement on pharyngeal mechanics and nocturnal oxygenation in patients with sleep-disordered breathing. Chest. 2000;117(4):1065-1072. doi:10.1378/chest.117.4.1065
- Walker-Engström ML, Ringqvist I, Vestling O, Wilhelmsson B, Tegelberg A. A prospective randomized study comparing two different degrees of mandibular advancement with a dental appliance in treatment of severe obstructive sleep apnea. Sleep Breath. 2003;7(3):119-130. doi:10.1007/s11325-003-0119-3
- Kastoer C, Dieltjens M, Oorts E, et al. The use of remotely controlled mandibular positioner as a predictive screening tool for mandibular advancement device therapy in patients with obstructive sleep apnea through single-night progressive titration of the mandible: A systematic review. J Clin Sleep Med. 2016;12(10):1411-1421. doi:10.5664/jcsm.6202
- Dort LC, Hadjuk E, Remmers JE. Mandibular advancement and obstructive sleep apnoea: A method for determining effective mandibular protrusion. Eur Respir J. 2006;27(5):1003-1009. doi:10.1183/09031936.06.00077804
- Remmers J, Charkhandeh S, Grosse J, et al. Remotely controlled mandibular protrusion during sleep predicts therapeutic success with oral appliances in patients with obstructive sleep apnea. Sleep. 2013;36(10):1517-1525. doi:10.5665/sleep.3048
- Remmers JE, Topor Z, Grosse J, et al. A feedback-controlled mandibular positioner identifies individuals with sleep apnea who will respond to oral appliance therapy. J Clin Sleep Med. 2017;13(07):871-880. doi:10.5664/jcsm.6656
- Attali V, Chaumereuil C, Arnulf I, et al. Predictors of long-term effectiveness to mandibular repositioning device treatment in obstructive sleep apnea patients after 1000 days. Sleep Med. 2016;27-28:107-114. doi:10.1016/j.sleep.2016.10.004
- Martinot JB, Le-Dong NN, Crespeigne E, et al. Mandibular movement analysis to assess efficacy of oral appliance therapy in OSA. Chest. 2018;154(6):1340-1347. doi:10.1016/j.chest.2018.08.1027
- Ten Berge DM, Braem MJ, Altenburg A, et al. Evaluation of the impact of a clinical pathway on the organization of a multidisciplinary dental sleep clinic. Sleep Breath. 2014;18(2):325-334. doi:10.1007/s11325-013-0888-2
- Bachour P, Bachour A, Kauppi P, Maasilta P, Mäkitie A, Palotie T. Oral appliance in sleep apnea treatment: respiratory and clinical effects and long-term adherence. Sleep Breath. 2016;20(2):805-812. doi:10.1007/s11325-015-1301-0
- Makihara E, Kawano T, Miyajima R, Masumi S, Enciso R, Clark GT. Assessment of oral appliance for obstructive sleep apnea patients. Clin Exp Dent Res. 2016;2(2):155-161. doi:10.1002/cre2.35
- Cruz MGME. Treatment of obstructive sleep apneas with a mandibular advancement device: A preliminary study about the impact on vigilance and sleep structure. 2010. http://repositorio.ul.pt/bitstream/10451/4694/3/630698_Tese.pdf. Accessed May 3, 2019.
- Okuno K, Sasao Y, Nohara K, et al. Endoscopy evaluation to predict oral appliance outcomes in obstructive sleep apnoea. Eur Respir J. 2016;47(5):1410-1419. doi:10.1183/13993003.01088-2015
- Perez CV, de Leeuw R, Okeson JP, et al. The incidence and prevalence of temporomandibular disorders and posterior open bite in patients receiving mandibular advancement device therapy for obstructive sleep apnea. Sleep Breath. 2013;17(1):323-332. doi:10.1007/s11325-012-0695-1
- Pliska BT, Nam H, Chen H, Lowe AA, Almeida FR. Obstructive sleep apnea and mandibular advancement splints: occlusal effects and progression of changes associated with a decade of treatment. J Clin Sleep Med. 2014;10(12):1285-1291. doi:10.5664/jcsm.4278
- Tsuiki S, Kobayashi M, Namba K, et al. Optimal positive airway pressure predicts oral appliance response to sleep apnoea. Eur Respir J. 2010;35(5):1098-1105. doi:10.1183/09031936.00121608
