Special Article 1, Issue 9.4
Dental Sleep Medicine Standards for Screening, Treatment, and Management of Sleep-Related Breathing Disorders in Adults Using Oral Appliance Therapy: An Update
http://dx.doi.org/10.15331/jdsm.7266Standards for Practice Committee of the American Academy of Dental Sleep Medicine: Mitchell Levine, DMD (Chair)1; Michelle K. Cantwell, DMD2; Kevin Postol, DDS3; David B. Schwartz, DDS4
1Saint Louis University Center for Advanced Dental Education, St. Louis, MO; 2Wellspan Health, Pulmonary and Sleep Medicine, York, PA; 3Sleep Disordered Dentistry, Ballwin, MO; 4Dental Professionals, Skokie, IL
Watch Video Summary
ABSTRACT
Oral appliance therapy is a proven, effective treatment for obstructive sleep apnea (OSA) and snoring. With more than 54 million adults having OSA in the United States, dentists play an integral role in increasing access to care for those with undiagnosed and untreated OSA. These standards outline an approach to patient management that underscores the collaborative care that is necessary between dentists and physicians and provides guidance for patient examination, patient screening, treatment management, education, and follow-up care. Although this article provides best practices for dental sleep medicine as it currently exists, the fluid and dynamic nature of DSM should be recognized, with the understanding that periodic updates to these standards will be required.
Keywords:
best practice, obstructive sleep apnea, oral appliance therapy, sleep-related breathing disorders, standard
Citation:
Levine M, Cantwell M, Postol K, Schwartz D. Dental sleep medicine standards for screening, treating, and management of sleep-related breathing disorders in adults using oral appliance therapy. J Dent Sleep Med. 2022;9(4)
INTRODUCTION
The American Academy of Dental Sleep Medicine (AADSM) initially published Dental Sleep Medicine Standards for Screening, Treating, and Managing Adults With Sleep-Related Breathing Disorders in 2018.1 The AADSM provides this update to reflect new and relevant educational considerations in the training of dentists and their staff members and the most up-to-date literature that supports these standards. This article incorporates evolutionary trends in the field and replaces the previous dental sleep medicine (DSM) standards for clinical practice.In the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10), obstructive sleep apnea (OSA) is listed as a sleep disorder and snoring is a sign of disordered breathing during sleep. Collectively, OSA and snoring constitute most sleep-related breathing disorders (SRBD). There is robust literature citing an association between OSA and cardiovascular, metabolic, and neurologic systems insult. An estimated 54 million adults in the United States have some degree of sleep apnea, with an estimated 45% of the population snoring, at least occasionally.2–4 Additionally, there is a plethora of literature to support the utility of oral appliances (OAs) or mandibular advancement devices (MADs), with these devices providing effective treatment for OSA and snoring in adults.5–7
The AADSM recognizes the variable nature of DSM curricula within the US and Canadian dental schools. To address this gap, the AADSM launched the AADSM Mastery Program (Mastery) in 2018. Mastery is a standardized, evidence-based curriculum designed to meet the growing need for qualified dentists and address access to care issues. Accordingly, Mastery affords dentists postgraduate education in the proper screening of patients and the management/follow-up of oral appliance therapy (OAT) to maximize patient outcomes.
In 2015, the AADSM and the AASM issued the “Clinical Practice Guideline for the Treatment of OSA and Snoring With OAT.” The guideline offers clarity on the desired qualifications of a dentist participating in the treatment and ongoing management of OSA and/ or snoring. The guideline states “ … dentist should receive diplomate certification in DSM...or seek the designation of “qualified dentist (QD).”8 Throughout this article, the term “qualified dentists” universally includes American Board of Dental Sleep Medicine (ABDSM) diplomates, AADSM qualified dentists, and ABDSM international certificants. At a minimum, these designations require successful completion of either all or certain components of Mastery. Intended competencies of a QD include, but are not limited to:
- Clinical Knowledge
- Basic sleep physiology, including the pathophysiology of SRBD
- Dentist and team member roles in managing SRBD
- Evidence-based therapeutic options and an awareness of emergent treatments and technologies for SRBD
- Comorbid nature of OSA and temporomandibular disorders and treatment effects from OAT on the temporomandibular joint (TMJ), dental occlusion, and related structures
- Patient Care
- Screening and risk assessment of SRBD
- Comprehensive, DSM-focused medical/dental examination and history, including relevant imaging
- Understanding objective sleep testing and other complementary assessments
- Gathering and synthesizing information from sleep medicine patients to appropriately screen patients and establish a treatment plan including: OA selection, device fitting and calibration, long-term care, and management of potential side effects. These decisions should take into consideration patient values and preferences.
