Review Article, Issue 4.4
Periodontitis and Obstructive Sleep Apnea: A Literature Review
http://dx.doi.org/10.15331/jdsm.6744
Charles Tremblay, DMD1 ; Pascale Beaudry, DMD1 ; Caroline Bissonnette, DMD1 ; Carole-Anne Gauthier, DMD1 ; Samuel Girard, DMD1 ; Marie-Pier Milot, DMD1 ; Robert Durand, DMD, MSc1 ; Nelly Huynh, PhD1,2
ABSTRACT
Study Objectives:
The aim of this literature review was to investigate the possible association between periodontitis and obstructive sleep apnea (OSA) by highlighting hypotheses, probing evidence and current research.
Methods:
The PubMed database from 2006 to October 2016 was used to select the eligible articles. Six independent evaluators extracted data from studies investigating the association between periodontitis and OSA and meeting the selection criteria.
Results:
Eleven studies were selected for analysis. Three of them only measured the levels of cytokines and collagenases. Five studies found a significant association between periodontitis and OSA, and two studies found no significant association. Different study limitations were observed, thus increasing the risk of bias. A few examples are the lack of standardization for diagnosis of periodontitis and OSA, differences in therapeutic approaches and study design.
Conclusions:
A causal relationship between periodontitis and OSA is still debatable due to the heterogeneity of studies and divergence of results. The benefits of periodontal treatment as an adjunct therapy for OSA still need further evaluation in randomized controlled studies with an emphasis on inflammatory plasma and salivary markers linking these two conditions.
Keywords:
obstructive sleep apnea, periodontal diseases, periodontitis
Citation:
Tremblay C, Beaudry P, Bissonnette C, Gauthier CA, Girard S, Milot MP, Durand R, Huynh N. Periodontitis and obstructive sleep apnea: a literature review. Journal of Dental Sleep Medicine. 2017;4(4):103–110
INTRODUCTION
Obstructive sleep apnea (OSA), a chronic multifactorial respiratory disease, consists of a temporary decrease or cessation of breath for ≥ 10 seconds and leads to a reduction in blood oxygen saturation of more than 3% to 4% and/or neurological arousal.1–3 OSA involves the upper respiratory tract, and it has been proven that snoring and OSA have systemic consequences in humans.4 It has been recently suggested that OSA may be related to periodontitis, another chronic multifactorial disease.5,6 Periodontitis is characterized by chronic inflammation of tooth-supporting tissues.1,5,6 In addition, these conditions are associated with similar systemic inflammatory responses and involve common inflammatory mediators such as interleukins, metalloproteinases, and tumor necrosis factor (TNF)-α.
Indeed, both conditions have been shown to be associated with the development of systemic diseases including cardiovascular diseases and diabetes.3,7,8 An association between these conditions could also have repercussions on the practice of dentistry and medicine. In order to guide the health care professional on diagnostic methods, risk factors, and treatments, the research is currently focused on whether there is a causal relationship between periodontitis and OSA. This would not only encourage more comprehensive dental care but also contribute to establish a partnership between the dentist and the physician.
Objective
This review of the literature aimed to evaluate the current evidence regarding the association between periodontitis and OSA and the potential mechanisms involved.
METHODS
Electronic Search
A systematic approach was used to identify articles investigating a potential association between periodontitis and OSA. A detailed search of PubMed electronic literature with a 10-year limit (2006 to October 2016) was applied. The search strategy involved the following keywords: “obstructive sleep apnea” AND “periodontal disease.”
Selection of Studies
Selection of studies by title and abstracts review was carried out individually by each of the 6 reviewers (CT, PB, CB, CAG, SG, MM). To be eligible, studies had to investigate whether there was an association between the two conditions. Abstracts of articles not covering the subject of association were eliminated. The original article of the incomplete abstracts was revised for further details.
