Special Article 1, Issue 11.4
Digital Transformation in Dental Sleep Medicine and the Age of Intelligent Oral Appliances
http://dx.doi.org/10.15331/jdsm.7360Subha Giri, BDS, MS1, Timothy Morgenthaler, MD2
1 Department of Dental Specialties, Mayo Clinic, Rochester, MN; 2 Center for Sleep Medicine, Division of Pulmonary and Critical Care Medicine, Mayo Clinic, Rochester, MN
The COVID-19 pandemic has had myriad effects on healthcare professionals. As frontline workers, healthcare professionals experienced the direct effects of the disease. Concurrently, their ability to cater to critical patient care needs was affected by the convergence of digital technologies (telemedicine, remote monitoring, portable technologies. etc). Dentists were no exception to this collective experience.
Since the turn of the century, telemedicine has steadily gained significance for its ability to expand access to care, improve care quality, support continuity of care, and reduce overall healthcare costs.1 The Total Dental Access project convened by the US Department of Defense pioneered the application of telehealth to expand access to oral health care.2 The advent of digital patient records (electronic dental/medical records software) further facilitated storing, communicating, and transferring patient-sensitive information between patients and their collaborating healthcare professionals.3 The subsequent evolution in digital radiography and digital photogrammetry (intraoral scanning) paved the way toward a more complete digital patient record on the diagnostic side, whereas on the therapeutic side CAD/CAM and three-dimensional printing technology have rapidly evolved to deliver precise oral and maxillofacial prosthesis and orthodontic aligners.4-6
