Sleep Team Perspectives 1, Issue 9.2
Utilizing Combination Positive Airway Pressure/Oral Appliance Therapy to Build Relationships With Physicians
http://dx.doi.org/10.15331/jdsm.7238
James Hogg, DDS
Over the past 14 years, I have practiced in 4 different dental offices in 2 states – this makes me quite unique in the dental sleep medicine (DSM) field. I realized early on that I needed a good relationship with my physician partners to receive referrals for oral appliance therapy (OAT) and concentrated my efforts toward meeting with physicians, sharing information, and gaining their trust.
Struggling With Physician Referrals
My journey in DSM started in 2007 while I was still practicing restorative dentistry in my private dental office in the suburbs of Chicago. After 25 years, I was having increased back and neck pain and was searching for new, less taxing services to provide my patients and extend my career. After I attended DSM educational courses, I was asked by a patient intolerant to continuous positive airway pressure (CPAP) to fabricate an appliance for him. After trial and error, I was pleased that the sleep physician said he was treated in his current protrusive/vertical position. Just as important, the patient reported that he felt better than he had in years, was not waking his wife with loud snoring, and was no longer the irritable, sleep-deprived person he once was. I was hooked on DSM and continued to take as many continuing education courses as time allowed. Over the next couple of years, I transitioned most of the restorative dental procedures in the office to my associates, and I concentrated on treating patients with obstructive sleep apnea (OSA) and snoring.
Initially, I tried dropping off donuts and recent research articles on OAT to the sleep physician’s front office staff but failed to see the sleep physicians in most offices. After attending a seminar on combination therapy, I decided to change my approach. I knew CPAP therapy was prescribed by sleep physicians for most of their patients suffering from OSA but unfortunately, only 30% to 60% of those patients are adherent with this therapy. 1,2
Combination Therapy – A Foot in the Physician’s Door
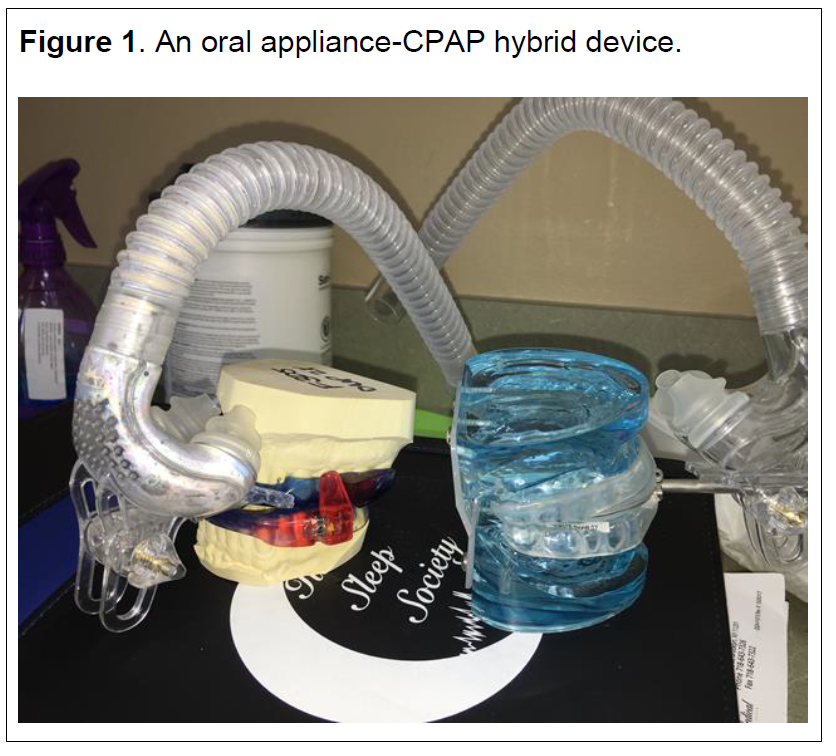
Combining CPAP therapy and OAT has proved to be a tolerable and effective therapeutic option. With combination therapy, many of the challenges of CPAP intolerance can be overcome, resulting in improved therapeutic outcomes. 4,5 Combination therapy uses a standard CPAP machine to deliver positive air pressure through a standard nasal and/or oronasal interface in conjunction with OAT (Figure 1).
