Special Article 1, Issue 10.4
Associations between Tooth Wear and Dental Sleep Disorders, a Narrative Overview
http://dx.doi.org/10.15331/jdsm.7310P. Wetselaar¹, D. Manfredini², J.Ahlberg³, A. Johansson, G. Aarab¹, C. E. Papagianni¹, M. Reyes Sevilla¹, M. Koutris¹, F. Lobbezoo¹
¹Department of Orofacial Pain and Dysfunction, Academic Centre for Dentistry Amsterdam (ACTA), University of Amsterdam and Vrije Universiteit Amsterdam, Amsterdam, The Netherlands; ²School of Dentistry, University of Padova, Padova, Italy; ³Dept. of Oral and Maxillofacial Diseases, Faculty of Medicine, University of Helsinki, Helsinki, Finland; Dept. of Clinical Dentistry-Prosthodontics, Faculty of Medicine, University of Bergen, Bergen, Norway
ABSTRACT
Objectives:
Tooth wear is a common finding in adult patients with dental sleep disorders. The aim of this paper was to review the literature on the possible associations between tooth wear and the following dental sleep disorders: sleep-related orofacial pain , oral moistening disorders, gastro-esophageal reflux disease (GERD), obstructive sleep apnea syndrome (OSAS), and sleep bruxism.
Methods:
A PubMed search was performed on June 1, 2018, using MeSH terms in the following query: Tooth Wear AND (Facial Pain OR Temporomandibular Joint Disorders OR Xerostomia OR Sialorrhea OR Gastroesophageal Reflux OR Sleep Apnea Syndrome OR Sleep Bruxism).
Results:
The query yielded 706 reports on tooth wear and the mentioned dental sleep disorders. Several associations between tooth wear and the dental sleep disorders were suggested in the literature. It could be concluded that: 1. tooth wear is associated with dental pain and/or hypersensitivity; 2. oral dryness is associated with tooth wear, orofacial pain, and sleep bruxism; 3. GERD is associated with tooth wear, orofacial pain, oral dryness, OSAS, and sleep bruxism; 4. OSAS is associated with oral dryness, GERD, and sleep bruxism; and 5. sleep bruxism is associated with tooth wear.
Conclusions:
Tooth wear is associated with the dental sleep disorders orofacial pain, oral dryness, GERD, and sleep bruxism. The dental sleep disorders are interlinked with each other, which leads to indirect associations as well, and makes the consequences of each single condition difficult to disentangle. Knowledge of these associations is clinically relevant, but more research is needed to confirm their validity.
Keywords:
tooth wear, orofacial pain, oral moistening disorders, xerostomia, hyposalivation, hypersalivation, sialorrhea, ptyalism, gastroesophageal reflux disease, sleep apnea, sleep bruxism, adult
Citation:
P. Wetselaar¹, D. Manfredini², J.Ahlberg³, A. Johansson, G. Aarab¹, C. E. Papagianni¹, M. Reyes Sevilla¹, M. Koutris¹, F. Lobbezoo¹
Reprinted with permission.
This is an open access article under the terms of the Creative Commons Attribution-NonCommercialNoDerivs License, which permits use and distribution in any medium, provided the original work is properly cited, the use is noncommercial and no modifications or adaptations are made.
© 2019 Journal of Oral Rehabilitation Published by John Wiley & Sons Ltd
INTRODUCTION
Tooth wear is a multifactorial condition, leading to the loss of dental hard tissues, viz., enamel, dentine and cementum (1). Based on the purported etiology, tooth wear can be mechanical or chemical (both intrinsic and extrinsic). Intrinsic mechanical wear (known as attrition) is a result of chewing and/or bruxism (e.g., grinding), due to tooth-to-tooth contact, whilst extrinsic mechanical wear (known as abrasion) is a result of other factors than chewing and/or bruxism, e.g., oral hygiene procedures and habits like nail- or pen-biting. Intrinsic and extrinsic chemical wear, both known as dental erosion, are the result of gastric acid and an acidic diet or environments containing airborne acid, respectively (2). Intrinsic mechanical tooth wear is a physiological process, as the dentition is “designed” for function (chewing). Additionally, when the other wear mechanisms are involved, it can become pathological. It should be noted that single wear mechanisms rarely act alone, but interact with each other (1). There is evidence that an acidic diet plays an increasingly important role in the multifactorial condition tooth wear (3). This is also a common believe amongst dental clinicians, nevertheless, having knowledge of the whole etiological spectrum is of utmost importance.
Regarding the diagnosis of tooth wear, a comprehensive approach is necessary due to its multifactorial origin and manifestation. Recently, the Tooth Wear Evaluation System (TWES), was described to implement a systematic approach to the diagnosis (qualification and quantification) and management of the condition (2). The diagnosis tooth wear is not difficult, being simply the loss of dental hard tissues that is easy to differentiate from dental caries or trauma. However, to distinguish between the different sub-forms (i.e., qualification) is very difficult. Regarding the qualification of tooth wear, there is no consensus at this time, although several proposals exist (2, 4, 5). No difference in reliability between setting the diagnosis of chemical or mechanical tooth wear can be hypothesized. In all the studies mentioned in this overview, it was not always clear how the diagnosis was set. Regarding the quantification of tooth wear, the existing situation is even worse: more than one hundred different evaluation systems exists (6.) Comparison of the most commonly used systems nevertheless reveal that a universally accepted modular evaluation system is a possibility and a necessity (6). Taking these considerations into account, it is clear that comparison of tooth wear research findings is difficult. It will take time before the dental community will reach consensus on this topic (see also Table 2).
According to literature, the prevalence of severe tooth wear in adults increases from 3% at the age of 20 years to 17% at the age of 70 years (7). The prevalence of tooth wear is increasing, although data are scarce and contradictory (8, 9). Physiological tooth wear is a slow process that does normally not lead to any subjective symptoms, but when it becomes pathological, dental hypersensitivity and/or dental pain (being a form of orofacial pain) may occur (10). Additionally, pathological tooth wear can result in difficulties with chewing/eating; impaired orofacial esthetics because of loss of dental hard tissue; crumbling off dental hard tissue; and deterioration of dental restorations (2, 10).
Tooth wear is irreversible, which may require repeated and increasingly complex and expensive restorations (10). Therefore, it is important that the diagnosis of tooth wear is made early, and adequate preventive measures are undertaken in order to prevent as much as possible the loss of dental hard tissue (10, 11).
