Review Article, Issue 2.4
Efficacy versus Effectiveness in the Treatment of Obstructive Sleep Apnea: CPAP and Oral Appliances
http://dx.doi.org/10.15331/jdsm.5120
Kate Sutherland, PhD1,2; Craig L. Phillips, PhD1,2; Peter A. Cistulli, MD, PhD1
ABSTRACT
Obstructive sleep apnea (OSA) is a chronic disorder and effective long-term treatment is necessary to prevent associated health risks. Standard treatment remains continuous positive airway pressure which is highly efficacious but has well-recognized limitations, with suboptimal patient acceptance and adherence rates, which in turn obviates the desired health benefits. The leading alternative device treatment is oral appliances. Patients often report preferring oral appliances to CPAP treatment, with better usage rates. However, unlike CPAP, inter-individual variability in the efficacy of oral appliance therapy means that patients are often left with some residual OSA. Despite discrepancies in efficacy (apnea-hypopnea index [AHI] reduction) between CPAP and oral appliances, randomized trials show similar improvements in health outcomes between treatments, including sleepiness, quality of life, driving performance, and blood pressure. Similar results in terms of health outcomes suggests that although the two treatments have different efficacy and treatment usage profiles, these result in similar overall effectiveness. In this narrative review, we discuss efficacy versus effectiveness in relation to CPAP and oral appliance treatment of OSA.
Keywords:
obstructive sleep apnea, treatment effectiveness, efficacy, CPAP, oral appliances
Citation:
Sutherland K, Phillips CL, Cistulli PA. Efficacy versus effectiveness in the treatment of obstructive sleep apnea: CPAP and oral appliances. Journal of Dental Sleep Medicine 2015;2(4):175–181.
Efficacy and effectiveness are important concepts to distinguish when evaluating treatment performance. Treatment efficacy refers to how well an intervention works under ideal circumstances whereas, effectiveness is how well an intervention performs in the real world where conditions are not controlled. Therefore treatment effectiveness is particularly important in management of chronic disease. Obstructive sleep apnea (OSA) is a common sleep disorder characterized by repetitive upper airway obstruction leading to intermittent hypoxia and sleep fragmentation. There has been a dramatic increase in OSA prevalence over the last two decades, attributable to the obesity epidemic, with at least moderate OSA now evident in 17% of middle-aged men and 9% of middle-aged women.1 OSA is associated with excessive daytime sleepiness and lower quality of life as well as increased risk of workplace and motor vehicle accidents, hypertension and cardiovascular disease, type 2 diabetes, and all-cause mortality.2–9 Therefore effective management of this chronic disorder is imperative to not only improve symptoms but to prevent long-term health risks. Standard care is the highly efficacious treatment, continuous positive airway pressure (CPAP). This therapy involves delivery of pressurized air to the upper airway during sleep via a nasal mask interface and tube connected to a pump. The pressurized air acts to splint open the upper airway preventing it from collapsing during sleep. The effectiveness of this therapy is therefore dependent upon its ability to overcome airway collapse (efficacy) as well as the time course over which a patient applies it during sleep (compliance). While the efficacy of CPAP is generally high, in the real world long-term health effects of CPAP are likely to be compromised by low compliance and suboptimal hours of treatment use. Treatment usage as a proportion of the total sleep period when a patient is vulnerable to OSA is often overlooked as a confounder of efficacy. However, treatment usage compared to sleep time is an important aspect of real-world effectiveness. Importantly, treatment effectiveness warrants consideration when comparing effects of other OSA treatment options which may not have the same level of efficacy as CPAP but may have a better usage profile. In this review we discuss efficacy and effectiveness between first line OSA treatment CPAP and the leading alternative device treatment, oral appliances.
EFFICACY VERSUS EFFECTIVENESS IN OSA
Efficacy, in the context of OSA, reflects the ability of treatment to prevent the occurrence of obstructive breathing events during periods when the treatment is being physically applied. This is assessed by the number of obstructive breathing events per hour of sleep or apnea-hypopnea index (AHI). An AHI < 5 events/h indicates absence of disease or a completely efficacious treatment. In a fully compliant patient (using treatment for 100% of sleep time) efficacy measured as AHI on treatment (AHITreatment) will give an accurate reflection of OSA treatment effectiveness. However sleep time off treatment becomes an important consideration when compliance is suboptimal. The potential impact of suboptimal CPAP compliance on AHI has been considered using formulas that adjust AHITreatment for sleep time off treatment when AHI can presumably revert to untreated levels (AHIUntreated).10,11 When the untreated portion of the night with OSA reoccurrence is taken into consideration, CPAP effectiveness can dramatically decrease depending on OSA severity and total sleep time. Good CPAP adherence is generally set at a benchmark of 4 h/night; however, the rationale for this benchmark is not overly evidence based. Moreover when taking into consideration sleep time off treatment, 4 h of CPAP use during an 8-h sleep period may only reduce the AHI by 50% due to reoccurrence of moderate OSA during the remaining 4 h without CPAP.10 In this case, the true AHI is poorly represented by AHITreatment. It has therefore been proposed that treatment comparisons should be made on overall effectiveness after adjustment of efficacy for hours of usage over total sleep time.12 In this context, although other OSA treatments such as surgery and oral appliances may be less efficacious, they offer more favorable compliance profiles (100% in the case of surgery), which may be an important determinant of the overall effectiveness, and may correlate more strongly with downstream health outcomes.
