Special Article 1, Issue 1.1
Definition of an Effective Oral Appliance for the Treatment of Obstructive Sleep Apnea and Snoring: A Report of the American Academy of Dental Sleep Medicine
http://dx.doi.org/10.15331/jdsm.3738
Consensus Conference Participants: Steven C. Scherr, DDS, Moderator1 *; Leslie C. Dort, DDS, Moderator2 *; Fernanda R. Almeida, DDS, PhD3 ; Kathleen M. Bennett, DDS4 ; Norman T. Blumenstock, DDS5 ; B. Gail Demko, DMD6 ; Gregory K. Essick, DDS, PhD7 *; Sheri G. Katz, DDS8 ; Paul M. McLornan, DDS9 ; Katherine S. Phillips, DDS10*; Ronald S. Prehn, DDS11*; Robert R. Rogers, DMD12; Thomas G. Schell, DMD13; Rose D. Sheats, DMD14*; Flavia P. Sreshta, DDS15
*Participated in writing the manuscript. 1 Pikesville, MD; 2 Calgary, Canada; 3 Vancouver, Canada; 4 Cincinnati, OH; 5 Monroe Township, NJ; 6 Weston, MA; 7 Chapel Hill, NC; 8 Decatur, GA; 9 San Antonio, TX; 10Oakbrook, IL; 11The Woodlands, TX; 12Wexford, PA; 13Lebanon, NH, 14Chapel Hill, NC; 15Cleveland, OH
ABSTRACT
In response to the demands of an emerging profession to set standards of care, the Board of Directors of the American Academy of Dental Sleep Medicine (AADSM) brought together leaders in the profession to develop the definition of an effective oral appliance for the treatment of sleep disordered breathing based on current research and clinical experience. On February 15-17, 2013, a consensus conference was held in Tampa, Florida. Fifteen leaders in the profession used the modified RAND/UCLA Appropriateness Method to craft an empiric definition of an effective oral appliance with emphasis on purpose, physical features and function. A definition was developed and in March 2013 was accepted by the Board of Directors of the AADSM.
The purpose of this report is twofold. First, it presents a systematic review of all available level one and two literature (based on Oxford Centre methodology) to validate the accepted definition of an effective oral appliance. Second, this report details the processes employed and clarifies inclusion and exclusion rationale.
Future research, improved methods, and innovations in biomaterials will continue to advance the profession of dental sleep medicine. This definition provides a foundation and framework to guide both future investigations and current treatment of individuals with sleep disordered breathing.
Citation:
Scherr SC, Dort LC, Almeida FR, Bennett KM, Blumenstock NT, Demko BG, Essick GK, Katz SG, McLornan PM, Phillips KS, Prehn RS, Rogers RR, Schell TG, Sheats RD, Sreshta FP. Definition of an effective oral appliance for the treatment of obstructive sleep apnea and snoring: a report of the American Academy of Dental Sleep Medicine. Journal of Dental Sleep Medicine 2014;1(1):39–50.
1.0 INTRODUCTION
Sleep disordered breathing constitutes a spectrum of repetitive upper airway narrowing episodes during sleep characterized by snoring, elevated upper airway resistance, and/or obstructive sleep apnea (OSA).1 Recurring airflow restriction often results in blood oxyhemoglobin desaturation, arousals from sleep, and sleep fragmentation.2,3 Common symptomatic manifestations include hypersomnolence4 , insomnia, neurocognitive deficits,5,6 bed partner disturbance, mood disorders,7,8 nocturia,9 and fatigue. Diminished reaction time and increased susceptibility to motor vehicle crashes have also been reported.10,11 OSA is an independent risk factor for the development of hypertension, coronary artery disease, epithelial dysfunction leading to ischemia,12 cardiac arrhythmias,13 stroke, insulin resistance,14,15 and all-cause mortality.16-22 Addressing the anatomic and physiologic deficiencies related to sleep disordered breathing improves outcomes and quality of life.23-25
Oral appliances, designed for the treatment of sleep disordered breathing, are commonly used today.26 Oral appliances are silent, portable, noninvasive, and well tolerated.27,28 Most side effects tend to be transient, though permanent dental consequences may occur.29-33 There has been a proliferation of various designs since the first commercially available oral appliances were introduced in the 1980s.34 To date, the United States Food and Drug Administration (FDA) has cleared numerous oral appliances, nearly all with 510k clearance, which acknowledges that the design has substantial equivalence to another appliance that had already been cleared.35 The vast majority of oral appliances today trace FDA clearance to a single orthodontic predicate device that was marketed prior to the 1976 passage of an amendment that required medical device registration with the FDA.36 FDA clearance is primarily directed at patient safety and requires minimal evidence of effectiveness.
Pierre Robin was the first to document the use of a mandibular advancement oral appliance for the treatment of nocturnal airway obstruction in 1923. However, oral appliances were apparently forgotten until 1982, when Cartwright and Samelson reported the use of a novel tongue retainer.38 Within a few years, several authors rediscovered mandibular advancement oral appliances.39 Research on these devices has increased exponentially since that time.40 Efficacy depends on a number of factors including severity of the sleep disordered breathing, materials, method of fabrication, adjustability, and the degree of protrusion.41 Much creativity and ingenuity have gone into developing various oral appliance design features. This has contributed to confusion regarding which features are fundamental to treatment success. The absence of accepted standards of appliance design encumbers interpretation and comparison of research findings. Third-party payers are challenged by the lack of an empirical definition of an effective oral appliance as well. In order to address these deficiencies, a consensus conference was held to develop an evidence-based definition of an effective oral appliance for the treatment of sleep disordered breathing and to establish a standardized benchmark for both research and clinical practice.
The definition presented herein is intended to represent the best practices of oral appliance purpose, physical features, and function. Using a standardized definition for an effective oral appliance will foster consistency in clinical practice and research, allowing for results to be more easily compared. It is expected that the empirical definition of an effective oral appliance will be reevaluated and revised as new methods and evidence become available. This definition is not intended to supersede clinical judgment as individual patient needs may dictate alternative methods. It does serve as a clinically relevant standard for oral appliance selection by dental sleep medicine practitioners, and as a guidepost for developers of the next generation of oral appliances.
2.0 BACKGROUND
The American Academy of Sleep Medicine (AASM) first published practice parameters for the use of oral appliances in the treatment of OSA and snoring in 1995.42 These practice parameters were updated in 200543 and are currently being revised by a joint AADSM and AASM task force. “Oral appliances are indicated for use in patients with mild to moderate obstructive sleep apnea who prefer them to continuous positive airway pressure (CPAP) therapy, or who do not respond to, are not appropriate candidates for, or who fail treatment attempts with CPAP.” “Oral appliances should be fitted by qualified dental personnel who are trained and experienced in the overall care of oral health, the temporomandibular joint, dental occlusion and associated oral structures. Dental management of patients with oral appliances should be overseen by practitioners who have undertaken serious training in sleep medicine and/or sleep related breathing disorders with focused emphasis on the proper protocol for diagnosis, treatment, and follow up (Option).”44 This AASM clinical practice guideline does not describe or define an oral appliance and acknowledges that research is needed to clarify oral appliance design characteristics.
The Centers for Medicare and Medicaid Services (CMS) formally acknowledged oral appliance therapy when it published a local coverage determination (LCD) for oral appliances for obstructive sleep apnea that became effective January 3, 2011.45 The LCD outlined a mechanical definition of an oral appliance based on a predicate appliance received by medical directors in 1999. In July 2012, CMS revised its definition of an oral appliance in the LCD46 to be so narrow as to initially disallow all oral appliance designs except one. Though a few additional designs have since been accepted by the Medicare Pricing, Data Analysis and Coding (PDAC) contractor, our conversations with Medicare representatives have made it clear that their working definition of an oral appliance is based more on serendipity and statutory regulation, rather than science and clinical relevance.
The AADSM invited a spectrum of clinical and research dental sleep medicine experts from across North America to participate in a consensus conference to develop a formal definition of an effective oral appliance. Fifteen members accepted and attended a consensus conference held on February 15-17, 2013 in Tampa, Florida. All participants of the consensus conference and contributors to the accompanying paper completed thorough conflict-of-interest statements and were found to have no conflicts of interest with regard to this subject.
3.0 METHODS
The consensus conference followed a modified RAND/UCLA Appropriateness Method.47 Approximately one month before the conference, participants were provided the latest literature on oral appliance therapy, product information on oral appliances currently in use in clinical practice, and Medicare’s current billing and coverage criteria. Each participant was asked to review the materials provided and submit individual items that could be included in the final definition. These items, also referred to as elements, were to address the following about an oral appliance: the purpose (the intent of an oral appliance), physical features (what physical attributes are vital for an oral appliance to be effective), and function (how the oral appliance should work in order to fulfill its purpose). These individual elements were all compiled and each participant was asked to vote on a scale from 1-9 (1 being highly inappropriate and 9 being highly appropriate) whether it was appropriate to include each element in the final definition. Participants were asked to rate elements based on a combination of the evidence they reviewed and their best clinical judgment, considering the average patient and disregarding cost in order to focus on effectiveness. This Round 1 voting occurred via email before the conference. Scores were then grouped by median to determine the consensus of the group, and the level of agreement was determined based on the distribution of voting across the scale. This information comprised the starting point for the face-to-face discussions at the consensus conference.
Two members from the AADSM Board of Directors and staff members facilitated the conference and led participants through the consensus process. Over the course of three days, participants discussed the results from Round 1 voting in three sessions for elements that addressed the purpose, physical features, and function of an effective oral appliance. Additional rounds of voting were required to arrive at consensus and to develop a final list of elements that participants agreed were appropriate to be included in the final definition. The definition was drafted using this final list of elements which was unanimously accepted by vote of the consensus conference participants and later approved by the AADSM Board of Directors.