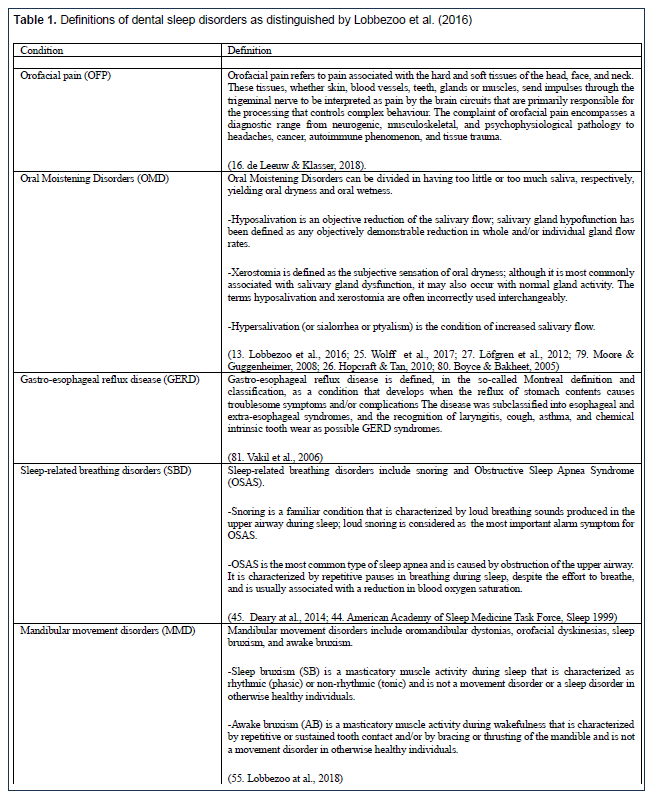
Not only tooth wear is becoming increasingly significant in the management of the long-term health of the dentition (11), but dentists are also becoming more involved with patients requesting information or needing management of oral and dental conditions in relation to dental sleep disorders (12). At this moment, dental sleep medicine is not yet recognised in the general medical literature, nor in the dental literature, although these terms were introduced already two decades ago (12). We do think, however, that we are at a turning point, as was mentioned in a recent review, in which a new definition of Dental Sleep Medicine was proposed (13): “Dental Sleep Medicine is the discipline concerned with the study of the oral and maxillofacial causes and consequences of sleep-related problems”. In our opinion the term Dental Sleep Medicine is an appropriate one, although debate continues. We do realize that other choices regarding definitions and terminology are possible. Importantly, however, the dental profession ultimately must make a definitive choice, in order to enable speaking the same language, using identically definitions and terms. The sleep-related problems to which the proposed definition of Dental Sleep Medicine refers, are: orofacial pain; oral moistening disorders (both oral dryness and oral wetness; in this narrative overview, we focus on oral dryness); gastro-esophageal reflux disorder (GERD); sleep-related breathing disorders (including snoring and obstructive sleep apnea, OSAS; in this narrative overview, we focus on OSAS); and mandibular movement disorders (including dyskinesia, dystonia, and sleep bruxism; in this narrative overview, we focus on sleep bruxism). Some peer-reviewed journals in the field allowed us to introduce the above concepts (14, 15). For descriptions/definitions of these conditions, see Table 1.
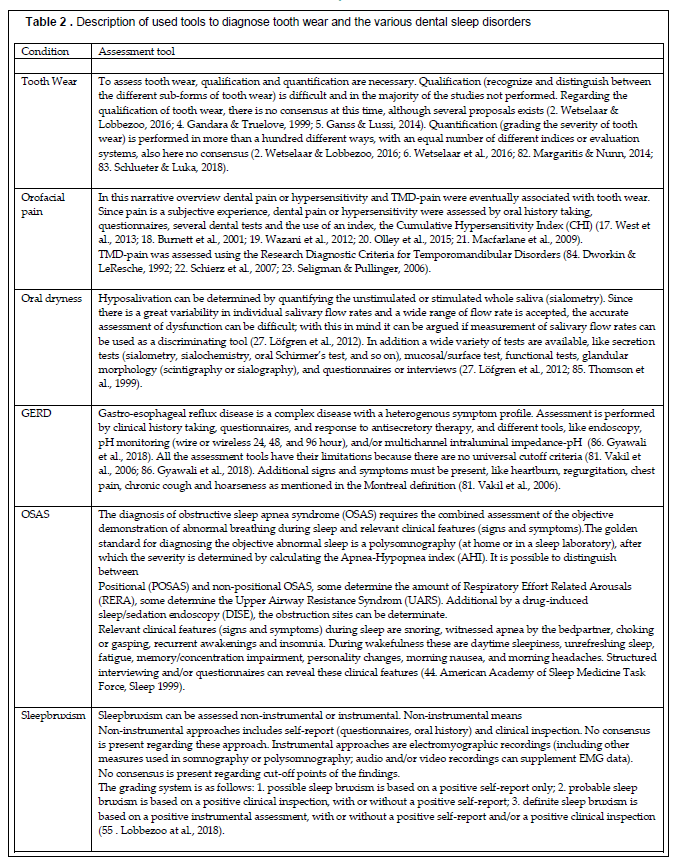
As in the case of the evaluation of tooth wear, also regarding the assessment of the dental sleep disorders, a wide variety of tools are used (see Table 2). For these reasons, it is hard to organize the available material into a qualitative systematic literature review. A narrative overview was instead performed in the attempt to summarize the available knowledge.
The aim of this paper was to review the literature on the possible associations between tooth wear (both mechanical and chemical) and dental sleep disorders (viz., orofacial pain, oral dryness, GERD, OSAS, and sleep bruxism), as well as the mutual associations between these disorders themselves. There is evidence that the mentioned dental sleep disorders do have an association with tooth wear, realizing that tooth wear is not the only sign or symptom of these disorders. By searching the available literature thoroughly, we update the existing knowledge and can probably set future research questions. The results can support dental clinicians to have a better comprehension of the possible etiological factors of tooth wear in their patients, and thus improve the provided dental care.
