Special Article 1, Issue 11.2
Novel Therapies for Preventing, Managing and Treating Obstructive Sleep Apnea and Snoring in Pediatric and Adult Patients
http://dx.doi.org/10.15331/jdsm.7332Rose Sheats, DMD, MPH1 (Co-Chair); Jean-Francois Masse, DMD, MSc, FACD2 (Co-Chair); Mitchell Levine, DMD, MS3; Ghizlane Aarab, DDS, PhD4; Miguel Meira e Cruz, DDS, MS5; Michael Simmons, DMD, MScMed, MPH, MSc, FAASM, FAAOP6-7; Jacy Stauffer, DMD, FAAPD8; Steve Carstensen, DDS9; Harmeet Chiang, DDS, MS10; Maria Therese Galang-Boquiren, DMD, MS11; Kevin Postol, DDS12
1Adams School of Dentistry, University of North Carolina, Chapel Hill, North Carolina (Retired); 2Laval University; 3Saint Louis University; 4Academic Centre for Dentistry Amsterdam (The Netherlands) Department of Orofacial Pain and Dysfunction; 5Sleep Unit, Cardiovascular Center of Lisbon University, Lisbon School of Medicine; 6UCLA School of Dentistry (1987-2018); 7Encino Center for Sleep and TMJ Disorders; 8Oregon Health and Science University; 9Sleep Solutions NW; 10Virginia Commonwealth University; 11University of Illinois-Chicago; 12Gateway Sleep and TMJ
INTRODUCTION
As the scope of practice for dental sleep medicine has evolved, medical and dental providers are increasingly interested in emerging dentistry-based interventions to address adult and pediatric obstructive sleep apnea (OSA) and snoring. The literature on newer therapies is hardly robust and has not withstood the test of time. Accordingly, providers remain uncertain as to how recent advancements in the field could be applied to their clinical practice. In recognition of this gap, the American Academy of Dental Sleep Medicine (AADSM) undertook a consensus conference of subject matter experts to review the published literature on several emerging therapies for OSA and snoring in both adults and children with the goal of providing guidance.
This consensus conference used a modified RAND/UCLA model (RAM), which is commonly used to develop clinical guidance for improved health care. RAM uses a quantitative approach for synthesizing qualitative data, aiming to achieve general agreement, convergence of opinion, or resolving inconsistencies in scientific information around a particular topic. During the RAM process, an expert panel rates the appropriateness of interventions using a 9-point Likert scale and then categorizes them based on the group median rating.1 For this consensus conference, the panel included experts from 4 different countries, all with extensive knowledge of dental sleep medicine. Additionally, key stakeholders in the fields of dentistry and sleep medicine were invited to observe and contribute to robust discussion prior to voting by the expert panel.
During this conference, the panel and observers focused exclusively on the use of novel therapies to manage diagnosed OSA and snoring. For the purposes of this conference, the panel relied on research that assessed sleep test data for OSA.2,3
Snoring is identified as respiratory sounds generated in the upper airway during sleep. In this paper, we refer to snoring as not the noise itself, but rather the diagnosis of snoring without OSA.2
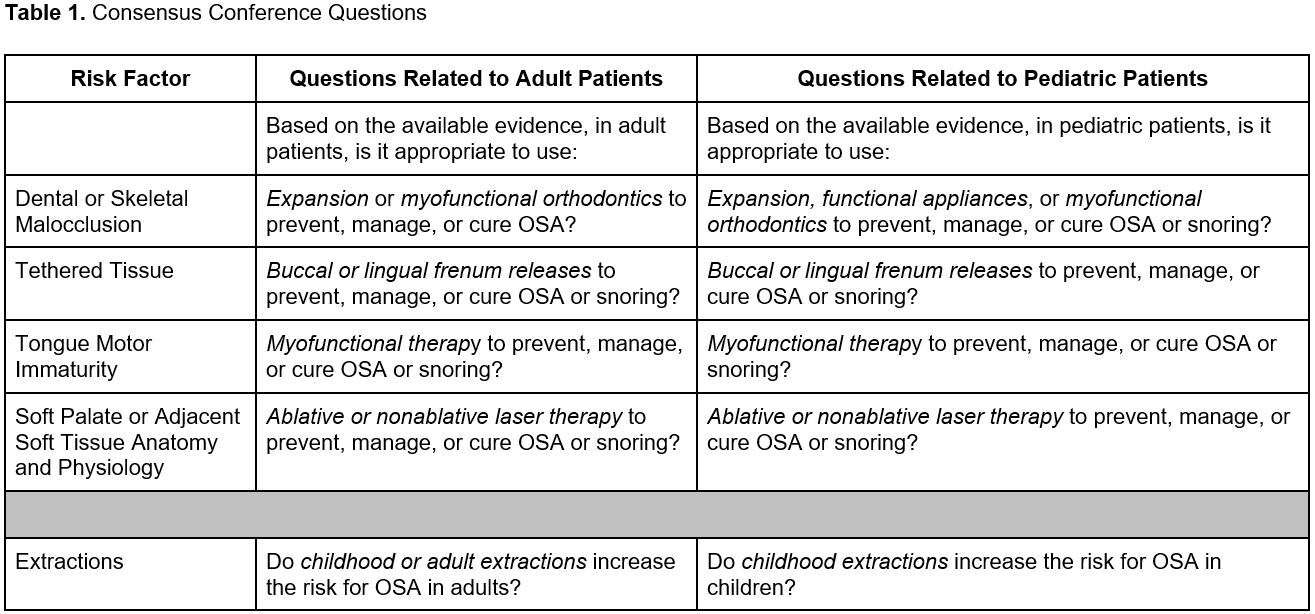
The conference participants explored specific therapies to prevent, manage, or cure adult and pediatric OSA and snoring. Treatment and management were used interchangeably. The therapies reviewed included 4 potential risk factors associated with OSA and snoring including malocclusion, intraoral tethered tissue, tongue motor activity patterns and soft palate/adjacent soft tissue anatomy and physiology. Specific questions were asked about the following novel or emerging therapies associated with each respective risk factor listed above (with therapies italicized in questions below). The emerging therapies for OSA and snoring were selected based on frequency of inquiries from AADSM members about these therapies.
When addressing these questions, the following definitions were used:
- Prevent - After the intervention/therapy, OSA or snoring will not develop during the time period of the age cohort. When discussing prevention in children, the therapy prevents OSA or snoring only during childhood and not into adulthood.
- Manage - The therapy will normalize OSA or snoring as much as possible during the time period of the cohort period.
- Cure - The therapy will resolve OSA or snoring without further need for therapy during the time period of the cohort. When discussing curing in children, the therapy cures OSA or snoring only during childhood and not into adulthood.
- Adults- Ages 18 years and older.
Table 1
Consensus Conference Questions
(more ...)
Because of overlap in terminology with the therapies listed above, it is helpful to distinguish between functional appliances, myofunctional therapy, and myofunctional orthodontics. Functional appliances refer to fixed or removable appliances. They are generally customized and advance the mandible in growing children, similar to oral appliance therapy in adults, except the goal may be to develop a permanent advanced mandibular position. Myofunctional therapy encompasses the field of strengthening the tongue and orofacial musculature to improve speech and swallowing and to correct improper oral function. Myofunctional orthodontics combines myofunctional therapy with removable appliances that are often prefabricated as opposed to customized.
{kind=link}
The conference participants considered each of these emerging therapies as monotherapies to determine whether they were appropriate to use in the majority of patient cases. The recommendations in this paper are therefore not intended to replace a clinician’s best judgment when determining the appropriate therapy for their individual patient. Emerging therapies may need to be considered in combination with other more proven therapies or when other more proven therapies have failed. Qualified dentists are strongly encouraged to use their clinical expertise, knowledge of the patient’s unique circumstances and the patient’s values and preferences to determine the best course of action4 and obtain informed consent from the patient, regardless of the therapy provided.
RESULTS
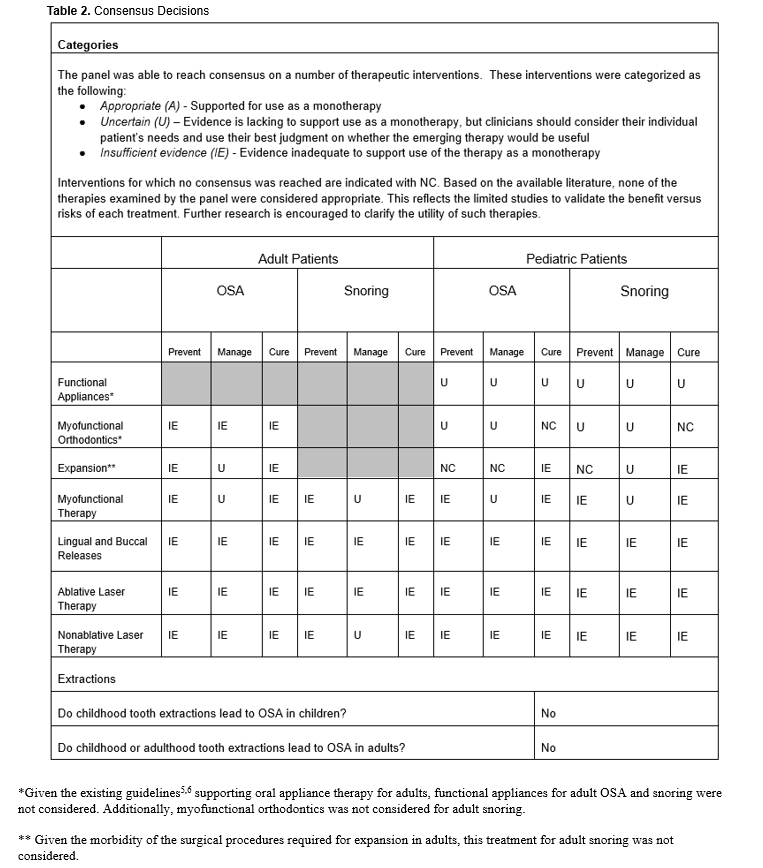
The following table details the decisions made by the panel at the consensus conference.
Table 2
Consensus Decisions
(more ...)