The purpose, key physical features and function of an effective oral appliance included in the definition were supported by evidence collected through a comprehensive review of current peer-reviewed scientific literature on oral appliances. The literature search was performed using a combination of medical subject heading (MeSH) terms and keywords in MEDLINE. The MeSH terms used were sleep apnea syndromes, snoring, orthodontic appliances, and mandibular advancement/instrumentation. The disorder keywords used were sleep apnea, OSA, sleep-related breathing disorder(s), SRBD, sleep-disordered breathing, SDB, and snoring. The treatment keywords used were oral, intraoral, dental, orthodontic(s), mandibular, tongue retaining, tongue stabilizing, occlusal, or titratable paired with appliance(s), splint(s), or device(s). Search results were retrieved for literature published from the beginning of indexing by MEDLINE through March 8, 2013. The limits of the search were: humans, English and French, no editorials, letters, biographies, newspaper articles, comments, or case reports. The literature search strategy resulted in a total of 772 articles.
The Writing Group, comprised of six participants of the consensus conference, reviewed the abstracts of all the available literature to identify articles that would support the different elements included in the final definition. Each reviewer made note of which section(s) of the definition (purpose, physical features, or function) that the article supported.
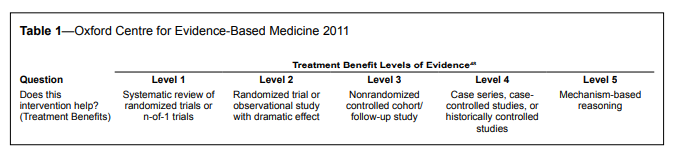
The assessment of evidence in the accepted articles was performed using the Oxford Centre for Evidence-based Medicine Levels of Evidence table (See Table 1). All accepted studies were assigned a level of evidence by a member of the Writing Group. Any article where the level was in question was reviewed by an additional group member for a final decision. The final evidence used to support the definition of an effective oral appliance was limited to Level 1 and 2 studies, where possible. The final number of articles accepted as evidence, from both the literature search and pearling, to support the final definition was 113.
Table 1Oxford Centre for Evidence-Based Medicine 2011 |
{kind=link}
This definition describes an effective oral appliance which should meet the needs of most patients in most situations. This definition should not, however, be considered inclusive of all proper methods of care or exclusive of other methods of care reasonably directed toward obtaining the same results. The ultimate judgment regarding the specific care of an individual patient must be made by the clinician, in light of the individual circumstances presented by the patient, available diagnostic tools, accessible treatment options, and resources.
4.0 DEFINITION
Following the conference, the drafted definition was presented to and approved by the AADSM Board of Directors in March 2013. The final approved definition is as follows:
The purpose of an oral appliance is to treat obstructive sleep apnea (OSA), primary snoring, and associated symptoms. Oral appliances are intended to decrease the frequency and/or duration of apneas, hypopneas, respiratory effort related arousals (RERAs) and/or snoring events. Oral appliances have been demonstrated to improve nocturnal oxygenation as well as the adverse health and social consequences of OSA and snoring. Oral appliances are indicated for patients with mild to moderate OSA and primary snoring. Oral appliances are accepted therapy for patients with severe OSA who do not respond to or are unable or unwilling to tolerate positive airway pressure (PAP) therapies. Although oral appliances are typically used as a stand-alone therapy, they can serve as an adjunct to PAP therapy and/or other treatment modalities for the management of OSA.
For this definition oral appliances refer to mandibular advancement devices because they are the most effective and widely used in clinical practice. Accordingly the function of an oral appliance is to protrude and help stabilize the mandible in order to maintain a patent upper airway during sleep.
An oral appliance is custom fabricated using digital or physical impressions and models of an individual patient’s oral structures. As such, it is not a primarily prefabricated item that is trimmed, bent, relined or otherwise modified. It is made of biocompatible materials and engages both the maxillary and mandibular arches. The oral appliance has a mechanism that allows the mandible to be advanced in increments of 1 mm or less with a protrusive adjustment range of at least 5 mm. In addition, reversal of the advancement must be possible. The protrusive setting must be verifiable. The appliance is suitable for placement and removal by the patient or caregiver. It maintains a stable retentive relationship to the teeth, implants or edentulous ridge and retains the prescribed setting during use. An oral appliance maintains its structural integrity over a minimum of 3 years.
This definition includes the key design features of effective oral appliances, is evidence based or, in the absence of evidence, is agreed upon using a modified RAND Appropriateness Method process. Its intent is not to replace clinical judgment but instead represents a compilation of the best currently available appliance design features.
5.0 DISCUSSION OF EVIDENCE SUPPORTING THE DEFINITION
5.1 Purpose of an Effective Oral Appliance
The purpose of an oral appliance is to treat obstructive sleep apnea, primary snoring, and associated symptoms. Historically, the most frequently measured outcomes of therapeutic efficacy and effectiveness of OSA treatment have been the apneahypopnea index (AHI) to measure severity of OSA and the Epworth Sleepiness Scale (ESS) to assess daytime somnolence. However, as oral appliance research has matured, measured outcomes have broadened to include effect on cardiovascular function, neurocognitive behavior, and quality of life.
5.1.1 Improvements in respiratory variables and daytime somnolence
The efficacy and effectiveness of oral appliance therapy have been confirmed by several high quality studies, including randomized controlled trials, systematic reviews, and meta-analyses.3,40,43,49-61 These studies have validated, via overnight polysomnography (PSG), the utility of mandibular advancement oral appliances in decreasing the frequency and/or duration of apneas, hypopneas, RERAs and/or snoring events, as well as improving nocturnal oxygenation. The ESS score, as a measure of daytime sleepiness, has been shown to normalize or improve by 2-4 points.55
In one of the earliest reports of a well-conducted study comparing pre- and post-appliance polysomnographic recordings, Yoshida demonstrated that post-treatment AHI was significantly reduced more than 50% of pre-treatment values.62 PSG parameters were not normalized, but these findings demonstrated that oral appliance therapy was capable of significantly improving sleep disordered breathing.
Subsequently, Marklund reported that in 72% of patients with mild to moderate obstructive sleep apnea, AHI was reduced to < 10 and that in the severe group, AHI was significantly reduced from a mean of 53 to a mean of 14.63 Other reports that followed corroborated these early findings and demonstrated longitudinal stability of the improvement in sleep parameters with oral appliances.64-70
In perhaps the largest study to date, Holley and colleagues described results of their retrospective study on a sample of 497 OSA patients with all levels of disease severity who were treated with oral appliance therapy.71 Oral appliance therapy reduced the mean AHI from 30.0 to 8.4, and the ESS improved significantly. A comparison of PSG parameters between oral appliance therapy and CPAP therapy was available for 397 subjects. Oral appliance therapy demonstrated equivalent efficacy relative to CPAP in the mild subjects (p = 0.15) where treatment was successful in reducing AHI < 5 in 76% of the CPAP and 62% of the oral appliance group. In the moderate and severe groups, CPAP was more effective than oral appliances in reducing AHI < 5 (71% vs. 51% in the moderate group and 63% vs. 40% in the severe group). However when the magnitude of reduction in AHI was compared between treatments, the decrease in AHI was significant for only the severe group where CPAP decreased AHI by an additional 5.9 events/hour (p < 0.001). The amount of reduction in AHI by both treatments in the mild and moderate groups differed by less than 2 events/hour and was not statistically significant.
Oral appliances are also intended to manage snoring, and studies that examined respiratory variables often also included snoring in their outcome assessments.72 Some investigations, however, have specifically focused on snoring outcomes and have demonstrated the success of oral appliance therapy in improving this outcome.73-77 In an effort to begin comparing respiratory outcomes of different oral appliance designs, Gauthier evaluated two oral appliances in a cross-over study to judge if they differed in effect on respiratory variables including snoring. Both appliances were equally therapeutic in improving snoring and mild to moderate OSA.73 Stouder examined the effect of an oral appliance on several snoring parameters including frequency of snoring, average and peak loudness, and anatomic site of snoring (palatal flutter or tongue base snoring).77 Snoring frequency, maximum and average loudness, and percent of palatal snoring all significantly decreased with the oral appliance. A decrease in tongue base snoring, although hypothesized, was not observed. On the other hand, the improvement in palatal snoring had not been anticipated, and the investigators speculated that mandibular advancement may have affected all levels of the pharyngeal airway, including the level of the soft palate.