- Learning and Improvement
- Clinical practice and decision-making guided by evidence-based principles
- Continuing education
- Reflective practice and personal growth
- Identifying opportunities to standardize, simplify, and improve quality of care
- Professionalism
- Ethical principles, including billing and coding practices
- Accountability and team training with adherence to applicable state and federal laws and regulations
- Subjective, Objective, Assessment and Plan (SOAP) note documentation, maintenance of treatment records, and protection of patient information
- Collaborative model of interdisciplinary care
- Informed consent
- Interpersonal and Communication Skills
- Effective patient communication
- Barrier and bias mitigation
- Interprofessional and team communication
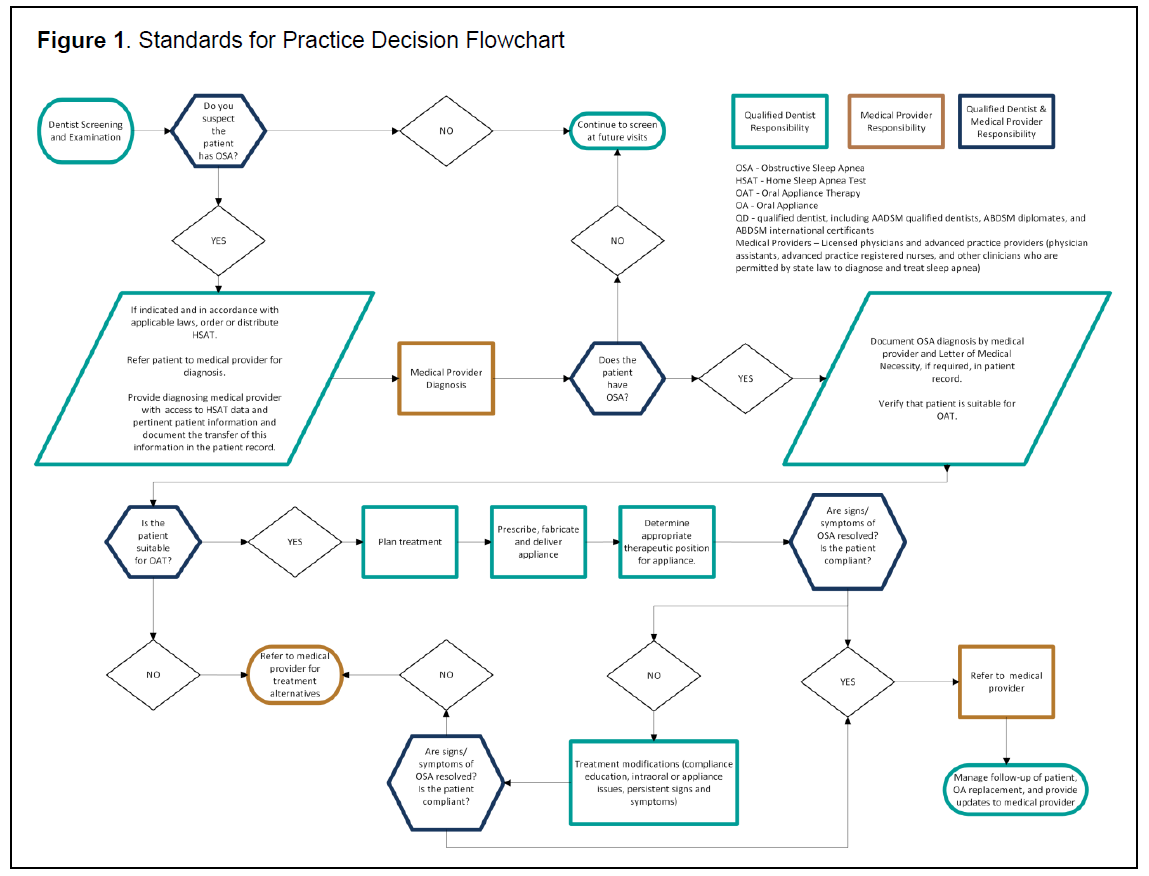
This article provides updated guidelines for the use of OAT as a treatment for OSA and snoring. Accordingly, this article revisits how an adult patient suspected of having a SRBD might be identified and then details a clinical care pathway for the management and treatment of the disorder (Figure 1). The article then describes standards for screening, patient examination, education, treatment management, and follow-up care. By standardizing the field, it is hoped that a methodologic approach to patient care is encouraged to enable the QD to collaborate with the patient’s medical provider(s) to deliver the best possible care. For the purposes of this article, the term “medical provider” includes licensed physicians, as well as advanced practice providers (physician assistants, advanced practice registered nurses, and other clinicians who are permitted by state law to diagnose and treat sleep apnea).
Figure 1Standards for Practice Decision Flowchart |
{kind=link}
There are two pathways that may lead a dental patient to evaluation for OSA, subsequent diagnosis, and OAT. In the first instance, a patient may initiate a visit to the QD, who provides a screening consultation that may include a review of the chief complaint(s), a clinical assessment of oral/craniofacial risk factors, and validated questionnaire(s). In 2017, the American Dental Association established a policy that all dentists should screen patients.9 If appropriate and in accordance with applicable laws, a home sleep apnea test (HSAT) may be ordered and administered by the QD, or the patient may be referred to a medical provider for sleep testing. In either instance, the patient must be referred to a medical provider, who is responsible for diagnosing OSA and/or other sleep-related conditions. Prior to commencing OAT, the QD should determine whether the patient is a candidate for OAT and select a suitable appliance through a comprehensive DSM examination that reviews oral/craniofacial condition risks and predictive factors for successful OAT.10 This examination should include informed consent and financial arrangements necessary to commence OAT. Upon patient acceptance of the treatment plan, relevant dental records and imaging may be obtained to determine the appropriate OA within the context of the patient’s oral presentation. Upon resolution of the signs and symptoms of OSA, the QD may elect to utilize pulse oximetry or HSAT, in accordance with applicable laws, to aid in identifying the appropriate therapeutic position of the appliance.11 Ultimately, the patient is referred to the medical provider for verification of treatment efficacy and long-term follow-up. If signs and symptoms do not resolve and treatment modifications do not lead to resolution, the patient should be referred to the medical provider for adjunct treatment or treatment alternatives.
In the second pathway, a medical provider may refer a patient with a diagnosis of OSA to the QD for OAT to manage the OSA. The QD should determine whether the patient is a candidate for OAT through a comprehensive examination and follow the same steps outlined in the first pathway.