{kind=link}
DISCUSSION
The prevalence of OSA in children ranges from 1% to 5% and tends to peak between the ages of 2 to 8 years.7–11 Pediatric OSA has been associated with a number of craniofacial features including maxillary constriction, mandibular retrusion, short mandibular length, high mandibular plane angle, and class II skeletal and dental malocclusion.12–17 The quality of evidence from these reports, however, was low to very low due to the types of studies conducted, and caution must be exercised in assuming that treatment to alter unfav orable craniofacial features will prevent, manage, or cure OSA in children.
Adenotonsillectomy (AT) is considered the first-line therapy for pediatric OSA typically under age 7. In a randomized clinical trial of pediatric OSA patients (5-9-year-olds), 79% of children with mild to moderate OSA experienced normalization of polysomnography (PSG) findings following standalone adenotonsillectomy.18 It is noteworthy, however, that in the control group of untreated patients, watchful waiting resulted in spontaneous normalization of PSG findings in 46% of the children with mild to moderate OSA, suggesting that nearly half of children with mild to moderate OSA will naturally improve without intervention. Cases of residual OSA were associated with obesity, higher pretreatment apnea-hypopnea index (AHI), and Black race.18
In cases of mild to moderate persistent OSA, alternative treatment options include using intranasal steroids, leukotriene receptor antagonists, and continuous positive airway pressure, as well as observation in asymptomatic children with mild OSA.19–22
While up to 28% of healthy children snore, habitual snoring is prevalent in 3% to 12% of the pediatric population.23 Snoring is not associated with apnea, oxygen desaturation, or hypoventilation and is a common finding in children.24 Snoring has been found to be associated with daytime cognitive and subsequent behavioral problems that are indistinguishable to those children with compromised nighttime breathing despite the missing features of hypoxia and periodic arousals.25 However, asymptomatic snoring in children is typically not considered to require medical intervention and may be transitional during growth and development or a short-term issue not requiring intervention.
Functional Appliances for Malocclusion
Functional appliances are customized devices that advance the mandible in children and have been historically used in orthodontics to address mandibular retrognathia. Functional appliances are predicated on stimulating growth primarily at the mandibular condyle, thus translating the mandible in a downwards and forward position. Functional appliances dictate function in an advanced mandibular position and have been shown to demonstrate improvement in dental and skeletal relationships in growing children.26 By comparison, natural growth and development has been recognized to also contribute to these favorable changes. As such, it is unclear what part of the correction is attributable to the functional appliance.
Pediatric OSA
Currently no studies have demonstrated that functional appliances are superior to AT in children with an AHI > 10. Most of the identified studies examining the role of functional appliances in treating childhood OSA were fraught with limitations, ranging from small sample sizes, inadequate control groups, short study duration, missing methodologic details, and absence of long-term follow-up studies to evaluate stability of changes.27–30
While a few studies enrolled children with confirmed OSA,31,32 most studies did not assess for the presence of OSA by a diagnostic PSG prior to study inclusion.33–44 Instead, these studies enrolled participants who might have OSA as demonstrated by an increased risk for sleep-disordered breathing, using methods such as questionnaires (PSQ45 or other unidentified questionnaires), parental report, symptoms, and/or craniofacial characteristics,33–42,44,46 all of which compromise the conclusions in addressing OSA. While the AHI is an imperfect measure of OSA, it is still recognized as the current standard measure in diagnosing pediatric OSA.10,47,48 A few studies relied on alternate outcomes such as changes in symptoms or quality of life, airway size, oxygen saturation, and the oxygen desaturation index (ODI).28–30,33,49,50 The majority of studies investigating airway size employed radiography to analyze changes in the posterior airway space as a primary outcome. Unfortunately, awake airway size does not reflect supine sleep airway anatomy due to an altered physiological state and head position.14,34–44,46,51,52 In addition to the lack of pre-intervention and post-intervention AHI data, another major study limitation was the lack of untreated controls to account for normal growth and development and, hence, self-correction during the study period. In essence, treating a child’s airway space would be equivalent to treating a child’s height and attributing credit for growth to an intervention that was simply coincident to the outcome of measured growth.
Since most studies did not meet the current standards for diagnosing pediatric OSA using the AHI,10,47,48 panelists were unable to judge the appropriateness of functional appliances to treat pediatric OSA. However, in certain cases of persistent OSA that fail to respond to first-line therapies, functional appliances may offer an alternative or supplemental therapy. Further research is warranted to identify appropriate responders. In the absence of identified studies and the absence of firm clinical judgment, the panel was Uncertain regarding using this treatment to prevent, manage, or cure childhood OSA.
Pediatric Snoring
While no studies explicitly investigated the role of functional appliances in preventing, managing, or curing pediatric snoring, some studies alluded to snoring without presenting data on the impact from functional appliances. One low-quality study used unidentified questionnaires to document changes in snoring patterns by parental report without showing data.42 Another study presented no data on pretreatment or post-treatment snoring in either treatment or control groups, but offered one comment in its results section stating that snoring improved in all treated patients while failing to comment on snoring changes in control patients.43 In the absence of useful data and the absence of firm clinical judgment, the panel was Uncertain regarding the use of this treatment to prevent, manage, or cure snoring in pediatric patients.
Myofunctional Orthodontics for Malocclusion
Not to be confused with functional appliances, myofunctional orthodontics relies on removable or fixed intraoral devices that use facial and masticatory muscles to modify skeletal and dental relationships. Myofunctional orthodontics attempts to guide or correct orofacial musculature forces that are believed to cause aberrant growth and/or dental malocclusions.
Pediatric OSA
Myofunctional orthodontic devices are often prefabricated, unlike functional appliances, which are customized, and claim to address pediatric airway development issues. Often treatment is initiated in children as young as 2 to 4 years old.
A single, preliminary small study by Levrini53 in 4- to 8-year-old children was identified in the literature. While AHI improved, changes in oxygen saturation were not statistically significant, and it is noted that study participants continued to snore post-treatment. Study limitations included short study duration, absence of imaging studies, and failure to include a control group to assess any possible changes due to growth.
In the absence of useful data on the efficacy of myofunctional orthodontics or firm clinical experience, the panel was Uncertain regarding the appropriateness of this treatment to prevent or manage OSA in pediatric patients. While the panel did not reach consensus regarding myofunctional orthodontic devices curing OSA, no panelist voted that the treatment was Appropriate.
It was noted by the panel, however, that this therapy may have a role in treating medically complex patients who have failed surgery, but only in collaboration with a sleep team including medical colleagues.
Pediatric Snoring
The panel did not identify any studies on the use of myofunctional orthodontics for pediatric snoring. As noted above, research participants in the Levrini53 study continued to snore despite possible reductions in AHI. Panelists determined this therapy was Uncertain to prevent or manage pediatric snoring. The panel did not have enough data to judge the efficacy of myofunctional orthodontics to cure pediatric snoring and as such, did not reach consensus on this topic. Consistent with pediatric guidelines,10 childhood snoring without OSA, in the absence of other symptoms, does not require treatment. Parents should be reassured in these situations.18,22
Adult OSA
In adults, some myofunctional orthodontic devices may be custom fit and titratable, while others may be stock devices and indirectly titrated by sequentially changing devices with greater advancement. Only one paper reviewed reported on the use of myofunctional orthodontics in adults for OSA. This was a lower-quality, single retrospective cohort study of 220 research participants.54 The cohort used either a maxillary expansion appliance or a mandibular anterior repositioning appliance combined with a maxillary expansion device. While the study reported a statistically significant reduction in OSA severity, the overall methodology and statistical approach were limiting factors. Furthermore, 16% of patients experienced an increase in AHI indicating that more research is needed to identify responders, nonresponders and those with a treatment-induced worsened clinical status. While the authors suggested these proprietary devices may harness the growth potential of the maxilla, it was not clear how they differentiated this phenomenon from other variables such as a component part of the therapy, placebo response, or attributable to night-to-night sleep test variability.54
During discussion, consensus conference participants expressed concern that bone growth may not be feasible in adult populations and that moving teeth into areas without bone can be associated with significant untoward adverse effects for the patient. When considering potential harms, alongside the lack of evidence, the panel found Insufficient Evidence to support the use of myofunctional orthodontics to prevent, manage, or cure adult OSA.
Expansion for Maxillary Constriction
Maxillary constriction is suggested to play a potential role in the pathophysiology of OSA.17 Rapid maxillary expansion (RME) is intended to lower nasal resistance, which may alter nasomaxillary flow dynamics, thus lowering the risk for pharyngeal collapse and improving OSA symptoms.55
Pediatric OSA
The panel reviewed several articles that analyzed the impact of RME on pediatric OSA.13,17,55–71 Since many of the studies identified were of low quality, the panel focused its attention on the systematic reviews, recognizing that many included weak or poor-quality studies. Study outcomes included changes in AHI, minimum O2 saturation, or posterior airway space.28,56,58,59,72–75
Study limitations included either very short or no follow-up assessments to judge the stability of changes or evaluation of parameters such as posterior airway space that do not correlate with improvement in AHI.62,76 It must also be recognized that research participants enrolled in the studies were undergoing RME to correct a maxillary transverse deficiency, and no data were found that examined RME in OSA patients without a transverse deficiency.
The panel was unable to reach consensus on using expansion as a prevention of OSA in children. The median of votes was in the Uncertain category. Of the panelists who voted outside the range of Uncertain, all deemed the treatment having insufficient evidence to support its use.
Similarly, the panel did not reach consensus on using expansion to manage OSA in children. Panelist votes spanned the 3 categories of Appropriate, Uncertain, and Insufficient Evidence. Clearly, better quality evidence and longer follow-ups are necessary before a consensus can be reached on this topic.
The panel did reach consensus that there was Insufficient Evidence to support RME as a treatment to cure pediatric OSA and stressed that expansion should only be considered in those patients who demonstrate maxillary constriction, independent of having pediatric OSA.
Pediatric Snoring
As with OSA, these studies analyzed patients who had previously been diagnosed with sleep-related breathing disorders (SRBD) or OSA. Thus, the panel was unable to arrive at a consensus about whether expansion was a viable prevention therapy for snoring. While most panelists voted in the Insufficient Evidence or Uncertain range, disagreement among the panelists included those who believed expansion is an Appropriate treatment to prevent pediatric snoring. No consensus was achieved after 3 rounds of voting, suggesting that further research on this topic should be conducted.
The panel arrived at consensus that the utility of maxillary expansion to treat pediatric snoring is Uncertain and that there is Insufficient Evidence to support maxillary expansion as a therapy to cure pediatric snoring.