5.1.2 Effect on cardiovascular function
In addition to improvements in respiratory variables and daytime sleepiness, other health sequellae related to sleep disordered breathing that improved with oral appliance therapy included hypertension24,78-83 and cardiovascular function.84,85
The effect of oral appliance therapy on hypertension has been summarized in Iftikhar’s systematic review and meta-analysis of seven observational and randomized controlled trial studies.80 A reduction of approximately 2 mm in systolic, diastolic, and mean arterial pressure was reported among the pooled 399 participants that met the inclusion criteria for these studies. In another study, evaluation of the impact of oral appliance therapy on blood pressure revealed a significant improvement in night time diastolic blood pressure compared to CPAP.78 Lam studied the effect of oral appliance therapy on blood pressure and found significant improvement in systolic blood pressure that was maintained at one-year follow-up.81 Gotsopoulos demonstrated a reduction in 24-hour mean diastolic blood pressure in patients with AHI > 10 and concluded that these findings mirrored those found with CPAP.79 Otsuka reported a significant reduction in mean arterial blood pressure and diastolic blood pressure during monitoring over a 20-hour period, and reported significant reductions in systolic, diastolic, and mean arterial blood pressure during sleep.82
Phillips found no differences between CPAP and oral appliance therapy in 24-hour ambulatory blood pressure profiles. In a subgroup of initially hypertensive subjects, both treatments had equally salutary effects of improving 24-hour blood pressure between 2-4 mm Hg.24 In addition, in this same study, a reduction in arterial stiffness of 1-2% from baseline was noted with no between-treatment differences.24 Likewise in a study comparing the impact of active and sham oral appliances on blood pressure, Andrén demonstrated at 3 months a reduction of 4.4 mm Hg in 24-hour mean systolic blood pressure with the active appliance in a subgroup of subjects with ambulatory daytime mean systolic BP > 135/85 mm Hg and AHI > 15 at baseline.86
In an effort to gain clarity on the effect of oral appliance therapy on markers for risk of development of cardiovascular disease, Itzhaki compared measurements of endothelial function and oxidative stress in 12 patients with a mean AHI of 29.5.85 At 3 months and 1 year follow-up, subsequent to the start of oral appliance therapy, these markers improved to normal or near-normal scores, suggesting that oral appliance therapy was effective in reducing the risk of cardiovascular disease. Hoekema assessed cardiovascular function in untreated moderate to severe OSA patients without cardiovascular disease before and after randomization to either oral appliance therapy or CPAP.84 Using a marker of cardiac impairment from venous blood samples, both treatment groups demonstrated improvement. However, the change was statistically significantly greater in the group treated with oral appliance therapy, suggesting greater improvement in cardiac function relative to patients treated with CPAP. In a controlled cohort study, Anandam examined the impact of oral appliance therapy and CPAP on cardiovascular mortality.87 The incidence of cardiovascular death in severe sleep apnea subjects treated with oral appliance therapy or CPAP was compared to those who refused treatment and healthy controls. The healthy controls had the lowest cardiovascular mortality rate (0.28 per 100 person years) and those who declined treatment had the highest death rate (2.1 per 100 person years). Although the residual AHI for oral appliance treated subjects was significantly higher than for CPAP treated subjects, there was no difference in cardiovascular death rate (0.61, 0.56 per 100 person years) between the two treatment groups. Both oral appliance therapy and CPAP may be equally effective in reducing the risk of fatal cardiovascular events in patients with severe obstructive sleep apnea.87
5.1.3 Impact on quality of life and neurocognitive behavior
Overall quality of life24,88-94 and neurobehavioral outcomes24,88,89,93,95 have been shown to improve with oral appliance therapy. Walker-Engstrom examined three quality of life dimensions (vitality, contentment, and sleep quality) in subjects who were randomized to either uvulopalatopharyngoplasty or oral appliance therapy.94 One year after intervention, both treatment groups demonstrated significant improvements in all three quality of life dimensions. Levendowski included several quality of life instruments in a small study of patients who underwent oral appliance therapy after failing CPAP treatment.89 Statistically significant reductions in sleepiness (76% of subjects) and depression (73% of subjects) were documented as well as improvement in a disease-specific quality of life index (60% of subjects). Saletu designed a study to examine not only respiratory variables but also additional outcomes of oral appliance therapy in a group of patients with all disease levels.93 Active and sham oral appliances were used to compare effects on morning mood, subjective impression of sleep quality, and cognitive and psychophysiological performance. All respiratory variables improved in the active oral appliance group compared to the sham appliance group. In addition, subjects demonstrated significant benefit in sleep quality, morning cognitive performance, fine motor activity, and reaction time.
Hoekema analyzed the effect of CPAP and oral appliances on simulated driving performance in a group of subjects ranging in OSA severity.95 Pre-treatment driving performance was similar between the two groups. After 2 to 3 months of treatment with CPAP or oral appliance therapy, subjects significantly improved equally in their performance on the driving test independent of which treatment was used.
While CPAP has been demonstrated to be more efficacious than oral appliance therapy when AHI was used as the primary outcome measure, when other outcome measures were examined, oral appliance therapy has been demonstrated to be equivalent to CPAP.24,49,54,78,89 In studies of mild to moderate OSA, oral appliances have been no less effective than CPAP for improving PSG parameters, daytime somnolence, quality of life measures, and neurobehavioral function.51,53,54,71,78,88,96,97
In a landmark crossover study of 126 moderate to severe OSA patients, Phillips demonstrated that while CPAP was more efficacious than oral appliance therapy in reducing AHI, no difference was detected when evaluating other health outcomes.24 Outcomes assessed included subjective sleepiness, driving simulator performance, and quality of life. Neurobehavioral outcomes improved similarly in ESS and quality of life with both treatments. However, oral appliance therapy outperformed CPAP on the Short Form (36) in four of eight domains and the overall mental component. Simulated driving performance improved equally in both treatments. At the time of the study, no objective measure of oral appliance adherence was available, but therapy adherence as reported by the subjects was superior to CPAP and may help explain the similar effectiveness of both treatments in neurobehavioral and quality of life outcomes.
5.1.4 Potential to enhance CPAP adherence
Finally, oral appliances may offer ways to improve CPAP compliance or effectiveness. Using phrenic nerve stimulation to assess upper airway dynamic properties, Borel established that concurrent use of nasal CPAP and oral appliances reduced velopharyngeal resistance to a greater extent than nasal CPAP alone.98 When oral appliances were used with nasal CPAP, maximal flow rate was significantly improved.
The simultaneous use of oral appliance therapy with CPAP is a relatively new concept in dental sleep medicine. While preliminary studies are promising, more research is warranted to validate improved effectiveness.
5.2 Physical Features of an Effective Oral Appliance
Oral appliances employ various mechanisms of action to provide a more patent upper airway in order to alleviate signs and symptoms of OSA. Types of appliances include tongue retention devices, non-adjustable and adjustable oral appliances and single arch tongue depressing devices.
5.2.1 Comparison of oral appliance types
Although there is evidence that tongue retention devices can be efficacious and may be the only appliance choice for completely edentulous individuals who do not or cannot have dental implants,50,99 they are usually not as effective as oral appliances due to poor compliance.100 Patients reported that tongue retention devices were not as comfortable as oral appliances100 and determining compliance has been problematic with tongue retention devices. Even if objective compliance measures can ascertain length of time in the mouth, the tongue retention device is only effective if the tongue is maintained in the bulb.101 Presently, there is no commercially available technology to confirm that the tongue is maintained in the bulb during the entire sleep period.
One of the first case series reports of tongue retention device use38 studied 20 subjects with severe OSA, and compared pretreatment and post-treatment data for the tongue retention device to published pre-treatment and post-treatment data for uvulopalatopharyngoplasty (UPPP) and tracheostomy.102,103 Fourteen of the twenty subjects were studied before and after training with the device. Ten of the twenty subjects were studied before use of the device, after training with the device, and for 2 nights after 4-6 months of use. The authors then compared the duration of apneas and the number of apneas per hour of sleep that occurred prior to the use of a tongue retention device, UPPP and tracheostomy to a night with treatment, and found that the post-therapeutic results were similar among all three treatments. In a later randomized study Cartwright found tongue retaining devices provided additional treatment effect when added to positional therapy for some patients.99 Dort compared the outcomes of a tongue retention device to an identical device that was designed not to allow suction to develop on the tongue. In 32 mild OSA patients, only the device capable of developing suction produced significant reductions in the respiratory disturbance index (RDI) and snoring index (snores/hour).104 Deane compared the outcomes of a tongue retention device to a non-adjustable mandibular advancement splint. Although both devices showed a similar reduction in AHI, complete response (AHI < 5/hour) was achieved in 68% of subjects with the mandibular advancement splint and in only 45% of subjects with the tongue retention device. A clinically relevant finding was that compliance was poor with the tongue retention device and 91% of subjects preferred the mandibular advancement splint.100
Non-adjustable appliances that engage both maxillary and mandibular arches have demonstrated efficacy, but the inability to gradually adjust these appliances to increase protrusion without sectioning the appliance make it a less desirable and practical option for many patients.41,50,51,105 The results of studies of non-adjustable appliances are confounded by research methodology that effectively mimics adjustable appliances. In some studies, adjustable appliances were used to find the most effective mandibular position prior to fabrication of the non-adjustable appliances.106,107 In other studies, multiple non-adjustable appliances were fabricated if the initial non-adjustable appliance was uncomfortable108-112 or to obtain an increased treatment effect.113 Rose reported that a non-adjustable appliance was more effective than an adjustable appliance; however, in this study the adjustable appliance was treated as if it were non-adjustable. Both appliances were set at 75% of maximal protrusion and no further titration was undertaken.114 Clinically, non-adjustable appliances are fabricated at a fixed protrusion that remains unchanged for the duration of treatment whereas the protrusive position of adjustable appliances is usually changed to increase treatment effect and patient comfort. Studies that reflect this clinical pathway revealed that the adjustable appliances resulted in greater improvements in the evaluated parameters.58
The only randomized trial that included a soft palate lifter found it had no significant effect on reducing snoring.115 We were unable to identify sufficient peer-reviewed level 1 or level 2 scientific evidence to support the use of single arch appliances for the treatment of OSA and conclude that an effective oral appliance must engage both maxillary and mandibular arches.