Optimal outcomes are often best realized when the QD, medical providers, and general dentist (if not the QD) collaborate to achieve the shared goal of successful treatment. The QD should frequently and openly communicate with these providers throughout treatment.
PRETREATMENT EXAMINATIONS
Screening Examination
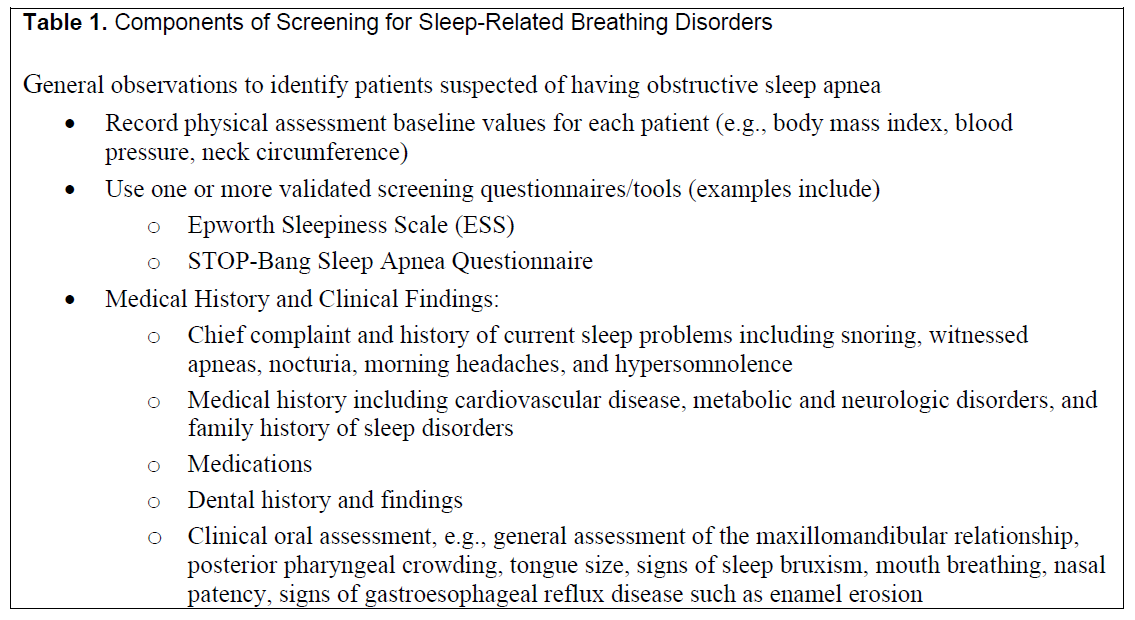
Patients should be screened for OSA using validated screening tools. The goal of pretreatment examination or initial screening is to identify patients with increased suspicion of having OSA. The use of validated tools (e.g. Epworth Sleepiness Scale, STOP-BANG Questionnaire), which focus on subjective and objective criteria, offer increasing predictive value with increasing OSA severity.12,13 Certain aspects of this screening visit may be completed by appropriately trained dental team members. Snoring cannot be distinguished from OSA and patients who snore should not be treated in the absence of a diagnosis.
It is important to note that although screening tools are valuable for identifying patients suspected of having OSA, they are nondiagnostic and not a substitute for a diagnostic sleep apnea test. Additionally, an oral examination should be performed to identify key physical features associated with OSA and snoring. Important considerations in patient screening for OSA are listed in Table 1.
Table 1Components of Screening for Sleep-Related Breathing Disorders |
{kind=link}
Comprehensive Dental Sleep Medicine Examination
Prior to commencing OAT, the QD should complete a comprehensive DSM examination that includes visualization, descriptive assessment, and relevant imaging of the craniofacial complex and the upper airway. This examination may occur simultaneously with screening or at a separate time. A list of important considerations in the comprehensive DSM examination for the patients with OSA is found in Table 2.
Table 2Components of Comprehensive Dental Sleep Medicine Examination |
{kind=link}
A comprehensive DSM examination of the patient should provide the necessary information to determine whether the patient is suitable for an OA and to assist with proper appliance selection. If the patient is a suitable candidate for an OA, both intraoral and extraoral photographs may be obtained as a record of the pretreatment dental condition. Additionally, conventional dental impressions or digital scans will be needed to create the OA and may be retained as part of the patient’s record for as long as state regulations require.
DIAGNOSIS
OSA Diagnosis
The QD may interpret and collate findings as part of the pretreatment examinations. If the patient is suspected of having OSA, the QD may choose to order or distribute a HSAT if the patient is an appropriate candidate, and it is in accordance with applicable laws. Alternatively, they may choose to refer the patient to a medical provider for sleep testing. In either instance, the patient must be referred to the medical provider for diagnosis. During the referral process, the medical provider should be sent any pertinent patient information and any information pertaining to the HSAT. When applicable, interpretation of sleep test data and diagnosis should be provided by a board-certified sleep medicine physician. Regardless of the type of testing used to assist with the diagnosis, the responsibility for diagnosis lies with a medical provider. If OSA is diagnosed, the medical provider may refer the patient to the QD for OAT and send any documentation of diagnosis. The importance of bidirectional referral patterns should be recognized, with the QD referring to the medical provider and the medical provider referring to the QD.
Snoring Diagnosis
In the confirmed absence of OSA, patients with a diagnosis of snoring may choose an oral device as first-line therapy.14 A referral for an OA to manage snoring is not required and treatment may commence at the discretion of the QD.