Despite steady growth in available dental digital technologies, their day-to-day utilization has been affected by limited clinical integration. As the COVID-19 pandemic-triggered lockdowns unfolded in the year 2020, many dental clinical teams recognized a critical need to expand access to oral health care while increasing their vigilance for safety around dental procedures routinely associated with aerosolized droplets of saliva. Equipped with computer systems that could maintain a comprehensive digital patient portfolio, dental clinical teams began leveraging new platforms such as Zoom, Doximity, etc. that expanded latent telehealth resources and made them available to practitioners nationwide. Such convergence proved to be an effective approach in certain areas of dentistry.
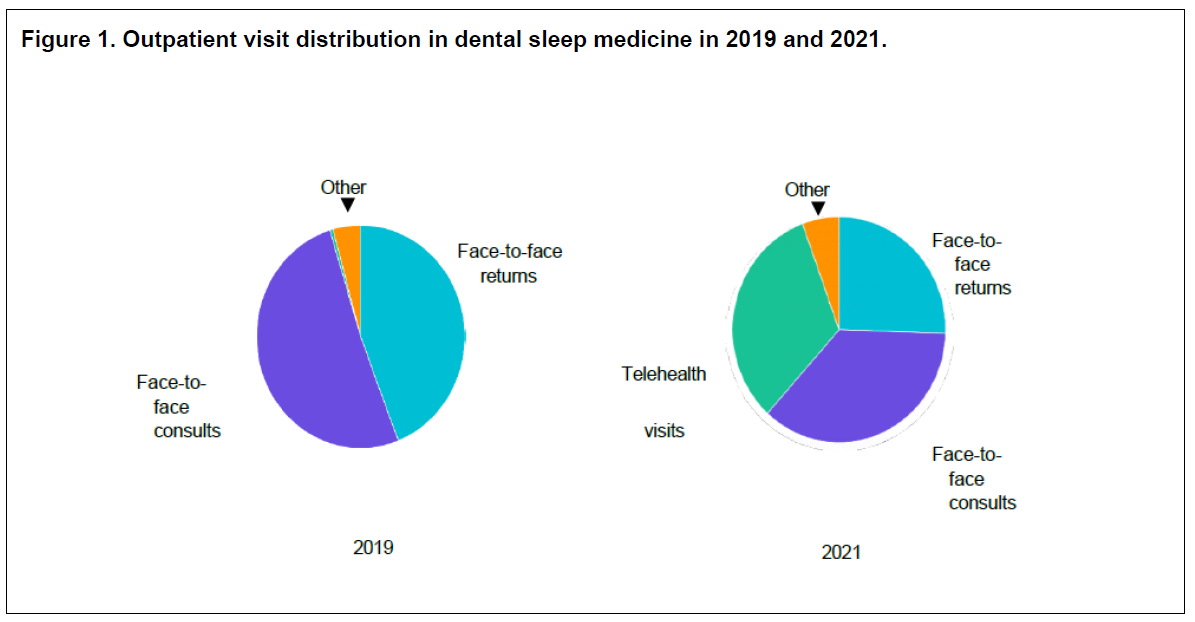
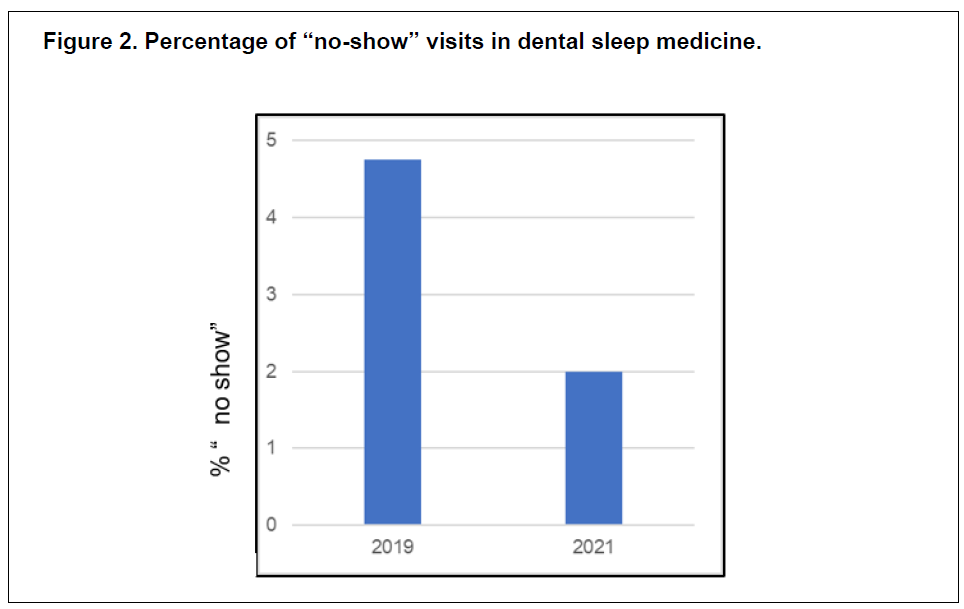
Dental sleep medicine practices served as one such environment for this new format of digitally integrated workflow. At Mayo Clinic’s dental sleep medicine practice, approximately one-third of the visits converted to telehealth (Figure 1). Simultaneously, the Mayo Clinic Center for Sleep Medicine pivoted to increased utilization of disposable home sleep apnea testing (HSAT) that could be delivered, administered, and the data received all without the patient physically connecting with the sleep center.7-9 Within a few months of the state of Minnesota’s Emergency Executive Order 20-20 that ordered residents who were not essential workers to stay at home, dropping total visit volumes by approximately 30%, the Center for Sleep Medicine had returned to visit volumes greater than those prior to the pandemic, but now with telehealth visits comprising more than 30% of total visits. The Center for Sleep Medicine and the dental sleep medicine practices share an integrated electronic health record and are fully integrated with regard to referrals, communication, and sharing of imaging and test results. With the implementation of the integrated digital workflow there was an increase in patients returning to the collaborating sleep physician for sleep testing considerations after oral appliance therapy, along with a significant reduction in patient “no-show” visits (Figure 2).