CPAP COMPLIANCE AND EFFECTIVENESS
Adequate CPAP compliance, based on reported average usage rates, is generally accepted as > 4 h on ≥ 70% if nights.13 However, even with strategies to enhance patient acceptance and usage, only ~50% of patients use CPAP ≥ 4 h per night after 6 months.14 The proportion of patients maintaining this minimally acceptable level of CPAP usage further drops to 17% after 5 years.15 Furthermore this 4-h threshold is arbitrary and not necessarily adequate to convey benefits for all important health outcomes. In reality, a dose response relationship has been observed between hours of CPAP use and a range of subjective and objective health benefits with differing benefit thresholds for different outcomes.16–18 For example, normalization of subjective sleepiness (ESS), objective sleepiness (multiple sleep latency test), and disease specific functional status (functional outcomes of sleep questionnaire [FOSQ]) requires 4, 6, and 7.5 h, respectively, of nightly CPAP usage.18 In hypertensive OSA patients, ≥ 5.6 h of CPAP usage is required to sustain a long-term reduction in blood pressure.19 CPAP usage > 6 h per night shows greatest reduction in mortality risk.20 Therefore to maximize treatment benefits for all important health outcomes, CPAP needs to be consistently used for the majority, if not all, of the sleep period. Given that this is generally not a reality for most CPAP users, there is a clear rationale for conducting comparative effectiveness trials against alternative less efficacious treatments which may still be equally effective at improving health outcomes due to higher compliance rates.
ORAL APPLIANCES IN TREATMENT OF OSA
Oral appliances are the leading device alternative to CPAP. Oral appliances cover the upper and lower dental arches and are configured so that the lower jaw is held forward in a more protruded position. The action of mandibular advancement results in an increase in pharyngeal airway space and reduces airway collapsibility.21,22 Oral appliances have a demonstrated role in improving snoring, obstructive apneas and hypopneas, and oxygen desaturation measures.23 Oral appliances also have demonstrated benefit on health outcome measures such as daytime sleepiness and blood pressure.23,24 However unlike CPAP which will prevent airway collapse in most people as long as sufficient pressure is applied, therapeutic response to oral appliance treatment shows intra-individual variability. In general terms, over a third of patients will show a complete response to oral appliance therapy with a reduction in AHI to < 5/h (or no OSA). Another third will have a clinically important response showing > 50% reduction in AHI,25 although AHI remains > 5/h and a third will not achieve > 50% reduction in AHI. There are many factors which may contribute to differences in therapeutic response to oral appliance therapy including differences in devices and treatment protocols but also craniofacial, upper airway, and obesity characteristics of the patient.25 Currently there is no validated clinical method to reliably pre-select patients who will receive sufficient benefit from oral appliance therapy from those who show minimal therapeutic response. Uncertainty around efficacy has essentially restricted oral appliance implementation to milder cases of OSA with consideration only in more severe OSA if CPAP fails.26COMPARISON OF HEALTH EFFECTS OF CPAP AND ORAL APPLIANCE THERAPY
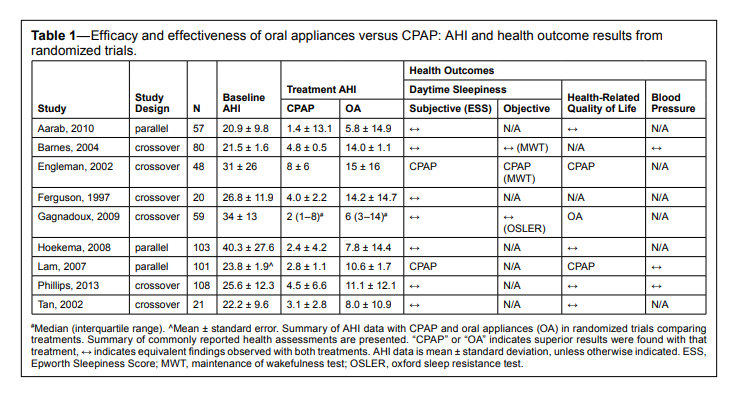
Although CPAP is clearly superior to oral appliances in terms of eliminating obstructive breathing events and improving nocturnal oxygen saturation,27 this is not the case for health outcomes. In randomized controlled trials comparing CPAP to oral appliance treatment, CPAP consistently demonstrates normalization of AHI, whereas average AHI remains in the range of mild OSA on oral appliance treatment.28–35 However the superiority of CPAP in terms of efficacy is generally not carried through to the actual health outcomes of treatment. A summary of randomized controlled trials comparing CPAP and oral appliances with commonly reported health