RESULTS AND DISCUSSION
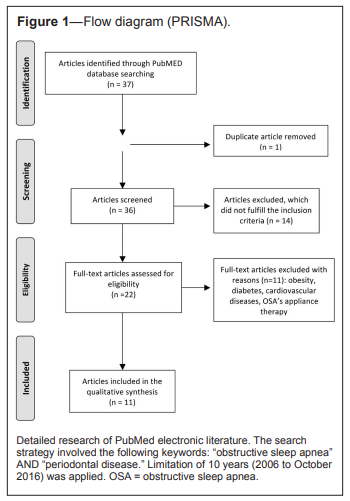
Thirty-six publications were initially selected. However, 25 articles were rejected for lack of emphasis on one or both conditions. For example, the focus for several studies was on obesity, diabetes, cardiovascular disease, and OSA therapeutics. Consequently, only 11 studies were included in this literature review (see Figure 1).
Figure 1Flow diagram (PRISMA) |
{kind=link}
In the selected studies, the apnea-hypopnea index (AHI) and the oxygen saturation rate were the objective measures frequently used to diagnose and measure the severity of OSA.2,3,5–7,9,10 Some authors have, however, relied on more subjective determinants such as the STOP1 and Berlin11,12 questionnaires. In regard to periodontitis, clinical parameters including pocket depth, level of clinical attachment, gingival recession, salivary and plasma cytokine levels, and plaque and gingival index were used.1–3,5–7,10,13 From articles on the association of chronic periodontitis with OSA, the following hypotheses linking these pathologies were described: systemic inflammation, mouth breathing, and common risk factors.8
Chronic Systemic Inflammation
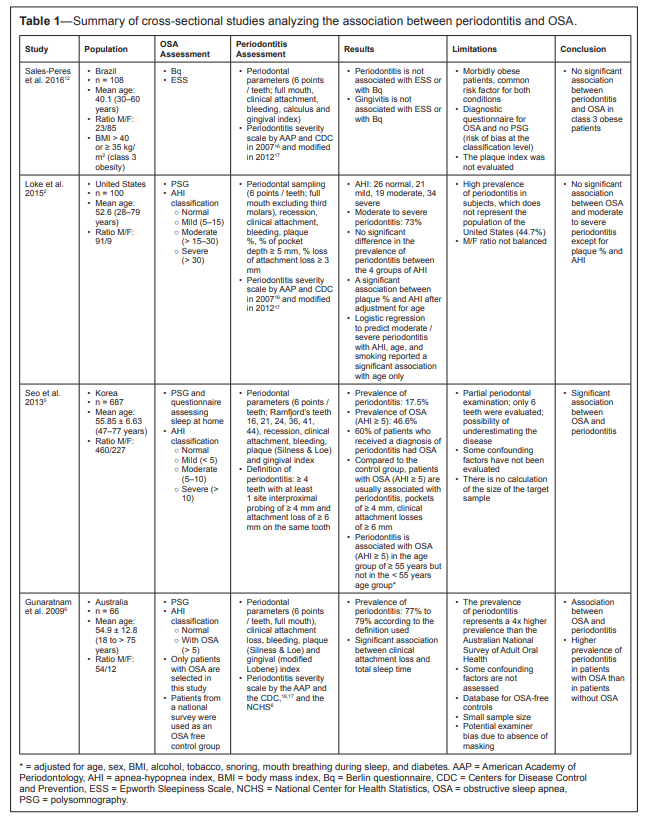
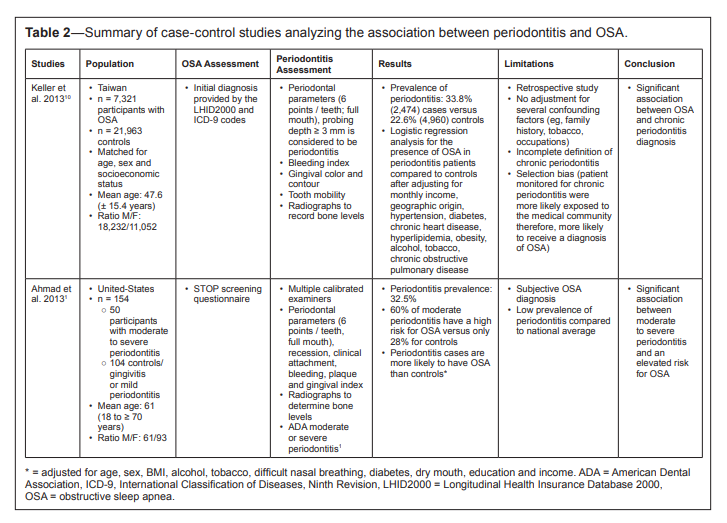
Gunaratnam et al. reported for the first time in 2009 that there may be an inflammatory link between periodontitis and OSA. They noted a high prevalence of periodontal disease in subjects with OSA (77% to 79%) but could not assert a causal link due to a significant lack of correlation of the measures.6 Nevertheless, they suggested that periodontitis may be one of the co-factors involved in the association between apnea and cardiovascular disease, or that a preexisting OSA could worsen the presence and severity of periodontal disease. Following these hypotheses, several studies (Table 1 2,5,6,12,16,17 and Table 2 1,10) have investigated the presence of an association between OSA and periodontitis.