Adult OSA
The expert panel agreed that it is important to differentiate how expansion in adult populations differs from expansion used in pediatric populations. While the intent of the therapy is to expand the midpalatal suture, this is more difficult to accomplish in adults because the midpalatal suture and adjacent circum-maxillary sutures are more resistant to expansion without surgical assistance or device enhancement. As a result, adults exposed to nonsurgical arch expansion are at increased risk for less stable tooth tipping, increased root resorption and cortical bone damage. Accordingly, surgical assistance or temporary anchorage devices in bone are often needed to facilitate adult maxillary arch expansion, sometimes in conjunction with corticotomy. Adult expansion includes procedures such as miniscrew-assisted rapid palatal expansion, surgically assisted RME, distraction osteogenesis for maxillary expansion and endoscopically assisted surgical expansion.
The panelists reviewed 1 published systematic review and 8 clinical cohort case series or review studies. The systematic review and meta-analysis indicated that expansion resulted in a statistically significant reduction in AHI and Epworth Sleepiness Scale (ESS) scores while changes in oxygen saturation nadir were not significant.79 Mixed outcomes were found among the remaining studies.80–87
While there is evidentiary literature to suggest that maxillary expansion in adults can result in significant reduction in AHI and improvement in subjective sleep quality, the available evidence indicated residual disease. When combined with unresolved symptoms, this may warrant further treatment. It may be possible that some patients presenting with mild OSA could experience a meaningful reduction in AHI following maxillary arch expansion, whereby no additional OSA management may be required. However, the reviewed literature did not include this population. Without longitudinal studies, it is uncertain how long any benefits of the procedure persist. Additionally, these studies cannot be generalized to all OSA patients as each of the research participants studied presented with some form of orthodontic transverse discrepancy.
Accordingly, the panel clarified that expansion of the maxilla to address OSA is only supported in the literature if a transverse discrepancy exists that requires expansion to manage the presentation. Expansion is not recommended at this time to solely address OSA or snoring in the absence of orthodontic transverse discrepancies. Thus, the panel reached consensus that there was Insufficient Evidence to support the use of expansion to prevent or cure OSA in adults. Additionally, the panel’s consensus was Uncertain regarding expansion to manage OSA.
Myofunctional Therapy for Tongue Motor Immaturity
Conceptually, myofunctional therapy (MFT) is primarily focused on improving speech and swallowing to enhance orofacial growth. It has evolved to include breathing exercises and orthopedic devices.88 The intervention uses a combination of isometric and isotonic oropharyngeal exercises,89,90 with the patient working on tasks such as speaking, breathing, blowing, sucking, and chewing through recruitment of the oropharyngeal musculature.90,91 Muscular endurance exercises aim to improve the tone, tension and mobility of oropharyngeal muscles and soft tissues, which may hypothetically reduce airway collapse during sleep.92 These exercises may also target parapharyngeal reduction of fat pads such as tongue fat.93
There is a large variation in type, intensity, time frame, and provider of intervention (speech pathologist, myofunctional therapist, or self-administered by using an app).94 There appear to be few, if any, common approaches between professionals, and therefore, it is increasingly difficult to draw solid conclusions.
Pediatric OSA
Evidence regarding the use of myofunctional therapy treating OSA is very limited. Hsu et al. (2020) published a systematic review of 9 randomized controlled trials (RCT).95 Two RCTs were performed in children with OSA (N=81).96,97 One study did not report AHI nor AI after the intervention,96 but the other demonstrated a significant decrease in AHI from baseline in the intervention group compared with controls.97 In a separate study by the same author, it was found that there was a significant improvement in ODI, mean minimum SaO2 percentage, and mean oxygen saturation.96 Rueda et al. (2020) evaluated the benefits and harms of MFT for treating OSA.94 In children, compared to nasal washing alone, myofunctional therapy and nasal washing resulted in little to no difference in AHI.
The panel found no studies reporting on the use of MFT to prevent OSA in children and, as such, concluded that there was Insufficient Evidence for its use. The panel also found that though there was a lack of evidence favoring MFT to manage OSA in children, the relative risk of therapy was low compared to potential benefits. As such, the panel reached consensus of Uncertain in providing MFT to manage OSA in children. Finally, due to lack of evidence to support that MFT can cure OSA in children, they concluded there was Insufficient Evidence to support its use as a monotherapy cure.
It is noteworthy that considerable discussion took place with feedback from the observers who emphasized that myofunctional therapy is a discipline that requires considerable education and training and that therapy is individualized to each patient. The American Speech-Language-Hearing Association (ASHA) describes the identification and treatment of orofacial myofunctional disorders and stresses that interventions be managed by appropriately trained speech and language pathologists (SLPs) in collaboration with an interdisciplinary team.98 Furthermore, the ASHA Code of Ethics stipulates that SLPs must be specifically educated and appropriately trained to provide this type of specialized care. Skepticism was expressed regarding the type and amount of training received by staff of dental offices that purport to use myofunctional therapy to treat pediatric OSA.
Pediatric Snoring
The panel did not identify any literature regarding the use of myofunctional therapy to prevent or cure snoring in children. Based on both the lack of evidence and clinical expertise, the panel found Insufficient Evidence to support MFT in this context.
As with pediatric OSA, the panel identified no literature regarding the use of myofunctional therapy to manage snoring in children. Considering the low risk of therapy, along with the lack of evidence, the panel remains Uncertain as to whether MFT should be used to manage snoring in children.
Adult OSA
Several high-quality systematic reviews (e.g. including only RCTs) on the use of myofunctional therapy in adult patients with OSA have been performed in recent years,94,95,99 resulting in mixed conclusions.
Hsu et al. (2020) evaluated the effects of respiratory muscle therapy compared with control therapy or no treatment in improving subjective sleepiness, AHI and other polysomnographic outcomes.95 Based on a meta-analyses in adult studies, MFT-based respiratory muscle therapy yielded an improvement in subjective sleepiness and snoring frequency in intervention groups compared with controls noting, however, that subjective improvements may also be attributable to placebo effects. Hsu (2020) concluded that their systematic review highlights that MFT-based respiratory muscle therapy has application as an adjunctive management for OSA suggesting that it is not sufficiently validated as a first-line OSA therapy. Study limitations included the nature and small number of participants and studies, heterogeneity of the interventions, high risk of bias and overall low quality of evidence reviewed.
Rueda et al. (2020) evaluated RCTs from the Cochrane Airways Trials Register and other web-based clinical trials registers to analyze the benefits and harms of MFT in treating OSA.94 Study outcomes included AHI, Epworth Sleepiness Scale (ESS) scores, and sleep quality assessments. They concluded that in adults with OSA, MFT compared to sham therapy reduced daytime sleepiness (ESS score), improved AHI and enhanced subjective sleep quality.
In contrast, Randerath et al. (2021) concluded that more RCTs including a larger number of patients and longer treatment periods are warranted to determine whether the benefits of MFT can be sustained over prolonged periods.99 While significant reductions in the AHI have been reported in several systematic reviews including RCTs,94,95,99 there was Insufficient Evidence to support the possibility that myofunctional therapy could result in a lasting benefit for OSA.
Review of the evidence showed that the lack of a standardized approach to MFT precludes justification of its wide use. As such, the panel determined there was Insufficient Evidence that myofunctional therapy prevents or cures OSA but it may have potential as a management therapy in some adults under some circumstances. Due to the mixed evidence, the panel found that it was Uncertain whether MFT could be recommended as effective in treating adult OSA as a primary standalone therapy.
Adult Snoring
Scant evidence was identified to explore the impact of MFT on snoring. Rueda et al. (2020) showed that it had little to no effect in reducing snoring frequency but slightly decreased subjective snoring intensity.94 The panel found that while other therapies could result in significant adverse effects or harm, the potential harm from MFT is relatively low, provided frequent reassessment and sufficient sleep testing is ongoing.
The panel agreed that MFT should be provided by a qualified clinician who has received appropriate training in providing the therapy in conjunction with medical assessment.
As with pediatric snoring, the panel found Insufficient Evidence to support use of MFT as a monotherapy to prevent and cure adult snoring. Due to its low risk, the panel was Uncertain as to whether MFT could be used to manage snoring.
Lingual and Buccal Releases for Tethered Tissue
The tongue plays an important role in the proper growth of the oral cavity and the whole stomatognathic system. Undisturbed tongue function in the neonatal period is also essential in developing proper suction during breastfeeding. The literature widely describes the influence of ankyloglossia on difficulties in breastfeeding, noting that 25% of newborns with a short lingual frenulum experience such problems.100 The surgical management of tethered oral tissues (TOTs) has increased greatly over the last 20 years.101–104
Buccal connective tissue tethering of lips or cheek may also be described as a tightness or restriction in movement of the maxillary and/or mandibular soft tissues affecting the ability to maintain lip competence during functional demands. An abnormal frenum might contribute to the establishment and progression of periodontal disease, contribute to gingival recession, and influence the fit or retention of dental prosthetics. A frenectomy involves complete removal of the frenulum, while a frenotomy involves the frenulum being modified and/or relocated.
Over the last decade, an increase in awareness has led to more frequent diagnosis and treatment. Nevertheless, there has been a 735 percent increase in the number of identified cases of ankyloglossia, and an 870 percent increase in surgical procedures of TOTs reported between 1997 to 2012.102
Our panel addressed the specific indications to surgically alter intraoral tethered tissue for OSA or snoring. Our perspective included review of published nonsurgical frenum changes occurring naturally with changes in frenum size and migration during growth and development. Therefore, desired changes in the frenum may be addressed through non-surgical interventions without surgical risk.
Pediatric OSA
In regard to OSA, the panel found 3 studies dealing with lingual releases for OSA in children.103,105,106 The evidence reviewed was from retrospective studies, not from cause and effect RCTs and, therefore, only offered plausibility. Two studies found that a short lingual frenum is a phenotypic aspect in pediatric OSA .105,106 An important consensus paper developed by a panel of experts concluded that there is no evidence that ankyloglossia causes OSA.103
Furthermore, the panel discussed that, in infants and children, these procedures can be associated with very serious adverse effects and permanent damage to tissue, including acute airway obstruction, excessive bleeding, formation of a mucus retention cyst, hematoma development, abscess formation, numbness or paresthesia, infection, scar tissue formation, and restriction in tongue movement.107 As such, the panel concluded that there was Insufficient Evidence to support use of these procedures to prevent, manage, or cure OSA in children. Combined with the potential for serious adverse effects, these procedures should not be used to treat pediatric SRBD.103
Pediatric Snoring
The panel was unable to identify any papers addressing the use of lingual or buccal releases in children with snoring. Since no studies were available to review, and clinical expertise found that the harms of lingual and buccal releases in children could outweigh any potential benefit in reducing snoring, the panel determined that there was Insufficient Evidence to support frenum releases to either prevent, manage or cure snoring in children.