outcomes is summarized in Table 1. Subjective daytime sleepiness, assessed by the Epworth Sleepiness Scale, does not differ following CPAP and oral appliance treatment.36 This has also been shown in objective tests of sleepiness32,37 and simulated driving performance.35,38 Furthermore, in terms of cardiovascular outcomes there is no demonstrated difference between treatments in short-term effects on blood pressure.29,34,35 In a small study both CPAP and oral appliances were found to improve endothelial function to the same degree.39 To date short-term treatment studies comparing CPAP and oral appliance overall consistently show minimal to no difference in health outcome measures despite demonstrating a higher AHITreatment with oral appliances. Longer term studies are lacking, although a recent 6-year observational study of untreated and treated (either CPAP or oral appliance) OSA patients found OSA treatment reduced the cardiovascular mortality rates regardless of whether CPAP or oral appliance treatment was used.40
Table 1Efficacy and effectiveness of oral appliances versus CPAP: AHI and health outcome results from randomized trials |
{kind=link}
A likely explanation for similarity in key health outcomes is that oral appliances are more consistently used for a greater proportion of the total sleep period, compared to CPAP. Greater usage may counterbalance the lower treatment efficacy and result in overall equivalent treatment effectiveness. Oral appliances were preferred to CPAP in four of six crossover trials asking for treatment preference at the end of the trial.30–32,35 This preference for oral appliance treatment may translate to significantly more hours of usage. A review of reported treatment times in oral appliance studies suggests usage remains at a median of 77% of nights after one year of treatment.41 However, it has been possible to objectively verify CPAP usage by data download for many years, while comparison to oral appliance usage has been limited to self-report until recently. Therefore, even though self-reported oral appliance usage appears to exceed that of objectively downloaded CPAP usage, it has been difficult to compare usage profiles between therapies. The recent advent of objective compliance monitors for oral appliances in the form of small embedded temperature-sensing chips42 now makes verification of usage patterns possible. Initial studies of objective oral appliance usage confirm good usage of > 7 hours a night in the initial 3 months of oral appliance treatment42 which is maintained at > 6 hours per night after one year.43 Furthermore the discrepancy of over an hour between subjective and objective CPAP usage13 does not seem to be apparent with oral appliance treatment, with initial studies reporting < 30 minutes difference between subjective estimates and objective data.43 Regardless, initial evidence from oral appliance compliance monitors lends support to greater usage of oral appliance therapy than CPAP.
SLEEP ADJUSTED RESIDUAL AHI (SARAH INDEX) FOR ASSESSMENT OF TREATMENT EFFECTIVENESS
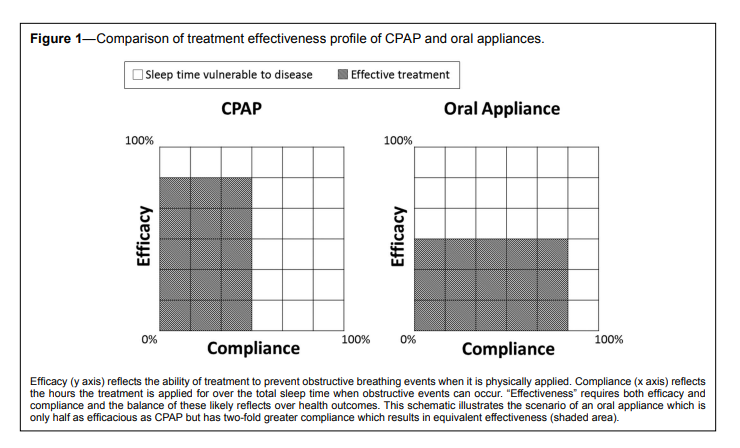
Evidence of equivalent health outcomes between oral appliances and CPAP suggest that real-world treatment effectiveness is not captured by the efficacy measure AHITreatment. However this is the metric on which clinical decisions are primarily made, although it is well recognized that CPAP is not used for all hours of sleep. The different treatment profiles of CPAP (high efficacy/low adherence) and oral appliances (moderate efficacy/high adherence) may conceptually result in similar profiles of treatment effectiveness. In the schematic in Figure 1, two identical sleep periods in which OSA can occur is represented by a grid (white boxes) for which CPAP and oral appliance are applied. Treatment effectiveness is a composite of efficacy (represented on the y axis of the grid) and hours of treatment usage (represented on the x axis). In this example MAS is only half as efficacious as CPAP, but compliance is two-fold greater. Despite these different treatment profiles, both treatments have similar overall effectiveness