METHODS
On June 1, 2018, the biomedical literature was searched in PubMed (US National Library of Medicine), using Mesh-Terms in the following query: Tooth Wear AND (Facial Pain OR Temporomandibular Joint Disorders OR Xerostomia OR Sialorrhea OR Gastroesophageal Reflux OR Sleep Apnea Syndrome OR Sleep Bruxism). The MeSH-term Tooth Wear includes Tooth Attrition, Tooth Abrasion and Tooth Erosion; The MeSH-term Facial Pain includes Toothache (dental pain and/or hypersensitivity); the MeSH-term Temporomandibular Joint Disorders includes Temporomandibular Joint Dysfunction Syndrome; the MeSH-term Sleep Apnea Syndrome includes OSAS. We have chosen to use MeSH-terms in order to select only those articles that focus on our research aim. The titles and (when available) the abstracts of the publications were screened to establish whether the publications could shed light on the research aim. In addition, it was examined if a direct association and/or an indirect association (meaning through another dental sleep disorder) was present between tooth wear and a sleep disorder. For all studies, the main inclusion criterion for retrieval of the full text was that the study related to the research question about associations between tooth wear, orofacial pain, oral dryness, GERD, OSAS, and/or sleep bruxism. To be included, the study had to describe the results of an original research in adults, had an appropriate study design, or included a review of one of the subtopics of this study. In order to avoid missing relevant literature, as a search expansion strategy, the reference lists of the full-text articles were hand-searched for additional studies. Publications were excluded for reasons like describing single cases, rare disorders, syndromes, subgroups of patients, restorative treatment procedures, or articles written in languages other than English or Dutch. The search resulted in 706 publications, of which 101 were included in this narrative review. Because of the heterogeneity in the design and quality of the studies, only a narrative approach was possible (see also Table 2)
Associations between Tooth Wear and Dental Sleep Disorders
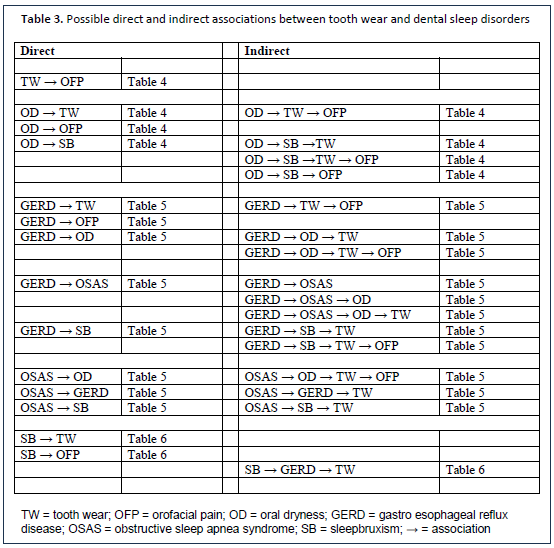
The possible associations (both direct and indirect) between tooth wear and orofacial pain, oral dryness, GERD, OSAS, and sleep bruxism are presented in Table 3.
Orofacial pain and tooth wear
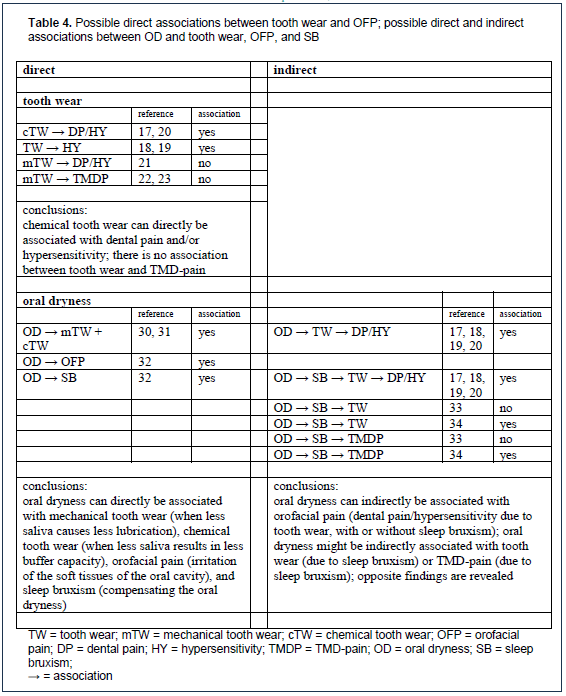
Orofacial pain is a multifactorial condition, with a prevalence of around 5.3% to 22% (16). Amongst the 706 publications, only 7 described the association between tooth wear and orofacial pain (17, 18, 19, 20, 21, 22, 23). The publications did not distinguish orofacial pain during wakefulness or sleep. Concerning the association between tooth wear and dental pain/hypersensitivity, at first sight, contradictory findings were reported (see Table 4). When looking into detail, one can conclude that the conflicting reports can be explained by the fact that tooth wear is used as an umbrella term. When tooth wear is differentiated between chemical wear and mechanical wear, one can conclude that chemical wear can cause orofacial pain (dental pain/hypersensitivity), while mechanical wear does not cause orofacial pain (dental pain/hypersensitivity). Regarding tooth wear and TMD-pain, Schierz and coworkers demonstrated an odds ratio of 1.11, concluding that there was no statistically significant or clinically relevant relationship between tooth wear and the risk of TMD pain (22). Although others (23) stated that multifactorial models using mechanical tooth wear severity and rates may differentiate masticatory muscle pain patients from asymptomatic controls, they commented that these models cannot determine causation or whether any of the differentiating mechanical tooth wear is secondary to TMD pain (23). Based on this available evidence, one may conclude that chemical tooth wear is directly associated with dental pain and/or hypersensitivity (most probably in young patients, when the tooth wear process develops fast) and not with TMD-pain. No publications were found in relation to other orofacial pains, like neuropathic pain or headache.
Oral Moistening Disorders and tooth wear
With the umbrella term oral moistening disorders, we cover all the disorders that have to do with an abnormal quantity or composition of the saliva, so both oral dryness (with the already longer existing terms hyposalivation and xerostomia) and oral wetness (with the already longer existing terms hypersalivation, sialorrhea, and ptyalism). It is not our intention to replace these terms with the umbrella term, nevertheless the umbrella term is in our opinion a useful one, and will only exist in addition to the familiar terms. Saliva is of paramount importance for the maintenance of oral health, and therefore in-depth knowledge amongst healthcare professionals is of great importance. Oral dryness is a multifactorial condition, with a prevalence that varies from 10% to 80% (24). Oral dryness can be physiological, and is related to age, gender, body weight, and the time of the day (24). Oral dryness can be caused by salivary gland hypofunction, thus an objectively measured decrease in salivation, hyposalivation (24, 25, 26, 27). Oral dryness can also be the subjective “feeling” of a dry mouth, xerostomia (26) or the subjective “sensation” of dry mouth, which is often (but not always) associated with hypofunction of the salivary glands” (25). In general, the pathological condition that most frequently causes oral dryness is the use of certain medications: more than a thousand drugs are denoted as xerogenic in the medical literature (25). Other pathological factors resulting in oral dryness are radiotherapy to the head and neck, and systematic disorders, like auto-immune diseases (e.g., Sjögren’s syndrome), diabetes, depression, anxiety, stress, or malnutrition (24, 26). Oral dryness upon awakening is considered a possible symptom of OSAS (28), a lower salivary secretion is seen in GERD patients (29). Oral wetness is also a multifactorial condition, for which prevalence rates at the general population level are not available. It can be physiological during tooth eruption, during the first half of pregnancy, during menstruation, as well as in association with smell and mechanical stimuli (such as mastication) and taste stimuli (24). The pathological causes of hypersalivation include those of: oral origin, such as the first stages of wearing dentures, dental pain, or any irritation or inflammatory process in the oral-pharyngeal or digestive regions (e.g., GERD); neurological disorders, such as Parkinson’s disease, epilepsy, encephalitis, or certain tumors; exogenous poisoning; several medications; and several serious infectious diseases (24). Amongst the included papers, none of them reported an association between oral wetness and tooth wear. Two reviews revealed a possible direct association between oral dryness and tooth wear, namely with mechanical tooth wear (when less saliva causes less lubrication) and chemical tooth wear (when less saliva results in less buffer capacity) (30, 31) (Table 4). Other direct associations were oral dryness with orofacial pain (causing irritation of the soft tissues of the oral cavity; 32), and sleep bruxism (compensating the oral dryness; 32). Oral dryness is indirectly associated with orofacial pain (dental pain/hypersensitivity through tooth wear, see above; regarding the indirect association between oral dryness and temporomandibular pain (through sleep bruxism), and tooth wear (through sleep bruxism), opposite findings revealed (33, 34).