Table 1Summary of cross-sectional studies analyzing the association between periodontitis and OSA |
{kind=link}
Table 2Summary of case-control studies analyzing the association between periodontitis and OSA |
{kind=link}
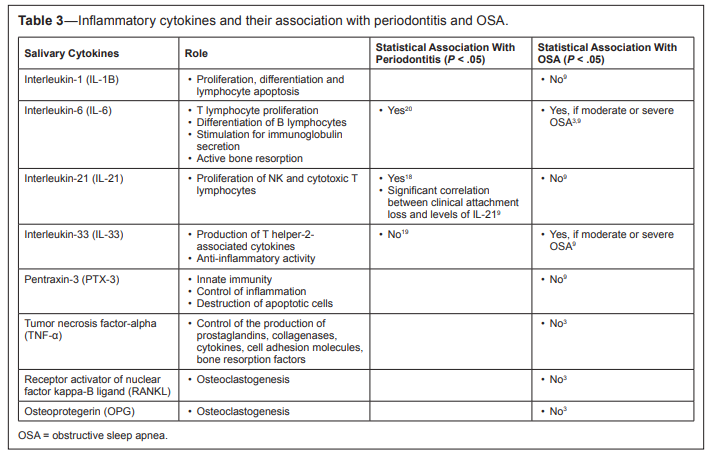
Nizam et al.9 have shown that OSA does not have a prominent effect on salivary IL-1B, IL-21, and PTX3, inflammatory markers of periodontitis (Table 3 3,9,18–20 and Table 4 3,21). However, they found that salivary IL-6 and IL-33 tend to increase in patients with apnea, regardless of severity, whereas IL-33 levels appear to decrease with the evolution of chronic periodontitis. Thus, being in higher concentration during periodontitis, only the salivary IL-6 could be related to the elevation found in OSA.9 This could then reflect the degree of subclinical inflammation present in the periodontal tissues and partly explain the pathogenesis. This potential causeeffect relationship has unfortunately not been fully demonstrated in another subsequent case-control study by the same authors.3 Larger population studies with different periodontal disease categories are needed to confirm this link and to test the possibility of a dose-response relationship. No differences were statistically significant with these same cytokines in serum according to the studies by Nizam et al.3,9 However, some studies have demonstrated a correlation between plasma IL-6 and TNF-α with moderate to severe OSA22–25 or periodontitis.26,27 It is suggested that this difference may be related to body mass index, periodontal diagnosis, and demographic status variations between studies.
Table 3Inflammatory cytokines and their association with the periodontitis and OSA |
{kind=link}
Table 4Peptide hormone and its association with periodontitis and OSA |
{kind=link}
A third case-control study by Nizam et al.7 examined the role of salivary and serum collagenases in the association between OSA and periodontal disease (Table 5 7,28,29). The hypothesis was that increased levels of biomarkers in patients with OSA could also affect the periodontal health of individuals. They evaluated the salivary and blood concentrations of neutrophils and their enzymes (metalloproteinases, myeloperoxidases, and elastases), which usually increase during inflammation. Several metalloproteinases (MMP-2, MMP-9) have already been associated with periodontal destruction.28,30 In this study by Nizam et al., a statistically significant inversely proportional relationship was demonstrated between the severity of OSA and the rate of salivary elastases, salivary proMMP-2s, serum proMMP-9s and the activation degree of salivary MMP-9s.