in relieving OSA (shaded area). This conceptual example likely reflects many patients in the real world, for whom CPAP is highly efficacious but treatment usage is modest, while oral appliances may have more modest efficacy but are used for relatively more of the sleep period. Potentially a more representative measure of treatment effectiveness than AHITreatment should also take into account hours ON treatment (AHITreatment) and hours OFF treatment (AHIUntreated) for the TOTAL sleep period. We adopt the formula of Ravesloot and colleagues,12 which accounts for these additional factors in order to assess a more accurate measure of treatment effectiveness, which we have called the Sleep Adjusted Residual AHI or SARAH Index. Potentially such an index which incorporates these currently overlooked factors could be a more accurate measure of treatment effectiveness and will better align with downstream health benefits. The formula is expressed below:[AHITreatment × HoursTreatment] + [AHIUntreated × HoursUntreated]
___________________________________________________________
HoursTotal Sleep Time
Figure 1Comparison of treatment effectiveness profile of CPAP and oral appliances. |
{kind=link}
COMPARISON OF AHI AND SLEEP ADJUSTED RESIDUAL AHI (SARAH INDEX) IN CPAP AND ORAL APPLIANCE TREATMENT
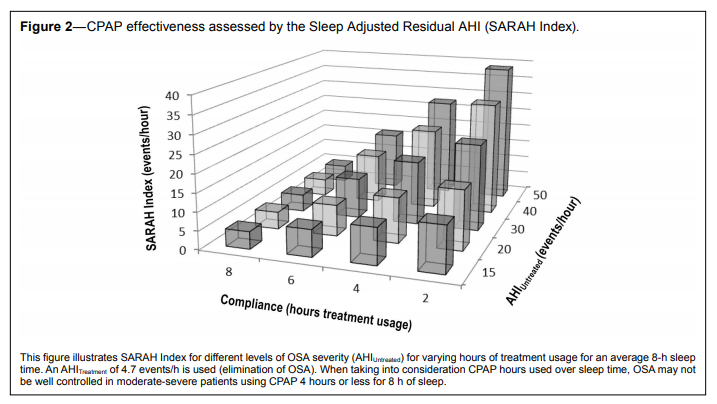
We have previously published a large cross-over study (108 completers) of one month each of optimized CPAP and oral appliance treatments.35 This study found that oral appliances were non-inferior to CPAP across a range of health outcomes in predominantly moderate-severe patients. There were no between-treatment difference in cardiovascular (24-h blood pressure, arterial stiffness), neurobehavioral (subjective sleepiness, driving simulator performance), or quality of life outcomes. In a subgroup of hypertensive patients, blood pressure during sleep reduced from baseline with both treatments, but more importantly, with no difference between them. In comparing the efficacy profiles of the two treatments, as expected, polysomnography confirmed OSA resolution on CPAP, whereas residual mild OSA was evident with oral appliance treatment (AHI 4.5 ± 6.6 vs. 11.1 ± 12.1/h). However, self-reported compliance favored oral appliances at an average 1.3 h more usage per night than CPAP. These efficacy and compliance profiles of CPAP and oral appliance treatment suggest that superior CPAP efficacy may be offset by greater oral appliance usage. We now use real data from this trial to compare AHI and SARAH Index between CPAP and oral appliance treatments across the spectrum of OSA severity.Median treatment AHI on CPAP from this trial was 4.7/h (i.e., elimination of OSA). We have used AHITreatment of 4.7/h to calculate the SARAH Index at different levels of treatment usage hours for an 8-h sleep period (healthy sleep time range44). Figure 2 shows the results from calculation of SARAH Index across a range of OSA severity (AHIUntreated). If CPAP is used for the total 8-h sleep, OSA is indeed resolved (AHI = 4.7) for all levels of OSA severity. However, it is recognized that as many as 50% of CPAP treated patients are using their treatment < 4 h of total sleep time.15 Using this example of an 8-h sleep period, the graph demonstrates that patients using their device for 4 and 2 h per night have at least mild OSA assessed by the SARAH Index, with much higher levels in those with more severe OSA. As total sleep time decreases, the SARAH Index reduces; however, for an average 8-h sleep period, the majority of CPAP users would be effectively under-treated based on known compliance rates. As CPAP usage further declines long term, CPAP treatment effectiveness may additionally become worse over time. This graph illustrates that when taking into consideration CPAP hours used over sleep time, OSA may not be well controlled, and even moderate-severe OSA may still be present in more severe and less compliant patients who sleep for longer periods. The SARAH Index calculation raises the possibility that despite high efficacy, CPAP users may not be effectively treated in practice.