Due to the lack of high quality evidence to support the use of tongue retention devices, non-adjustable appliances, and single arch appliances, the definition developed by the consensus conference focused solely on custom-fabricated adjustable oral appliances, as these are the most commonly used in clinical practice and have been shown to have the greatest efficacy.41,50,51,58
5.2.2 Custom versus non-custom oral appliances
Numerous studies have revealed that custom-fabricated oral appliances showed greater efficacy and patient acceptance than non-custom (pre-fabricated) oral appliances.60,116,117 Pre-fabricated oral appliances tend to be bulky and ill-fitting, resulting in difficulties retaining the device on the oral structures.118 This diminishes the ability of the appliance to maintain a stable mandibular protrusive position during sleep and may increase patient discomfort.60 A direct comparison study of a pre-fabricated thermoplastic oral appliance and custom-fabricated oral appliance by Vanderveken in 2008 evaluated whether the non-custom appliance could be a more cost-effective option for the treatment of sleep disordered breathing. The pre-fabricated oral appliance failed to reduce the AHI and had limited success in reducing snoring. This may have been a result of the pre-fabricated appliance not being retained adequately by the teeth or allowing sufficient mandibular protrusion. Additionally, the pre-fabricated appliance had decreased patient acceptance due to discomfort associated with the lack of retention during sleep.117 A custom oral appliance was associated with increased patient comfort, had greater range of protrusive movement, and was more effective.
5.2.3 Protrusion mechanism
Research indicates that the ability to advance the mandible is a key design feature, and that there is a dose dependent impact on AHI reduction and reduction in snoring.41,51,58,60,118,119 Protrusive range of movement varies greatly in individual subjects. The mean protrusive capability has been reported as approximately 11 mm with a range of 6-14 mm.120 The position at which an oral appliance is most effective also varies.51,119-121 Although the most effective protrusion was found to be as little as 25% of maximum in 5% of subjects,122 most studies reported that subjects required protrusion over 50% of maximum.61,88,120,122
The mandibular protrusion mechanism should allow for advancement in increments of 1 mm or less over a minimum of 5 mm.41,60 Smaller increments of advancement can allow for evaluation of subjective parameters, while minimizing potential temporomandibular discomfort.60,114,120,123 Current data support a starting protrusion position of at least 50% of the patient’s protrusive range, but there is no consensus as to whether this is measured from a starting position of maximal intercuspation or the maximally retruded position of the mandible.60,122 A minimum of 5 mm of advancement range in the mechanism allows for greater mandibular protrusion to be attempted without requiring modification of the protrusion mechanism.60
This definition makes no attempt to describe the exact nature of a suitable protrusion mechanism because effective design elements are continuously evolving.41,73,124-126 However, the mechanism should be stable, maintain the therapeutic level of protrusion/provider established position, and the patient or caregiver should be able to verify that the position is maintained to ensure optimal treatment effect. The mechanism should be reversible to allow for changes in the patient’s condition or to manage side effects.120,123 No recommendations regarding vertical adjustment were included in the definition. Vertical adjustability has been a controversial subject in the design of oral appliances. Despite anecdotal reports of patients benefiting from an increased vertical dimension, several studies suggested that increased vertical dimension, measured as inter-incisal distance, resulted in decreased patient acceptance and had no consistent impact on efficacy.41,106,127
5.2.4 Durability
In order to secure FDA clearance, oral appliances must be demonstrated to be safe for intra-oral patient use. Thus the oral appliance must be fabricated using biocompatible materials. Although allowance for extreme circumstances must be made, the consensus of the conference participants was that oral appliances should be expected to maintain structural integrity for a minimum of 3 years of use.5.3 Function of an Effective Oral Appliance
OSA is characterized by repetitive cycles of upper airway collapse with obstruction or limitation of airflow, followed by physiological arousal to restore airway patency in order to sustain life. The most effective oral appliances are mandibular advancement devices that stabilize the lower jaw in a forward and upward position. These devices function by reducing airway compliance and maintaining a patent upper airway during sleep.
Much research has been conducted over the past two decades to determine structural, anatomical and physiological factors that predict which patients with OSA will respond most favorably to oral appliance therapy. Many of these studies were conducted on upright and/or awake patients. Although the prognostic usefulness of these studies in patient selection for therapy has remained questionable, this evidence provides the major source of data bearing on the mechanisms by which mandibular advancement maintains airway patency.
In a systematic review published in 2004, Hoekema described three different plausible mechanisms underlying the efficacy of oral appliances in improving sleep respiration. First, mandibular advancement moves the suprahyoid and genioglossus muscles anteriorally, enlarging the airway, thus lessening the likelihood of its collapse. Second, downward movement of the mandible accompanies advancement, thereby exerting tension across the soft palate via the palatoglossal and palatopharyngeal arches, thereby preserving the velopharyngeal airway space. Third, the oral appliance maintains a forward position of the mandible and hyoid bone during sleep, preventing backward rotation of the jaw and retrolapse of the tongue into the airway.57 Hoffstein in a systematic review of the oral appliance literature concluded more generally that mandibular advancement produces anatomical changes that “result in the alterations of the intrinsic relationships between different muscle groups controlling the upper airway caliber.”34 He noted that these changes could prevent obstruction, worsen obstruction or have no effect on an individual patient basis. Hoffstein also concluded that abnormal anatomy, as well as abnormal physiology, is required for sleep disordered breathing.34
Although many studies have provided some insight into the anatomical or neuromuscular response to an oral appliance during sleep or wakefulness, it is generally accepted that the manner in which an oral appliance functions is incompletely understood and that the mechanisms underlying improved patency during sleep is unlikely the same for all patients with OSA.128-131 For this reason the definition of an oral appliance did not attempt to ascribe any specific mechanism underlying the improvement in airway patency that could be assumed for the patients whose sleep respiration is normalized by therapy. However, review of the literature made it clear that mandibular advancement is the critical feature of an oral appliance supporting its function in maintaining airway patency and that patency varies with the degree of advancement.
5.3.1 Efficacy of oral appliance therapy is dependent on mandibular advancement.
Four systematic reviews described controlled trials in which the efficacy of oral appliances that advance the mandible was compared to that of control devices, which did not advance the mandible.34,40,50,57 Compared to the control devices, the AHI was more effectively lowered by the mandibular advancement appliances.61,132-134 Thus, the presence of an occlusal device between the teeth that variably separated the jaws due to its thickness, but did not advance the mandible, was ineffective in maintaining airway patency during sleep in patients with sleep disordered breathing.
5.3.2 Efficacy of mandibular advancement is dose dependent
Three systematic reviews additionally concluded that efficacy of an oral appliance in normalizing sleep respiration increased with the degree of protrusion.34,40,57 These reviews described studies that demonstrated decreases in the AHI or oxygen desaturations with progressive mandibular advancement that was most commonly performed during the clinical titration of the oral appliance to achieve resolution of symptoms.63,113,114,123,135-138
5.3.3 Studies that support maintained airway patency during sleep
A large number of studies have evaluated anatomical and neuromuscular parameters relevant to airway patency. The strongest studies regarding mechanisms of improved airway patency were those that obtained data from subjects while asleep in a supine position to mimic the natural situation in which OSA occurs most commonly. Many of these studies mimic the natural sleep situation by using controlled anesthesia modalities to achieve nocturnal airway collapsibility. The weakest studies were those that obtained patency-relevant data from subjects while awake in an upright position. The patency of the airway in the upright position during wakefulness was not characteristic of that during natural sleep and the difference was likely greater for patients with OSA than for non-apneic individuals.139-1415.3.4 Physiological evidence in support of maintained airway patency during sleep
A decrease in the frequency and/or duration of apneas, hypopneas, RERAs and/or snoring events, and improved nocturnal oxygenation can only occur if the airway is made more patent. Arguably, the single best measure of airway patency is the highest intraluminal air pressure below which the airway collapses.142 The more negative this pressure, the less likely the airway will collapse in response to the negative pressures generated during inspiration.In a landmark but small study, Kato demonstrated that mandibular advancement with appliances producing 2, 4 and 6 mm of jaw advancement progressively lowered the critical closing pressures from supra- to sub-atmospheric pressures in subjects (n = 4) who responded to the appliances with a significant reduction in nocturnal oxygen desaturations, but not in subjects who continued to exhibit significant oxygen desaturation (n = 2).138 The closing pressure represents the net outcome of all structural, anatomical and physiological factors at the time of its measurement, affecting the integrity of the upper airway. Measurements of the closing pressures were made during drug induced sleep and neuromuscular block in order to characterize the behavior of the completely passive pharynx, void of any reflex response to maintain airway patency. Similar results were obtained using less invasive methods by other teams of investigators. For example, by experimentally occluding nasal airflow during natural sleep, Ng estimated the closing pressure at the point at which nasal air pressure ceased to decrease with continued respiratory effort. The oral appliance not only lowered (by 10-20%) the upper airway closing pressures, but those patients who demonstrated the greatest improvements in airway patency exhibited the greatest improvements in the AHI with use of the oral appliance.143,144 These two small studies suggested that oral appliances do not maintain airway patency by altering the location at which airway occlusion is likely to occur.
5.3.5 Direct anatomical evidence in support of maintained airway patency during sleep
Convincing evidence of improved airway patency has also been obtained by studies employing sleep endoscopy. This procedure has enabled direct observation of a patent airway upon mandibular advancement in sleeping patients who respond favorably to oral appliance therapy. Sleep was typically induced by the intravenous administration of pharmacological agents such as midazolam and/or propofol, that have shown similar effects on the airway as natural non-rapid eye movement (NREM) sleep.145 A flexible thin endoscope (laryngoscope) was inserted through a nostril enabling direct videoscopic imaging of the airway. Vroegop assessed improvements in airway patency of 200 patients with pre-made interocclusal records that captured the jaw position of the individual patient’s maximal comfortable protrusion, a position similar to that anticipated for an oral appliance.146 The level, degree and configuration of airway collapse were compared with and without the simulation bite. The response of the airway to the simulation bite was found to be a significant predictor of a favorable response to oral appliance therapy (i.e., reduction of the AHI ≥ 50% compared to baseline).Other groups have similarly observed improvement in airway patency upon mandibular advancement during sleep endoscopy. Johal and Battagel observed improved airway patency and a reduction of snoring upon advancement of the mandible 4 or 5 mm to mimic the effect of an oral appliance as well as upon placement of an oral appliance on the patients’ teeth.147-149 Consistent with these findings the oral appliance reduced the mean AHI, ESS scale scores, and partner-reported snoring scores.