Figure 1An oral appliance-CPAP hybrid device |
{kind=link}
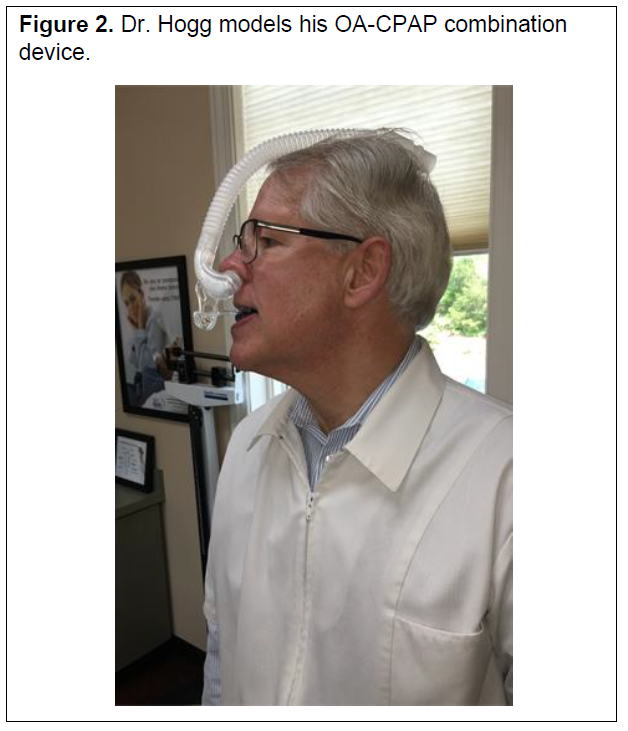
I have always personally trialed every new appliance that I order for a patient (I am up to 26 so far) and decided to combine the appliance I was wearing with a hybrid therapy mask and connect it to an AutoPAP (Figure 2). As a patient with moderate OSA, my apnea was controlled by my oral appliance alone, but I trialed the combination therapy at different protrusive positions and pressures. I found the combination of devices to be more comfortable to wear than my AutoPAP alone because I had no straps to deal with. Also, because the oral appliance was stabilizing my jaw, I experienced less leakage and required less pressure.
After these personal trials, I reached out to the sleep physicians’ offices and asked if I could do a lunch and learn with the doctors about combination PAP/OAT. The doctors were enthusiastic to meet with me because this therapy offered a new option to their partial responders/nonresponders to OAT. It could also increase compliance with their patients who were previously PAP noncompliant and reengage these patients for follow-up visits and titration of PSG to reset pressures.
Figure 2Dr. Hogg models his OA-CPAP combination device |
{kind=link}
At the lunch and learns, I demonstrated combination therapy using my personal devices and provided them with articles on combination therapy. 5,6 I was pleasantly surprised that I received a steady stream of referrals after these lunch and learns. Most of the time it was for OAT only, but if the patient had severe OSA, a multitude of comorbidities, and was PAP noncompliant, sometimes the sleep physician had me fabricate the combination therapy as a first-line therapy. In those cases, I would encourage the sleep physician to do a split study with only the oral appliance the first half of the night and the oral appliance and CPAP the second part of the night to see how the patient would respond to the oral appliance only.
After I sold my restorative practice, I merged my DSM practice with a multicenter (five offices) Chicagoland DSM practice. We collectively had completed approximately 10,000 cases with OAT when I left there in 2017. After joining, I continued to build referring relationships for my new group. In addition to presenting DSM lectures and grand rounds to primary care physicians, sleep physicians, and sleep technologists, I also visited hospital-based sleep physicians to demonstrate combination therapy and share articles. I felt success when I was able to convince these physicians to add combination PAP/OAT to the stock recommendations written in their assessment of the sleep study. Previously, only return to CPAP, weight loss, positional therapy, and further calibration of the appliance for partial/non responders to OAT were factors that were included in the notes. Once this information was included in the notes, it was easier to discuss combination therapy as an option with the patient.
New Location, Same Effective Strategy
After 7 years with this practice, I decided to move to Asheville, North Carolina to enjoy the local hiking and music. I worked for 2 years in a prosthodontic office that had a small DSM department. To introduce myself to the primary care physicians, sleep physicians, ear, nose, and throat physicians, endocrinologists, and cardiologists in Asheville, I again used combination therapy as a foot in the door to gain access to their offices. Although not as receptive as the Chicago physicians, I soon started to receive referrals from these contacts.
I now work in a large group practice in Brevard, North Carolina.I still only practice DSM and continue to treat patients with combination PAP/OAT.
In summary, there are multiple ways to build referral relationships with physicians in your area. Promoting combinations CPAP/OAT in real-time face-to-face meetings has been the most successful means I have found to becoming a valuable member of their sleep team.
CITATION
Hogg J. Utilizing combination positive airway pressure/oral appliance therapy to build relationships with physicians. J Dent Sleep Med. 2022;9(2).
REFERENCES
- Weaver TE, Sawyer AM. Adherence to continuous positive airway pressure treatment for obstructive sleep apnoea: implications for future interventions. Indian J Med Res. 2010;131:245–258.
- Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc. 2008;5(2):173–178.
- Sutherland K, Phillips CL, Cistulli PA. Efficacy versus effectiveness in the treatment of obstructive sleep apnea: CPAP and oral appliances. J of Dent Sleep Med 2015;2(4):175–181.
- Denbar MA. A case study involving the combination treatment of an oral appliance and auto-titrating CPAP unit. Sleep Breath. 2002;6(3):125–128.
- El-Solh AA, Moitheennazima B, Akinnusi ME, Churder PM, Lafornara AM. Combined oral appliance and positive airway pressure therapy for obstructive sleep apnea: a pilot study. Sleep Breath. 2011;15(2):203–208.
- de Vries GE, Doff MH, Hoekema A, Kerstjens HA, Wijkstra PJ. Continuous positive airway pressure and oral appliance hybrid therapy in obstructive sleep apnea: patient comfort, compliance and preference: a pilot study. J Dent Sleep Med. 2016;3(1):5–10.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted August 15, 2021.
Submitted in final revised form December 2, 2021.
Accepted for publication January 23, 2022
Address correspondence to: James Hogg, DDS, Carolina Smiles Family Dental, 4 Market Street, Suite 200, Brevard, NC 28712; Email: drjamesjhogg@gmail.com