TREATMENT OPTIONS
In the event of a primary snoring diagnosis. OAT should be prescribed as first-line therapy. In the event of an OSA diagnosis, OAT may be a first-line therapy15 or may be used when other treatment choices have fallen short of maximum efficacy.16 There are several reasons to consider OAT as a viable therapy for OSA. First, several studies demonstrate that OAs and positive airway pressure (PAP) therapy are comparable in improving daytime somnolence, hypertension, neurocognitive function, quality-of-life indices, and cardiovascular mortality.7,17 Second, OAs are indicated for patients with mild, moderate, and severe OSA.18 Third, patients tend to strongly prefer OAT when compared to PAP and tend to be more compliant with treatment than patients using PAP;19,20 therefore, patient preference should be carefully considered when recommending OSA therapy.
Patients successfully treated with PAP should be encouraged to continue this treatment course. However, PAP intolerance remains a pervasive problem. OAT is recommended for patients who are intolerant of PAP or in whom PAP therapy has failed, or who prefer OAT. PAP intolerance is a frequent chief complaint among referrals for OAT.
Patients using PAP may often struggle with pressure settings and mask leaks, leading to PAP adherence issues. Combination therapy, in which an OA is used in concert with PAP, may allow for lower pressure and improve PAP adherence.21 Combination therapy may reduce upper airway resistance and allow a more comfortable and lower pressure required to maintain patency of the airway. The use of customized masks and interfaces can be fabricated by QDs to facilitate the use of combination therapy.22 Some patients may also elect to alternate between PAP and OAT to accommodate lifestyle needs or to minimize the side effects of either therapy.
Depending on OSA severity, surgery23,24 may be another treatment option. Noninvasive options such as OAT and PAP should be offered first, prior to considering more invasive treatments. However, OA can also be used in concert with surgery and may further reduce signs and symptoms of OSA. The most effective treatment plans for resolution of OSA are comprehensive and interdisciplinary in nature. For many patients, this will include weight reduction, positional therapy, and/or behavioral modifications on their own, or in combination with OAT.
Following a diagnosis of OSA, the QD should collaborate with the medical provider(s) to develop properly sequenced treatment(s), involving either solo OAT or OAT in combination with nonsurgical or surgical therapies. Prior to treatment, QDs should work with medical providers and patients to determine the goal of treatment success and identify agreed-upon metrics for success. This discussion should include parameters for verification of treatment efficacy.
There are many instances in which patients with a diagnosis of OSA elect not to continue with active treatment. For example, many patients are prescribed PAP and find they are intolerant or unable to use PAP and may abandon therapy. In these cases, QDs can play a larger role in OSA treatment by prescribing OAT to such patients. If a patient seeks treatment for OAT directly and has documentation of the diagnosis by a medical provider, it is appropriate, in accordance with applicable laws, to initiate OAT and communicate this with the patient’s medical providers and general dentist (if not the QD).
Although it is accepted that face-to-face interaction between collaborating providers will improve patient outcomes, much of the communication between clinicians occurs asynchronously. Further recommendations on the timing and format for these discussions may be found in the AADSM’s “Protocol for Communicating With a Patient’s Treating Physician.”25
PATIENT EDUCATION
Many patients seek to understand the implications of their SRBD and what, if any, mitigating actions may be taken to reduce the collective effect on their overall health. The patient should be educated about how OSA can lead to untoward effects on bodily functions, including those within the circulatory, metabolic, and neurologic systems. Additionally, the QD should convey risk factors related to demographics, ethnicity, and sex. In addition to these factors, there are known risk modifiers that can shape disease severity. The patient should be advised that disease severity and/or treatment success may be negatively influenced by using tobacco, alcohol, caffeine, or recreational substances.26,27 The effect of both weight loss and weight gain should be discussed with the patient.27 The educated and informed patient may attempt to reduce the effects of disease by modifying these behaviors.
The patient undergoing OAT should be informed of their OSA severity and should be given a very basic explanation of their sleep study. The patient should also be informed that OAT success may be affected by fragmented sleep, oxygen desaturation, and other coexisting sleep disorders. The QD should discuss with the patient the metrics that they and their medical provider decided would be critical for determining whether OAT treatment is successful. Additionally, the patient should be informed of what additional therapies might be considered in the face of an inadequate response to OAT. Open communication with the patient is important in achieving success with OAT, and the QD should be sensitive to patient concerns and desired outcomes. 26–28
Finally, the patient should be educated about the importance of sleep hygiene and duration.29 The patient should understand the effect of ambient room lighting, temperature, the use of electronics in bed, and the importance of regular sleep schedules. Although these considerations may not directly affect OA efficacy, they can collectively fragment sleep and exacerbate daytime sleepiness, thus reducing the patient’s perception of OA benefit.
OAT INITIATION
QDs have the appropriate training to evaluate the patient’s oral cavity and suitability for an OA. The QD must examine the health and stability of the dentition including angulation, alignment and contours of the teeth, the shape of the arch, and how the lower and upper jaws align to determine whether an OA may be appropriate. The QD must also select a device that has the appropriate materials and retention to ensure that the appliance can effectively move and keep the jaw in the appropriate position throughout the night to manage the OSA, as well as maximize comfort and minimize side effects to ensure compliance.
Once the patient is determined to be a suitable candidate for OAT, the QD should use their knowledge and understanding of the patient’s health history, dental history, dental and skeletal anatomy, and TMJ history to develop a treatment plan.
Initiating OAT includes obtaining informed consent from the patient and verifying the diagnosis from a medical provider and should allow for modification of the treatment plan as needed to obtain the desired therapeutic result. Informed consent is the process by which appropriate information is disclosed to a competent patient, so the patient can make a voluntary choice to accept or refuse treatment. The patient should be provided with an opportunity to ask questions about the risks associated with treatment, as well as be educated about the risks associated with no treatment. Informed consent also requires that the patient is informed about alternate therapies to OAT, such as PAP therapy, positional therapy, or sleep-related surgery. Upon acceptance of the treatment plan, the patient should sign the informed consent in the presence of the QD or other dental team members. The QD should then countersign and date the document, which should be kept as part of the patient’s record of care.