Figure 2CPAP effectiveness assessed by the Sleep Adjusted Residual AHI (SARAH Index). |
{kind=link}
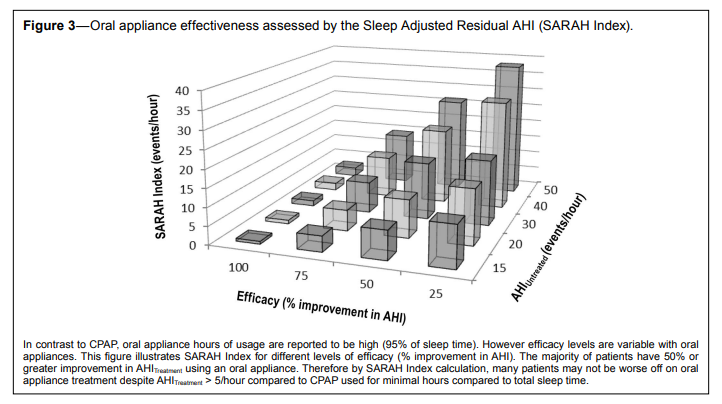
Oral appliance usage data from this same trial35 found median reported usage time to be 95% of total sleep time. We have used this 95% compliance rate to assess oral appliance treatment effectiveness by the SARAH Index. With good self-reported usage of nearly 100% of sleep time the influencing factor on treatment effectiveness for oral appliances is their efficacy, expressed as a percentage improvement in OSA from baseline levels. We show SARAH Index for different OSA severities across different levels of oral appliance efficacy of 25%, 50%, 75%, and 100% improvement in Figure 3. Oral appliance treatment effectiveness expressed by SARAH Index varies with efficacy and OSA severity. We have shown in a large audit of oral appliance treated patients that the majority (70%) will have ≥ 50% improvement in OSA using an oral appliance.45 If we compare Figures 2 and 3, CPAP and oral appliance treatment effectiveness measured by the SARAH Index, conceptually we can see that many patients may be effectively undertreated with either treatment. However, with half of all CPAP treated patients using it < 4 h per night and two-thirds of oral appliance treated patients reducing OSA by at least half, theoretically many patients with incomplete efficacy on oral appliance may be no worse off than when on fully efficacious CPAP in terms of treatment effectiveness.
Figure 3Oral appliance effectiveness assessed by the Sleep Adjusted Residual AHI (SARAH Index). |
{kind=link}
POTENTIAL CONFOUNDERS OF EFFECTIVENESS CALCULATION
Although treatment efficacy is not an adequate indicator of health benefit, effectiveness measures, such as the calculation presented as the SARAH Index, also have potential limitations. The formula assumes that OSA will return to baseline levels once treatment is removed before the end of the sleep period. Withdrawal of CPAP results in return of OSA.46–48 However, short-term carryover effects after CPAP removal may occur resulting in reduced OSA despite being without treatment. Sustained effects of CPAP may be due to an ongoing increase in pharyngeal volume and airflow due to reduced soft tissue edema as a consequence of CPAP use.49,50 The evidence for existence and duration of CPAP washout effects has been recently reviewed.51 Studies re-assessing OSA after CPAP withdrawal for several nights to weeks find lower AHI levels then recorded at baseline, potentially more evident in severe OSA patients,48 although this is not always observed.47,52,53 Regardless of baseline severity, AHI does appear to deteriorate between the first and seventh night of CPAP withdrawal.54 Furthermore, although some CPAP washout effect is observed in studies, the extent and duration is highly variable and potentially confounded by issues of night to night variability in measurement of sleep-disordered breathing.55,56 In particular, it is unknown whether such a phenomenon occurs within a single night. In terms of oral appliances, OSA levels return to baseline after a week of a placebo oral appliance (no active advancement).57 However residual effects of mandibular advancement once the lower jaw returns to normal position, or a washout effect, may be less plausible with oral appliances than CPAP.This effectiveness assessment also does not take into account differences in OSA severity due to body position and sleep stage. OSA may become more severe in the supine position and REM sleep and treatment effectiveness, particularly of oral appliances, may vary under these conditions.45 CPAP removal after several hours may leave the patient exposed to the portion of the night with more concentrated REM sleep, and hence more severe OSA. Treatment carryover effects and OSA variability due to body position and sleep stage are not captured in the simple assessment of time on versus off treatment at AHITreatment and AHIBaseline, and would be difficult to do so routinely. However, whether this approximation of effectiveness will be more clinically useful than relying only on a potentially false reassurance of AHITreatment needs further assessment. If proven to give a more reliable measure of effectiveness, another obstacle to adopting an index such as SARAH Index would be related to technological limitations with estimating sleep time in the home setting. Although the growing adoption of lifestyle wearable devices that monitor aspects of sleep may prove useful in this regard.