5.3.6 Radiographic evidence in support of maintained airway patency during sleep
Most radiographic studies have involved analyses of two-dimensional, sagittal images of the skull (lateral cephalographic images) taken at a single time point in upright, awake subjects. However, in a few studies sleep was induced pharmacologically to assess the impact of mandibular advancement on the airway over time in all three dimensions. For example, using ultrafast computed tomography, Choi evaluated the cross-sectional areas of the airway with and without mandibular advancement (67% maximum protrusion).150 At each site, mandibular advancement was found to significantly restore in most subjects some of the loss in cross-sectional area observed upon induction of sleep, effectively maintaining patency of the upper airway. However, for a small number of subjects, no change was observed or there was a reduction in cross-sectional area at one or more levels.
Using a different three dimensional imaging technique, videofluoroscopy, Lee obtained similar results from 76 patients before and after receipt of a customized oral appliance.151,152 Images were obtained during wakefulness, sleep during normal oxygen saturation, and sleep during oxygen desaturation. The oral appliance was found to increase the retropalatal and retrolingual spaces and decrease the length of the soft palate. Upon comparing the changes in patients who were deemed treatment success, widening of the retropalatal space was the primary discriminating observation. This demonstrated that not all airway changes suggestive of improved patency translated to better sleep respiration.
Numerous radiographic studies were conducted on awake patients to elucidate tissue changes upon mandibular advancement that correlate with measures of improved sleep respiration. A limitation in all of these papers is that the pharyngeal muscles actively contract to assist airway patency during wakefulness, particularly in patients with sleep disordered breathing.141 Thus, airway dimensions and physiological responses differ during wakefulness and sleep. Many of the studies employing lateral cephalographic images have concluded that the velopharyngeal area is enlarged to a greater extent than the retroglossal or hypoglossal areas by an oral appliance or mandibular advancement. However, contemporary computed tomography (CT) and magnetic resonance imaging (MRI) of awake patients revealed both increases and decreases in the retroglossal and hypoglossal areas. Moreover, the largest changes in the airway upon insertion of an oral appliance were often observed in the transverse dimension, limiting the interpretation of cephalographic images of the sagittal plane. These disparate findings suggested that the results of imaging studies are, in part, dependent on the methods employed. Thus, radiographic changes (lateral cephalographic, fluoroscopic, computerized tomographic, and magnetic resonant imaging) observed upon jaw advancement in awake patients have not provided to date a reliable means to predict treatment outcomes.
5.3.7 Electrophysiological evidence of maintained airway patency during sleep
Electromyographic recordings of patients with OSA have been compared with and without oral appliances during polysomnography. Yoshida found that activity in the genioglossus, lateral pterygoid, and masseter muscles was higher in sleeping patients when wearing an oral appliance.153 A similar finding was reported by Kurtulmus for the submental and masseter muscles.154 In both studies, the oral appliance significantly reduced the AHI of the patients. These studies suggested that an oral appliance may alter neuromuscular activity in muscles associated with tongue and mandibular protraction and elevation and offer additional support that oral appliances improve airway patency during sleep.6.0 CONCLUSION
The science of dental sleep medicine has greatly expanded in recent years. After an exhaustive review of the literature, only level 1 and level 2 studies were referenced in this paper to support conference recommendations regarding the purpose, physical features, and function of an effective oral appliance. It is important to acknowledge that the definition developed does not represent endorsement of any one practice protocol, nor is it a comprehensive description of all available oral appliance designs. Rather, this definition delineates the best practices related to the essential elements of an effective oral appliance for the treatment of sleep disordered breathing.
Current literature provides robust evidence that custom, adjustable dual-arch mandibular advancement oral appliances are highly efficacious for the treatment of snoring and mild-moderate OSA. Though less efficacious than CPAP for improving AHI in moderate-severe OSA, several recent studies found that oral appliances and CPAP were equally effective at improving daytime somnolence, hypertension, neurocognitive function, quality of life indices, and cardiovascular mortality. Though little objective adherence data is available, numerous crossover studies have demonstrated oral appliance self-reported adherence to be superior to CPAP. There is much work yet to be done. Further comparative study is needed to establish the impact of various available appliance designs on therapeutic success, patient compliance and potential side effects. Only a few publications to date have explored the simultaneous use of oral appliances and CPAP. Preliminary results suggest combination therapy may hold promise for those patients who are insufficiently responsive to a monotherapy.
The function of an oral appliance is to protrude and help stabilize the mandible in order to maintain a patent upper airway during sleep. However, identification of the specific predominant mechanical and physiologic modes of action remains elusive. Most investigations of oral appliance function were limited by small sample size, as well as dependence on primarily upright and/or awake subjects which may not be an accurate reflection of the real world sleep state. Further research into oral appliance physiology in the sleeping, supine sleep apnea patient may help formulate strategies for identifying the best candidates for oral appliance therapy and facilitate development of the next generation of oral appliance design.
It is hoped that the publication of an empiric definition of an oral appliance will improve standardization for future research and produce more comparable results. It is also intended to serve as a useful guide to clinicians when evaluating and selecting oral appliances. We expect the definition will evolve as new information becomes available.
7.0 ACKNOWLEDGMENTS
The consensus conference participants are indebted to the proficient guidance and vital support provided by Sherene Thomas, PhD, Director of Science and Research, Lauren Loeding, MS, Science and Research Project Manager, Randi Prince, AADSM Coordinator, and Jerome Barrett, Executive Director. We would like to acknowledge the foresight of the American Academy of Dental Sleep Medicine for recognizing an unfilled need and for willingly providing the financial and logistical support required. The manuscript authors would particularly like to thank each of the consensus conference participants who leant their valuable time and thoughtful expertise to bring focus to the key elements of the definition of an effective oral appliance.
8.0 REFERENCES
2. American Academy of Sleep Medicine. Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. Sleep 1999;22:667-89.
3. Epstein LJ, Kristo D, Strollo PJ, Jr., et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med 2009;5:263-76.
4. Nieto FJ, Young TB, Lind BK, et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study. Sleep Heart Health Study. JAMA 2000;283:1829-36.
5. Kim HC, Young T, Matthews CG, Weber SM, Woodward AR, Palta M. Sleep-disordered breathing and neuropsychological deficits. A population-based study. Am J Respir Critical Care Med 1997;156:1813-9.
6. Yaffe K, Laffan AM, Harrison SL, et al. Sleep-disordered breathing, hypoxia, and risk of mild cognitive impairment and dementia in older women. JAMA 2011;306:613-9.
7. Harris M, Glozier N, Ratnavadivel R, Grunstein RR. Obstructive sleep apnea and depression. Sleep Med Rev 2009;13:437-44.
8. Ong JC, Gress JL, San Pedro-Salcedo MG, Manber R. Frequency and predictors of obstructive sleep apnea among individuals with major depressive disorder and insomnia. J Psychosom Res 2009;67:135-41.
9. Parthasarathy S, Fitzgerald M, Goodwin JL, Unruh M, Guerra S, Quan SF. Nocturia, sleep-disordered breathing, and cardiovascular morbidity in a community-based cohort. PloS One 2012;7:e30969.
10. George CF. Reduction in motor vehicle collisions following treatment of sleep apnoea with nasal CPAP. Thorax 2001;56:508-12.
11. Tregear S, Reston J, Schoelles K, Phillips B. Obstructive sleep apnea and risk of motor vehicle crash: systematic review and meta-analysis. J Clin Sleep Med 2009;5:573-81.
12. Kohler M, Stradling JR. Mechanisms of vascular damage in obstructive sleep apnea. Nature reviews. Cardiology 2010;7:677-85.
13. Mehra R, Benjamin EJ, Shahar E, et al. Association of nocturnal arrhythmias with sleep-disordered breathing: The Sleep Heart Health Study. Am J Respir Critical Care Med 2006;173:910-6.
14. Goodson BL, Wung SF, Archbold KH. Obstructive sleep apnea hypopnea syndrome and metabolic syndrome: a synergistic cardiovascular risk factor. J Am Acad Nurse Pract 2012;24:695-703.
15. Ip MS, Lam B, Ng MM, Lam WK, Tsang KW, Lam KS. Obstructive sleep apnea is independently associated with insulin resistance. Am J Respir Critical Care Med 2002;165:670-6.
16. Balk EM, Moorthy D, Obadan NO, et al. Comparative Effectiveness Review No. 32. (Prepared by Tufts Evidence-based Practice Center under Contract No. 290-2007-10055-1). AHRQ Publication No. 11-EHC052-EF. Rockville (MD), 2011.
17. Marshall NS, Wong KK, Liu PY, Cullen SR, Knuiman MW, Grunstein RR. Sleep apnea as an independent risk factor for all-cause mortality: the Busselton Health Study. Sleep 2008;31:1079-85.
18. Punjabi NM, Caffo BS, Goodwin JL, et al. Sleep-disordered breathing and mortality: a prospective cohort study. PLoS Med 2009;6:e1000132.
19. Redline S, Yenokyan G, Gottlieb DJ, et al. Obstructive sleep apneahypopnea and incident stroke: the sleep heart health study. Am J Respir Critical Care Med 2010;182:269-77.