- El Ibrahimi M, Laabouri M. Pilot study of a new adjustable thermoplastic mandibular advancement device for the management of obstructive sleep apnoea-hypopnoea syndrome: a brief research letter. Open Respir Med J. 2016;10:46-50. doi:10.2174/1874306401610010046
- Galic T, Bozic J, Ivkovic N, Gunjaca G, Kurir Ticinovic T, Dogas Z. Effects of mandibular advancement device treatment on arterial stiffness and glucose metabolism in patients with mild to moderate obstructive sleep apnea: A prospective 1 year study. Sleep Breath. 2016;20(1):69-77. doi:10.1007/s11325-015-1186-y
- Jo SY, Lee SM, Lee KH, Kim D-K. Effect of long-term oral appliance therapy on obstruction pattern in patients with obstructive sleep apnea. Eur Arch Oto-Rhino-Laryngology. 2018;275(5):1327-1333. doi:10.1007/s00405-018-4909-4
- de Almeida FR, Bittencourt LR, de Almeida CIR, Tsuiki S, Lowe AA, Tufik S. Effects of mandibular posture on obstructive sleep apnea severity and the temporomandibular joint in patients fitted with an oral appliance. Sleep. 2002;25(5):505-511. doi:10.1093/sleep/25.5.505
- Almeida FR, Mulgrew A, Ayas N, et al. Mandibular advancement splint as short-term alternative treatment in patients with obstructive sleep apnea already effectively treated with continuous positive airway pressure. J Clin Sleep Med. 2013;09(04):319-324. doi:10.5664/jcsm.2576
- Bishop B, Verrett R, Girvan T. A randomized crossover study comparing two mandibular repositioning appliances for treatment of obstructive sleep apnea. Sleep Breath. 2014;18(1):125-131. doi:10.1007/s11325-013-0859-7
- Dieltjens M, Vanderveken OM, Hamans E, et al. Treatment of obstructive sleep apnea using a custom-made titratable duobloc oral appliance: A prospective clinical study. Sleep Breath. 2013;17(2):565-572. doi:10.1007/s11325-012-0721-3
- Doff MHJ, Hoekema A, Pruim GJ, Huddleston Slater JJR, Stegenga B. Long-term oral-appliance therapy in obstructive sleep apnea: A cephalometric study of craniofacial changes. J Dent. 2010;38(12):1010-1018. doi:10.1016/J.JDENT.2010.08.018
- Marco Pitarch R, Selva García M, Puertas Cuesta J, Marco Algarra J, Fernández Julian E, Fons Font A. Effectiveness of a mandibular advancement device in obstructive sleep apnea patients: a prospective clinical trial. Eur Arch Oto-Rhino-Laryngology. 2018;275(7):1903-1911. doi:10.1007/s00405-018-4978-4
- Arya D, Tripathi A, Singh SV, Tripathi S, Nagar A, Mishra A. A pilot study to evaluate posttreatment cephalometric changes in subjects with OSA. J Prosthet Dent. 2010;103(3):170-177. doi:10.1016/S0022-3913(10)60024-8
- Vecchierini MF, Attali V, Collet JM, et al. Sex differences in mandibular repositioning device therapy effectiveness in patients with obstructive sleep apnea syndrome. Sleep and Breathing. 2019;23:837-848.
- Collop NA, Anderson WMD, Boehlecke B, et al. Clinical guidelines for the use of unattended portable monitors in the diagnosis of obstructive sleep apnea in adult patients. J Clin Sleep Med. 2007;3(7):737-747. doi:10.5664/jcsm.27032
- Metz JE, Attarian HP, Harrison MC, et al. High-resolution pulse oximetry and titration of a mandibular advancement device for obstructive sleep apnea. Front Neurol. 2019;10:757. doi:10.3389/fneur.2019.00757
- Fleury B, Rakotonanahary D, Petelle B, et al. Mandibular advancement titration for obstructive sleep apnea: Optimization of the procedure by combining clinical and oximetric parameters. Chest. 2004;125(5):1761-1767. doi:10.1378/chest.125.5.1761
- ADA Adopts Policy on Dentistry’s Role in Treating Obstructive Sleep Apnea, Similar Disorders. American Dental Association. https://www.ada.org/en/press-room/news-releases/2017-archives/october/ada-adopts-policy-on-dentistry-role-in-treating-obstructive-sleep-apnea. Accessed May 3, 2019.
