Special Article 1, Issue 1.3
Rapid Maxillary Expansion for Pediatric Sleep Disordered Breathing
http://dx.doi.org/10.15331/jdsm.4134
Rose D. Sheats, DMD, MPH
Adjunct Associate Professor, Oral Facial Pain Group, Dental Sleep Medicine Unit, University of North Carolina School of Dentistry, Chapel Hill, NC
Rapid maxillary expansion (RME), also known as rapid palatal expansion, is gaining interest in the medical and dental community as a potential therapeutic modality to treat sleep disordered breathing in pediatric patients. RME is an orthodontic procedure indicated for children who demonstrate a transverse deficiency in the width of their maxilla, usually manifested by the presence of a posterior crossbite.
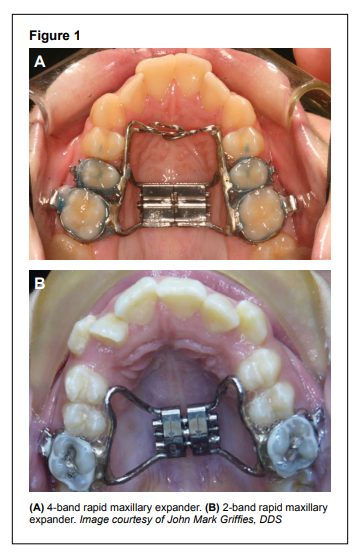
Increase in the width of the maxilla is accomplished by placement of an expansion screw in the palate that is secured to the dentition. Generally RME appliances are deferred until the maxillary permanent first molars have erupted. Two-band expanders are secured to permanent first molars; 4-band expanders also incorporate either second primary molars or first or second premolars (Figure 1). The goal is to increase maxillary width by skeletal expansion (orthopedic) and not by dental expansion (orthodontic), but in reality both skeletal and dental expansion occur.
Figure 1 |
{kind=link}
Activation of the expansion screw separates the two halves of the maxilla at the midline suture but also impacts the other circumaxillary sutures. The zygomaticomaxillary, zygomaticotemporal, zygomaticofrontal, nasomaxillary, and nasofrontal sutures are also impacted by this procedure.1,2 Occasionally patients report feeling pressure at the nasofrontal suture or other circumaxillary sutures when the expander is activated.
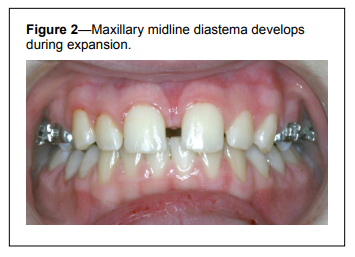
Sufficient expansion occurs in days to a few weeks, and a telltale sign of skeletal expansion is the appearance of a transient maxillary midline diastema (Figure 2). Typical expansion rates vary from 0.25 mm to 0.5 mm per day until the desired expansion is achieved. The maxilla is intentionally over-expanded to accommodate anticipated dental and skeletal relapse.3
Figure 2Maxillary midline diastema develops during expansion. |
{kind=link}
Bone remineralization of the expanded suture requires 3-6 months, during which the expander must remain in place.4 To manage relapse when the expander is removed,3,5 another form of retention is indicated as discussed below.
As early as 1965, Haas described the ability of RME to increase nasal cavity volume and to improve nasal respiration,6 and other studies followed that investigated the association between RME and nasal airway resistance with variable results.7-10 These reports preceded the widespread medical recognition of sleep disordered breathing (SDB), and thus the technique was not advanced at the time as a treatment option for SDB.
In 2004 Pirelli and coworkers described a case series of 31 children diagnosed with obstructive sleep apnea syndrome (OSAS) whose AHI normalized after RME and remained stable at 4 months.11 Villa evaluated 14 OSAS children who underwent RME and demonstrated significant improvement in sleep parameters and symptoms of SDB at 12 months and again in 36 months in a follow-up study of 10 of the original 14 children.12,13 Limitations of these studies included the small sample size and absence of a control group, but they nevertheless demonstrated the potential value of the procedure in the management of pediatric SDB.
To date, no randomized clinical trials have been conducted to assess more rigorously the effect of RME on pediatric sleep disordered breathing. Studies are lacking to identify the optimal age for RME and to determine the stability of improvement in respiratory parameters, the effect on behavioral and cognitive outcomes, and the long-term impact on health outcomes.