Adult OSA
Since no studies were available that supported lingual or buccal tethered tissue releases as having any efficacy in addressing adult OSA, the panel reached consensus that there was Insufficient Evidence to support their use to prevent, manage, or cure OSA.
Adult Snoring
As with OSA, the panel found no clinical studies addressing either lingual or buccal releases in adults successfully addressing snoring. Additionally, the panel felt that there are unnecessary risks and potentially significant harms in surgical approaches releasing tethered intraoral tissues for OSA or snoring concerns when there is no proven biological benefit. Risks include scarring, altered sensory or motor function, pain, and infection. As such, the panel concluded that there is Insufficient Evidence to support buccal and lingual releases to prevent, manage, or cure snoring in adults.
Ablative and Nonablative Lasers for Elongated or Edematous Soft Palate and Adjacent Tissue
The ablative carbon dioxide (CO2) laser-assisted uvulopalatoplasty (LAUP) was initially considered to be effective in addressing OSA and snoring, as the removal of excess upper airway tissue prone to vibration and collapse appeared to be an obvious approach. Pharyngeal tissue reduction started with conventional surgical uvulopalatopharyngoplasty (UPPP) proposed by Fujita108 in 1981 followed by LAUP109 in 1990 and later updated with radiofrequency tissue volume reduction also termed coblation110 in 1998. Due to high complications and relatively low benefit, LAUP is not recommended by the American Academy of Sleep Medicine (AASM) as a treatment for OSA.111 With more specific endotyping and phenotyping, specific patients may be identified as responders in future and resurrect LAUP.
Nonablative laser therapy (NALT) uses laser radiation energies that do not coagulate, cut, burn, carbonize or vaporize tissues. NALT does not require anesthesia although topical anesthetic has been occasionally reported as useful to prevent a gag reflex during treatment. NALT for OSA and snoring is applied to various soft tissues in the upper airway especially the soft palate, uvula and surrounding tissues. More recently NALT has been applied to the posterior tongue and sublingual areas to address OSA and snoring. A limited number of scientific articles in the literature have indicated various application times, energies, frequency of application and anatomy irradiated, making results difficult to reproduce.
Pediatric OSA
The panel reached consensus that there was Insufficient Evidence to support use of either ablative or nonablative lasers on the soft palate as a monotherapy to prevent, manage, or cure pediatric OSA.
Pediatric Snoring
The panel reached consensus that there was Insufficient Evidence to support use of either ablative or nonablative lasers as a monotherapy to prevent, manage, or cure pediatric snoring.
Adult OSA
The panel reviewed 2 meta-analyses112,113 and several studies addressing NALT in treating adult OSA or snoring.114–124 The majority of the studies used Er:YAG 2940-nm laser stimulation. The successful outcomes reported in one of the review articles113 confounded ablative and nonablative studies as well as animal studies and, therefore, overstated the limited evidence to support NALT. The limitations to the studies included lack of control groups and control group dropout data.
The vast majority of studies of research participants undergoing NALT lacked sleep studies to confirm the presence of OSA. Parameters measuring significant improvement in AHI or the respiratory disturbance index were limited to 2 studies, one of which had significant design flaws rendering the outcomes questionable119 and the other using proprietary diode 810-nm laser settings that are not shared by the laser manufacturer.124 Other study outcomes included static soft palate length using Mallampati scores, airway volume and minimal cross-sectional area by cone-beam computed tomography in awake nonsupine study participants, ESS, snoring using subjective measures or a smartphone app, treatment satisfaction, and untoward adverse effects. While such outcomes are commonly assessed in such studies, they are not currently recognized as valid measures to judge treatment success.
There was little evidence to support general use of both ablative laser and NALT therapy for OSA. The panel concluded that there was Insufficient Evidence to support use of either ablative or nonablative laser therapy to prevent, manage, or cure adult OSA.
Adult Snoring
Minimal low-level evidence was identified in studies on the efficacy of NALT in treating snoring in adults. The studies the panel reviewed lacked objective scientific rigor and did not clarify which patients would be responders, nor clarify any standard dosing, energies or techniques that would be effective.125,126 Most of the studies used an Erbium laser, and no human studies with NALT used a CO2 laser. Notably, in the reviewed studies, approximately three-quarters of all research participants were male, so generalization to female participants may be suspect.
Unlike ablative laser therapy, NALT does not result in scarring and, as such, presents less untoward adverse effects to the patient. Most of the studies reported subjective improvement in snoring and minimal untoward adverse effects that were short-lived. While treatment had high satisfaction ratings, it was acknowledged that duration of effect was limited and that repeat treatments were necessary about annually in order to sustain snoring reduction.
There was consensus that there was Insufficient Evidence to support the use of ablative laser therapy to prevent, manage, or cure snoring. Due to its low risk and high patient satisfaction it was Uncertain whether NALT could be used to manage adult snoring. There was consensus that there is Insufficient Evidence to support NALT to prevent or cure snoring in adults.
Extractions
Pediatric OSA
There has been controversy within the dental community as to whether extractions that take place during childhood orthodontic treatment might result in decreased airway space and tongue crowding, and thus could lead to childhood OSA.127 The panel reviewed 3 articles, with evidence ranging from weak to strong.127–129 The strongest evidence derived from 7 studies with high-quality evidence described by Hu and colleagues in their systematic review.127 The authors found no evidence that supported a relationship between upper airway (UA) dimensions and functional breathing indices or that reductions in UA dimension increase airway collapsibility.127
Additional articles pertaining to pediatric OSA were identified in the systematic review by Ng and colleagues who reviewed 9 studies including both adult and adolescent research participants.130 Their conclusions on adolescents mirrored those of Hu’s systematic review, noting that the findings on airway response to premolar extractions were highly variable among the studies and did not consistently present an association between incisor retraction and airway dimensions. Ng also cautioned that these studies examined morphologic changes only and did not offer evidence of impact on functional breathing indices.
Based on the available evidence, the consensus of the panel was that extractions in children are not a risk factor for OSA. While there is evidentiary literature to suggest that extractions with significant incisor retraction might affect tongue space and UA dimensions in adults, it is also evident that extraction therapy employing moderate or mild incisor retraction may actually increase UA dimensions by mesial movement of molars.127 In general, it was noted that the incidence of extractions in the pediatric population has been significantly reduced in orthodontic practice and that the employment of maximum anchorage (i.e. maximum incisor retraction) is rarely used, except in the most severe cases of malocclusions where the extractions serve to camouflage the anterior-posterior discrepancy in lieu of surgery or the crowding is most severe.
Adult OSA
Researchers have also posited that extractions that take place during childhood or adulthood could potentially cause or contribute to OSA during adulthood. Four articles, with evidence ranging from strong to moderate were reviewed,127,130–132 including 2 systematic reviews.127,130 The systematic reviews did not support a relationship between static, awake and nonsupine posture UA dimensions and functional breathing indices during sleep.127,130 Two retrospective studies were also reviewed.131,132 The first found that research participants who had extractions did not experience a change in sleep quality or increased OSA risk as measured by questionnaire.132 The second study found no difference in OSA risk between participants who had 4 premolars extracted and those with all of their premolars retained.131
Furthermore, airway alterations relative to tooth extraction studies are based only on surrogate measures of changes in UA volume with the patient awake and in a nonsupine posture, or patient subjective questionnaire outcomes. Unfortunately, these limited static wake measures do not accurately assess functional respiration during the various sleep stages and head positions. Other limitations of these studies include research participant selection and sampling biases, as well as a lack of assessment of functional breathing parameters either awake or while asleep. As such, the panel concluded that neither childhood nor adulthood tooth extractions lead to OSA in adults.
METHODS
The AADSM Board of Directors selected a panel of 12 experts to participate in the task force by independently and anonymously voting on the therapies in question. One panelist was unable to attend the conference, leaving the final number of panelists at 11. Additionally, 7 expert observers also were invited to provide feedback during the consensus conference. These observers were key stakeholders in the areas of dentistry (e.g. pediatric dentistry, orofacial pain, prosthodontics, orthodontics), sleep medicine, pediatric otolaryngology and speech-language pathology. Seven of the panelists participated as members of a writing group that reviewed all of the literature and presented to the remaining 4 panelists and 7 observers.
The consensus conference operated under a modified RAND/UCLA methodology.1 This entailed a literature review and voting process (described below) to arrive at consensus recommendations. The panel was instructed to consider both relevant evidence presented by the writing group, as well as their own clinical expertise and judgment. While observers were permitted to offer insight and critiques of the literature, only panelists participated in the voting process.
Literature Review
A nonsystematic literature search was conducted using a combination of keywords and Medical Subject Heading Terms (MeSH) in PubMed. Two separate searches were conducted. The initial search was conducted for each of the 4 assumed risk factors by combining keywords relating to OSA and snoring, the 4 risk factors and the therapies. A subsequent search was done to refine these results by searching for disease and risk factor keywords as well as disease and therapy keywords, again for each of the 4 assumed risk factors. For the first search, results were limited to the past 10 years (January 1, 2013 to August 3, 2023). For the second search, results were limited to the past 10 years (January 1, 2013 to August 30, 2023) and only to human studies.
A total of 2059 articles were reviewed by the writing group, using titles and abstracts to screen for articles whose full texts were then retrieved. The writing group was instructed to exclude any articles that were in languages other than English, editorials, opinion pieces, book chapters, and any that were irrelevant to the questions being asked. This preliminary screening resulted in 392 articles, which were examined in detail by the writing group for inclusion in the literature review presented to the conference panelists.
