Special Article 2, Issue 7.3
Reopening an Academic Dental Sleep Medicine and Orofacial Pain Clinic Amid COVID-19
http://dx.doi.org/10.15331/jdsm.7140
Imran Y. Patel, DMD1,2; Salma I. Patel, MD, MPH1,2.; Sairam Parthasarathy, MD1,2; Rose D. Sheats, DMD, MPH3
1UAHS Center for Sleep and Circadian Sciences, University of Arizona; 2Division of Pulmonary, Allergy, Critical Care Medicine and Sleep Medicine, University of Arizona; 3University of North Carolina Chapel Hill.
CORONAVIRUS DISEASE 2019 EFFECT ON DENTISTRY
The virus resulting in coronavirus disease 2019 (COVID-19) is the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).1 SARS-CoV-2 is thought to transmit person to person predominantly via respiratory droplets that can travel horizontally up to 26 feet with viability after aerosolization of 3 hours.2 All 50 states have been affected with 1,920,904 cases of COVID-19, including 109,901 related deaths as of June 8, 2020, in the United States.3 With dental sleep medicine and orofacial pain health care providers predominantly working in the head/neck regions and because of the high likelihood of aerosolization from day-to-day patient care activities, the pandemic has placed an immense amount of strain on clinics and their patients.
In an effort to limit transmission of SARS-CoV-2 and conserve personal protective equipment for frontline health care workers, the American Dental Association appropriately recommended on March 16, 2020 that dentists limit their office visits to emergency and urgent dental care including treatment of severe dental pain and infection,4 which has left many patients without routine dental care in addition to placing significant financial burdens on dental offices.
KEEPING DOORS OPEN
Teledentistry has never needed to be at the forefront of dental care until the past few months. Dentists have needed to enhance their abilities to provide dental care virtually either through just telephone visits or audiovisual visits requiring use of different online platforms. In order to ensure continued patient care and access, we moved our clinic to a virtual platform utilizing both audiovisual platforms and telephone visits with an encouragement to continue as the Department of Health and Human Services Centers for Medicare & Medicaid Services expanded its coverage for telehealth services.5 However, given the highly procedural nature of our clinic, not as many patients (when compared to the volumes normally seen) have benefited from telehealth services.
REOPENING ALGORITHM
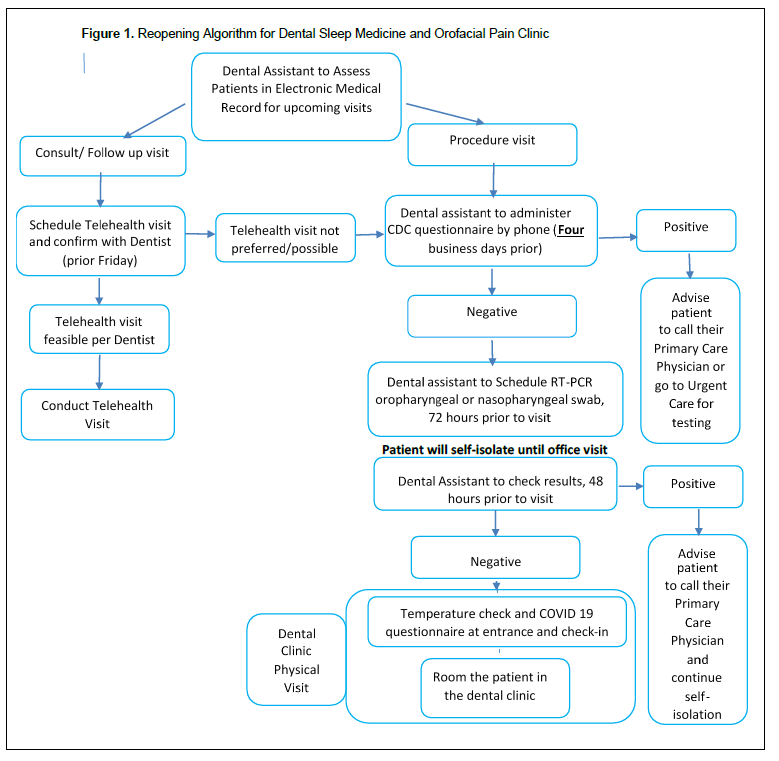
With the stay-at-home and shelter-in-place orders ending in many states, there has been pressure to resume elective procedures to keep hospitals and clinics financially afloat in addition to ensuring that patient medical and dental needs are addressed. The stay-at-home order in Arizona ended on May 15, 2020. We are therefore cautiously planning on opening our doors to elective patient visits and have developed an algorithm (Figure 1) utilizing guidance from the Centers for Disease Control and Prevention (CDC) for Health Care Workers6 in addition to available local resources and expertise. We have proposed to divide our clinic visits into two forms to simplify the re-opening algorithm: (1) nonprocedural consult visits and (2) procedural visits. For the non-procedural visits, telehealth visits will first be attempted and if not feasible or not preferred, an in-office visit will be offered adhering to the protocol for the procedural visit guidance.