- Morgan TD. Novel approaches to the management of sleep-disordered breathing. Sleep Med Clin. 2016;11(2):173-187. doi:10.1016/j.jsmc.2016.03.001
- Dioguardi A, Al-Halawani M. Oral appliances in obstructive sleep apnea. Otolaryngol Clin North Am. 2016;49(6):1343-1357. doi:10.1016/j.otc.2016.07.005
- Levendowski DJ, Morgan TD, Patrickus JE, et al. In-home evaluation of efficacy and titration of a mandibular advancement device for obstructive sleep apnea. Sleep Breath. 2007;11(3):139-147. doi:10.1007/s11325-006-0094-6
- Bosshard V, Masse J-F, Series F. Prediction of oral appliance efficiency in patients with apnoea using phrenic nerve stimulation while awake. Thorax. 2011;66(3):220-225. doi:10.1136/thx.2010.150334
- Gakwaya S, Melo-Silva CA, Borel J-C, Rousseau E, Masse J-F, Sériès F. Impact of stepwise mandibular advancement on upper airway mechanics in obstructive sleep apnea using phrenic nerve magnetic stimulation. Respir Physiol Neurobiol. 2014;190:131-136. doi:10.1016/j.resp.2013.10.004
- Norrhem N, Marklund M. An oral appliance with or without elastic bands to control mouth opening during sleep—a randomized pilot study. Sleep Breath. 2016;20(3):929-938. doi:10.1007/s11325-016-1312-5
- Collop NA. Portable monitoring for the diagnosis of obstructive sleep apnea. Curr Opin Pulm Med. 2008;14(6):525-529. doi:10.1097/MCP.0b013e328312ed4a
- Rosen IM, Kirsch DB, Chervin RD, et al. Clinical use of a home sleep apnea test: An American academy of sleep medicine position statement. J Clin Sleep Med. 2017;13(10):1205-1207. doi:10.5664/jcsm.6774
- Holley AB, Lettieri CJ, Shah AA. Efficacy of an adjustable oral appliance and comparison with continuous positive airway pressure for the treatment of obstructive sleep apnea syndrome. Chest. 2011;140(6):1511-1516. doi:10.1378/chest.10-2851
- Almeida FR, Parker JA, Hodges JS, Lowe AA, Ferguson KA. Effect of a titration polysomnogram on treatment success with a mandibular repositioning appliance. J Clin Sleep Med. 2009;5(3):198-204.
- Krishnan V, Collop NA, Scherr SC. An evaluation of a titration strategy for prescription of oral appliances for obstructive sleep apnea. Chest. 2008;133(5):1135-1141. doi:10.1378/chest.07-1644
- Pételle B, Vincent G, Gagnadoux F, Rakotonanahary D, Meyer B, Fleury B. One-night mandibular advancement titration for obstructive sleep apnea syndrome: A pilot study. Am J Respir Crit Care Med. 2002;165(8):1150-1153. doi:10.1164/ajrccm.165.8.2108056
- Berry R, Quan S, Abreu S, et al. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. 2.6. Darien, IL; 2020.
- Chiang H, Bauschard M, Nord R. AADSM Accepted Abstracts (2020). J Dent Sleep Med. 7(2):2020. doi:10.15331/jdsm.7128
- Cunha TCA, Guimarães TDM, Schultz THC, et al. Predictors of success for mandibular repositioning appliance in obstructive sleep apnea syndrome. Braz Oral Res. 2017;31(0). doi:10.1590/1807-3107bor-2017.vol31.0037
- Lam B, Sam K, Lam JCM, Lai AYK, Lam CL, Ip MSM. The efficacy of oral appliances in the treatment of severe obstructive sleep apnea. Sleep Breath. 2011;15(2):195-201. doi:10.1007/s11325-011-0496-y
- Petri N, Svanholt P, Solow B, Wildschiødtz G, Winkel P. Mandibular advancement appliance for obstructive sleep apnoea: Results of a randomised placebo controlled trial using parallel group design. J Sleep Res. 2008;17(2):221-229. doi:10.1111/j.1365-2869.2008.00645.x
- El-Solh AA, Homish GG, Ditursi G, et al. A randomized crossover trial evaluating continuous positive airway pressure versus mandibular advancement device on health outcomes in veterans with posttraumatic stress disorder. J Clin Sleep Med. 2017;13(11):1327-1335. doi:10.5664/jcsm.6808
- Phillips CL, Grunstein RR, Darendeliler MA, et al. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea: A randomized controlled trial. Am J Respir Crit Care Med. 2013;187(8):879-887. doi:10.1164/rccm.201212-2223OC
- Cohen-Levy J, Pételle B, Pinguet J, Limerat E, Fleury B. Forces created by mandibular advancement devices in OSAS patients. Sleep Breath. 2013;17(2):781-789. doi:10.1007/s11325-012-0765-4
- Dieltjens M, Vroegop AV, Verbruggen AE, et al. A promising concept of combination therapy for positional obstructive sleep apnea. Sleep Breath. 2015;19(2):637-644. doi:10.1007/s11325-014-1068-8
- Gao X, Otsuka R, Ono T, Honda EI, Sasaki T, Kuroda T. Effect of titrated mandibular advancement and jaw opening on the upper airway in nonapneic men: A magnetic resonance imaging and cephalometric study. Am J Orthod Dentofac Orthop. 2004;125(2):191-199. doi:10.1016/S0889-5406(03)00508-0
- Zhao X, Liu Y, Gao Y. Three-dimensional upper-airway changes associated with various amounts of mandibular advancement in awake apnea patients. Am J Orthod Dentofac Orthop. 2008;133(5):661-668. doi:10.1016/j.ajodo.2006.06.024
- Okawara Y, Tsuiki S, Hiyama S, Hashimoto K, Ono T, Ohyama K. Oral appliance titration and nasal resistance in nonapneic subjects. Am J Orthod Dentofac Orthop. 2004;126(5):620-622. doi:10.1016/j.ajodo.2004.05.016
- Hoffstein V, Fredberg JJ. The acoustic reflection technique for non-invasive assessment of upper airway area. Eur Respir J. 1991;4(5):602-611.