Figure 1Outpatient visit distribution in dental sleep medicine in 2019 and 2021. |
{kind=link}
Figure 2Percentage of “no-show” visits in dental sleep medicine. |
{kind=link}
Figure 3Linear workflow versus a fully integrated digital workflow in dental sleep medicine. |
{kind=link}
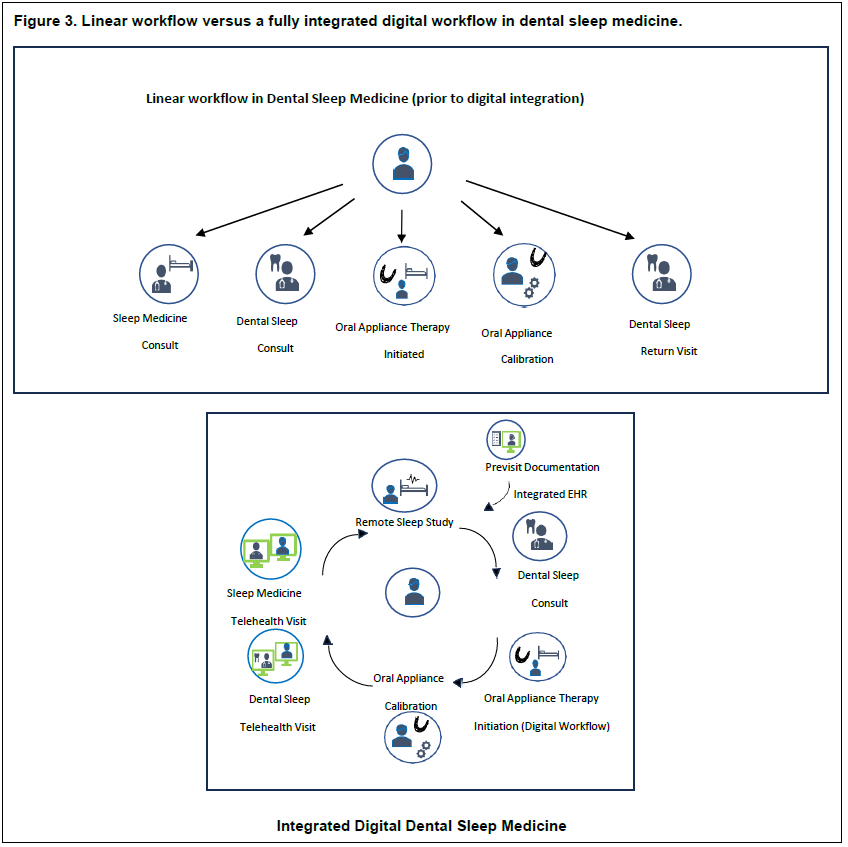
Oral appliance therapy is a well-evidenced treatment alternative for obstructive sleep apnea provided by qualified dentists in the field of dental sleep medicine, in collaboration with the patient’s sleep physician. As the pandemic affected dental practices, the American Academy of Dental Sleep Medicine acknowledged the role telehealth could play in delivering oral appliance therapy and provided web resources for member dentists outlining the technologic infrastructure and the method to integrate telehealth in their respective practices.10 Enhanced digital capabilities of oral appliance therapy platforms provided by appliance manufacturers and licensed dental laboratories complemented this at the therapeutic aspect, thus favoring a convergence of these technologies for this niche environment.11 In addition, remote sleep monitoring tools such as HSATs gained significance because in-laboratory polysomnograms were restricted during the pandemic.7 The expansion in access to care, safety, and efficiencies of telehealth could now be combined with the precision of digitally generated therapeutic (milled or printed) oral appliances, which can be tested for optimal efficacy using HSATs and interacting with the sleep medicine specialist, all via digital means. Thus, for the first time, an end-to-end digitally integrated workflow is feasible between collaborating dentists and physicians in caring for their patients with obstructive sleep apnea (Figure 3).
Although many aspects of dentistry may not be amenable to this digital convergence, future trends favor a complete digital transformation in dental sleep medicine. Current advances in microelectronic and nanoelectronic biosensor systems and artificial intelligence (AI) shall contribute to a future generation of oral appliances that seamlessly assist physicians and dentists in defining collaborative treatment plans for their patients.
Already, oral appliance compliance monitoring is currently feasible, with embedded sensor technology that has proved to be reliable in confirming patients’ adherence to therapy.12 The next generation of oral appliances would facilitate additional physiologic monitoring and reporting, which would be made available to patients, their physician, and the dentist collaborators at once. AI algorithms are most likely to facilitate a prediction of oral appliance candidacy using phenotyping and disease modeling, as well as guide individualized therapy with smart oral appliances, closing the loop in therapy calibration and outcomes monitoring.
These changes require action now to re-think and re-skill our practices. Various changes likely have specific technical and talent implications for our practices:
- Increased Telehealth Integration: Telehealth will become more prevalent in dentistry, allowing for remote consultations, follow-ups, and initial assessments. This has implications for office size, layout, health record and appointment software, desk staff skills, information technology acquisition, and a need for policies to guide desired at-home versus office work.