Gastroesophageal reflux disease (GERD) and tooth wear
The prevalence of GERD is high in the Western world, ranging from 10% to 40% (35). The prevalence increases with age and BMI, and men are more frequently affected than women (35). GERD can be considered physiological when occurring after a meal without further complaints and during pregnancy. It becomes pathological when a mechanical impairment of the esophagogastric junction is present and complaints develop (35). GERD is considered as a multifactorial disease; instigating factors are obesity, age, and trauma.
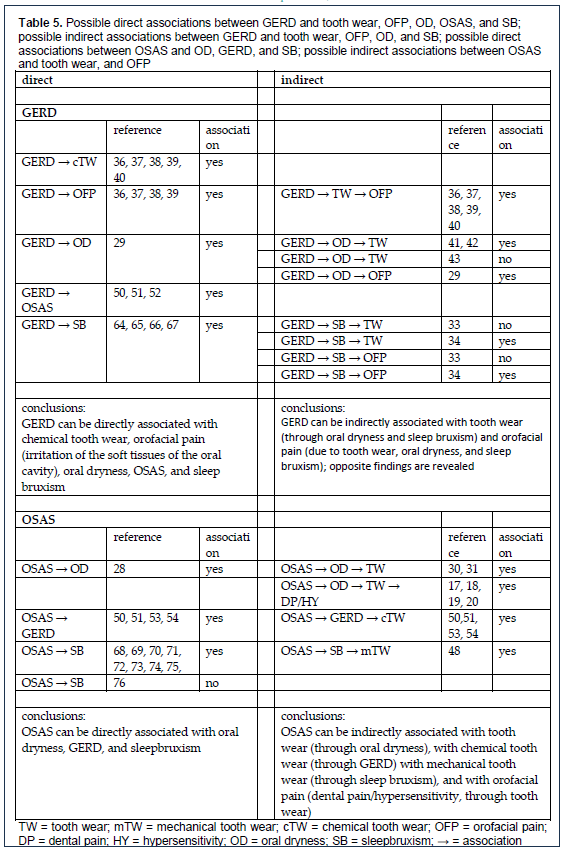
Amongst the included papers, 65 publications described the direct association between GERD and tooth wear and orofacial pain (irritation of the soft tissues), including 5 recent reviews (Table 5). In a systematic review from the gastroenterological community (36), it was concluded that there is a strong association between GERD and intrinsic chemical tooth wear, and that the severity of the tooth wear seems to be correlated with the severity of GERD symptoms. Recently, this was concluded again by 4 reviews from the dental community (37, 38, 39, 40) (Table 5). It is suggested that inspection of the oral cavity in search for intrinsic chemical tooth wear should become a routine maneuver in patients with GERD, and cooperation between physicians and dentists is strongly advocated to prevent or ameliorate possible oral effects of GERD (40).
Three others studies described the possible indirect association between GERD and tooth wear through oral dryness (41, 42, 43). On the one hand, it was revealed that patients with GERD had an impaired salivary flow rate as compared to controls (41, 42) and additionally a poorer salivary buffering capacity (42). However, on the other hand, Saksena and coauthors reported no difference in salivary flow or buffer capacity between GERD patients and controls (43)(see Table 5). Based on the available evidence, one may conclude that GERD is directly associated with intrinsic chemical tooth wear, orofacial pain (irritation of the soft tissues), OMD (see above), OSAS (see below), and sleep bruxism (see below). GERD is indirectly associated with chemical and mechanical tooth wear (due to OMD and sleep bruxism; see above, and below), and orofacial pain (due to tooth wear, oral dryness, and sleep bruxism; see above, and below; see Table 5).
Tooth wear and obstructive sleep apnea syndrome (OSAS)
Obstructive sleep apnea syndrome (OSAS) is the most common type of a sleep-related breathing disorders that is caused by transient obstruction of the upper airway, and is a multifactorial condition as well. It is characterized by repetitive interruptions in breathing during sleep, despite the effort to breathe, and is usually associated with a reduction in blood oxygen saturation (44). Snoring is a familiar condition that is characterized by loud breathing sounds, produced in the upper airway during sleep. Although these sounds give rise to social embarrassment, it still can be considered as physiological, while OSAS is considered as a pathological condition (45).
The prevalence of OSAS, according to general population-based studies, is approximately 3 to 7% for adult men and 2 to 5% for adult women (46) but higher figures have been reported. In this regard, a recent systematic review highlighted that the prevalence depends on the severity of the condition, with estimated ranges between 9% and 38% for mild OSAS, and 6% to 17% for moderate OSAS, men more affected than women (47). Factors that increase vulnerability for the disorder include higher age, male sex, obesity, family history, menopause, craniofacial abnormalities, and certain health behaviors like cigarette smoking and alcohol usage (46).
A direct association between tooth wear and OSAS cannot be hypothesized. Amongst the included papers, only 1 publication described a possible indirect association between tooth wear and OSAS (48)(Table 5). These authors concluded that patients with tooth wear had a high frequency of OSAS, and they found a positive association between tooth wear severity and the severity of the OSAS. Although they did not differentiate between chemical and mechanical tooth wear, the authors suggest that tooth wear assessment can be a tool to identify patients at risk for having OSAS (48). An explanation given by the authors is the possible association between OSAS and sleep bruxism. The patients in the study were treated with an oral appliance, and in that context, it is worth noting that evidence exists that the use of an occlusal splint can worsen the sleep apnea (49).
The possible association between GERD and tooth wear was already described, concluding a strong association between GERD and chemical intrinsic tooth wear. The possible associations between OSAS and GERD themselves are described as well. There is an association because of common risk factors, like gender and obesity (50, 51). GERD can proceed OSAS because an inflammation that results from reflux into the hypopharynx causes weakening and edema in these tissues, thus resulting in worsening an upper airway obstruction (52). The opposite, namely that an apnea event precedes an GERD event is also described; the reflux is then probably due to the generation of negative intrathoracic pressures during obstructive apneas and arousals (53, 54)(Table 5). Independent of the temporal relationship, one can hypothesize that, because of the coexistence of GERD and OSA, OSA patients show more (intrinsic chemical) tooth wear in comparison to healthy individuals, because the associated GERD activities cause more chemical tooth wear.