- Viviano JS. Acoustic reflection: Review and clinical applications for sleep-disordered breathing. Sleep Breath. 2002;6(3):129-149. doi:10.1055/s-2002-34315
- Viviano JS. Assessing orthotic normalization of pharyngeal dynamics. Cranio. 2004;22(3):192-208. doi:10.1179/crn.2004.025
- Jung DG, Cho HY, Grunstein RR, Yee B. Predictive value of kushida index and acoustic pharyngometry for the evaluation of upper airway in subjects with or without obstructive sleep apnea. J Korean Med Sci. 2004;19(5):662. doi:10.3346/jkms.2004.19.5.662
- Kamal I. Test-retest validity of acoustic pharyngometry measurements. Otolaryngol Neck Surg. 2004;130(2):223-228. doi:10.1016/j.otohns.2003.08.024
- Thulesius HL, Thulesius HO, Jessen M. Pharyngometric correlations with obstructive sleep apnea syndrome. Acta Otolaryngol. 2004;124(10):1182-1186. doi:10.1080/00016480410018232
- DeYoung PN, Bakker JP, Sands SA, et al. Acoustic pharyngometry measurement of minimal cross-sectional airway area is a significant independent predictor of moderate-to-severe obstructive sleep apnea. J Clin Sleep Med. 2013;09(11):1161-1164. doi:10.5664/jcsm.3158
- Kendzerska T, Grewal M, Ryan CM. Utility of acoustic pharyngometry for the diagnosis of obstructive sleep apnea. Ann Am Thorac Soc. 2016;13(11):2019-2026. doi:10.1513/AnnalsATS.201601-056OC
- Kim BY, Cho JH, Kim DH, et al. Utility of acoustic pharyngometry for screening of obstructive sleep apnea. Auris Nasus Larynx. 2019. doi:10.1016/j.anl.2019.10.007
- Friedman M, Shnowske K, Hamilton C, et al. Mandibular advancement for obstructive sleep apnea. JAMA Otolaryngol Neck Surg. 2014;140(1):46. doi:10.1001/jamaoto.2013.5746
- Kochar GD, Sharma M, Roy Chowdhury SK, et al. Pharyngeal airway evaluation following isolated surgical mandibular advancement: A 1-year follow-up. Am J Orthod Dentofacial Orthop. 2019;155(2):207-215. doi:10.1016/j.ajodo.2018.03.023
- Khosla S, Deak MC, Gault D, et al. Consumer sleep technology: An American Academy of Sleep Medicine position statement. J Clin Sleep Med. 2018;14(05):877-880. doi:10.5664/jcsm.7128
- Narayan S, Shivdare P, Niranjan T, Williams K, Freudman J, Sehra R. Noncontact identification of sleep-disturbed breathing from smartphone-recorded sounds validated by polysomnography. Sleep Breath. 2019;23(1):269-279. doi:10.1007/s11325-018-1695-6
- Fitch K, Bernstein SJ, Aguilar MD, et al. The RAND/UCLA Appropriateness Method User’s Manual: 2001.
- Lai V, Carberry JC, Eckert DJ. Sleep apnea phenotyping: Implications for dental sleep medicine. J Dent Sleep Med. 2019;6(2). doi:10.15331/jdsm.7072
- Sutherland K, Chan ASL, Ngiam J, Darendeliler MA, Cistulli PA. Qualitative assessment of awake nasopharyngoscopy for prediction of oral appliance treatment response in obstructive sleep apnoea. Sleep Breath. 2018;22(4):1029-1036. doi:10.1007/s11325-018-1624-8
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted in final revised form August 28, 2020.
Address correspondence to: Rose Sheats, DMD, MPH; Email: rosesheats@gmail.com
DISCLOSURE STATEMENT
The authors declare no conflicts of interest.