Voting Process
Prior to the in-person conference, panelists were sent a number of consensus statements to clarify the appropriateness of the following therapies: functional appliances, dental arch expansion, myofunctional orthodontics, myofunctional therapy, buccal/lingual tethered tissue releases, and laser therapy (ablative and nonablative). They were asked to independently rate each therapy from 1 (least appropriate) to 9 (most appropriate) as a treatment for OSA and snoring in adults and children. Adults and pediatric populations were considered separately. Voting was organized into 3 ranges, with 1 to 3 being classified as treatments having Insufficient Evidence regarding their use as a monotherapy, 4 to 6 classified as treatments presenting Uncertain regarding their use as a monotherapy and 7 to 9 classified as treatments that are Appropriate for use as a monotherapy.
Additionally, the panelists were asked to rate their level of agreement with whether tooth extractions could cause OSA, and they independently rated this question from 1 (strongly disagree) to 9 (strongly agree). Again, these votes were organized into 3 ranges, with 1 to 3 being classified as Disagree with causation/contribution, 4 to 6 classified as Uncertain causation/contribution and 7 to 9 classified as Agree as to causation/contribution.
The RAND/UCLA method does not require a unanimous vote to arrive at consensus.1 Rather, the median of all panelist votes is calculated and consensus is achieved when at least 8 out of 11 panelists voted within one of the three aforementioned ranges.
During the in-person conference on November 3-4, 2023, the writing group presented findings from the literature via PowerPoint summaries regarding the therapies and extractions. All members had access to the literature for personal review. After each presentation, discussions took place with observers being allowed to ask questions or contribute to robust discussion. Following discussion, the 11 panelists participated in a second vote. They were permitted to change their vote from the initial voting round, based on discussion and consideration of evidence presented. If consensus was not achieved after the second round of voting, further discussion and a third round of voting took place. If consensus was not achieved after 3 rounds of voting, no further discussion or voting was conducted, and a lack of consensus for that therapy was declared.
LIMITATIONS
This consensus paper was not without limitations. First, as this was an introductory review of the literature in this field, only the PubMed database was searched. We did not search other databases or any gray/white literature. As such, some non-indexed studies may not have been considered. Furthermore, most of the studies reviewed were assessed to be based on a low quality of evidence. For instance, many of the systematic reviews and meta-analyses were considered to be of a lower quality evidence, because they failed to include controls and/or randomization, or had high between-study heterogeneity in their primary endpoints, as well as a lack of standardization of therapeutic regimens and study measures. Additionally, any literature which was published after the search cutoff date was not considered during the conference. Accordingly, our recommendations should be evaluated in this context and future studies should incorporate updated literature as it becomes available.
In particular, the dearth of controls poses a challenge when studying growing children. Numerous longitudinal studies, including the crossover Childhood Adenoid Tonsil Study (CHAT), suggests that somatic growth, inherent to the upper airways, can mitigate the presence or severity of disease.18 While longitudinal studies such as those undertaken at Penn State8 show a mild incidence in refractory disease after 8 years, the CHAT study showed that in as little as 7 months, nearly half of children with nothing more than watchful waiting may experience resolution of OSA.18 The identification of pediatric phenotypes, including possible genetic determinants of growth and maturation, may be helpful in predicting which children may require intervention and those who are likely to outgrow the presentation.
CONCLUSION & FUTURE RESEARCH
In total, there was concurrence among panelists that none of the reviewed therapies were Appropriate as first-line monotherapies. The implication does not necessarily preclude the use of these therapies, especially as possible secondary, tertiary, or rescue options, and tends to reflect both chasms within the literature, as well as a dearth of high-level research. In the absence of evidence demonstrating that a treatment is effective, the panelists relied on their respective clinical judgment and experience to make decisions. This may have led to either Uncertainty or concluding that Insufficient Evidence existed to support a specific treatment option, particularly if the discussion suggested that a therapy was possibly unnecessary or associated with potential risk. Furthermore, the future portends that specific pheno-, endo- and other sub-typing of patients may be identified as better suited to specific novel therapies.
Novel treatments continue to emerge that were not explored herein, either because no relevant peer-reviewed studies were identified, however weak, or because these therapies were so recent that they were not included among novel treatment options at the time that the consensus conference agenda was being developed. For example, claims of the possibility of using removable orthodontic appliances to foster adult bone growth or expansion to improve sleep and breathing require further studies. The explosion of lingual frenectomy procedures and centers devoted to this treatment warrants greater scrutiny to ensure that this treatment is not indiscriminately provided or urged upon patients in the absence of evidence to support its efficacy. Myofunctional therapy should be guided by clarification of minimum educational qualifications and standardized protocols underpinned by high-quality evidence.
All therapies, emerging or not, must be provided by following standard safety protocols by licensed professionals trained in their use, along with adequate informed consent, including whether the use of the treatment is considered off-label by the US Food and Drug Administration.
As with all consensus documents, our recommendations rely on the clinical expertise of panelists in conjunction with the available literature. When considering these recommendations, qualified dentists should use their best clinical judgment and knowledge of the patient’s specific needs. We believe this paper is the first of its kind to review the use of these novel therapies in both children and adults and, as such, can provide guidance to clinicians on effective treatment measures, while also directing researchers to consider studies in those areas where more complete data are needed. Moving forward, greater uniformity and standardization in reporting among studies is needed. Additionally, long-term randomized controlled studies with larger sample sizes should offer greater understanding as to the benefits and limitations of novel therapies and, in turn, provide clinicians with increased clarity on when best to consider these novel approaches in their patient populations.
ACKNOWLEDGEMENTS
The AADSM would like to thank Clinical Informationist Denise Nunes, MS, RN, MSLIS for her assistance on this project. The AADSM would also like to thank observing organizations including the American Academy of Sleep Medicine, the American Academy of Pediatric Dentistry, the American Society of Pediatric Otolaryngology, the American Academy of Orofacial Pain, the American Association of Orthodontists, the American College of Prosthodontists, and the American Speech-Language Hearing Society.
REFERENCES
- Fitch K, Bernstein SJ, Aguilar MD, et al. The RAND/UCLA Appropriateness Method User’s Manual. RAND Corporation; 2001. Accessed January 18,2024. https://www.rand.org/pubs/monograph_reports/MR1269.html
- Sateia MJ. International classification of sleep disorders-third edition: highlights and modifications. Chest. 2014;146(5):1387-1394. doi:10.1378/chest.14-0970
- World Health Organization (WHO). International Classification of Diseases, Eleventh Revision (ICD-11). Published 2021 2019. Accessed January 18,2024.https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/1919233290
- Levine M, Cantwell MK, Postol K, Schwartz DB. Dental sleep medicine standards for screening, treatment, and management of sleep-related breathing disorders in adults using oral appliance therapy: an update. J Dent Sleep Med. 2022;9(4). doi:10.15331/jdsm.7266
- Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: an update for 2015. J Clin Sleep Med JCSM Off Publ Am Acad Sleep Med. 2015;11(7):773-827. doi:10.5664/jcsm.4858
- Yeghiazarians Y, Jneid H, Tietjens JR, et al. Obstructive sleep apnea and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021;144(3):e56-e67. doi:10.1161/CIR.0000000000000988
- Kheirandish-Gozal L, Gozal D, eds. Sleep Disordered Breathing in Children: A Comprehensive Clinical Guide to Evaluation and Treatment. 1st edition. Humana; 2012.
- Bixler EO, Vgontzas AN, Lin HM, et al. Sleep disordered breathing in children in a general population sample: prevalence and risk factors. Sleep. 2009;32(6):731-736. doi:10.1093/sleep/32.6.731
- Li AM, So HK, Au CT, et al. Epidemiology of obstructive sleep apnoea syndrome in Chinese children: a two-phase community study. Thorax. 2010;65(11):991-997. doi:10.1136/thx.2010.134858
- Marcus CL, Brooks LJ, Draper KA, et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012;130(3):e714-755. doi:10.1542/peds.2012-1672
- Rosen CL, Larkin EK, Kirchner HL, et al. Prevalence and risk factors for sleep-disordered breathing in 8- to 11-year-old children: association with race and prematurity. J Pediatr. 2003;142(4):383-389. doi:10.1067/mpd.2003.28
- Ngiam J, Cistulli PA. Dental treatment for paediatric obstructive sleep apnea. Paediatr Respir Rev. 2015;16(3):174-181. doi:10.1016/j.prrv.2014.11.002
- Moin Anwer HM, Albagieh HN, Kalladka M, et al. The role of the dentist in the diagnosis and management of pediatric obstructive sleep apnea. Saudi Dent J. 2021;33(7):424-433. doi:10.1016/j.sdentj.2021.02.001
- Katyal V, Pamula Y, Daynes CN, et al. Craniofacial and upper airway morphology in pediatric sleep-disordered breathing and changes in quality of life with rapid maxillary expansion. Am J Orthod Dentofac Orthop. 2013;144(6):860-871. doi:10.1016/j.ajodo.2013.08.015
- Liu Y, Zhao T, Ngan P, Qin D, Hua F, He H. The dental and craniofacial characteristics among children with obstructive sleep apnoea: a systematic review and meta-analysis. Eur J Orthod. 2023;45(3):346-355. doi:10.1093/ejo/cjac074