CONCLUSIONS AND FUTURE DIRECTIONS
Although effectiveness, as a combined measure of real world usage and efficacy, is difficult to accurately assess, proposed formulas which account for sleep time on and off treatment potentially may be a more accurate marker of health outcome responses. However this remains to be assessed in prospective trials. There is limited evidence of comparative effectiveness of CPAP and oral appliance treatments longer-term. If equivalent short-term health outcomes are found to be sustained in the long term, this opens up treatment options for patients with this chronic disease. Comparative-effectiveness and Patient-Centered Outcomes Research aims to help patients (and their healthcare providers) to make informed decisions about health and healthcare options base on outcomes that are important to them.58 We propose a greater emphasis on treatment effectiveness rather than efficacy as part of a chronic disease management approach. Future comparative effectiveness research of CPAP and Oral appliance treatment could allow patients more freedom to choose their preferred treatment over all aspects of treatment effectiveness and health outcomes.REFERENCES
2. Baldwin CM, Griffith KA, Nieto FJ, O’Connor GT, Walsleben JA, Redline S. The association of sleep-disordered breathing and sleep symptoms with quality of life in the Sleep Heart Health Study. Sleep 2001;24:96–105.
3. Gottlieb DJ, Yenokyan G, Newman AB, et al. Prospective study of obstructive sleep apnea and incident coronary heart disease and heart failure: the Sleep Heart Health Study. Circulation 2010;122:352–60.
4. Lacasse Y, Godbout C, Series F. Health-related quality of life in obstructive sleep apnoea. Eur Respir J 2002;19:499–503.
5. Marin JM, Agusti A, Villar I, et al. Association between treated and untreated obstructive sleep apnea and risk of hypertension. JAMA 2012;307:2169–76.
6. Marshall NS, Wong KK, Cullen SR, Knuiman MW, Grunstein RR. Sleep apnea and 20-year follow-up for all-cause mortality, stroke, and cancer incidence and mortality in the Busselton Health Study cohort. J Clin Sleep Med 2014;10:355–62.
7. Marshall NS, Wong KK, Phillips CL, Liu PY, Knuiman MW, Grunstein RR. Is sleep apnea an independent risk factor for prevalent and incident diabetes in the Busselton Health Study? J Clin Sleep Med 2009;5:15–20.
8. Rakel RE. Clinical and societal consequences of obstructive sleep apnea and excessive daytime sleepiness. Postgrad Med 2009;121:86–95.
9. Sassani A, Findley LJ, Kryger M, Goldlust E, George C, Davidson TM. Reducing motor-vehicle collisions, costs, and fatalities by treating obstructive sleep apnea syndrome. Sleep 2004;27:453–8.
10. Ravesloot MJ, de Vries N. Reliable calculation of the efficacy of nonsurgical and surgical treatment of obstructive sleep apnea revisited. Sleep 2011;34:105–10.
11. Stuck BA, Leitzbach S, Maurer JT. Effects of continuous positive airway pressure on apnea-hypopnea index in obstructive sleep apnea based on long-term compliance. Sleep Breath 2012;16:467–71.
12. Ravesloot MJ, de Vries N, Stuck BA. Treatment adherence should be taken into account when reporting treatment outcomes in obstructive sleep apnea. Laryngoscope 2014;124:344–5.
13. Kribbs NB, Pack AI, Kline LR, et al. Objective measurement of patterns of nasal CPAP use by patients with obstructive sleep apnea. Am Rev Respir Dis 1993;147:887–95.
14. Bartlett D, Wong K, Richards D, et al. Increasing adherence to obstructive sleep apnea treatment with a group social cognitive therapy treatment intervention: a randomized trial. Sleep 2013;36:1647–54.
15. Weaver TE, Sawyer A. Management of obstructive sleep apnea by continuous positive airway pressure. Oral Maxillofac Surg Clin North Am 2009;21:403–12.
16. Antic NA, Catcheside P, Buchan C, et al. The effect of CPAP in normalizing daytime sleepiness, quality of life, and neurocognitive function in patients with moderate to severe OSA. Sleep 2011;34:111–9.
17. Martinez-Garcia MA, Capote F, Campos-Rodriguez F, et al. Effect of CPAP on blood pressure in patients with obstructive sleep apnea and resistant hypertension: the HIPARCO randomized clinical trial. JAMA 2013;310:2407–15.