20. Shahar E, Whitney CW, Redline S, et al. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J Respir Critical Care Med 2001;163:19-25.
21. Shamsuzzaman AS, Gersh BJ, Somers VK. Obstructive sleep apnea: implications for cardiac and vascular disease. JAMA 2003;290:1906-14.
22. Young T, Finn L, Peppard PE, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep 2008;31:1071-8.
23. Li W, Xiao L, Hu J. The comparison of CPAP and oral appliances in treatment of patients with OSA: a systematic review and meta-analysis. Respir Care 2013;58:1184-95.
24. Phillips CL, Grunstein RR, Darendeliler MA, et al. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea: a randomized controlled trial. Am J Respir Critical Care Med 2013;187:879-87.
25. Tan YK, L’Estrange PR, Luo YM, et al. Mandibular advancement splints and continuous positive airway pressure in patients with obstructive sleep apnoea: a randomized cross-over trial. Eur J Orthod 2002;24:239-49.
26. Sutherland K, Cistulli P. Mandibular advancement splints for the treatment of sleep apnea syndrome. Swiss Med Wkly 2011;141:w13276.
27. Randerath WJ, Verbraecken J, Andreas S, et al. Non-CPAP therapies in obstructive sleep apnoea. Eur Respir J 2011;37:1000-28.
28. Vanderveken OM, Dieltjens M, Wouters K, De Backer WA, Van de Heyning PH, Braem MJ. Objective measurement of compliance during oral appliance therapy for sleep-disordered breathing. Thorax 2013;68:91-6.
29. Chen H, Lowe AA, de Almeida FR, Fleetham JA, Wang B. Threedimensional computer-assisted study model analysis of long-term oralappliance wear. Part 2. Side effects of oral appliances in obstructive sleep apnea patients. Am J Orthod Dentofacial Orthop 2008;134:408-17.
30. de Almeida FR, Lowe AA, Tsuiki S, et al. Long-term compliance and side effects of oral appliances used for the treatment of snoring and obstructive sleep apnea syndrome. J Clin Sleep Med 2005;1:143-52.
31. Doff MH, Finnema KJ, Hoekema A, Wijkstra PJ, de Bont LG, Stegenga B. Long-term oral appliance therapy in obstructive sleep apnea syndrome: a controlled study on dental side effects. Clin Oral Investig 2013;17:475-82.
32. Doff MH, Veldhuis SK, Hoekema A, et al. Long-term oral appliance therapy in obstructive sleep apnea syndrome: a controlled study on temporomandibular side effects. Clin Oral Investig 2012;16:689-97.
33. Martinez-Gomis J, Willaert E, Nogues L, Pascual M, Somoza M, Monasterio C. Five years of sleep apnea treatment with a mandibular advancement device. Side effects and technical complications. Angle Orthod 2010;80:30-6.
34. Hoffstein V. Review of oral appliances for treatment of sleep-disordered breathing. Sleep Breath 2007;11:1-22.
35. FDA. FDA Class II Special Controls Guidance Document: Intraoral Devices for Snoring and/or Obstructive Sleep Apnea; Guidance for Industry and FDA. 2002 [cited September 9, 2013]; Available from: http://www.fda.gov/MedicalDevices/DeviceRegulationandGuidance/ GuidanceDocuments/ucm072728.htm
36. Dental devices; classification for intraoral devices for snoring and/or obstructive sleep apnea. Final rule. Federal Register 2002;67:68510-2.
37. Bulletin de L’Academie de Medecine. In: 2 Janvier 1923. p. 37-41.
38. Cartwright RD, Samelson CF. The effects of a nonsurgical treatment for obstructive sleep apnea. The tongue-retaining device. JAMA 1982;248:705-9.
39. Meyer-Ewert K, Schafer H, Kloss W. Treatment of sleep apnea by mandibular protecting device. In: 7th European Congress of Sleep Research; 1984, 1984. p. A217.
40. Ferguson KA, Cartwright R, Rogers R, Schmidt-Nowara W. Oral appliances for snoring and obstructive sleep apnea: a review. Sleep 2006;29:244-62.
41. Ahrens A, McGrath C, Hagg U. A systematic review of the efficacy of oral appliance design in the management of obstructive sleep apnoea. Eur J Orthod 2011;33:318-24.
42. American Sleep Disorders Association. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances. American Sleep Disorders Association. Sleep 1995;18:511-3.
43. Kushida CA, Morgenthaler TI, Littner MR, et al. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances: an update for 2005. Sleep 2006;29:240-3.
44. AASM/AADSM. Policy Statement on the Diagnosis and Treatment of Obstructive Sleep Apnea. 2012 [cited September 9, 2013]; Available from: http://www.aasmnet.org/resources/pdf/AADSMJointOSApolicy.pdf
45. CMS. Oral Appliances for Obstructive Sleep Apnea (L28603). 2011 [cited September 9, 2013]; Available from: http://www.medicarenhic.com/ dme/medical_review/mr_lcds/mr_lcd_archived/L28603_2011-01-01_ PA_2011-01.pdf
46. CMS. Medicare LCD L28603 Revision OAOSA1. 2012 [cited September 9, 2013]; Available from: http://www.medicarenhic.com/dme/medical_ review/mr_lcds/mr_lcd_current/L28603_2012-07-01_PA_2012-07.pdf
47. Fitch K, Bernstein SJ, Aguilar MD, et al. The RAND/UCLA Appropriateness Method User’s Manual. Santa Monica, CA: RAND, 2001.
48. OCEBM Levels of Evidence Working Group. The Oxford Levels of Evidence 2. [cited September 9, 2013]; Available from: http://www.cebm. net/index.aspx?o=5653
49. Oral appliances for obstructive sleep apnea: an evidence-based analysis. Ontario health technology assessment series 2009;9:1-51.
50. Oral appliances for treatment of snoring and obstructive sleep apnea: a review of clinical effectiveness. CADTH technology overviews 2010;1:e0107.
51. Aarab G, Lobbezoo F, Hamburger HL, Naeije M. Oral appliance therapy versus nasal continuous positive airway pressure in obstructive sleep apnea: a randomized, placebo-controlled trial. Respiration 2011;81:411-9.
52. Bennett LS, Davies RJ, Stradling JR. Oral appliances for the management of snoring and obstructive sleep apnoea. Thorax 1998;53 Suppl 2:S58-64.
53. Ferguson KA, Ono T, Lowe AA, Keenan SP, Fleetham JA. A randomized crossover study of an oral appliance vs nasal-continuous positive airway pressure in the treatment of mild-moderate obstructive sleep apnea. Chest 1996;109:1269-75.
54. Giles TL, Lasserson TJ, Smith BJ, White J, Wright J, Cates CJ. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst Rev 2006:CD001106.
55. Hensley M, Ray C. Sleep apnoea. Clinical Evid 2009;2009.
56. Hoekema A. Efficacy and comorbidity of oral appliances in the treatment of obstructive sleep apnea-hypopnea: a systematic review and preliminary results of a randomized trial. Sleep Breath 2006;10:102-3.
57. Hoekema A, Stegenga B, De Bont LG. Efficacy and co-morbidity of oral appliances in the treatment of obstructive sleep apnea-hypopnea: a systematic review. Crit Rev Oral Biol Med 2004;15:137-55.
58. Lettieri CJ, Paolino N, Eliasson AH, Shah AA, Holley AB. Comparison of adjustable and fixed oral appliances for the treatment of obstructive sleep apnea. J Clin Sleep Med 2011;7:439-45.
59. Lim J, Lasserson TJ, Fleetham J, Wright J. Oral appliances for obstructive sleep apnoea. The Cochrane Database Syst Rev 2006:CD004435.
60. Marklund M, Verbraecken J, Randerath W. Non-CPAP therapies in obstructive sleep apnoea: mandibular advancement device therapy. Eur Respir J 2012;39:1241-7.
61. Mehta A, Qian J, Petocz P, Darendeliler MA, Cistulli PA. A randomized, controlled study of a mandibular advancement splint for obstructive sleep apnea. Am J Respir Critical Care Med 2001;163:1457-61.
62. Yoshida K. Prosthetic therapy for sleep apnea syndrome. J Prosthet Dent 1994;72:296-302.
63. Marklund M, Franklin KA, Sahlin C, Lundgren R. The effect of a mandibular advancement device on apneas and sleep in patients with obstructive sleep apnea. Chest 1998;113:707-13.
64. Aarab G, Lobbezoo F, Heymans MW, Hamburger HL, Naeije M. Longterm follow-up of a randomized controlled trial of oral appliance therapy in obstructive sleep apnea. Respiration 2011;82:162-8.
65. Ferguson KA, Ono T, Lowe AA, al-Majed S, Love LL, Fleetham JA. A shortterm controlled trial of an adjustable oral appliance for the treatment of mild to moderate obstructive sleep apnoea. Thorax 1997;52:362-8.
66. Marklund M, Franklin KA. Long-term effects of mandibular repositioning appliances on symptoms of sleep apnoea. J Sleep Res 2007;16:414-20.
67. Marklund M, Franklin KA, Persson M. Orthodontic side-effects of mandibular advancement devices during treatment of snoring and sleep apnoea. Eur J Orthod 2001;23:135-44.
68. Randerath WJ, Heise M, Hinz R, Ruehle KH. An individually adjustable oral appliance vs continuous positive airway pressure in mild-to-moderate obstructive sleep apnea syndrome. Chest 2002;122:569-75.
69. Tegelberg A, Wilhelmsson B, Walker-Engstrom ML, et al. Effects and adverse events of a dental appliance for treatment of obstructive sleep apnoea. Swed Dent J 1999;23:117-26.