Table 5Salivary or plasma enzymes and their association with periodontitis and OSA |
{kind=link}
This finding contradicts in part the previously described pathophysiological relationship, establishing a proportional relationship between plasma MMP-9 and the severity of OSA.29,31 Again, these differences may be related to various periodontal diagnostics and demographic status from these studies.
Mouth Breathing
Second, there is the hypothesis that mouth breathing would be indirectly associated with periodontitis through changes it can cause in the oral environment. In a healthy patient with no nasal involvement, mouth breathing accounts for approximately 4% of total ventilation.5 This percentage tends to increase with aging. In a study by Seo et al.,5 the prevalence of mouth breathing appeared to be higher in patients with OSA. By generating dry mouth, this type of breathing tends to diminish the self-cleaning and antibacterial effect of saliva. It is then possible to note an increase in bacterial colonization and subsequent gingival inflammation. These two factors may increase the risk of developing periodontal disease or trigger its progression.5,13 However, in this study, the presence of mouth breathing was subjectively measured using a questionnaire, which limits the interpretation of the results. A case-control study using another type of questionnaire demonstrated an opposite relationship between mouth breathing and periodontitis.1 It is suggested that a more objective approach (for example, using the AHI) be used in subsequent studies. Confirmation of a bidirectional relationship between OSA and periodontitis through mouth breathing remains to be proved.13Common Risk Factors
Finally, the third hypothesis often presented in the literature is the comorbidity relationship between the two conditions, given that they have several common risk factors such as tobacco use, sex (male), aging, alcohol consumption, obesity, and diabetes.1,3,5,7,9,10 In periodontitis, we also observe ethnicity (Hispanic and African), stress, social class, and poor oral hygiene.1,6 The simultaneous presence of periodontitis and OSA in an individual would then be attributable to the common risk factors and would act as a comorbidity link in contrast to the first two assumptions where there is a causal link.8 It should also be noted that periodontitis is a common disease. According to the National Health and Nutrition Examination Survey, it would affect up to 47.2% of the population in the years 2009–2010.8 According to a study by Lee et al.,32 OSA would reach 2% to 4% of middle-aged Caucasian men and women. It is therefore to be expected that these two conditions may very well be present in the same individual without there necessarily being a causal link between them.As a result of these studies, a systematic review and metaanalysis was published by Al-Jewair in 2015.8 Including 6 studies, the authors concluded that an association is still possible but that the recent evidence is insufficient to support a causal link, or to assert that the treatment of periodontitis has a significant effect on OSA.1,2,5,6,9,10 Thus, for the time being, it is preferable to refer to systemic inflammatory pathways common to the two diseases where further studies will be required to fully demonstrate a cause-and-effect relationship.8,13 As such, a 2016 study by Al Habashneh et al. including 294 men in Jordan evaluated this association link.11 The Berlin questionnaire was used to assess the risk of OSA. Subjects at high risk of OSA were more frequently and severely affected by periodontitis (odds ratio = 2.3 with 95% confidence interval = 1.03–5.10) than those at low risk of OSA. However, the diagnostic value of the Berlin questionnaire remains debatable in comparison to polysomnography and this study was only carried out with male subjects.