Sleep bruxism and tooth wear
According to a recent consensus paper, sleep bruxism and awake bruxism are considered different behaviors observed during wakefulness and during sleep. Both are multifactorial conditions as well (55). This means that a single definition for bruxism is no longer recommended, so that two separate definitions are proposed. Within this framework, sleep bruxism is a masticatory muscle activity during sleep that is characterized as rhythmic (phasic) or non-rhythmic (tonic) and is not a movement disorder or a sleep disorder in otherwise healthy individuals, whilst awake bruxism is a masticatory muscle activity during wakefulness that is characterized by repetitive or sustained tooth contact and/or by bracing or thrusting of the mandible and is not a movement disorder in otherwise healthy individuals (55). In otherwise healthy individuals, bruxism should not be considered as a disorder, but rather as a behavior, a physiological phenomenon, that can be a risk (and/or protective) factor for certain clinical consequences. Bruxism will be considered as pathological when a person experiences the possible negative consequences, like orofacial pain (e.g., meaning pain in the masticatory system) (55). The prevalence of bruxism varies from 8% to 31.4%, that of sleep bruxism from 9.7% to 15.9%, depending on the diagnostic methods used. Bruxism activities were found to be unrelated to gender, and a decrease with age was described in older people (56). Considering the possible association between bruxism and tooth wear, three possible interactions are described in the literature: tooth wear causes bruxism; tooth wear is a valid clinical diagnostic tool for bruxism; and tooth wear is a consequence of bruxism, meaning directly or indirectly associated with bruxism.
Considering the first interaction, viz., that tooth wear causes bruxism, it was concluded that there is no evidence available that occlusal interferences (worn dentitions) are involved in the etiology of bruxism (34, 57). Considering tooth wear possibly being a valid diagnostic tool for bruxism, five studies concluded that this is not the case (58, 59, 60, 61, 62), while only one study concluded the opposite (63). This can be explained by the fact that tooth wear is a multifactorial condition, and therefore always a combination of mechanical and chemical wear. Furthermore, tooth wear is irreversible, hence assessing tooth wear does provide information regarding the actual amount of tooth surface loss, but does not provide information regarding the timing of the tooth surface loss, in other words: whether the process is ongoing or a result from earlier loss.
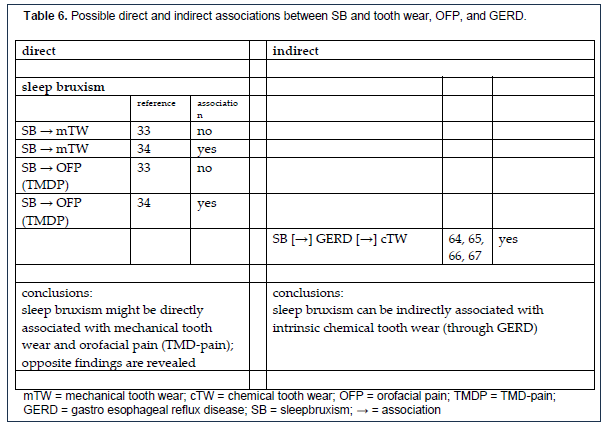
Considering the third interaction, sleep bruxism is (directly) associated with tooth wear, amongst the included papers and the additional relevant literature, one review concluded that bruxism is not directly associated with tooth wear and with orofacial pain (33)(table 6), while another conclude that the direct association exist (34)(table 6). The different conclusions are possible due to the fact that if sleep bruxism has been diagnosed more robustly, no consistent relationship has been found between sleep bruxism and tooth wear (33).
Above, the association between GERD and tooth wear was outlined. Interestingly, also evidence exists that sleep bruxism and GERD are associated with each other (64, 65, 66, 67(table 6). Hypothetically, when the onset of a GERD event precedes the onset of a sleep bruxism event, more tooth wear can be caused by the fact that grinding on the acid stomach contents covering the teeth can accelerate the amount of hard tissue loss.
Another interesting finding is the existing evidence of the possible association between sleep bruxism and OSA, in order to find out the possible implications for tooth wear. Two studies showed this association based on self-report (68, 69)(table 6). Six studies showed the association based on polysomnography (70, 71, 72, 73, 74, 76)(table 6). One study opposed regarding the possible association between sleep bruxism and OSAS (76)(table 6). A review discussed the possible theories regarding the associations between sleep bruxism and OSAS (77)(table 6). Hypothetically, when sleep bruxism and OSA are related, it is possible that OSA patients show more tooth wear in comparison to healthy individuals, because the associated sleep bruxism activities cause more mechanical tooth wear. The temporal relationship between sleep bruxism and OSA is not important regarding their influence on tooth wear, since only the SB activities cause mechanical tooth wear. The temporal relationship between sleep bruxism and GERD is important regarding their influence on tooth wear, because when GERD precedes sleep bruxism, the softening of the hard dental tissues by the stomach acid can accelerate the tooth surface loos by the sleep bruxism activities.
Table 1Definitions of dental sleep disorders as distinguished by Lobbezoo et al. (2016) |
{kind=link}
Table 2Description of used tools to diagnose tooth wear and the various dental sleep disorders |
{kind=link}
Table 3Possible direct and indirect associations between tooth wear and dental sleep disorders |
{kind=link}
Table 4Possible direct associations between tooth wear and OFP; possible direct and indirect associations between OD and tooth wear, OFP, and SB |
{kind=link}
Table 5Possible direct associations between GERD and tooth wear, OFP, OD, OSAS, and SB; possible indirect associations between GERD and tooth wear, OFP, OD, and SB; possible direct associations between OSAS and OD, GERD, and SB; possible indirect associations between OSAS and tooth wear, and OFP |
{kind=link}
Table 6Possible direct and indirect associations between SB and tooth wear, OFP, and GERD. |
{kind=link}
CONCLUSIONS
Dental sleep disorders and tooth wear are associated with each other, and all are common multifactorial conditions. For some disorders, this association can be direct, while for others the association can be indirect or both. The multifactorial nature of these conditions leads to a variety of assessment tools, which makes comparison of the findings in the literature difficult. Therefore, the below-mentioned conclusions are drawn with caution and must be used in a restraint way. We would like to stress out that further research is a necessity to better substantiate the conclusions in the future. The results of this narrative overview, however, can nevertheless serve as a starting point for further research.
For chemical tooth wear, a direct association with dental pain and/or hypersensitivity can exist. OMD can directly be associated with mechanical tooth wear (when less saliva causes less lubrication), chemical tooth wear (when less saliva results in less buffer capacity), orofacial pain (irritation of the soft tissues of the oral cavity, and sleep bruxism (compensating the oral dryness). Oral dryness can indirectly be associated with tooth wear, orofacial pain (dental pain/hypersensitivity due to tooth wear, and TMD pain through sleep bruxism). GERD can directly be associated with chemical tooth wear, orofacial pain (irritation of the soft tissues of the oral cavity), oral dryness, OSAS, and sleep bruxism. GERD can indirectly be associated with tooth wear (through oral dryness and sleep bruxism) and orofacial pain (due to tooth wear, oral dryness, and sleep bruxism). OSAS can directly be associated with oral dryness, GERD, and sleep bruxism, and can indirectly be associated with chemical tooth wear (through GERD) and mechanical tooth wear (through sleep bruxism), and orofacial pain (dental pain/hypersensitivity through tooth wear). Sleep bruxism seems to be directly associated with mechanical tooth wear and orofacial pain (TMD-pain). Sleep bruxism is indirectly associated with chemical tooth wear (through GERD).