Patient Selection
The following criteria must be considered in determining the most appropriate patients for RME:
- Maxillomandibular transverse relationships
- Mid-palatal suture patency
- Anatomy of dental crowns that will retain the fixed device
- Ability of patient to tolerate dental procedures and impressions as well as a bulky intra-oral appliance fixed to the maxillary dentition
Maxillomandibular Transverse Relationships
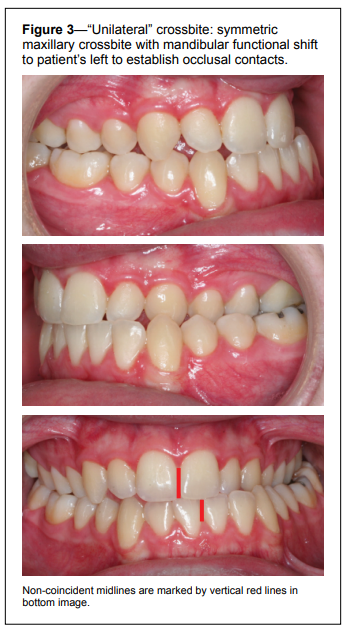
Orthodontic expansion of the maxilla is undertaken in the presence of maxillary constriction. This is generally revealed by either a unilateral or bilateral posterior crossbite. Often unilateral crossbites represent a symmetric bilateral maxillary constriction in which the patient compensates by shifting the mandible to one side or the other to establish occlusal contacts (“functional shift”) (Figure 3). This can be readily seen by the presence of non-coincident midlines but must be confirmed by ascertaining the mandibular shift to distinguish from a true unilateral maxillary constriction.Figure 3“Unilateral” crossbite: symmetric maxillary crossbite with mandibular functional shift to patient’s left to establish occlusal contacts. |
{kind=link}
In some instances the mandibular dentition masks a maxillary constriction by lingual tipping of the mandibular posterior teeth to compensate. The classic crossbite will not be present, and a decision must be made regarding the feasibility of correcting the mandibular constriction as well. Efforts to expand the mandible are limited to what can be accomplished by dental expansion as skeletal expansion of the mandible is more challenging and has met with more limited success.
Mid-Palatal Suture Patency
Palatal expansion is most effectively accomplished in patients whose mid-palatal suture is still patent. This suture fuses, or is resistant to expansion, around puberty14; thus prepubertal and adolescent patients are most desirable. Adults can also be expanded by RME; however, the procedure requires surgical release of not only the palatal suture but also the maxillary circumferential sutures and the pterygoid plates, a technique known as surgically assisted rapid palatal expansion.15 It approximates a Le Fort I osteotomy procedure without the down-fracture of the maxilla and is therefore not a trivial procedure for an adult.Crown Anatomy
Crown anatomy is critical to minimize dislodging of the appliance during treatment. The decreased crown height and conical shape of the primary dentition do not favor adequate band adaptation and retention. Furthermore, exfoliation of deciduous teeth during the expansion or the retention phases could jeopardize the procedure.If crown anatomy is not conducive to retaining bands, an alternative design of the expander includes acrylic occlusal coverage of the dentition.5 The expander is cemented onto the occlusal and/or buccal surfaces of the teeth which necessitates practitioner vigilance to monitor for cement leaks that may lead to demineralization and caries formation under the appliance. Such appliances, if secured to deciduous teeth, may also impede exfoliation of the primary dentition and delay emergence of the permanent successor. This concern is generally of minor consequence, however, as the permanent tooth will erupt shortly after the appliance is removed. Patients and parents must be alerted to the possibility that deciduous teeth may dislodge upon removal of such an expander.
Tolerance of Technical Procedures and Intra-Oral Appliance
The age at which a young patient may be considered suitable for a rapid maxillary expansion appliance is also dictated by his or her ability to tolerate sizing and seating of bands, dental impressions, cementation of the lab-fabricated expansion appliance, and daily activation of the expansion screw. Treatment of an apprehensive or uneasy patient may need to be deferred until further maturity enables cooperation with the procedures.The patient must also be able to accept the presence of a fixed bulky palatal appliance that interferes with eating and requires enhanced oral hygiene measures for many months.