- Galeotti A, Festa P, Viarani V, et al. Prevalence of malocclusion in children with obstructive sleep apnoea. Orthod Craniofac Res. 2018;21(4):242-247. doi:10.1111/ocr.12242
- McNamara JAJ, Lione R, Franchi L, et al. The role of rapid maxillary expansion in the promotion of oral and general health. Prog Orthod. 2015;16:33. doi:10.1186/s40510-015-0105-x
- Marcus CL, Moore RH, Rosen CL, et al. A randomized trial of adenotonsillectomy for childhood sleep apnea. N Engl J Med. 2013;368(25):2366-2376. doi:10.1056/NEJMoa1215881
- Ishman SL, Maturo S, Schwartz S, et al. Expert consensus statement: management of pediatric persistent obstructive sleep apnea after adenotonsillectomy. Otolaryngol--Head Neck Surg Off. 2023;168(2):115-130. doi:10.1002/ohn.159
- Mussi N, Forestiero R, Zambelli G, et al. The first-line approach in children with obstructive sleep apnea syndrome. J Clin Med. 2023;12(22):7092. doi:10.3390/jcm12227092
- Gozal D, Tan HL, Kheirandish-Gozal L. Treatment of obstructive sleep apnea in children: handling the unknown with precision. J Clin Med. 2020;9(3):888. doi:10.3390/jcm9030888
- Redline S, Cook K, Chervin RD, et al. Adenotonsillectomy for snoring and mild sleep apnea in children: a randomized clinical trial. JAMA. 2023;330(21):2084-2095. doi:10.1001/jama.2023.22114
- Tan YH, How CH, Chan YH, Teoh OH. Approach to the snoring child. Singapore Med J. 2020;61(4):170-175. doi:10.11622/smedj.2020054
- Muzumdar H, Arens R. Physiological effects of obstructive sleep apnea syndrome in childhood. Respir Physiol Neurobiol. 2013;188(3):370-382. doi:10.1016/j.resp.2013.05.006
- Guilleminault C, S Sullivan S. Towards restoration of continuous nasal breathing as the ultimate treatment goal in pediatric obstructive sleep apnea. Enliven Pediatr Neonatal Biol. 2014;01(01). doi:10.18650/2379-5824.11001
- Antonarakis GS, Kiliaridis S. Short-term anteroposterior treatment effects of functional appliances and extraoral traction on class II malocclusion. A meta-analysis. Angle Orthod. 2007;77(5):907-914. doi:10.2319/061706-244
- Carvalho F, Lentini-Oliveira D, Prado LB, Prado GF, Carvalho LB. Oral appliances and functional orthopaedic appliances for obstructive sleep apnoea in children. Cochrane Database Syst Rev. 2016;10(10):CD005520. doi:10.1002/14651858.CD005520.pub3
- Bucci R, Rongo R, Zunino B, et al. Effect of orthopedic and functional orthodontic treatment in children with obstructive sleep apnea: A systematic review and meta-analysis. Sleep Med Rev. 2023;67:101730. doi:10.1016/j.smrv.2022.101730
- Bariani RCB, Bigliazzi R, Cappellette Junior M, Moreira G, Fujita RR. Effectiveness of functional orthodontic appliances in obstructive sleep apnea treatment in children: literature review. Braz J Otorhinolaryngol.2022;88(2):263-278. doi:10.1016/j.bjorl.2021.02.010
- Bernardes R, Di Bisceglie Ferreira LM, Machado Júnior AJ, Jones MH. Effectiveness of functional orthopedic appliances as an alternative treatment among children and adolescents with obstructive sleep apnea: Systematic review and meta-analysis. Sleep Med. 2023;105:88-102. doi:10.1016/j.sleep.2023.03.008
- Machado-Júnior AJ, Signorelli LG, Zancanella E, Crespo AN. Randomized controlled study of a mandibular advancement appliance for the treatment of obstructive sleep apnea in children: A pilot study. Med Oral Patol Oral Cirugia Bucal. 2016;21(4):e403-407. doi:10.4317/medoral.21072
- Zhang C, He H, Ngan P. Effects of twin block appliance on obstructive sleep apnea in children: a preliminary study. Sleep Breath Schlaf Atm. 2013;17(4):1309-1314. doi:10.1007/s11325-013-0840-5
- Radwan ES, Maher A, Montasser MA. Effect of functional appliances on sleep-disordered breathing in Class II division 1 malocclusion children: Randomized controlled trial. Orthod Craniofac Res. Published online July 2023. doi:10.1111/ocr.12696
- Rizk S, Kulbersh VP, Al-Qawasmi R. Changes in the oropharyngeal airway of Class II patients treated with the mandibular anterior repositioning appliance. Angle Orthod. 2016;86(6):955-961. doi:10.2319/042915-295.1
- Cortese M, Pigato G, Casiraghi G, Ferrari M, Bianco E, Maddalone M. Evaluation of the Oropharyngeal Airway Space in Class II Malocclusion Treated with Mandibular Activator: A Retrospective Study. J Contemp Dent Pract. 2020;21(6):666-672.
- Abdalla Y, Kiliaridis S, Sonnesen L. Airway changes after fixed functional appliance treatment in children with and without morphologic deviations of the upper spine: A 3-dimensional CBCT study. Am J Orthod Dentofac Orthop Off Publ Am Assoc Orthod Its Const Soc Am Board Orthod. 2022;161(6):791-797. doi:10.1016/j.ajodo.2021.01.029
- Ghodke S, Utreja AK, Singh SP, Jena AK. Effects of twin-block appliance on the anatomy of pharyngeal airway passage (PAP) in class II malocclusion subjects. Prog Orthod. 2014;15(1):68. doi:10.1186/s40510-014-0068-3
- Temani P, Jain P, Rathee P, Temani R. Volumetric changes in pharyngeal airway in Class II division 1 patients treated with Forsus-fixed functional appliance: A three-dimensional cone-beam computed tomography study. Contemp Clin Dent. 2016;7(1):31-35. doi:10.4103/0976-237X.177100
- Horihata A, Ueda H, Koh M, Watanabe G, Tanne K. Enhanced increase in pharyngeal airway size in Japanese class II children following a 1-year treatment with an activator appliance. Int J Orthod Milwaukee Wis. 2013;24(4):35-40
- Keerthana P, Negi G, Chitra P. Airway changes in patients with sleep apnea using AdvanSync2 Class II correctors - a case series. Med Pharm Rep. 2022;95(3):337-347. doi:10.15386/mpr-1922
- Thereza-Bussolaro C, Oh HS, Lagravère M, Flores-Mir C. Pharyngeal dimensional changes in class II malocclusion treatment when using Forsus® or intermaxillary elastics - An exploratory study. Int Orthod. 2019;17(4):667-677. doi:10.1016/j.ortho.2019.08.023
- Batra A, Shetty V. Effect of twin-block appliance on pharyngeal airway, sleep patterns, and lung volume in children with class II malocclusion. J Contemp Dent Pract. 2022;23(1):66-73
- Maspero C, Giannini L, Galbiati G, Kairyte L, Farronato G. Upper airway obstuction [sic] in class II patients. Effects of Andresen activator on the anatomy of pharingeal [sic] airway passage. Cone beam evalution [sic]. Stomatologija. 2015;17(4):124-130.
- Iwasaki T, Takemoto Y, Inada E, et al. Three-dimensional cone-beam computed tomography analysis of enlargement of the pharyngeal airway by the Herbst appliance. Am J Orthod Dentofac Orthop Off Publ Am Assoc Orthod Its Const Soc Am Board Orthod. 2014;146(6):776-785. doi:10.1016/j.ajodo.2014.08.017
- Chervin RD, Hedger K, Dillon JE, Pituch KJ. Pediatric sleep questionnaire (PSQ): validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problems. Sleep Med. 2000;1(1):21-32. doi:10.1016/s1389-9457(99)00009-x
- Pavoni C, Cretella Lombardo E, Lione R, Bollero P, Ottaviani F, Cozza P. Orthopaedic treatment effects of functional therapy on the sagittal pharyngeal dimensions in subjects with sleep-disordered breathing and Class II malocclusion. Acta Otorhinolaryngol Ital Organo Uff Della Soc Ital Otorinolaringol E Chir Cerv-facc. 2017;37(6):479-485. doi:10.14639/0392-100X-1420
- Aurora RN, Zak RS, Karippot A, et al. Practice Parameters for the Respiratory Indications for Polysomnography in Children. Sleep. 2011;34(3):379-388.
- Kirk V, Baughn J, D’Andrea L, et al. American Academy of Sleep Medicine Position Paper for the Use of a Home Sleep Apnea Test for the Diagnosis of OSA in Children. J Clin Sleep Med JCSM Off Publ Am Acad Sleep Med. 2017;13(10):1199-1203. doi:10.5664/jcsm.6772
- Duan J, Xia W, Yang K, et al. The efficacy of twin-block appliances for the treatment of obstructive sleep apnea in children: a systematic review and meta-analysis. BioMed Res Int. 2022;2022:3594162. doi:10.1155/2022/3594162
- Yanyan M, Min Y, Xuemei G. Mandibular advancement appliances for the treatment of obstructive sleep apnea in children: a systematic review and meta-analysis. Sleep Med. 2019;60:145-151. doi:10.1016/j.sleep.2018.12.022
- Xiang M, Hu B, Liu Y, Sun J, Song J. Changes in airway dimensions following functional appliances in growing patients with skeletal class II malocclusion: A systematic review and meta-analysis. Int J Pediatr Otorhinolaryngol.2017;97:170-180. doi:10.1016/j.ijporl.2017.04.009
- Paolantonio EG, Ludovici N, Saccomanno S, La Torre G, Grippaudo C. Association between oral habits, mouth breathing and malocclusion in Italian preschoolers. Eur J Paediatr Dent. 2019;20(3):204-208. doi:10.23804/ejpd.2019.20.03.07
- Levrini L, Salone GS, Ramirez-Yanez GO. Efficacy of a pre-fabricated myofunctional appliance for the treatment of mild to moderate pediatric obstructive sleep apnea: a preliminary report. J Clin Pediatr Dent. 2018;42(6):475-477. doi:10.17796/1053-4625-42.6.14
- Katz D, DeMaria S, Heckman S, Lin F, Kushida C. Use of the Complete Airway Repositioning and Expansion (CARE) approach in 220 patients with Obstructive Sleep Apnea (OSA): A retrospective cohort study. Sleep Med. 2022;99:18-22. doi:10.1016/j.sleep.2022.07.005
- Buccheri A, Chinè F, Fratto G, Manzon L. Rapid maxillary expansion in obstructive sleep apnea in young patients: cardio-respiratory monitoring. J Clin Pediatr Dent. 2017;41(4):312-316. doi:10.17796/1053-4628-41.4.312
- Camacho M, Chang ET, Song SA, et al. Rapid maxillary expansion for pediatric obstructive sleep apnea: A systematic review and meta-analysis. Laryngoscope. 2017;127(7):1712-1719. doi:10.1002/lary.26352
- Niu X, Di Carlo G, Cornelis MA, Cattaneo PM. Three-dimensional analyses of short- and long-term effects of rapid maxillary expansion on nasal cavity and upper airway: A systematic review and meta-analysis. Orthod Craniofac Res. 2020;23(3):250-276. doi:10.1111/ocr.12378
- Machado AJJ, Crespo AN, Pauna HF. Rapid maxillary expansion in pediatric patients with obstructive sleep apnea: current and future perspectives. Sleep Med. 2018;51:7-8. doi:10.1016/j.sleep.2018.06.002
- Huynh NT, Desplats E, Almeida FA. Orthodontics treatments for managing obstructive sleep apnea syndrome in children: A systematic review and meta-analysis. Sleep Med Rev. 2016;25:84-94. doi:10.1016/j.smrv.2015.02.002
- Pirelli P, Fiaschetti V, Fanucci E, et al. Cone beam CT evaluation of skeletal and nasomaxillary complex volume changes after rapid maxillary expansion in OSA children. Sleep Med. 2021;86:81-89. doi:10.1016/j.sleep.2021.08.011
- Fastuca R, Perinetti G, Zecca PA, Nucera R, Caprioglio A. Airway compartments volume and oxygen saturation changes after rapid maxillary expansion: a longitudinal correlation study. Angle Orthod. 2015;85(6):955-961. doi:10.2319/072014-504.1
- Fastuca R, Meneghel M, Zecca PA, et al. Multimodal airway evaluation in growing patients after rapid maxillary expansion. Eur J Paediatr Dent. 2015;16(2):129-134.