Since the dental sleep disorders are interlinked with each other, the consequences are difficult to disentangle. When several sleep disorders are present at the same time, several scenarios are possible. The sleep disorders can have a synergetic effect to accelerate the tooth wear process. For example when during sleep a reflux event is followed by a bruxing event (the stomach acid will soften the hard dental tissues, which will wear away more easily by the followed grinding), or counteract and slow down the tooth wear process (for example when a bruxing event is followed by an increase of salivary flow, the risk of mechanical tooth wear is neutralized by the improved lubrication). Although more research is needed to confirm the validity of the assumed associations between the dental sleep disorders, improving knowledge is clinically relevant, because avoiding damage to the hard dental tissues during a lifespan is key. The results can support dental clinicians in finding all the etiological factors of the assessed tooth wear in their patients, and thus improve the provided dental care. Furthermore, there is a strong need for an interdisciplinary clinical team to manage oral health-related sleep disorders (79). Such a team ideally should consist of dentists specialized in TMD/orofacial pain, dentists specialized in dental sleep medicine, and dentist specialized in restorative/prosthetic dentistry, particularly in diagnosing and managing tooth wear. Only a comprehensive approach can result in a state of the art diagnostic process and thereby resulting in optimal care.
REFERENCES
- Shellis RP, Addy M. The interactions between attrition, abrasion and erosion in tooth wear. Monogr Oral Sci. 2014; 25: 32-45. Review.
- Wetselaar P, Lobbezoo F. The Tooth Wear Evaluation System (TWES): a modular clinical guideline for the diagnosis and management planning of worn dentitions. J Oral Rehabil. 2016; 43: 69-80. Review.
- Johansson AK, Omar R, Carlsson GE, Johansson A. Dental erosion and its growing importance in clinical practice: from past to present. Int J Dent. 2012; 2012: 632907.
- Gandara BK, Truelove EL. Diagnosis and management of dental erosion. J Contemp Dent Pract. 1999; 1: 16-23. Review.
- Ganss C, Lussi A. Diagnosis of erosive tooth wear. Monogr Oral Sci. 2014; 25:22-31.
- Wetselaar P, Faris A, Lobbezoo F. A plea for the development of an universally accepted modular tooth wear evaluation system. BMC Oral Health. 2016; 16: 115.
- Van’t Spijker A, Rodriguez JM, Kreulen CM, Bronkhorst EM, Bartlett DW, Creugers NH. Prevalence of tooth wear in adults. Int J Prosthodont. 2009; 22: 35-42.
- Jaeggi T, Lussi A. Prevalence, incidence and distribution of erosion. Monogr Oral Sci. 2014; 25: 55-73. Review.
- Wetselaar P, Vermaire JH, Visscher CM, Lobbezoo F, Schuller AA. The Prevalence of Tooth Wear in the Dutch Adult Population. Caries Res. 2016; 50: 543-550.
- Loomans B, Opdam N, Attin T, Bartlett D, Edelhoff D, Frankenberger R, Benic G, Ramseyer S, Wetselaar P, Sterenborg B, Hickel R, Pallesen U, Mehta S, Banerji S, Lussi A, Wilson N. Severe Tooth Wear: European Consensus Statement on Management Guidelines. J Adhes Dent. 2017; 19: 111-119.
- Lussi A, Carvalho TS. Erosive tooth wear: a multifactorial condition of growing concern and increasing knowledge. Monogr Oral Sci. 2014; 25: 1-15. Review.
- Lavigne GJ, Goulet JP, Zuconni M, Morrison F, Lobbezoo F. Sleep disorders and the dental patient: an overview. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 88: 257-72. Review.
- Lobbezoo F, Aarab G, Wetselaar P, Hoekema A, de Lange J, de Vries N. A new definition of dental sleep medicine. J Oral Rehabil. 2016; 430: 786-90.
- Aarab G, Lobbezoo F. Dental Sleep Medicine redefined. Sleep Breath. 2018; 22: 1233.
- Lobbezoo F, Aarab G. Increasing the Visibility of Dental Sleep Disorders. J Clin Sleep Med. 2018; 14: 1827.
- de Leeuw R, Klasser GD (eds) Orofacial pain. Guidelines for assessment, diagnosis, and management. Sixth Edition. The American Academy of Orofacial Pain. Chicago, IL: Quintessence Publishing Co, Inc; 2018.
- West NX, Sanz M, Lussi A, Bartlett D, Bouchard P, Bourgeois D. Prevalence of dentine hypersensitivity and study of associated factors: a European population-based cross-sectional study. J Dent. 2013; 41: 841-51.
- Burnett CA, Hussey DL, Clifford TJ. Presentation, diagnosis and initial management of patients referred to a hospital tooth wear clinic. Eur J Prosthodont Restor Dent. 2001; 9: 5-7.
- Wazani BE, Dodd MN, Milosevic A. The signs and symptoms of tooth wear in a referred group of patients. Br Dent J. 2012; 213: E10.
- Olley RC, Moazzez R, Bartlett D. The relationship between incisal/occlusal wear, dentine hypersensitivity and time after the last acid exposure in vivo. J Dent. 2015; 43: 248-52.
- Macfarlane TV, Kenealy P, Kingdon HA, Mohlin B, Pilley JR, Mwangi CW, Hunter L, Richmond S, Shaw WC. Orofacial pain in young adults and associated childhood and adulthood factors: results of the population study, Wales, United Kingdom. Community Dent Oral Epidemiol. 2009; 37: 438-50.
- Schierz O, John MT, Schroeder E, Lobbezoo F. Association between anterior tooth wear and temporomandibular disorder pain in a German population. J Prosthet Dent. 2007; 97: 305-9.
- Seligman DA, Pullinger AG. Dental attrition models predicting temporomandibular joint disease or masticatory muscle pain versus asymptomatic controls. J Oral Rehabil. 2006; 33: 789-99.
- Llena-Puy C. The rôle of saliva in maintaining oral health and as an aid to diagnosis. Med Oral Patol Oral Cir Bucal. 2006; 11: E449-55.
- Wolff A, Joshi RK, Ekström J, Aframian D, Pedersen AM, Proctor G, Narayana N, Villa A, Sia YW, Aliko A, McGowan R, Kerr AR, Jensen SB, Vissink A, Dawes C. A Guide to Medications Inducing Salivary Gland Dysfunction, Xerostomia, and Subjective Sialorrhea: A Systematic Review Sponsored by the World Workshop on Oral Medicine VI. Drugs R D. 2017; 17: 1-28. Review.