Appliance Management
Responsibility for appliance effectiveness includes not only the provider but also the patient and the parent or caregiver to manage the following:- Intra-oral activation of the expansion screw
- Appliance dislodgment
- Retention of the correction after the active phase of expansion
- Other complications
Activation of the Expansion Screw
After the appliance is fixed to the dentition, the parent or caregiver will need to activate the expansion screw by turning it once or twice a day according to the practitioner’s recommendations. This necessitates cooperation and patience from the patient as the parent must identify intra-orally the hole of the expansion screw in which to insert the key in order to turn the screw.Appliance Dislodgment
Dietary restrictions are advised to minimize dislodgment of the appliance from the dentition. “Oooey, gooey, sticky, chewy” foods should be avoided as should ice, popcorn, and other hard foods. Unfavorable crown anatomy may preclude adequate fitting of bands which may loosen even in the most compliant patient. Occasionally bands fracture, and a new appliance will need to be fabricated.Usually the expander dislodges only partially, but it must be completely removed in order to repair and properly re-seat. If unable to be re-seated at the same appointment, loss of expansion will occur, and when the appliance is re-cemented at a subsequent appointment, it requires reversing the screw advancement to match appliance width to the maxillary width.
Retention Protocol
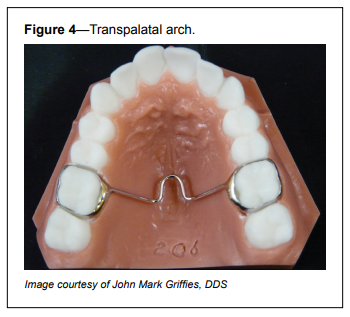
As noted earlier, even after the suture has remineralized, dental and skeletal relapse in the expansion occurs. To avoid complete loss of the correction, retention is a critical aspect of the procedure.The retention protocol should be discussed with the patient and parent. Protocols may include keeping the expander in place until comprehensive orthodontics is undertaken. If the expander is removed after 3-6 months, it may be replaced with another fixed but less bulky appliance called a transpalatal arch (Figure 4).
Figure 4Transpalatal arch. |
{kind=link}
Removable retainers such as a Hawley retainer rely on excellent compliance from the patient and may be contraindicated in the mixed dentition as the retainer depends on close adaptation to dental units to maintain corrections. A thin clear plastic horseshoe retainer that covers only the dentition will likely have insufficient strength to prevent skeletal relapse.
Retention poses particular challenges in patients in the early or mixed dentition. Not only must retention be maintained for years, but also as teeth exfoliate, critical dental units that secure the skeletal expansion are lost. Careful follow-up is required to ensure that the retainer does not impede eruption of permanent teeth and to adapt or replace the retainer during the tooth exchange period.
Other Complications
Because expansion forces are applied to the teeth at a distance coronal to their center of rotation, teeth will tip buccally in addition to their lateral displacement as the palatal bones separate at the mid-palatal suture. The absence of suture release during expansion (e.g., due to suture maturation) will lead to excessive buccal crown tipping of the teeth attached to the expander and little to no skeletal expansion. This not only creates an unstable occlusion but is also prone to near complete relapse of the accomplished expansion.The force required to move a tooth is very light and in the range of 1-4 oz. Even with such light forces, orthodontic treatment has been associated with root resorption.16 Forces of the magnitude applied with expansion appliances have been reported to range from 3 to 10 lbs,17 but little is known about the risk or extent of root resorption secondary to these force levels. Nevertheless RME has been successfully used for decades in orthodontic treatment with no apparent untoward clinical sequelae of this nature, but use of this procedure in much younger patients bears careful monitoring to ensure that unfavorable side effects do not occur
Little research has been conducted into examining risk of root fenestrations or dehiscences as the roots of teeth are displaced buccally toward the cortical plate, however it has been raised as a potential concern.18 In younger patients, the bone is less mature and mineralized (“softer”), leading to speculation that it might be a greater risk to undertake expansion in such patients. On the other hand, one may argue that less force is required to separate the midline palatal suture and/ or that the alveolar bone of younger patients is better able to adapt to expansion and may tolerate such forces better than mature alveolar bone. The studies are lacking.