Limitations
There are inevitable limitations in the collection of data and the comparative analysis between several studies. Thus, the research methods and conclusions of the studies often differ from each other. Among others, compared to the study by Gunaratnam et al. where the odds ratio between periodontitis and OSA was almost 4,6 according to Keller,10 this ratio would be closer to 1.75. The case-control study of Ahmad et al. also came to the conclusion that there was an association.1 However, unlike the study by Gunaratnam et al., patients did not receive a clinical diagnosis before they were categorized with OSA. The study used a validated questionnaire (STOP) to obtain an estimate of the risk of OSA.1 In contrast, Loke et al. concluded that there was a significant association between OSA severity and plaque percentage but no correlation between OSA and the prevalence of moderate or severe periodontitis.2 These examples of contradictory results demonstrate the importance of the limiting factors present in the studies.The selection of cases in the studies can be done either by using databases of patients who have responded positively to questionnaires or by means of an examination done clinically. It is evident that an individualized and standardized approach is more accurate for the diagnosis of periodontal diseases.10 Despite the calibrated classification of the periodontal disease, the case-control division is performed using various measures that can be influenced by the operator. Measurement of plaque level, bleeding, mobility, furcation defect, and loss of attachment by several operators using different techniques may create a certain variance and a margin of error.1,10 In addition, not all studies used the same definition of periodontitis, which could lead to underestimation or over-estimation of prevalence.8 In addition, the geographical location may vary from one study to another, which leads to the lack of uniformity in the prevalence and severity of the disease.8
Being aware of the initial hypotheses, the objectivity of the examiner may be biased during the periodontal data collection, hence the need for a blind approach.6 In addition, some studies are limited to a partial periodontal evaluation of the mouth5 compared to others with 6 measurement points for each tooth.2 In order to make an objective diagnosis of OSA, in contrast to the rather subjective approach of the STOP1 or Berlin11,12 questionnaires, polysomnography assessing rapid eye movement, oxygen saturation index, and AHI were used.2,3,5–7,9,10
The often unequal proportion between the case-control groups and the therapeutic irregularity in patients with OSA also affects the results. In addition, untreated OSA is usually associated with mouth breathing. This causes both dry mouth and a decrease in the self-cleaning effect of the saliva, which ultimately promotes bacterial colonization. Patients treated with continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BPAP) will have less of this type of breathing. As a result, a mixture of treated and untreated patients in the same group affects its uniformity and thus, the potential correlation with periodontitis.13 Similarly, the possibility of having members of the control group with an asymptomatic, undiagnosed OSA or other sleep disorder (eg, snoring) may also lead to a lack of uniformity in the control groups.13
Studies that did not distinguish smokers from nonsmokers included a limitation because smoking affects not only the salivary levels of cytokines but also the risk of OSA or chronic periodontitis.7,9,10 The absence or variation of the AHI is another cited factor that can obscure the uniformity of the observed cases.2,8 The standardization of study groups according to each of these categories is therefore necessary in order to improve the internal validity of the studies. It is also important to note that some studies had a limited number of participants.7,9 Severe inclusion criteria and lack of patient availability are reasons.6,7 In general, it is also possible that in a patient treated for periodontitis, OSA is more likely to be diagnosed in comparison with a person unaware of having this condition. This might again increase the correlation rate.10
Future Research and Current Practice Suggestions
Carra et al.13 recently published a study on the potential improvement of periodontitis with CPAP and/or BPAP. This treatment with a facial mask, a novel therapy for OSA, may include a humidification device, which reduces dry mouth. Even if the link between mouth breathing associated with OSA and periodontitis is still debated to this day, this device opens several avenues of research. This study failed to observe a difference in inflammation, plaque, calculus, number of missing teeth, or masticatory function between individuals using these devices and those who did not use them. However, this study has some limitations. Patients using the CPAP/BPAP could have been particularly motivated to maintain their oral hygiene and receive regular medical follow-ups. Also, the controls were subjectively selected using a questionnaire and the adhesion to the CPAP/BPAP could not be measured. The potential presence of patients with asymptomatic or undiagnosed OSA in the control group is another limitation. Thus, one cannot conclude if this OSA therapy has a beneficial effect on the periodontitis, even if it succeeds in decreasing mouth breathing.In light of recent studies, a diligent dentist could incorporate new OSA front-line detection techniques into his or her clinical evaluation. According to Ahmad et al.,1 on average, a patient visits the dentist more often than his or her physician. Having the responsibility to promote oral health and hygiene,33 it was suggested that the STOP questionnaire (Appendix 1, supplemental material) be included in the dental examination. As a rapid and effective method, this self-reported questionnaire identifies patients at risk for sleep apnea without, however, providing a categorical diagnosis. The integration of this questionnaire could thus intercept systemic diseases. Collaboration and possible exchange of results between the dentist and the family physician would then be necessary in order to carry out a more objective examination such as polysomnography or polygraphy.