- Hopcraft MS, Tan C. Xerostomia: an update for clinicians. Aust Dent J. 2010; 553: 238–244.
- Löfgren CD, Wickström C, Sonesson M, Lagunas PT, Christersson C. A systematic review of methods to diagnose oral dryness and salivary gland function. BMC Oral Health. 2012; 12: 29. Review.
- Oksenberg A, Froom P, Melamed S. Dry mouth upon awakening in obstructive sleep apnea. J Sleep Res. 2006; 15: 317-20.
- Campisi G, Lo Russo L, Di Liberto C, Di Nicola F, Butera D, Vigneri S, Compilato D, Lo Muzio L, Di Fede O. Saliva variations in gastro-oesophageal reflux disease. J Dent. 2008; 36: 268-71.
- Hara AT, Zero DT. The potential of saliva in protecting against dental erosion. Monogr Oral Sci. 2014; 25: 197-205. Review.
- Young WG. The oral medicine of tooth wear. Aust Dent J. 2001; 46: 236-50; Review.
- Thie NM, Kato T, Bader G, Montplaisir JY, Lavigne GJ. The significance of saliva during sleep and the relevance of oromotor movements. Sleep Med Rev. 2002; 6: 213-27. Review100. Huynh NT, Emami E, Helman JI, Chervin RD. Interactions between sleep disorders and oral diseases. Oral Dis. 2014; 20: 236-45.
- Johansson A, Omar R, Carlsson GE. Bruxism and prosthetic treatment: a critical review. J Prosthodont Res. 2011; 55: 127-36.
- Lobbezoo F, Ahlberg J, Manfredini D, Winocur E. Are bruxism and the bite causally related? J Oral Rehabil. 2012; 39: 489-501. Review.
- Boeckxstaens G, El-Serag HB, Smout AJ, Kahrilas PJ. Symptomatic reflux disease: the present, the past and the future. Gut. 2014; 63: 1185-93.
- Pace F, Pallotta S, Tonini M, Vakil N, Bianchi Porro G. Systematic review: gastro-oesophageal reflux disease and dental lesions. Aliment Pharmacol Ther. 2008; 27: 1179-86. Review.
- Moazzez R, Bartlett D. Intrinsic causes of erosion. Monogr Oral Sci. 2014; 25: 180-96. Review.
- Schlueter N, Tveit AB. Prevalence of erosive tooth wear in risk groups. Monogr Oral Sci. 2014; 25: 74-98. Review.
- Marsicano JA, de Moura-Grec PG, Bonato RC, Sales-Peres M de C, Sales-Peres A, Sales-Peres SH. Gastroesophageal reflux, dental erosion, and halitosis in epidemiological surveys: a systematic review. Eur J Gastroenterol Hepatol. 2013; 25: 135-41. Review.
- Ranjitkar S, Smales RJ, Kaidonis JA. Oral manifestations of gastroesophageal reflux disease. J Gastroenterol Hepatol. 2012; 27: 21-7. Review.
- Moazzez R, Bartlett D, Anggiansah A. Dental erosion, gastro-oesophageal reflux disease and saliva: how are they related? J Dent. 2004; 32: 489-94.
- Yoshikawa H, Furuta K, Ueno M, Egawa M, Yoshino A, Kondo S, Nariai Y, Ishibashi H, Kinoshita Y, Sekine J. Oral symptoms including dental erosion in gastroesophageal reflux disease are associated with decreased salivary flow volume and swallowing function. J Gastroenterol. 2012; 47: 412-20.
- Saksena R, Bartlett DW, Smith BG. The role of saliva in regurgitation erosion. Eur J Prosthodont Restor Dent. 1999; 7: 121-4.
- Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. Sleep. 1999; 22: 667-89.
- Deary V, Ellis JG, Wilson JA, Coulter C, Barclay NL. Simple snoring: not quite so simple after all? Sleep Med Rev. 2014; 18: 453–462.
- Punjabi NM. The epidemiology of adult obstructive sleep apnea. Proc Am Thorac Soc. 2008; 5: 136-43.
- Senaratna CV, Perret JL, Lodge CJ, Lowe AJ, Campbell BE, Matheson MC, Hamilton GS, Dharmage SC. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med Rev. 2017; 34: 70-81. Review.
- Durán-Cantolla J, Alkhraisat MH, Martínez-Null C, Aguirre JJ, Guinea ER, Anitua E. Frequency of obstructive sleep apnea syndrome in dental patients with tooth wear. J Clin Sleep Med. 2015; 11: 445-50.
- Nikolopoulou M, Naeije M, Aarab G, Hamburger HL, Visscher CM, Lobbezoo F. The effect of raising the bite without mandibular protrusion on obstructive sleep apnea. J Oral Rehabil. 2011; 38: 643-7.
- Zanation AM, Senior BA. The relationship between extraesophageal reflux (EER) and obstructive sleep apnea (OSA). Sleep Med Rev. 2005; 9: 453-8. Review.
- Basoglu OK, Vardar R, Tasbakan MS, Ucar ZZ, Ayik S, Kose T, Bor S. Obstructive sleep apnea syndrome and gastroesophageal reflux disease: the importance of obesity and gender. Sleep Breath. 2015; 19: 585-92.
- Emilsson ÖI, Bengtsson A, Franklin KA, Torén K, Benediktsdóttir B, Farkhooy A, Weyler J, Dom S, De Backer W, Gislason T, Janson C. Nocturnal gastro-oesophageal reflux, asthma and symptoms of OSA: a longitudinal, general population study. Eur Respir J. 2013; 41: 1347-54.
- Foresman BH. Sleep-related gastroesophageal reflux. J Am Osteopath Assoc. 2000; 100 (12 Suppl Pt 2): S7-10. Review.
- Yang YX, Spencer G, Schutte-Rodin S, Brensinger C, Metz DC. Gastroesophageal reflux and sleep events in obstructive sleep apnea. Eur J Gastroenterol Hepatol. 2013; 25: 1017-23.
- Lobbezoo F, Ahlberg J, Raphael KG, Wetselaar P, Glaros AG, Kato T, Santiago V, Winocur E, De Laat A, De Leeuw R, Koyano K, Lavigne GJ, Svensson P, Manfredini D, Assessment of bruxism: the international consensus revisited. J Oral Rehabil. 2018; 45: 837-844.
- Manfredini D, Winocur E, Guarda-Nardini L, Paesani D, Lobbezoo F. Epidemiology of bruxism in adults: a systematic review of the literature. J Orofac Pain. 2013; 27: 99-110.
- Lobbezoo F, Naeije M. Bruxism is mainly regulated centrally, not peripherally. J Oral Rehabil. 2001; 28: 1085-91. Review.