- Eichenberger M, Baumgartner S. The impact of rapid palatal expansion on children’s general health: a literature review. Eur J Paediatr Dent. 2014;15(1):67-71.
- Akkari M, Marianowski R, Chalumeau F, et al. French Society of Otorhinolaryngology and Head and Neck Surgery (SFORL) guidelines concerning the role of otorhinolaryngologists in the management of paediatric obstructive sleep apnoea syndrome: Follow-up protocol for treated children. Eur Ann Otorhinolaryngol Head Neck Dis. 2018;135(6):427-431. doi:10.1016/j.anorl.2018.09.006
- Villa MP, Rizzoli A, et al. Rapid maxillary expansion outcomes in treatment of obstructive sleep apnea in children. Sleep Med. 2015;16(6):709-716. doi:10.1016/j.sleep.2014.11.019
- Quo SD, Hyunh N, Guilleminault C. Bimaxillary expansion therapy for pediatric sleep-disordered breathing. Sleep Med. 2017;30:45-51. doi:10.1016/j.sleep.2016.03.011
- Rdescu OD, Colosi HA, Albu S. Effects of rapid palatal expansion (RPE) and twin block mandibular advancement device (MAD) on pharyngeal structures in Class II pediatric patients from Cluj-Napoca, Romania. Cranio J Craniomandib Pract. 2020;38(1):22-29. doi:10.1080/08869634.2018.1475940
- Pirelli P, Fanucci E, Giancotti A, Di Girolamo M, Guilleminault C. Skeletal changes after rapid maxillary expansion in children with obstructive sleep apnea evaluated by low-dose multi-slice computed tomography. Sleep Med. 2019;60:75-80. doi:10.1016/j.sleep.2018.11.023
- Kim A, Cho HJ, Choi EK, Choi YJ. Improvement in obstructive sleep apnea in a child with Down syndrome with rapid palatal expansion. J Clin Sleep Med JCSM Off Publ Am Acad Sleep Med. 2022;18(7):1885-1888. doi:10.5664/jcsm.9968
- Galeotti A, Gatto R, Caruso S, et al. Effects of rapid palatal expansion on the upper airway space in children with obstructive sleep apnea (OSA): a case-control study. Child Basel Switz. 2023;10(2). doi:10.3390/children10020244
- Hoxha S, Kaya-Sezginer E, Bakar-Ates F, Köktürk O, Toygar-Memikoğlu U. Effect of semi-rapid maxillary expansion in children with obstructive sleep apnea syndrome: 5-month follow-up study. Sleep Breath Schlaf Atm. 2018;22(4):1053-1061. doi:10.1007/s11325-018-1636-4
- Bellon M, Boutin F, Haddad R, Frapier L. Effectiveness of orthopaedic treatments on the enlargement of the upper airways: Overview of systematic reviews. Int Orthod. 2023;21(2):100745. doi:10.1016/j.ortho.2023.100745
- Barbosa DF, Bana LF, Michel MCB, Meira E Cruz M, Zancanella E, Machado Júnior AJ. Rapid maxillary expansion in pediatric patients with obstructive sleep apnea: an umbrella review. Braz J Otorhinolaryngol. 2023;89(3):494-502. doi:10.1016/j.bjorl.2023.02.004
- Fernández-Barriales M, Lafuente-Ibáñez de Mendoza I, Alonso-Fernández Pacheco JJ, Aguirre-Urizar JM. Rapid maxillary expansion versus watchful waiting in pediatric OSA: A systematic review. Sleep Med Rev. 2022;62:101609. doi:10.1016/j.smrv.2022.101609
- Bariani RCB, Bigliazzi R, de Moura Guimarães T, Tufik S, Moreira GA, Fujita RR. The effects of rapid maxillary expansion on persistent pediatric snoring post-tonsillectomy. Sleep Breath Schlaf Atm. 2023;27(4):1227-1235. doi:10.1007/s11325-022-02724-w
- Caprioglio A, Meneghel M, Fastuca R, Zecca PA, Nucera R, Nosetti L. Rapid maxillary expansion in growing patients: correspondence between 3-dimensional airway changes and polysomnography. Int J Pediatr Otorhinolaryngol. 2014;78(1):23-27. doi:10.1016/j.ijporl.2013.10.011
- Giannasi LC, Santos IR, Alfaya TA, et al. Effect of a rapid maxillary expansion on snoring and sleep in children: a pilot study. Cranio J Craniomandib Pract. 2015;33(3):169-173. doi:10.1179/2151090314Y.0000000029
- Bariani RCB, Bigliazzi R, Badreddine FR, et al. A clinical trial on 3D CT scan and polysomnographyc changes after rapid maxillary expansion in children with snoring. Braz J Otorhinolaryngol. 2022;88:S162-S170. doi:10.1016/j.bjorl.2022.04.004
- Abdullatif J, Certal V, Zaghi S, et al. Maxillary expansion and maxillomandibular expansion for adult OSA: A systematic review and meta-analysis. J Cranio-Maxillo-fac Surg Off Publ Eur Assoc Cranio-Maxillo-fac Surg. 2016;44(5):574-578. doi:10.1016/j.jcms.2016.02.001
- Vinha PP, Faria AC, Xavier SP, Christino M, de Mello-Filho FV. Enlargement of the Pharynx Resulting From Surgically Assisted Rapid Maxillary Expansion. J Oral Maxillofac Surg Off J Am Assoc Oral Maxillofac Surg. 2016;74(2):369-379. doi:10.1016/j.joms.2015.06.157
- Pereira-Filho VA, Monnazzi MS, Gabrielli MAC, et al. Volumetric upper airway assessment in patients with transverse maxillary deficiency after surgically assisted rapid maxillary expansion. Int J Oral Maxillofac Surg. 2014;43(5):581-586. doi:10.1016/j.ijom.2013.11.002
- Liu SYC, Guilleminault C, Huon LK, Yoon A. Distraction Osteogenesis Maxillary Expansion (DOME) for Adult Obstructive Sleep Apnea Patients with High Arched Palate. Otolaryngol Neck Surg Off J Am Acad Otolaryngol-Head Neck Surg. 2017;157(2):345-348. doi:10.1177/0194599817707168
- Behrents RG, Shelgikar AV, Conley RS, et al. Obstructive sleep apnea and orthodontics: An American Association of Orthodontists White Paper. Am J Orthod Dentofac Orthop Off Publ Am Assoc Orthod Its Const Soc Am Board Orthod. 2019;156(1):13-28.e1. doi:10.1016/j.ajodo.2019.04.009
- Carré F, Nguyen XL, Garrec P, Baujat B, and Lacau St Guily J, Pételle B. Surgically assisted rapid maxillary expansion for obstructive sleep apnea adult patients: Our experience in 7 cases. Clin Otolaryngol Off J ENT-UK Off J Neth Soc Oto-Rhino-Laryngol Cervico-Facial Surg. 2021;46(6):1200-1204. doi:10.1111/coa.13816
- Abdelwahab M, Yoon A, Okland, T, et al. Impact of distraction osteogenesis maxillary expansion on the internal nasal valve in obstructive sleep apnea. Otolaryngol Head Neck Surg. 2019;161(2):362-367. doi:10.1177/0194599819842808
- Vinha PP, Eckeli AL, Faria AC, Xavier SP, de Mello-Filho FV. Effects of surgically assisted rapid maxillary expansion on obstructive sleep apnea and daytime sleepiness. Sleep Breath Schlaf Atm. 2016;20(2):501-508. doi:10.1007/s11325-015-1214-y
- Li K, Quo S, Guilleminault C. Endoscopically-assisted surgical expansion (EASE) for the treatment of obstructive sleep apnea. Sleep Med. 2019;60:53-59. doi:10.1016/j.sleep.2018.09.008
- Carrasco-Llatas M, O’Connor-Reina C, Calvo-Henríquez C. The role of myofunctional therapy in treating sleep-disordered breathing: a state-of-the-art review. Int J Environ Res Public Health. 2021;18(14). doi:10.3390/ijerph18147291
- Camacho M, Certal V, Abdullatif J, et al. Myofunctional therapy to treat obstructive sleep apnea: a systematic review and meta-analysis. Sleep. 2015;38(5):669-675. doi:10.5665/sleep.4652
- Guimarães KC, Drager LF, Genta PR, Marcondes BF, Lorenzi-Filho G. Effects of oropharyngeal exercises on patients with moderate obstructive sleep apnea syndrome. Am J Respir Crit Care Med. 2009;179(10):962-966. doi:10.1164/rccm.200806-981OC
- de Felício CM, da Silva Dias FV, Folha GA, et al. Orofacial motor functions in pediatric obstructive sleep apnea and implications for myofunctional therapy. Int J Pediatr Otorhinolaryngol. 2016;90:5-11. doi:10.1016/j.ijporl.2016.08.019
- Diaféria G, Santos-Silva R, Truksinas E, et al. Myofunctional therapy improves adherence to continuous positive airway pressure treatment. Sleep Breath Schlaf Atm. 2017;21(2):387-395. doi:10.1007/s11325-016-1429-6
- Kim AM, Keenan BT, Jackson N, et al. Tongue fat and its relationship to obstructive sleep apnea. Sleep. 2014;37(10):1639-1648. doi:10.5665/sleep.4072
- Rueda JR, Mugueta-Aguinaga I, Vilaró J, Rueda-Etxebarria M. Myofunctional therapy (oropharyngeal exercises) for obstructive sleep apnoea. Cochrane Database Syst Rev. 2020;11(11):CD013449. doi:10.1002/14651858.CD013449.pub2
- Hsu B, Emperumal CP, Grbach VX, Padilla M, Enciso R. Effects of respiratory muscle therapy on obstructive sleep apnea: a systematic review and meta-analysis. J Clin Sleep Med JCSM Off Publ Am Acad Sleep Med. 2020;16(5):785-801. doi:10.5664/jcsm.8318