Appendix 1STOP Obstructive Sleep Apnea Questionnaire |
CONCLUSIONS
To date, association studies between OSA and periodontitis are often based on different diagnostic criteria and show conflicting results. The many limiting factors and the difficulty in recruiting high numbers of participants preclude scientists and clinicians from drawing any conclusions. However, there seems to be a possible link between periodontitis and OSA syndrome via plasma and salivary inflammatory markers. Despite recent awareness, few studies have specifically focused on these aspects. Thus, well-structured, randomized control trials are needed to confirm this association and to clarify the mechanism of interaction between the two conditions.
REFERENCES
2. Loke W, Girvan T, Ingmundson P, Verrett R, Schoolfield J, Mealey BL. Investigating the association between obstructive sleep apnea and periodontitis. J Periodontol. 2015;86(2):232–243.
3. Nizam N, Basoglu OK, Tasbakan MS, Lappin DF, Buduneli N. Is there an association between obstructive sleep apnea syndrome and periodontal inflammation? Clin Oral Investig. 2016;20(4):659–668.
4. Huynh NT, Desplats E, Almeida FR. Orthodontics treatments for managing obstructive sleep apnea syndrome in children: a systematic review and meta-analysis. Sleep Med Rev. 2016;25:84–94.
5. Seo WH, Cho ER, Thomas RJ, et al. The association between periodontitis and obstructive sleep apnea: a preliminary study. J Periodontal Res. 2013;48(4):500–506.
6. Gunaratnam K, Taylor B, Curtis B, Cistulli P. Obstructive sleep apnoea and periodontitis: a novel association? Sleep Breath. 2009;13(3):233–239.
7. Nizam N, Basoglu OK, Tasbakan MS, et al. Do salivary and serum collagenases have a role in an association between obstructive sleep apnea syndrome and periodontal disease? A preliminary case-control study. Arch Oral Biol. 2015;60(1):134–143.
8. Al-Jewair TS, Al-Jasser R, Almas K. Periodontitis and obstructive sleep apnea’s bidirectional relationship: a systematic review and metaanalysis. Sleep Breath. 2015;19(4):1111–1120.
9. Nizam N, Basoglu OK, Tasbakan MS, Nalbantsoy A, Buduneli N. Salivary cytokines and the association between obstructive sleep apnea syndrome and periodontal disease. J Periodontol. 2014;85(7):e251–e258.
10. Keller JJ, Wu CS, Chen YH, Lin HC. Association between obstructive sleep apnoea and chronic periodontitis: a population-based study. J Clin Periodontol. 2013;40(2):111–117.
11. Al Habashneh R, Khassawneh B, Khader YS, Abu-Jamous Y, Kowolik MJ. Association between obstructive sleep apnea and periodontitis among male adults attending a primary healthcare facility in Jordan. Oral Health Prev Dent. 2016;14(2):157–164.
12. Sales-Peres SH, Groppo FC, Rojas LV, de C Sales-Peres M, Sales-Peres A. A periodontal status in morbidly obese patients with and without obstructive sleep apnea syndrome risk: a cross-sectional study. J Periodontol. 2016;87(7):772–782.
13. Carra MC, Thomas F, Schmitt A, Pannier B, Danchin N, Bouchard P. Oral health in patients treated by positive airway pressure for obstructive sleep apnea: a population-based case-control study. Sleep Breath 2016;20(1):405–411.
14. Trombone AP, Cardoso CR, Repeke CE, et al. Tumor necrosis factoralpha -308G/A single nucleotide polymorphism and red-complex periodontopathogens are independently associated with increased levels of tumor necrosis factor-alpha in diseased periodontal tissues. J Periodontal Res. 2009;44(5):598–608.
15. Sales-Peres SH, de Moura-Grec PG, Yamashita JM, et al. Periodontal status and pathogenic bacteria after gastric bypass: a cohort study. J Clin Periodontol. 2015;42(6):530–536.
16. Page RC, Eke PI. Case definitions for use in populationbased surveillance of periodontitis. J Periodontol. 2007;78(7 Suppl):1387–1399.