70. Walker-Engstrom ML, Tegelberg A, Wilhelmsson B, Ringqvist I. 4-year follow-up of treatment with dental appliance or uvulopalatopharyngoplasty in patients with obstructive sleep apnea: a randomized study. Chest 2002;121:739-46.
71. Holley AB, Lettieri CJ, Shah AA. Efficacy of an adjustable oral appliance and comparison with continuous positive airway pressure for the treatment of obstructive sleep apnea syndrome. Chest 2011;140:1511-6.
72. O’Sullivan RA, Hillman DR, Mateljan R, Pantin C, Finucane KE. Mandibular advancement splint: an appliance to treat snoring and obstructive sleep apnea. Am J Respir Critical Care Med 1995;151:194-8.
73. Gauthier L, Laberge L, Beaudry M, Laforte M, Rompre PH, Lavigne GJ. Efficacy of two mandibular advancement appliances in the management of snoring and mild-moderate sleep apnea: a cross-over randomized study. Sleep Med 2009;10:329-36.
74. Johnston CD, Gleadhill IC, Cinnamond MJ, Peden WM. Oral appliances for the management of severe snoring: a randomized controlled trial. Eur J Orthod 2001;23:127-34.
75. Maguire J, Steele JG, Gibson GJ, Wilson JA, Steen N, McCracken GI. Randomised cross-over study of oral appliances for snoring. Clin Otolaryngol 2010;35:204-9.
76. Robertson S, Murray M, Young D, Pilley R, Dempster J. A randomized crossover trial of conservative snoring treatments: mandibular repositioning splint and nasal CPAP. Otolaryngol Head Neck Surg 2008;138:283-8.
77. Stouder S, Jones L, Brietzke S, Mair EA. Does an oral appliance reduce palatal flutter and tongue base snoring? Otolaryngol Head Neck Surg 2007;136:827-31.
78. Barnes M, McEvoy RD, Banks S, et al. Efficacy of positive airway pressure and oral appliance in mild to moderate obstructive sleep apnea. Am J Respir Critical Care Med 2004;170:656-64.
79. Gotsopoulos H, Kelly JJ, Cistulli PA. Oral appliance therapy reduces blood pressure in obstructive sleep apnea: a randomized, controlled trial. Sleep 2004;27:934-41.
80. Iftikhar IH, Hays ER, Iverson MA, Magalang UJ, Maas AK. Effect of oral appliances on blood pressure in obstructive sleep apnea: a systematic review and meta-analysis. J Clin Sleep Med 2013;9:165-74.
81. Lam B, Sam K, Lam JC, Lai AY, Lam CL, Ip MS. The efficacy of oral appliances in the treatment of severe obstructive sleep apnea. Sleep Breath 2011;15:195-201.
82. Otsuka R, Ribeiro de Almeida F, Lowe AA, Linden W, Ryan F. The effect of oral appliance therapy on blood pressure in patients with obstructive sleep apnea. Sleep Breath 2006;10:29-36.
83. Yoshida K. Effect on blood pressure of oral appliance therapy for sleep apnea syndrome. Int J Prosthodont 2006;19:61-6.
84. Hoekema A, Voors AA, Wijkstra PJ, et al. Effects of oral appliances and CPAP on the left ventricle and natriuretic peptides. Int J Cardiol 2008;128:232-9.
85. Itzhaki S, Dorchin H, Clark G, Lavie L, Lavie P, Pillar G. The effects of 1-year treatment with a herbst mandibular advancement splint on obstructive sleep apnea, oxidative stress, and endothelial function. Chest 2007;131:740-9.
86. Andren A, Hedberg P, Walker-Engstrom ML, Wahlen P, Tegelberg A. Effects of treatment with oral appliance on 24-h blood pressure in patients with obstructive sleep apnea and hypertension: a randomized clinical trial. Sleep Breath 2013;17:705-12.
87. Anandam A, Patil M, Akinnusi M, Jaoude P, El Solh AA. Cardiovascular mortality in obstructive sleep apnea treated with continuous positive airway pressure or oral appliance: an observational study. Respirology 2013;18:1184-90.
88. Hoekema A, Stegenga B, Wijkstra PJ, van der Hoeven JH, Meinesz AF, de Bont LG. Obstructive sleep apnea therapy. J Dent Res 2008;87:882-7.
89. Levendowski DJ, Morgan TD, Patrickus JE, et al. In-home evaluation of efficacy and titration of a mandibular advancement device for obstructive sleep apnea. Sleep Breath 2007;11:139-47.
90. Machado MA, Prado LB, Carvalho LB, et al. Quality of life of patients with obstructive sleep apnea syndrome treated with an intraoral mandibular repositioner. Arq Neuropsiquiatr 2004;62:222-5.
91. Naismith SL, Winter VR, Hickie IB, Cistulli PA. Effect of oral appliance therapy on neurobehavioral functioning in obstructive sleep apnea: a randomized controlled trial. J Clin Sleep Med 2005;1:374-80.
92. Rose EC, Barthlen GM, Staats R, Jonas IE. Therapeutic efficacy of an oral appliance in the treatment of obstructive sleep apnea: a 2-year follow-up. Am J Orthod Dentofacial Orthop 2002;121:273-9.
93. Saletu A, Anderer P, Parapatics S, Matthai C, Matejka M, Saletu B. Effects of a mandibular repositioning appliance on sleep structure, morning behavior and clinical symptomatology in patients with snoring and sleepdisordered breathing. Neuropsychobiology 2007;55:184-93.
94. Walker-Engstrom ML, Wilhelmsson B, Tegelberg A, Dimenas E, Ringqvist I. Quality of life assessment of treatment with dental appliance or UPPP in patients with mild to moderate obstructive sleep apnoea. A prospective randomized 1-year follow-up study. J Sleep Res 2000;9:303-8.
95. Hoekema A, Stegenga B, Bakker M, et al. Simulated driving in obstructive sleep apnoea-hypopnoea; effects of oral appliances and continuous positive airway pressure. Sleep Breath 2007;11:129-38.
96. Clark GT, Blumenfeld I, Yoffe N, Peled E, Lavie P. A crossover study comparing the efficacy of continuous positive airway pressure with anterior mandibular positioning devices on patients with obstructive sleep apnea. Chest 1996;109:1477-83.
97. Engleman HM, McDonald JP, Graham D, et al. Randomized crossover trial of two treatments for sleep apnea/hypopnea syndrome: continuous positive airway pressure and mandibular repositioning splint. Am J Respir Critical Care Med 2002;166:855-9.
98. Borel JC, Gakwaya S, Masse JF, Melo-Silva CA, Series F. Impact of CPAP interface and mandibular advancement device on upper airway mechanical properties assessed with phrenic nerve stimulation in sleep apnea patients. Respir Physiol Neurobiol 2012;183:170-6.
99. Cartwright R, Ristanovic R, Diaz F, Caldarelli D, Alder G. A comparative study of treatments for positional sleep apnea. Sleep 1991;14:546-52.
100. Deane SA, Cistulli PA, Ng AT, Zeng B, Petocz P, Darendeliler MA. Comparison of mandibular advancement splint and tongue stabilizing device in obstructive sleep apnea: a randomized controlled trial. Sleep 2009;32:648-53.
101. Ono T, Lowe AA, Ferguson KA, Fleetham JA. A tongue retaining device and sleep-state genioglossus muscle activity in patients with obstructive sleep apnea. Angle Orthod 1996;66:273-80.
102. Fujita S, Conway W, Zorick F, Roth T. Surgical correction of anatomic azbnormalities in obstructive sleep apnea syndrome: uvulopalatopharyngoplasty. Otolaryngol Head Neck Surg 1981;89:923-34.
103. Weitzman ED, Kahn E, Pollak CP. Quantitative analysis of sleep and sleep apnea before and after tracheostomy in patients with the hypersomniasleep apnea syndrome. Sleep 1980;3:407-23.
104. Dort L, Brant R. A randomized, controlled, crossover study of a noncustomized tongue retaining device for sleep disordered breathing. Sleep Breath 2008;12:369-73.
105. Blanco J, Zamarron C, Abeleira Pazos MT, Lamela C, Suarez Quintanilla D. Prospective evaluation of an oral appliance in the treatment of obstructive sleep apnea syndrome. Sleep Breath 2005;9:20-5.
106. Pitsis AJ, Darendeliler MA, Gotsopoulos H, Petocz P, Cistulli PA. Effect of vertical dimension on efficacy of oral appliance therapy in obstructive sleep apnea. Am J Respir Critical Care Med 2002;166:860-4.
107. Zhou J, Liu YH. A randomised titrated crossover study comparing two oral appliances in the treatment for mild to moderate obstructive sleep apnoea/hypopnoea syndrome. J Oral Rehabil 2012;39:914-22.
108. Bloch KE, Iseli A, Zhang JN, et al. A randomized, controlled crossover trial of two oral appliances for sleep apnea treatment. Am J Respir Critical Care Med 2000;162:246-51.
109. Lam B, Sam K, Mok WY, et al. Randomised study of three non-surgical treatments in mild to moderate obstructive sleep apnoea. Thorax 2007;62:354-9.
110. Marklund M, Legrell PE. An orthodontic oral appliance. Angle Orthod 2010;80:1116-21.
111. Marklund M, Stenlund H, Franklin KA. Mandibular advancement devices in 630 men and women with obstructive sleep apnea and snoring: tolerability and predictors of treatment success. Chest 2004;125:1270-8.
112. Petri N, Svanholt P, Solow B, Wildschiodtz G, Winkel P. Mandibular advancement appliance for obstructive sleep apnoea: results of a randomised placebo controlled trial using parallel group design. J Sleep Res 2008;17:221-9.