OA SELECTION
Selection of an appropriate OA should include both patient’s preference as well as the QD’s assessment. The 2019 AADSM Definition of an Effective Oral Appliance for the Treatment of Obstructive Sleep Apnea and Snoring describes the purpose, function, and physical features of an effective OA.30An effective OA helps to protrude and stabilize the mandible to preserve the patency of the upper airway during sleep.30 Custom, adjustable dual-arch OAs have been shown to be highly efficacious for treating primary snoring and OSA.31
Appliance selection should consider craniofacial structures and oral, dental, and periodontal tissues. Other elements to consider include the patient’s cognitive ability, manual dexterity, visual acuity, range of motion, and nasal patency, as well as number, location, and health of remaining teeth. The clinical tooth height, angulation, undercuts, current dental restorative conditions, and anticipated dental restorative needs, along with allergies and/or sensitivities, are also to be considered because they may limit the type and material to be used in the fabrication of an OA.
Additionally, appliance selection should be patient-centered and take preferences into account (perceived comfort, ease of use, patient financial considerations). The appliance should not be selected solely due to the requirements of governmental or private insurers. Ultimately, the choice of the appliance should be the decision of the QD and the patient. As materials, methods of engineering, and technology evolve this will increase the likelihood of treatment success and patient compliance.
OA FABRICATION AND THE CONSTRUCTION BITE
The QD fabricates the OA by first taking accurate digital or analog impressions and a protrusive bite record.. The initial protrusive setting should be at the QD’s discretion, based on patient comfort and clinical data from the comprehensive DSM examination.11 Various types of protrusive bite records may be used and customized to accommodate an individual’s dental, muscular, and anatomic range. Although the QD has discretion as to the initial position of the OA, literature suggests a protrusive range of 25% to 75% is within both the comfort and therapeutic range.32–34 Each OA may require a different vertical dimension to allow for proper fabrication. Both the horizontal and vertical dimensions should be considered in the context of the patient’s dental and craniofacial anatomy and occlusion. It should be noted that increasing vertical dimension has been associated with reduced efficacy of the OA.35
OA DELIVERY
The QD should verify the fit and comfort of the OA, and the QD or team members should review the adjustment protocol, home care instructions, and the warranty information specific to the OA selected. It is recommended that a written copy of the instructions, delivery form, and warranty be signed and dated by the patient and a team member, with one copy being provided to the patient and the other retained in the medical record.
The QD should consider how to maximize comfort and minimize the development of dental changes including, but not limited to, occlusal irregularities and interdental spacing. Additionally, appropriate measures should be taken to attenuate the possible development of jaw discomfort and muscle fatigue. These provisions may include morning exercises, the use of a morning repositioning device, and associated palliative care. Ideally, follow-up with the patient after OA delivery should be done to ascertain whether the patient has any immediate concerns, and the follow-up should be done in a timely manner to evaluate efficacy and comfort, and to address any patient concerns. In the event of combination therapy, there should be ongoing coordination with the durable medical equipment provider and/or referring medical provider.
SIDE EFFECTS
The potential for side effects6,36,37 must be explained to the patient and discussed prior to initiating treatment and as situations arise during treatment. The potential for TMJ-related side effects, intraoral tissue-related side effects, occlusal changes, damage to teeth or restorations, and appliance issues are among the topics that should be reviewed prior to treatment and during the informed consent process.37
Management of reported side effects36 should be well documented and tailored to the individual patient’s needs. When applicable, side effects and management techniques should be relayed to the general dentist. The presence of side effects should be discussed with the general dentist and medical provider as pertaining directly to an individual patient’s clinical history. Should side effects affect adherence or effectiveness of the OA or if treatment is discontinued, the patient’s medical provider should be informed.37