- Villa MP, Evangelisti M, Martella S, Barreto M, Del Pozzo M. Can myofunctional therapy increase tongue tone and reduce symptoms in children with sleep-disordered breathing? Sleep Breath Schlaf Atm. 2017;21(4):1025-1032. doi:10.1007/s11325-017-1489-2
- Villa MP, Brasili L, Ferretti A, et al. Oropharyngeal exercises to reduce symptoms of OSA after AT. Sleep Breath Schlaf Atm. 2015;19(1):281-289. doi:10.1007/s11325-014-1011-z
- Orofacial Myofunctional Disorders. American Speech-Language-Hearing Association. Accessed January 18, 2024. https://www.asha.org/practice-portal/clinical-topics/orofacial-myofunctional-disorders/
- Randerath, W, Verbraecken J, de Raaff CAL, et al. European Respiratory Society guideline on non-CPAP therapies for obstructive sleep apnoea. Eur Respir Rev Off J Eur Respir Soc. 2021;30(162). doi:10.1183/16000617.0200-2021
- O’Shea JE, Foster JP, O’Donnell CP, et al. Frenotomy for tonguetie in newborn infants. Cochrane Database Syst Rev. 2017;(3). doi:10.1002/14651858.CD011065.pub2
- Frenectomy for the Correction of Ankyloglossia: A Review of Clinical Effectiveness and Guidelines. Canadian Agency for Drugs and Technologies in Health; 2016. Accessed January 18, 2024. http://www.ncbi.nlm.nih.gov/books/NBK373454/
- Walsh J, Links A, Boss E, Tunkel D. Ankyloglossia and lingual frenotomy: national trends in inpatient diagnosis and management in the United States, 1997-2012. Otolaryngol Head Neck Surg. 2017;156(4):735-740. doi:10.1177/0194599817690135
- Messner AH, Walsh J, Rosenfeld RM, et al. Clinical Consensus Statement: Ankyloglossia in Children. Otolaryngol Neck Surg Off J Am Acad Otolaryngol-Head Neck Surg. 2020;162(5):597-611. doi:10.1177/0194599820915457
- Tadros S, Ben-Dov T, Catháin ÉÓ, Anglin C, April MM. Association between superior labial frenum and maxillary midline diastema - a systematic review. Int J Pediatr Otorhinolaryngol. 2022;156:111063. doi:10.1016/j.ijporl.2022.111063
- Guilleminault C, Huseni S, Lo L. A frequent phenotype for paediatric sleep apnoea: short lingual frenulum. ERJ Open Res. 2016;2(3):00043-02016. doi:10.1183/23120541.00043-2016
- Huang Y, Quo S, Berkowski, JA, Guilleminault, C. Short lingual frenulum and obstructive sleep apnea in children. Int J Pediatr Res. 2015;1(003)
- Varadan M, Chopra A, Sanghavi AD, Sivaraman K, Gupta K. Etiology and clinical recommendations to manage the complications following lingual frenectomy: A critical review. J Stomatol Oral Maxillofac Surg. 2019;120(6):549-553. doi:10.1016/j.jormas.2019.06.003
- Fujita S, Conway W, Zorick F, Roth T. Surgical correction of anatomic azbnormalities [sic] in obstructive sleep apnea syndrome: uvulopalatopharyngoplasty. Otolaryngol Head Neck Surg. 1981;89(6):923-934. doi:10.1177/019459988108900609
- Kamami YV. Laser CO2 for snoring. Preliminary results. Acta Otorhinolaryngol Belg. 1990;44(4):451-456.
- Powell NB, Riley RW, Troell RJ, Li K, Blumen MB, Guilleminault C. Radiofrequency volumetric tissue reduction of the palate in subjects with sleep-disordered breathing. Chest. 1998;113(5):1163-1174. doi:10.1378/chest.113.5.1163
- Aurora RN, Casey KR, Kristo D, et al. Practice parameters for the surgical modifications of the upper airway for obstructive sleep apnea in adults. Sleep. 2010;33(10):1408-1413. doi:10.1093/sleep/33.10.1408
- Neruntarat C, Khuancharee K, Shoowit P. Er:YAG laser for snoring: a systemic review and meta-analysis. Lasers Med Sci. 2020;35(6):1231-1238. doi:10.1007/s10103-020-02987-3
- Kakkar M, Malik S, Gupta B, Vaid N, George R, Singh S. Use of Laser in Sleep Disorders: A Review on Low Laser Uvulopalatoplasty. Sleep Disord. 2021;2021:8821073. doi:10.1155/2021/8821073
- Picavet VA, Dellian M, Gehrking E, Sauter A, Hasselbacher K. Treatment of snoring using a non-invasive Er:YAG laser with SMOOTH mode (NightLase): a randomized controlled trial. Eur Arch Otorhinolaryngol. 2023;280(1):307-312. doi:10.1007/s00405-022-07539-9
- Kassab AN, Kharbotly AE, Elsamie AA, Ahmed MR. A Long-Term Follow-up Study for the Treatment of Snoring after Using Patterned Non-Ablative Erbium: YAG 2,940 nm Laser. Int Arch Otorhinolaryngol. 2023;27(1):e104-e110. doi:10.1055/s-0042-1744171
- Cetinkaya EA, Turker M, Kiraz K, Gulkesen HK. Er:Yag laser treatment of simple snorers in an outpatient setting. ORL J Oto-Rhino-Laryngol Its Relat Spec. 2016;78(2):70-76. doi:10.1159/000443510
- Miracki K, Vizintin Z. Nonsurgical Minimally Invasive Er:YAG Laser Snoring Treatment. J Laser Health Acad. 2013;2013(1):36-41.
- Monteiro L, Macedo A, Corte-Real L, Salazar F, Pacheco JJ. Treatment of snoring disorder with a non-ablactive [sic] Er:YAG laser dual mode protocol. An interventional study. J Clin Exp Dent. 2020;12(6):e561-e567. doi:10.4317/jced.56953
- Shiffman HS, Khorsandi, J, Cauwels NM. Minimally Invasive Combined Nd:YAG and Er:YAG Laser-Assisted Uvulopalatoplasty for Treatment of Obstructive Sleep Apnea. Photobiomodulation Photomed Laser Surg. 2021;39(8):550-557. doi:10.1089/photob.2020.4947
- Storchi IF, Parker S, Bovis F, Benedicenti S, Amaroli A. Outpatient erbium:YAG (2940 nm) laser treatment for snoring: a prospective study on 40 patients. Lasers Med Sci. 2018;33(2):399-406. doi:10.1007/s10103-018-2436-6
- Svahnström K. Er:YAG Laser Treatment of Sleep-Disordered Breathing. J Laser Health Acad. 2013;2013(2):13-16.
- Frelich H, cierski W, Marków M, Frelich J, Frelich H, Maciej M. Minimally invasive erbium laser treatment for selected snorers. Lasers Med Sci. 2019;34(7):1413-1420. doi:10.1007/s10103-019-02731-6
- Y. S. Lee C, C. Y. Lee C. Evaluation of a non-ablative Er: YAG laser procedure to increase the oropharyngeal airway volume: A pilot study. Dent Oral Craniofacial Res. 2015;1(3). doi:10.15761/DOCR.1000113
- Fini Storchi I, Frosecchi M, Bovis F, et al. Snoring and Sleep-Related Symptoms: A Novel Non-Invasive 808 nm Wavelength Diode Laser Non-Ablative Outpatient Treatment. A Prospective Pilot-Study on 45 Patients. Photonics. 2021;8(3):69. doi:10.3390/photonics8030069
- Camacho M, Nesbitt NB, Lambert E, et al. Laser-Assisted Uvulopalatoplasty for Obstructive Sleep Apnea: A Systematic Review and Meta-Analysis. Sleep. 2017;40(3). doi:10.1093/sleep/zsx004
- Wischhusen J, Qureshi U, Camacho M. Laser-assisted uvulopalatoplasty (LAUP) complications and side effects: a systematic review. Nat Sci Sleep. 2019;11:59-67. doi:10.2147/NSS.S178540
- Hu Z, Yin X, Liao J, Zhou C, Yang Z, Zou S. The effect of teeth extraction for orthodontic treatment on the upper airway: a systematic review. Sleep Breath Schlaf Atm. 2015;19(2):441-451. doi:10.1007/s11325-015-1122-1
- Stefanovic N, El H, Chenin DL, Glisic B, Palomo JM. Three-dimensional pharyngeal airway changes in orthodontic patients treated with and without extractions. Orthod Craniofac Res. 2013;16(2):87-96. doi:10.1111/ocr.12009
- Guilleminault C, Abad VC, Chiu HY, Peters B, Quo S. Missing teeth and pediatric obstructive sleep apnea. Sleep Breath Schlaf Atm. 2016;20(2):561-568. doi:10.1007/s11325-015-1238-3
- Ng JH, Song YL, Yap AUJ. Effects of bicuspid extractions and incisor retraction on upper airway of Asian adults and late adolescents: A systematic review. J Oral Rehabil. 2019;46(11):1071-1087. doi:10.1111/joor.12854
- Larsen AJ, Rindal DB, Hatch JP, et al. Evidence supports no relationship between obstructive sleep apnea and premolar extraction: an electronic health records review. J Clin Sleep Med JCSM Off Publ Am Acad Sleep Med. 2015;11(12):1443-1448. doi:10.5664/jcsm.5284
- Vejwarakul W, Ko EWC, Lin CH. Evaluation of pharyngeal airway space after orthodontic extraction treatment in class II malocclusion integrating with the subjective sleep quality assessment. Sci Rep. 2023;13(1):9210. doi:10.1038/s41598-023-36467-9
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted in final revised form April 8, 2024
Address correspondence to: Dr. Rose Sheats, DMD, MPH; Email: rosesheats@gmail.com
DISCLOSURE STATEMENT
Dr Aarab reports receiving research grants from Vivisol-ResMed/Stichting Life Sciences Health. Dr Stauffer reports receiving sample displays of myofunctional appliances and habit correctors, as well as a G-series appliance for personal use.