113. Walker-Engstrom ML, Ringqvist I, Vestling O, Wilhelmsson B, Tegelberg A. A prospective randomized study comparing two different degrees of mandibular advancement with a dental appliance in treatment of severe obstructive sleep apnea. Sleep Breath 2003;7:119-30.
114. Rose E, Staats R, Virchow C, Jonas IE. A comparative study of two mandibular advancement appliances for the treatment of obstructive sleep apnoea. Eur J Orthod 2002;24:191-8.
115. Marklund M, Franklin KA. Dental appliances in the treatment of snoring. A comparison between an activator, a soft-palate lifter, and a mouthshield. Swed Dent J 1996;20:183-8.
116. Ahrens A, McGrath C, Hagg U. Subjective efficacy of oral appliance design features in the management of obstructive sleep apnea: a systematic review. Am J Orthod Dentofacial Orthop 2010;138:559-76.
117. Vanderveken OM, Devolder A, Marklund M, et al. Comparison of a custom-made and a thermoplastic oral appliance for the treatment of mild sleep apnea. Am J Respir Critical Care Med 2008;178:197-202.
118. Cooke ME, Battagel JM. A thermoplastic mandibular advancement device for the management of non-apnoeic snoring: a randomized controlled trial. Eur J Orthod 2006;28:327-38.
119. Gagnadoux F, Fleury B, Vielle B, et al. Titrated mandibular advancement versus positive airway pressure for sleep apnoea. Eur Respir J 2009;34:914- 20.
120. Campbell AJ, Reynolds G, Trengrove H, Neill AM. Mandibular advancement splint titration in obstructive sleep apnoea. Sleep Breath 2009;13:157-62.
121. Tegelberg A, Walker-Engstrom ML, Vestling O, Wilhelmsson B. Two different degrees of mandibular advancement with a dental appliance in treatment of patients with mild to moderate obstructive sleep apnea. Acta Odontol Scand 2003;61:356-62.
122. Aarab G, Lobbezoo F, Hamburger HL, Naeije M. Effects of an oral appliance with different mandibular protrusion positions at a constant vertical dimension on obstructive sleep apnea. Clin Oral Investig 2010;14:339-45.
123. Fleury B, Rakotonanahary D, Petelle B, et al. Mandibular advancement titration for obstructive sleep apnea: optimization of the procedure by combining clinical and oximetric parameters. Chest 2004;125:1761-7.
124. Gauthier L, Laberge L, Beaudry M, Laforte M, Rompre PH, Lavigne GJ. Mandibular advancement appliances remain effective in lowering respiratory disturbance index for 2.5-4.5 years. Sleep Med 2011;12:844-9.
125. Ghazal A, Sorichter S, Jonas I, Rose EC. A randomized prospective longterm study of two oral appliances for sleep apnoea treatment. J Sleep Res 2009;18:321-8.
126. Lawton HM, Battagel JM, Kotecha B. A comparison of the Twin Block and Herbst mandibular advancement splints in the treatment of patients with obstructive sleep apnoea: a prospective study. Eur J Orthod 2005;27:82-90.
127. Nikolopoulou M, Naeije M, Aarab G, Hamburger HL, Visscher CM, Lobbezoo F. The effect of raising the bite without mandibular protrusion on obstructive sleep apnoea. J Oral Rehabil 2011;38:643-7.
128. Gale DJ, Sawyer RH, Woodcock A, Stone P, Thompson R, O’Brien K. Do oral appliances enlarge the airway in patients with obstructive sleep apnoea? A prospective computerized tomographic study. Eur J Orthod 2000;22:159-68.
129. L’Estrange PR, Battagel JM, Harkness B, Spratley MH, Nolan PJ, Jorgensen GI. A method of studying adaptive changes of the oropharynx to variation in mandibular position in patients with obstructive sleep apnoea. J Oral Rehabil 1996;23:699-711.
130. Sam K, Lam B, Ooi CG, Cooke M, Ip MS. Effect of a non-adjustable oral appliance on upper airway morphology in obstructive sleep apnoea. Respir Med 2006;100:897-902.
131. Woodson BT, Feroah T, Connolly LA, Toohill RJ. A method to evaluate upper airway mechanics following intervention in snorers. Am J Otolaryngol 1997;18:306-14.
132. Gotsopoulos H, Chen C, Qian J, Cistulli PA. Oral appliance therapy improves symptoms in obstructive sleep apnea: a randomized, controlled trial. Am J Respir Critical Care Med 2002;166:743-8.
133. Hans MG, Nelson S, Luks VG, Lorkovich P, Baek SJ. Comparison of two dental devices for treatment of obstructive sleep apnea syndrome (OSAS). Am J Orthod Dentofacial Orthop 1997;111:562-70.
134. Johnston CD, Gleadhill IC, Cinnamond MJ, Gabbey J, Burden DJ. Mandibular advancement appliances and obstructive sleep apnoea: a randomized clinical trial. Eur J Orthod 2002;24:251-62.
135. de Almeida FR, Bittencourt LR, de Almeida CI, Tsuiki S, Lowe AA, Tufik S. Effects of mandibular posture on obstructive sleep apnea severity and the temporomandibular joint in patients fitted with an oral appliance. Sleep 2002;25:507-13.
136. Esaki K, Kanegae H, Uchida T, Mizuma H, Sakamoto T, Kameyama T. Treatment of sleep apnea with a new separated type of dental appliance (mandibular advancing positioner). Kurume Med J 1997;44:315-9.
137. Gindre L, Gagnadoux F, Meslier N, Gustin JM, Racineux JL. Mandibular advancement for obstructive sleep apnea: dose effect on apnea, long-term use and tolerance. Respiration 2008;76:386-92.
138. Kato J, Isono S, Tanaka A, et al. Dose-dependent effects of mandibular advancement on pharyngeal mechanics and nocturnal oxygenation in patients with sleep-disordered breathing. Chest 2000;117:1065-72.
139. Fransson AM, Svenson BA, Isacsson G. The effect of posture and a mandibular protruding device on pharyngeal dimensions: a cephalometric study. Sleep Breath 2002;6:55-68.
140. Johal A, Sheriteh Z, Battagel J, Marshall C. The use of videofluoroscopy in the assessment of the pharyngeal airway in obstructive sleep apnoea. Eur J Orthod 2011;33:212-9.
141. Mezzanotte WS, Tangel DJ, White DP. Waking genioglossal electromyogram in sleep apnea patients versus normal controls (a neuromuscular compensatory mechanism). J Clinical Invest 1992;89:1571-9.
142. Dempsey JA, Veasey SC, Morgan BJ, O’Donnell CP. Pathophysiology of sleep apnea. Physiol Rev 2010;90:47-112.
143. Ng AT, Gotsopoulos H, Qian J, Cistulli PA. Effect of oral appliance therapy on upper airway collapsibility in obstructive sleep apnea. Am J Respir Critical Care Med 2003;168:238-41.
144. Ng AT, Qian J, Cistulli PA. Oropharyngeal collapse predicts treatment response with oral appliance therapy in obstructive sleep apnea. Sleep 2006;29:666-71.
145. Morrison DL, Launois SH, Isono S, Feroah TR, Whitelaw WA, Remmers JE. Pharyngeal narrowing and closing pressures in patients with obstructive sleep apnea. Am Rev Respir Dis 1993;148:606-11.
146. Vroegop AV, Vanderveken OM, Van de Heyning PH, Braem MJ. Effects of vertical opening on pharyngeal dimensions in patients with obstructive sleep apnoea. Sleep Med 2012;13:314-6.
147. Battagel JM, Johal A, Kotecha BT. Sleep nasendoscopy as a predictor of treatment success in snorers using mandibular advancement splints. J Laryngol Otol 2005;119:106-12.
148. Johal A, Battagel JM, Kotecha BT. Sleep nasendoscopy: a diagnostic tool for predicting treatment success with mandibular advancement splints in obstructive sleep apnoea. Eur J Orthod 2005;27:607-14.
149. Johal A, Hector MP, Battagel JM, Kotecha BT. Impact of sleep nasendoscopy on the outcome of mandibular advancement splint therapy in subjects with sleep-related breathing disorders. J Laryngol Otol 2007;121:668-75.
150. Choi JK, Hur YK, Lee JM, Clark GT. Effects of mandibular advancement on upper airway dimension and collapsibility in patients with obstructive sleep apnea using dynamic upper airway imaging during sleep. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109:712-9.
151. Lee CH, Kim JW, Lee HJ, et al. Determinants of treatment outcome after use of the mandibular advancement device in patients with obstructive sleep apnea. Arch Otolaryngol Head Neck Surg 2010;136:677-81.
152. Lee CH, Kim JW, Lee HJ, et al. An investigation of upper airway changes associated with mandibular advancement device using sleep videofluoroscopy in patients with obstructive sleep apnea. Arch Otolaryngol Head Neck Surg 2009;135:910-4.
153. Yoshida K. Effect of a prosthetic appliance for treatment of sleep apnea syndrome on masticatory and tongue muscle activity. J Prosthet Dent 1998;79:537-44.
154. Kurtulmus H, Cotert S, Bilgen C, On AY, Boyacioglu H. The effect of a mandibular advancement splint on electromyographic activity of the submental and masseter muscles in patients with obstructive sleep apnea. Int J Prosthodont 2009;22:586-93.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication October, 2013
Accepted for publication October, 2013
Address correspondence to: American Academy of Dental Sleep Medicine, 2510 N. Frontage Road, Darien, IL 60561; Tel: (630) 737-9705.
DISCLOSURE STATEMENT
This was not an industry supported study. The authors have indicated no financial conflicts of interest.
PDF