OA CALIBRATION
Within 30 days after insertion and on regular intervals as needed, the patient should be evaluated and reassessed for signs and symptoms with the same questionnaires/tools used at initial assessment.11 Any advancement of the OA from its initial setting is based on multiple factors including the patient’s range of motion, level of disease severity, patient comfort, and resolution or improvement of signs and symptoms.11
The QD will need to determine an appropriate endpoint to the OA advancement process that achieves improvement of signs, symptoms, or objective indices, while also allowing the patient to use the appliance comfortably, on a nightly basis. Excessive increase in the patient’s protrusive position may affect patient compliance and has not been shown to guarantee improved efficacy. In some instances, overprotrusion may worsen the patient’s sleep-disordered breathing.32 However, individuals who fail to achieve satisfactory improvements in signs and symptoms or who have lack of improvement in objective parameters may show further improvement with continued gradual advancement.11
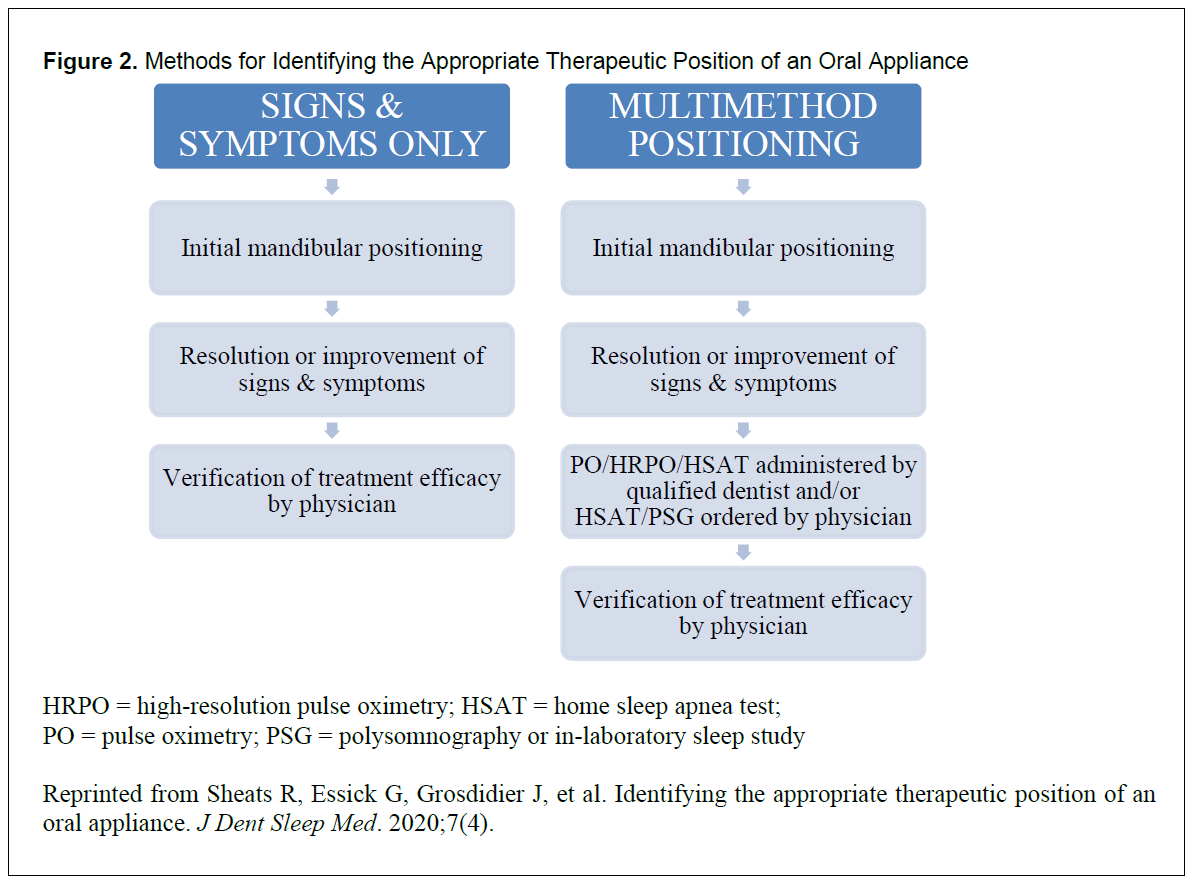
As such, the QD and medical provider should have a mutually agreed-upon process that enables the OA to be assessed objectively. The use of pulse oximeters or HSAT to verify the therapeutic position of the OA may be appropriate and used in accordance with applicable laws.9,38 OA advancement should continue until target parameter values are attained, can no longer be improved, or the maximum comfortable position is reached.11 Ultimately, any decisions regarding the use of HSATs or pulse oximetry, and the resulting objective data, should be made in concert with the patient, the treating medical provider, and QD. Figure 2 provides additional details.
Figure 2Methods for Identifying the Appropriate Therapeutic Position of an Oral Appliance |
{kind=link}
Upon reaching the therapeutic position, the patient should be referred to the medical provider to verify treatment efficacy. The medical provider should be given any notes and/or findings that may contribute to their assessment. Should the medical provider deem the calibrated position to be subtherapeutic, the medical provider and QD should discuss the possibility of further calibration, adjunct treatment, or alternative treatment. In consultation with the patient’s medical provider, a patient may elect to continue with OAT despite subtherapeutic results. The patient’s general dentist should also be kept abreast of treatment progress.
OA FOLLOW-UP/MANAGEMENT
Patient compliance with OAT should also be evaluated. The AADSM defines compliance as “the appliance being worn for a minimum of ≥80% per night, starting when the OA is placed in the mouth and ending when the OA is removed from the mouth, ≥5 nights per week.”29 Compliance can be measured either subjectively (diaries and questionnaires) and/or objectively (use of compliance monitors). OA compliance should stress that the patient should sleep a minimum of 7 hours per night and wear their appliance for the duration of their sleep every night. Additionally, as part of this discussion on compliance and duration of sleep, proper sleep hygiene should also be reinforced.29
The patient may be categorized as fully compliant, improving over time, or noncompliant based on the collected compliance data. Because patients with untreated or subtherapeutic OSA can eventually experience long-term health risks, noncompliant patients should be referred to their medical provider to consider alternate therapies.29
OAs should be evaluated by the QD on a yearly basis for signs of wear, fractures, and bacterial and/ or fungal growth and replaced according to the patient’s needs. The medical provider should also be notified if the patient terminates OAT.
OA REPLACEMENT
DISCUSSION
Additionally, telehealth usage has revolutionized the field of DSM. Telehealth visits may be used during screening, as well as for many follow-up visits with patients. The use of telehealth could expand access to care to a greater number of patients, especially those who live in areas that are remote or do not have a nearby QD. As telehealth is considered, it is important to keep in mind that the level of service provided during a telehealth appointment should be the same as an in-person appointment. Each patient’s needs vary, so the use of telehealth should be flexible and patients should be allowed to choose telehealth versus in-person appointments based on their technologic capabilities and preference. To keep up to date, QDs should participate in an ongoing, comprehensive educational strategy best suited to their individual learning.