- Digital Imaging Advancements: Digital imaging technologies will continue to improve, offering more accurate and comprehensive diagnostic tools, such as high-resolution three-dimemsional imaging and intraoral scanners. Equipment half-life will vary depending on upgrade capacity and physical construction. Cloud-based systems will require enhanced security.
- AI-assisted Diagnosis: AI will play a significant role in dental diagnosis, aiding in the interpretation of digital images and patient records. This can enhance the speed and accuracy of diagnoses. It may also expand the capabilities of oral disease diagnosis and require new or strengthened collaborations with other healthcare professionals, such as oncologists.
- Personalized Treatment Plans: Dentists will be able to create more personalized treatment plans based on AI-assisted assessments, leading to more effective and efficient care. Use of AI to advise regarding therapies will require a firm educational and ethical framework that a practice is comfortable with and that keeps accountability for decision making at the appropriate level.
- Streamlined Workflow: Automation and AI-driven administrative tasks will streamline dental practices, reducing paperwork and improving overall efficiency. Required skill sets for coworkers will change, mandating a strategy for upskilling long-term practice members and acquiring the new talent needed.
- Continuing Education: The dental workforce should prioritize ongoing education to stay updated on emerging technologies and practices in digital dentistry and AI applications.
- Patient Education: Dentists should focus on educating patients about the benefits and limitations of telehealth and AI in dentistry to ensure informed decision-making. AI will be affecting their lives in many ways, and they will need confidence in this new form of integrated digital machine- augmented care.
- Regulatory Changes: Anticipate potential changes in regulations and insurance coverage related to telehealth and AI in dentistry, which may vary by region. The dental profession will want to not only keep informed but contribute to and shape regulatory work in this area so that they as a stakeholder and profession can be most comfortable with changes as they occur.
REFERENCES
- Majerowicz C, Tracey S. Telemedicine: Bridging Gaps in Healthcare Delivery. J AHIMA. 2010; 81(5):52-53.
- Rocca MA, Kudryk VL, Pajak JC, Morris T. The evolution of a teledentistry system within the Department of Defense. Proc AMIA Symp.1999:921-924.
- Delrose DC, Steinberg RW. Clinical significance of the digital patient record. J Amer Den Assoc. 2000;131 Suppl:57S-60S.
- Chadwick RG. Close range photogrammetry- a clinical dental research tool. J Dent. 1992;20(4):235-239.
- Rekow ED. CAD/CAM in dentistry: A historical perspective and view of the future. J Can Dent Assoc.1992;58(4):283, 287-88.
- Ashtiani RE, Khanlar LN, Mahshid M, Moshaverinia A. Comparison of dimensional accuracy of conventionally and digitally manufactured intracoronal restorations. J Prosthet Dent. 2018;119(2):233-238.
- Yoon D-W, Shin H-W. Sleep tests in the non-contact era of the COVID-19 pandemic: home sleep tests versus in-laboratory polysomnography. Clin Exp Otorhinolaryngol.2020;13(4):318-319.
- Alsaif SS, , Kelly JL, Little S, et al. Virtual consultations for patients with obstructive sleep apnoea: a systematic review and meta-analysis. Eur Respir Rev. 2022;31(166):220180.
- Kosky C, Madeira N, Boulton K, et al. Telemedicine compared to standard face-to-face care for continuous positive airway pressure treatment: Real-world Australian experience. Sleep. 2022;45(10):zsac157.
- Masse, JF. Teledentistry, DSM and the COVID-19 pandemic: The beginning of a new era? J Dent Sleep Med. 2020;7(3).
- Charkhandeh S, Kuhn D, Kim S. A fully digital workflow and device manufacturing for Mandibular Repositioning Devices for the treatment of Obstructive Sleep apnea: a feasibility study. J Dent Sleep Med. 2017;4(4):97-102.
- Dieltjens M, Braem MJ, Vroegop AVMT, et al. Objectively measured vs self-reported compliance during oral appliance therapy for sleep-disordered breathing. Chest. 2013;144(5):1495-1502.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication November 27, 2023Submitted in final revised form January 16, 2024
Accepted for publication May 19, 2024
Address correspondence to: Subha Giri BDS MS, Department of Dental Specialties, Mayo Clinic
200 First Street SW, Rochester, MN 55905;
Email: giri.subha@mayo.edu