18. Weaver TE, Maislin G, Dinges DF, et al. Relationship between hours of CPAP use and achieving normal levels of sleepiness and daily functioning. Sleep 2007;30:711–9.
19. Barbe F, Duran-Cantolla J, Capote F, et al. Long-term effect of continuous positive airway pressure in hypertensive patients with sleep apnea. Am J Respir Crit Care Med 2010;181:718–26.
20. Campos-Rodriguez F, Pena-Grinan N, Reyes-Nunez N, et al. Mortality in obstructive sleep apnea-hypopnea patients treated with positive airway pressure. Chest 2005;128:624–33.
21. Chan AS, Sutherland K, Schwab RJ, et al. The effect of mandibular advancement on upper airway structure in obstructive sleep apnoea. Thorax 2010;65:726–32.
22. Ng AT, Gotsopoulos H, Qian J, Cistulli PA. Effect of oral appliance therapy on upper airway collapsibility in obstructive sleep apnea. Am J Respir Crit Care Med 2003;168:238–41.
23. Lim J, Lasserson TJ, Fleetham JA, Wright JJ. Oral applainces for obstructive sleep apnoea (Review). Cochrane Database Syst Rev 2006 Jan 25;CD004435.
24. Iftikhar IH, Hays ER, Iverson MA, Magalang UJ, Maas AK. Effect of oral appliances on blood pressure in obstructive sleep apnea: a systematic review and meta-analysis. J Clin Sleep Med 2013;9:165–74.
25. Sutherland K, Vanderveken OM, Tsuda H, et al. Oral appliance treatment for obstructive sleep apnea: an update. J Clin Sleep Med 2014;10:215–27.
26. Kushida CA, Morgenthaler TI, Littner MR, et al. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances: an update for 2005. Sleep 2006;29:240–3.
27. Giles TL, Lasserson TJ, Smith BJ, White J, Wright J, Cates CJ. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Systematic Rev 2006:CD001106.
28. Aarab G, Lobbezoo F, Hamburger HL, Naeije M. Oral appliance therapy versus nasal continuous positive airway pressure in obstructive sleep apnea: a randomized, placebo-controlled trial. Respiration 2011;81:411–9.
29. Barnes M, McEvoy RD, Banks S, et al. Efficacy of positive airway pressure and oral appliance in mild to moderate obstructive sleep apnea. Am J Respir Crit Care Med 2004;170:656–64.
30. Ferguson KA, Ono T, Lowe AA, al-Majed S, Love LL, Fleetham JA. A short-term controlled trial of an adjustable oral appliance for the treatment of mild to moderate obstructive sleep apnoea. Thorax 1997;52:362–8.
31. Ferguson KA, Ono T, Lowe AA, Keenan SP, Fleetham JA. A randomized crossover study of an oral appliance vs nasal-continuous positive airway pressure in the treatment of mild-moderate obstructive sleep apnea. Chest 1996;109:1269–75.
32. Gagnadoux F, Fleury B, Vielle B, et al. Titrated mandibular advancement versus positive airway pressure for sleep apnoea. Eur Respir J 2009;34:914–20.
33. Hoekema A, Stegenga B, Wijkstra PJ, van der Hoeven JH, Meinesz AF, de Bont LG. Obstructive sleep apnea therapy. J Dent Res 2008;87:882–7.
34. Lam B, Sam K, Mok WY, et al. Randomised study of three non-surgical treatments in mild to moderate obstructive sleep apnoea. Thorax 2007;62:354–9.
35. Phillips CL, Grunstein RR, Darendeliler MA, et al. Health outcomes of CPAP versus oral appliance treatment for obstructive sleep apnea: a randomised controlled trial. Am J Respir Crit Care Med 2013;187:879– 87.
36. Li W, Xiao L, Hu J. The comparison of CPAP and oral appliances in treatment of patients with OSA: a systematic review and meta-analysis. Respir Care 2013;58:1184–95.
37. Engleman HM, McDonald JP, Graham D, et al. Randomized crossover trial of two treatments for sleep apnea/hypopnea syndrome: continuous positive airway pressure and mandibular repositioning splint. Am J Respir Crit Care Med 2002;166:855–9.
38. Hoekema A, Stegenga B, Bakker M, et al. Simulated driving in obstructive sleep apnoea-hypopnoea; effects of oral appliances and continuous positive airway pressure. Sleep Breath 2007;11:129–38.
39. Trzepizur W, Gagnadoux F, Abraham P, et al. Microvascular endothelial function in obstructive sleep apnea: impact of continuous positive airway pressure and mandibular advancement. Sleep Med 2009;10:746–52.