For procedural visits, all patients will be screened via telephone using a COVID-19 symptoms checklist as per the CDC (fever, cough, fatigue, anorexia, shortness of breath, sputum production, myalgias, etc).6 If any of these symptoms are present, the patient is advised to contact his or her primary care physician (PCP) or go to Urgent Care for testing and to reach out to us once symptoms have resolved for re-screening with a minimum of 14 days between telephone screening visits.
If there are no alarming symptoms, the patient will be offered nucleic acid amplification tests (NAATs), primarily reverse transcription polymerase chain reaction (RT-PCR) via oropharyngeal or nasopharyngeal swab,7 72 weekday hours before the scheduled procedural visit. This allows enough time for the test results to be available for review while minimizing the time to clinic visit. The patient will be asked to self-isolate during this time to reduce the risk of infection with SARS-CoV-2.
If the RT-PCR is positive, the patient will be asked to contact his or her PCP and will not be scheduled for a procedural visit until at least 10 days since the RT-PCR has resulted in the absence of any clinic symptoms.8 If the RT-PCR is negative, the patient will again be screened for COVID-19 upon arrival to the clinic for their procedural visit. The COVID-19 questionnaire and temperature check will be administered at the entrance of the hospital prior to admittance. Additionally, all patients will be required to wear a facemask during the visit except during the clinical examination. All clinic personnel (front desk staff, dentist, and dental assistant) will be required to wear an N95 mask, face shield, gown, and gloves at all times.
As we reopen our clinic, we will initially schedule only two procedural patients in the morning and two in the afternoon in order to limit time in the lobby and patient interactions. Over the summer, we plan to gradually increase our patient load with the expectation of transitioning to our regular full schedule by August 2020. As with many dental initiatives, the effort is a collaboration between the dentist and the support staff who are actively involved in all steps in the algorithm.
We are well aware of asymptomatic COVID-19 patients and the sensitivity and specificity of RT-PCR, which may lead to erroneous test results. However, we anticipate that with careful screening of our patients and judicious utilization of technology currently available, we may safely resume care of dental sleep medicine patients and those with orofacial pain. We hope others will find our protocol useful.
Figure 1Reopening Algorithm for Dental Sleep Medicine and Orofacial Pain Clinic |
{kind=link}
CITATION
Patel IY, Patel SI, Parthasarathy S, Sheats, RD. Reopening an academic dental sleep medicine and orofacial pain clinic amid COVID-19. J Dent Sleep Med. 2020;7(3).
REFERENCES
- Coronaviridae Study Group of the International Committee on Taxonomy of V. The species Severe acute respiratory syndrome-related coronavirus: classifying 2019-nCoV and naming it SARS-CoV-2. Nat Microbiol 2020;5:536-544.
- Bahl P, Doolan C, de Silva C, Chughtai AA, Bourouiba L, MacIntyre CR. Airborne or droplet precautions for health workers treating COVID-19? J Infect Dis 2020.
- Centers for Disease Control and Prevention. Cases in the U.S. 2020. (Accessed June 8, 2020, at https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html.)
- American Dental Association. ADA develops guidance on dental emergency, nonemergency care. Recommendations part of dentists’ response over COVID-19 concerns. 2020. (Accessed May 16, 2020, at https://www.ada.org/en/publications/ada-news/2020-archive/march/ada-develops-guidance-on-dental-emergency-nonemergency-care.)
- Department of Health and Human Services Center for Medicaid and Medicare Services. Medicare and Medicaid Programs, Basic Health Program, and Exchanges; Additional Policy and Regulatory Revisions in Response to the COVID-19 Public Health Emergency and Delay of Certain Reporting Requirements for the Skilled Nursing Facility Quality Reporting Program. 2020. (Accessed May 16, 2020, at https://www.cms.gov/files/document/covid-medicare-and-medicaid-ifc2.pdf.)
- Centers for Disease Control and Prevention. Information for Healthcare Professionals about Coronavirus (COVID-19). 2020. (Accessed May 16, 2020, at https://www.cdc.gov/coronavirus/2019-ncov/hcp/index.html.)
- Patel A, Jernigan DB, 2019-nCoV CDC Response Team. Initial Public Health Response and Interim Clinical Guidance for the 2019 Novel Coronavirus Outbreak - United States, December 31, 2019-February 4, 2020. MMWR Morb Mortal Wkly Rep 2020;69:140-6.
- Centers for Disease Control and Prevention. Dental Settings Interim Infection Prevention and Control Guidance for Dental Settings During the COVID-19 Response. 2020. (Accessed May 19, 2020, at https://www.cdc.gov/coronavirus/2019-ncov/hcp/dental-settings.html.)
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication May 25, 2020
Accepted for publication May 27, 2020
Address correspondence to: Imran Patel, DMD, University of Arizona College of Medicine, PO Box 245040-A 1501 N. Campbell Ave. Tucson, AZ 85724-5030A; Phone: (520) 626-8309; Fax: (520) 626-1876; Email: ipatel@deptofmed.arizona.edu
DISCLOSURE STATEMENT
Dr. Parthasarathy has a patent UA 14-018 U.S.S.N. 90 61/884,654; PTAS 502570970 (Home breathing device) issued. The above-mentioned conflicts including the patent are unrelated to the topic of this paper. Dr. I. Patel, Dr. S. Patel and Dr. Sheats have no conflicts of interest to report.
PDF