17. Eke PI, Dye BA, Wei L, et al. Prevalence of periodontitis in adults in the United States: 2009 and 2010. J Dent Res. 2012;91(10):914–920.
18. Mootha A, Malaiappan S, Jayakumar ND, Varghese SS, Toby Thomas J. The effect of periodontitis on expression of interleukin-21: a systematic review. Int J Inflam. 2016;2016:3507503.
19. Buduneli N, Özçaka Ö, Nalbantsoy A. Interleukin-33 levels in gingival crevicular fluid, saliva, or plasma do not differentiate chronic periodontitis. J Periodontol. 2012;83(3):362–368.
20. Costa PP, Trevisan GL, Macedo GO, et al. Salivary interleukin-6, matrix metalloproteinase-8, and osteoprotegerin in patients with periodontitis and diabetes. J Periodontol. 2010;81(3):384–391.
21. Henley DE, Buchanan F, Gibson R, et al. Plasma apelin levels in obstructive sleep apnea and the effect of continuous positive airway pressure therapy. J Endocrinol. 2009;203(1):181–188.
22. Inancli HM, Enoz M. Obstructive sleep apnea syndrome and upper airway inflammation. Recent Pat Inflamm Allergy Drug Discov. 2010;(1):54–57.
23. Medeiros CA, de Bruin VM, Andrade GM, Coutinho WM, de Castro-Silva C, de Bruin PF. Obstructive sleep apnea and biomarkers of inflammation in ischemic stroke. Acta Neurol Scand. 2012;126(1):17–22.
24. Arnardottir ES, Maislin G, Schwab RJ, et al. The interaction of obstructive sleep apnea and obesity on the inflammatory markers C-reactive protein and interleukin-6: the Icelandic Sleep Apnea Cohort. Sleep. 2012;35(7):921–932.
25. Ryan S, Taylor CT, McNicholas WT. Selective activation of inflammatory pathways by intermittent hypoxia in obstructive sleep apnea syndrome. Circulation. 2005;112(17):2660–2667.
26. Marcaccini AM, Meschiari CA, Sorgi CA, et al. Circulating interleukin-6 and high-sensitivity C-reactive protein decrease after periodontal therapy in otherwise healthy subjects. J Periodontol. 2009;80(4):594–602.
27. Iwamoto Y, Nishimura F, Soga Y, et al. Antimicrobial periodontal treatment decreases serum C-reactive protein, tumor necrosis factor-alpha, but not adiponectin levels in patients with chronic periodontitis. J Periodontol. 2003;74(8):1231–1236.
28. Mäkelä M, Salo T, Uitto VJ, Larjava H. Matrix metalloproteinases (MMP-2 and MMP-9) of the oral cavity: cellular origin and relationship to periodontal status. J Dent Res. 1994;73(8):1397–1406.
29. Ye J, Liu H, Li Y, Liu X, Zhu JM. Increased serum levels of C-reactive protein and matrix metalloproteinase-9 in obstructive sleep apnea syndrome. Chin Med J. 2007;120(17):1482–1486.
30. Birkedal-Hansen H, Moore WG, Bodden MK, et al. Matrix metalloproteinases: a review. Crit Rev Oral Biol Med. 1993;4(2):197–250.
31. Chuang LP, Chen NH, Lin SW, Chang YL, Chao IJ, Pang JH. Increased matrix metalloproteinases-9 after sleep in plasma and in monocytes of obstructive sleep apnea patients. Life Sci. 2013;93(5–6):220–225.
32. Lee W, Nagubadi S, Kryger MH, Mokhlesi B. Epidemiology of obstructive sleep apnea: a population-based perspective. Expert Rev Respir Med. 2008;2(3):349–364.
33. Giddon DB, Swann B, Donoff RB, Hertzman-Miller R. Dentists as oral physicians: the overlooked primary health care resource. J Prim Prev. 2013;34(4):279–291.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication April 25, 2017
Submitted in final revised form April 25, 2017
Accepted for publication July 13, 2017
DISCLOSURE STATEMENT
The authors report no financial conflicts of interest.
PDF