40. Anandam A, Patil M, Akinnusi M, Jaoude P, El Solh AA. Cardiovascular mortality in obstructive sleep apnea treated with continuous positive airway pressure or oral appliance: an observational study. Respirology 2013;18:1184–90.
41. Ferguson KA, Cartwright R, Rogers R, Schmidt-Nowara W. Oral appliances for snoring and obstructive sleep apnea: a review. Sleep 2006;29:244–62.
42. Vanderveken OM, Dieltjens M, Wouters K, De Backer WA, Van de Heyning PH, Braem MJ. Objective measurement of compliance during oral appliance therapy for sleep-disordered breathing. Thorax 2013;68:91–6.
43. Dieltjens M, Braem MJ, Vroegop AV, et al. Objectively measured vs. self-reported compliance during oral appliance therapy for sleepdisordered breathing. Chest 2013;144:1495–502
44. Watson NF, Badr MS, Belenky G, et al. Joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society on the recommended amount of sleep for a healthy adult: methodology and discussion. Sleep 2015;38:1161–83.
45. Sutherland K, Takaya H, Qian J, Petocz P, Ng AT, Cistulli PA. Oral appliance treatment response and polysomnographic phenotypes of obstructive sleep apnea. J Clin Sleep Med 2015;11:861–8.
46. Kribbs NB, Pack AI, Kline LR, et al. Effects of one night without nasal CPAP treatment on sleep and sleepiness in patients with obstructive sleep apnea. Am Rev Respir Dis 1993;147:1162–8.
47. Rauscher H, Popp W, Wanke T, Zwick H. Breathing during sleep in patients treated for obstructive sleep apnea. Nasal CPAP for only part of the night. Chest 1991;100:156–9.
48. Young LR, Taxin ZH, Norman RG, Walsleben JA, Rapoport DM, Ayappa I. Response to CPAP withdrawal in patients with mild versus severe obstructive sleep apnea/hypopnea syndrome. Sleep 2013;36:405–12.
49. Corda L, Redolfi S, Montemurro LT, La Piana GE, Bertella E, Tantucci C. Short- and long-term effects of CPAP on upper airway anatomy and collapsibility in OSAH. Sleep Breath 2009;13:187–93.
50. Ryan CF, Lowe AA, Li D, Fleetham JA. Magnetic resonance imaging of the upper airway in obstructive sleep apnea before and after chronic nasal continuous positive airway pressure therapy. Am Rev Respir Dis 1991;144:939–44.
51. Vroegop AV, Smithuis JW, Benoist LB, Vanderveken OM, de Vries N. CPAP washout prior to reevaluation polysomnography: a sleep surgeon’s perspective. Sleep Breath 2015;19:433–9.
52. Yang Q, Phillips CL, Melehan KL, Rogers NL, Seale JP, Grunstein RR. Effects of short-term CPAP withdrawal on neurobehavioral performance in patients with obstructive sleep apnea. Sleep 2006;29:545–52.
53. Boudewyns A, Sforza E, Zamagni M, Krieger J. Respiratory effort during sleep apneas after interruption of long-term CPAP treatment in patients with obstructive sleep apnea. Chest 1996;110:120–7.
54. Phillips CL, Yang Q, Williams A, et al. The effect of short-term withdrawal from continuous positive airway pressure therapy on sympathetic activity and markers of vascular inflammation in subjects with obstructive sleep apnoea. J Sleep Res 2007;16:217–25.
55. Le Bon O, Hoffmann G, Tecco J, et al. Mild to moderate sleep respiratory events: one negative night may not be enough. Chest 2000;118:353–9.
56. Chediak AD, Acevedo-Crespo JC, Seiden DJ, Kim HH, Kiel MH. Nightly variability in the indices of sleep-disordered breathing in men being evaluated for impotence with consecutive night polysomnograms. Sleep 1996;19:589–92.
57. Mehta A, Qian J, Petocz P, Darendeliler MA, Cistulli PA. A randomized, controlled study of a mandibular advancement splint for obstructive sleep apnea. Am J Respir Crit Care Med 2001;163:1457–61.
58. Gabriel SE, Normand SL. Getting the methods right--the foundation of patient-centered outcomes research. N Engl J Med 2012;367:787–90.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication July, 2015Submitted in final revised form July, 2015
Accepted for publication August, 2015
Address correspondence to: Kate Sutherland, PhD, Department of Respiratory & Sleep Medicine, 8A, Acute Services Building, Royal North Shore Hospital, Reserve Road, St Leonards, NSW 2065 Australia; Tel: +61 2 9463 2924; Fax: +61 2 9463 2099; Email: kate.sutherland@sydney.edu.au