METHODOLOGY
ACKNOWLEDGMENTS
Disclaimer: These standards were developed by the AADSM to assist dentists in making decisions about appropriately screening, managing, and treating adults with obstructive sleep apnea and snoring using oral appliance therapy. The information and recommendations within this document reflect current scientific and clinical knowledge at the time of publication, are only current as of their publication date, and are subject to change without notice as advances emerge. Variations in practice, which take into account applicable laws and regulations, the needs of individual patients, and the resources and limitations unique to a practice, may warrant approaches, treatments and/or procedures that differ from the recommendations outlined in this document. The recommendations in this document should not be construed as dictating an exclusive course of management, nor does the use of such recommendations guarantee a particular outcome. This document is not intended to displace a dentist’s best clinical judgement. It is published for educational and informational purposes only; the AADSM does not “approve” or “endorse” any specific methods, practices, or sources of information.
ABBREVIATIONS
AADSM – American Academy of Dental Sleep Medicine
AADSM qualified dentists – Licensed dentists who have professional liability coverage and successfully completed required continuing education in dental sleep medicine to be awarded the AADSM Qualified Dentist designation
ABDSM – The American Board of Dental Sleep Medicine is an independent, self-designated nonprofit testing organization of dentists who treat snoring and obstructive sleep apnea with oral appliance therapy
ABDSM diplomates – Licensed dentists who have received the highest credential a dentist can earn in dental sleep medicine. They have demonstrated competency in dental sleep medicine by passing a rigorous written examination
ABDSM international certificants – Dentists licensed outside the US or Canada who have demonstrated competency in dental sleep medicine by passing a rigorous written examination
DSM – dental sleep medicine
HSAT – home sleep apnea test
Medical Providers – Licensed physicians and advanced practice providers (physician assistants, advanced practice registered nurses, and other clinicians who are permitted by state law to diagnose and treat sleep apnea)
Mastery – AADSM Mastery Program
OA – oral appliance
OAT – oral appliance therapy
OSA – obstructive sleep apnea
PAP – positive airway pressure
QD – qualified dentist, including AADSM qualified dentists, ABDSM diplomates, and ABDSM international certificants
SRBD – sleep-related breathing disorders
REFERENCES
- Levine M, Bennett KM, Cantwell MK, Postol K, Schwartz DB. Dental sleep medicine standards for screening, treating and managing adults with sleep-related breathing disorders. Standards of Practice Committee of the American Academy of Dental Sleep Medicine. J Dent Sleep Med. 2018;5(3)61-68.
- Frost & Sullivan. Hidden Health Crisis Costing America Billions - Underdiagnosing and Undertreating Obstructive Sleep Apnea Draining Healthcare System. http://www.aasmnet.org/Resources/pdf/sleep-apnea-economic-crisis.pdf. Accessed July 1, 2022.
- Why Do People Snore? Answers for Better Health | Johns Hopkins Medicine. https://www.hopkinsmedicine.org/health/wellness-and-prevention/why-do-people-snore-answers-for-better-health. Accessed March 1, 2022.
- Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687-698.
- Gagnadoux F, Fleury B, Vielle B, et al. Titrated mandibular advancement versus positive airway pressure for sleep apnoea. Eur Respir J. 2009;34(4):914-920.
- Marklund M, Verbraecken J, Randerath W. Non-CPAP therapies in obstructive sleep apnoea: Mandibular advancement device therapy. Eur Respir J. 2012;39(5):1241-1247.
- Phillips CL, Grunstein RR, Darendeliler MA, et al. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea. Am J Respir Crit Care Med. 2013;187(8):879-887.
- Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: An update for 2015. J Clin Sleep Med. 2015;11(7):773-828.
- ADA Adopts Policy on Dentistry’s Role in Treating Obstructive Sleep Apnea, Similar Disorders. American Dental Association. https://www.ada.org/-/media/project/ada-organization/ada/ada-org/files/resources/research/the-role-of-dentistry-in-sleep-related-breathing-disorders.pdf. Accessed July 1, 2022.
- Okuno K, Pliska BT, Hamoda M, Lowe AA, Almeida FR. Prediction of oral appliance treatment outcomes in obstructive sleep apnea: A systematic review. Sleep Med Rev. 2016;30:25-33.
- Sheats R, Essick G, Grosdidier J, et al. Identifying the appropriate therapeutic position of an oral appliance. J Dent Sleep Med. 2020;7(4).
- Ramachandran SK, Josephs LA. A Meta-analysis of clinical screening tests for obstructive sleep apnea. Anesthesiology. 2009;110(4):928-939.
- Boynton G, Vahabzadeh A, Hammoud S, Ruzicka DL, Chervin RD. Validation of the STOP-BANG Questionnaire among patients referred for suspected obstructive sleep apnea. J Sleep Disord Treat Care. 2013;2(4).
- Almeida FR, Lowe AA. Principles of oral appliance therapy for the management of snoring and sleep disordered breathing. Oral Maxillofac Surg Clin North Am. 2009;21(4):413-420.
- Park P, Jeon HW, Han DH, et al. Therapeutic outcomes of mandibular advancement devices as an initial treatment modality for obstructive sleep apnea. Medicine (Baltimore). 2016;95(46).
- Cistulli PA, Gotsopoulos H, Marklund M, Lowe AA. Treatment of snoring and obstructive sleep apnea with mandibular repositioning appliances. Sleep Med Rev. 2004;8(6):443-457.
- Sutherland K, Vanderveken OM, Tsuda H, et al. Oral appliance treatment for obstructive sleep apnea: An update. J Clin Sleep Med. 2014;10(2):215-227.