- Abe S, Yamaguchi T, Rompré PH, De Grandmont P, Chen YJ, Lavigne GJ. Tooth wear in young subjects: a discriminator between sleep bruxers and controls? Int J Prosthodont. 2009; 22: 342-50.
- Palinkas M, De Luca Canto G, Rodrigues LA, Bataglion C, Siéssere S, Semprini M, Regalo SC. Comparative Capabilities of Clinical Assessment, Diagnostic Criteria, and Polysomnography in Detecting Sleep Bruxism. J Clin Sleep Med. 2015; 11: 1319-1325.
- Castroflorio T, Bargellini A, Rossini G, Cugliari G, Deregibus A, Manfredini D. Agreement between clinical and portable EMG/ECG diagnosis of sleep bruxism. J Oral Rehabil. 2015; 42: 759-64.
- Jonsgar C, Hordvik PA, Berge ME, Johansson AK, Svensson P, Johansson A. Sleep bruxism in individuals with and without attrition-type tooth wear: An exploratory matched case-control electromyographic study. J Dent. 2015; 43: 1504-10.
- Casett E, Réus JC, Stuginski-Barbosa J, Porporatti AL, Carra MC, Peres MA, de Luca Canto G, Manfredini D. Validity of different tools to assess sleep bruxism: a meta-analysis. J Oral Rehabil. 2017; 44: 722-734. Review
- Yoshizawa S, Suganuma T, Takaba M, Ono Y, Sakai T, Yoshizawa A, Kawana F, Kato T, Baba K. Phasic jaw motor episodes in healthy subjects with or without clinical signs and symptoms of sleep bruxism: a pilot study. Sleep Breath. 2014; 18: 187-93.
- Miyawaki S, Tanimoto Y, Araki Y, Katayama A, Fujii A, Takano-Yamamoto T. Association between nocturnal bruxism and gastroesophageal reflux. Sleep. 2003; 26: 888-92
- Miyawaki S, Tanimoto Y, Araki Y, Katayama A, Imai M, Takano-Yamamoto T. Relationships among nocturnal jaw muscle activities, decreased esophageal pH, and sleep positions. Am J Orthod Dentofacial Orthop. 2004; 126: 615-9.
- Ohmure H, Oikawa K, Kanematsu K, Saito Y, Yamamoto T, Nagahama H, Tsubouchi H, Miyawaki S. Influence of experimental esophageal acidification on sleep bruxism: a randomized trial. J Dent Res. 2011; 90: 665-71.
- Mengatto CM, Dalberto da S, Scheeren B, Barros SG. Association between sleep bruxism and gastroesophageal reflux disease. J Prosthet Dent. 2013; 110: 349-55.
- Ohayon MM, Li KK, Guilleminault C. Risk factors for sleep bruxism in the general population. Chest 2001; 119: 53-61.
- Hesselbacher S, Subramanian S, Rao S, Casturi L, Surani S. Self-reported sleep bruxism and nocturnal gastroesophageal reflux disease in patients with obstructive sleep apnea: relationship to gender and ethnicity. Open Respir Med J. 2014; 8: 34-40.
- Phillips BA, Okeson J, Paesani D, Gilmore R. Effect of sleep position on sleep apnea and parafunctional activity. Chest. 1986; 90: 424-9.
- Okeson JP, Phillips BA, Berry DTR, Cook YR, Cabelka JF. Nocturnal bruxism events in subjects with sleep-disordered breathing and control subjects. J Craniomandib Dis Facial Oral Pain 1991; 5: 258-64.
- Sjoholm TT, Lowe AA, Miyamoto K, Fleetham JA, Ryan CF. Sleep bruxism in sleep-disordered breathing. Arch Oral Biol 2000; 45: 889-96.
- Oksenberg A, Arons E. Sleep bruxism related to obstructive sleep apnea: the effect of continuous positive airway pressure. Sleep Med 2002; 3: 513-5.
- Hosoya H, Kitaura H, Hashimoto T, Ito M, Kinbara M, Deguchi T, Irokawa T, Ohisa N, Ogawa H, Takano-Yamamoto T. Relationship between sleep bruxism and sleep respiratory events in patients with obstructive sleep apnea syndrome. Sleep Breath. 2014; 18: 837-44.
- Saito M, Yamaguchi T, Mikami S, Watanabe K, Gotouda A, Okada K, Hishikawa R, Shibuya E, Lavigne G. Temporal association between sleep apnea-hypopnea and sleep bruxism events. J Sleep Res. 2013 Nov 4.
- Saito M, Yamaguchi T, Mikami S, Watanabe K, Gotouda A, Okada K, Hishikawa R, Shibuya E, Shibuya Y, Lavigne G. Weak association between sleep bruxism and obstructive sleep apnea. A sleep laboratory study. Sleep Breath. 2016; 20: 703-9.
- Manfredini D, Guarda-Nardini L, Marchese-Ragona R, Lobbezoo F. Theories on possible temporal relationships between sleep bruxism and obstructive sleep apnea events. An expert opinion. Sleep Breath. Sleep Breath. 2015; 19: 1459-65. Review
- Lobbezoo F, van der Zaag J, Visscher CM, Naeije M. Oral kinesiology. A new postgraduate programme in the Netherlands. J Oral Rehabil. 2004; 31: 192-8.
- Moore PA, Guggenheimer J. Medication-induced hyposalivation: etiology, diagnosis, and treatment. Compend Contin Educ Dent. 2008; 29: 50-5. Review
- Boyce HW, Bakheet MR. Sialorrhea: a review of a vexing, often unrecognized sign of oropharyngeal and esophageal disease. J Clin Gastroenterol. 2005; 39: 89-97.
- Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R; Global Consensus Group. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006; 101: 1900-20.
- Margaritis V, Nunn J. Challenges in assessing erosive tooth wear. Monogr Oral Sci. 2014;25:46-54
- Schlueter N, Luka B. Erosive tooth wear - a review on global prevalence and on its prevalence in risk groups. Br Dent J. 2018; 224: 364-370.
- Dworkin SF, LeResche L. Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord. 1992; 6: 301-55. Review.
- Thomson WM, Chalmers JM, Spencer AJ, Williams SM. The Xerostomia Inventory: a multi-item approach to measuring dry mouth. Community Dent Health. 1999; 16: 12-7.
- Gyawali CP, Kahrilas PJ, Savarino E, Zerbib F, Mion F, Smout AJPM, Vaezi M, Sifrim D, Fox MR, Vela MF, Tutuian R, Tack J, Bredenoord AJ, Pandolfino J, Roman S. Modern diagnosis of GERD: the Lyon Consensus. Gut. 2018; 67: 1351-1362. Review.
SUBMISSION & CORRESPONDENCE INFORMATION
Address correspondence to: Peter Wetselaar, Department of Orofacial Pain and Dysfunction, Academic Centre for Dentistry Amsterdam (ACTA), Gustav Mahlerlaan 3004, 1081 LA Amsterdam, The Netherlands, E-mail: p.wetselaar@acta.n