Finally, non-compliance with or poor design of the retention protocol will result in loss of the expansion. While this will certainly have implications for subsequent orthodontic treatment, it may have variable implications on the management of pediatric sleep disordered breathing. If the expansion is accomplished and maintained at a critical point in airway or craniofacial skeletal growth and development, it is possible that the airway benefit will have been attained and relapse of the crossbite may be inconsequential other than from an orthodontic perspective. Clearly more research is needed to guide decisions about timing of early intervention.
Further Research
While RME is a promising tool to manage SDB in pediatric patients, further investigation is required to elucidate:- The optimal age for initiating RME treatment
- The feasibility of offering this treatment in patients prior to the eruption of permanent posterior teeth
- The design and duration of effective retention protocols
- The benefits/risks in patients without significant maxillary constriction
- The long-term cognitive, behavioral, and health outcomes of early intervention with RME
CITATION
Sheats RD. Rapid maxillary expansion for pediatric sleep disordered breathing. Journal of Dental Sleep Medicine 2014;1(3):131–134.REFERENCES
2. Leonard R, Sicurezza E, Cutrera A, Barbato E. Early post-treatment changes of circumaxillary sutures in young patients treated with rapid maxillary expansion. Angle Orthod 2011;81:36-41.
3. Bishara SE, Staley RN. Maxillary expansion: clinical implications. Am J Orthod Dentofacial Orthop 1987;91:3-14.
4. Ekstrom C, Henrikson CO, Jensen R. Mineralization in the midpalatal suture after orthodontic expansion. Am J Orthod 1977;71:449-55.
5. Geran RG, McNamara JA, Baccetti T, Franchi L, Shapiro LM. A prospective long-term study on the effects of rapid maxillary expansion in the early mixed dentition. Am J Orthod Dentofacial Orthop 2006:129:631-40.
6. Haas AJ. The treatment of maxillary deficiency by opening the midpalatal suture. Angle Orthod 1965;35:200-17.
7. Wertz RA. Changes in nasal airflow incident to rapid maxillary expansion. Angle Orthod 1968;38:1-11.
8. Hershey HG, Stewart BL, Warren DW. Changes in nasal airway resistance associated with rapid maxillary expansion. Am J Orthod 1976;69:274-84.
9. Timms DJ. The reduction of nasal airway resistance by rapid maxillary expansion and its effect on respiratory disease. J Laryngol Otol 1984;98:357-62.
10.. Warren DW, Hershey G , Turvey T, Hinton VA, Hairfield WM. The nasal airway following maxillary expansion. Am J Orthod Dentofacial Orthop 1987;91:111-6.
11. Pirelli P, Saponara M, Guilleminault C. Rapid maxillary expansion in children with obstructive sleep apnea syndrome. Sleep 2004;27:761-6.
12. Villa MP, Malagola C, Pagani J, et al. Rapid maxillary expansion in children with obstructive apnea sleep syndrome: 12 -month follow-up. Sleep Med 2007;8:128-34.
13. Villa M P, Rizzoli A, Miano S, Malagola C. Efficacy of rapid maxillary expansion in children with obstructive sleep apnea syndrome: 36 months of follow-up. Sleep Breath 2011;15:179-84.
14. Persson M, Thilander B. Palatal suture closure in man from 15 to 35 years of age. Am J Orthod 1977;72:42-52.
15. Kraut RA. Surgically assisted rapid maxillary expansion by opening the midpalatal suture. J Oral Maxillofac Surg 1984;42:651-5.
16. Roberts-Harry D, Sandy J. Orthodontics. Part 11: Orthodontic tooth movement. Br Dent J 2004:196:391-4.
17. Isaacson RJ, Ingram AH. Forces produced by rapid maxillary expansion 2: Forces present during treatment. Angle Orthod 1964;34:261-9.
18. Davidovitch M, Efstathiou S, Sarne O, Vardimon A. Skeletal and dental response to rapid maxillary expansion with 2- versus 4-band appliances. J Am Orthod Dentofacial Orthop 2005;127:483-92.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication September, 2014
Accepted for publication September, 2014
Address correspondence to: Rose D. Sheats, University of North Carolina, School of Dentistry, CB 7450, Chapel Hill, NC 27599; E-mail: Rose_ Sheats@unc.edu
DISCLOSURE STATEMENT
This was not an industry supported study. The authors have indicated no financial conflicts of interest.
PDF