- Trzepizur W, Cistulli PA, Glos M, et al. Health outcomes of continuous positive airway pressure versus mandibular advancement device for the treatment of severe obstructive sleep apnea: an individual participant data meta-analysis. Sleep. 2021;44(7): zsab015.
- Tan YK, L’Estrange PR, Luo YM, et al. Mandibular advancement splints and continuous positive airway pressure in patients with obstructive sleep apnoea: A randomized cross-over trial. Eur J Orthod. 2002;24(3):239-249.
- Vanderveken OM, Dieltjens M, Wouters K, De Backer WA, Van De Heyning PH, Braem MJ. Objective measurement of compliance during oral appliance therapy for sleep-disordered breathing. Thorax. 2013;68(1):91-96.
- Liu HW, Chen YJ, Lai YC, et al. Combining MAD and CPAP as an effective strategy for treating patients with severe sleep apnea intolerant to high-pressure PAP and unresponsive to MAD. PLoS One. 2017;12(10).
- Tanaka Y, Adame JMl, Kaplan A, Almeida FR. The simultaneous use of positive airway pressure and oral appliance therapy with and without connector: A preliminary study. J Dent Sleep Med. 9(2):2022.
- Garg RK, Afifi AM, Sanchez R, King TW. Obstructive sleep apnea in adults: The role of upper airway and facial skeletal surgery. Plast Reconstr Surg. 2016;138(4):889-898.
- Phan NT, Wallwork B, Panizza B. Surgery for adult patients with obstructive sleep apnoea: A review for general practitioners. Aust Fam Physician. 2016;45(8):574-578.
- White J, Richardson S, Levine M. Protocol for communicating with a patient’s treating physician. American Academy of Dental Sleep Medicine. https://www.aadsm.org/referral_and_marketing_resourc.php. Accessed July 1, 2022.
- Peppard PE, Austin D, Brown RL. Association of alcohol consumption and sleep disordered breathing in men and women. J Clin Sleep Med. 2007;3(3):265.
- Wetter DW, Young TB, Bidwell TR, Badr MS, Palta M. Smoking as a risk factor for sleep-disordered breathing. Arch Intern Med. 1994;154(19):2219-2224.
- Newman AB, Foster G, Givelber R, Nieto FJ, Redline S, Young T. Progression and regression of sleep-disordered breathing with changes in weight: the Sleep Heart Health Study. Arch Intern Med. 2005;165(20):2408-2413.
- Radmand R, Chiang H, Di Giosia M, et al. Defining and measuring compliance with oral appliance therapy. J Dent Sleep Med. 2021; 8(3).
- Mogell K, Blumenstock N, Mason E, Rohatgi R, Shah S, Schwartz D. Definition of an effective oral appliance for the treatment of obstructive sleep apnea and snoring: An update for 2019. J Dent Sleep Med. 2019;6(3).
- Gjerde K, Lehmann S, Berge ME, Johansson AK, Johansson A. Oral appliance treatment in moderate and severe obstructive sleep apnoea patients non-adherent to CPAP. J Oral Rehabil. 2016;43(4):249-258.
- Aarab G, Lobbezoo F, Hamburger HL, Naeije M. Effects of an oral appliance with different mandibular protrusion positions at a constant vertical dimension on obstructive sleep apnea. Clin Oral Investig. 2010;14(3):339-345.
- Tegelberg Å, Walker-Engström ML, Vesding O, Wilhelmsson B. Two different degrees of mandibular advancement with a dental appliance in treatment of patients with mild to moderate obstructive sleep apnea. Acta Odontol Scand. 2003;61(6):356-362.
- Walker-Engström ML, Ringqvist I, Vestling O, Wilhelmsson B, Tegelberg A. A prospective randomized study comparing two different degrees of mandibular advancement with a dental appliance in treatment of severe obstructive sleep apnea. Sleep Breath. 2003;7(3):119-130.
- Vroegop AV, Vanderveken OM, Van de Heyning PH, Braem MJ. Effects of vertical opening on pharyngeal dimensions in patients with obstructive sleep apnoea. Sleep Med 2012;13:314-316.
- Sateia MJ. International classification of sleep disorders-third edition: highlights and modifications. Chest. 2014;146(5):1387-1394.
- Sheats RD, Schell TG, Blanton AO, et al. Management of side effects of oral appliance therapy for sleep-disordered breathing. J Dent Sleep Med. 2017;04(04):111-125.
- Schwartz D, Adame M, Addy N, et al. American Academy of Dental Sleep Medicine Position on the Scope of Practice for Dentists Ordering or Administering Home Sleep Apnea Tests. J Dent Sleep Med. 2020;7(4).
- Ainge-Allen HW, Yee BJ, Ip MSM. Contemporary Concise Review 2020: Sleep. Respirology. 2021;26(7):700-706.
- Al-Jewair TS, Al-Jasser R, Almas K. Periodontitis and obstructive sleep apnea’s bidirectional relationship: a systematic review and meta-analysis. Sleep Breath. 2015;19(4):1111-1120.
- Vanderveken OM, Dieltjens M, Wouters K, De Backer WA, Van De Heyning PH, Braem MJ. Objective measurement of compliance during oral appliance therapy for sleep-disordered breathing. Thorax. 2013;68(1):91-96.
SUBMISSION AND CORRESPONDENCE INFORMATION
Submitted in final revised form September 27, 2022.Address correspondence to: Mitchell Levine, DMD; Email: mlevine@aadsm.org
DISCLOSURE STATEMENT
Dr. Schwartz declares investments in Prosomnus Sleep.*Download PDF for full article features.