Review Article, Issue 2.1
Cardiovascular Benefits of Oral Appliance Therapy in Obstructive Sleep Apnea: A Systematic Review
http://dx.doi.org/10.15331/jdsm.4430
Gilles Van Haesendonck, BSc1 ; Marijke Dieltjens, MBS1,2; Chloé Kastoer, MD3 ; Bharati Shivalkar, MD, PhD1,4; Christiaan Vrints, MD, PhD1,4; Caroline M. Van De Heyning, MD, PhD1,4; Marc J. Braem, DDS, PhD1,2; Olivier M. Vanderveken, MD, PhD1,3
ABSTRACT
Study Objectives:
To perform a systematic review of the current evidence regarding the cardiovascular benefits of oral appliance (OA) therapy in obstructive sleep apnea (OSA) patients.
Methods:
A systematic review of relevant articles retrieved from online databases (PubMed, Web of Science, Medline, OvidSP) was conducted. All relevant studies published prior to January 20, 2013 that examined the effects of OA on any of the cardiovascular parameters were included.
Results:
OA therapy could have a beneficial effect on blood pressure (BP), endothelial function (EF), and left ventricular (LV) function of the heart. Eleven articles were included in this systematic review; 7 of 8 studies showed a significant reduction in BP with a mean BP decrease of 4.2 mm Hg, 2 studies showed significant improvement in EF, and 1 study showed significant improvement in LV heart function.
Conclusions:
OA therapy showed beneficial effects on the cardiovascular comorbidity in OSA patients. In studies comparing OA to CPAP therapy, effects of OA therapy were in the same order of magnitude as the effect of CPAP therapy.
Keywords:
obstructive sleep apnea, cardiovascular, oral appliance therapy, blood pressure
Citation:
Van Haesendonck G, Dieltjens M, Kastoer C, Shivalkar B, Vrints C, Van De Heyning CM, Braem MJ, Vanderveken OM. Cardiovascular benefits of oral appliance therapy in obstructive sleep apnea: a systematic review. Journal of Dental Sleep Medicine 2015;2(1):9–14.
Obstructive sleep apnea (OSA) is characterized by repetitive episodes of partial or total upper airway obstruction during sleep, resulting in a decrease of oronasal airflow.1 OSA is acknowledged as a serious health problem,2,3 and it is the most common sleep-related breathing disorder. The current prevalence estimates of moderate to severe sleep disordered breathing (apnea-hypopnea index [AHI], measured as events/ hour, ≥ 15) are 10% among 30- to 49-year-old men, 17% among 50- to 70-year-old men, 3% among 30- to 49-year-old women, and 9% among 50- to 70-year-old women.4
The pathophysiology of OSA and its effect on cardiovascular conditions has been reviewed extensively.2,5,6 During an episode of upper airway obstruction, respiratory effort against the occluded airway generates a negative intrathoracic pressure that increases left ventricular transmural pressure. The increased stress on cardiac muscle stimulates autoregulatory mechanisms that lead to thickening of the left ventricular (LV) wall over time. Negative intrathoracic pressure also increases right ventricular pressure during diastole, and the apnea-induced hypoxia causes pulmonary vasoconstriction, increasing right ventricular afterload.7 Long-term intermittent hypoxia can induce oxidative stress and activate inflammatory pathways that impair vascular endothelial function (EF).8,9 The brief arousal from sleep that accompanies apnea termination increases sympathetic activity and suppresses vagal tone. These acute effects do not only lead to oscillations in blood pressure (BP) and heart rate during sleep, but these may also result in daytime hypertension, increased heart rate during the day, and congestive heart failure.10,11 Hypertension has been found in a large group of OSA patients, and a positive correlation between BP and OSA severity has been shown.12–14 The repetitive interruptions in breathing cause sleep fragmentation associated with hypoxia and provoke overnight hypertension, leading to atrial fibrillation (AF), myocardial infarction, (MI) and sudden death.15
Continuous positive airway pressure (CPAP) is the gold standard treatment for OSA.16 However, despite its high therapeutic efficacy, CPAP is often not well tolerated by patients, resulting in low compliance rate and limited clinical effectiveness.17,18 Today, oral appliances, particularly mandibular advancement devices (OAm), are considered to be a valuable non-invasive treatment option for patients with sleep apnea and for patients who do not comply with or refuse CPAP treatment.19–23 They are worn intraorally at night in order to advance the mandible, thereby reducing the collapsibility of the upper airway.18,21,24 Studies have shown that OAm patients have been more compliant than CPAP patients. This higher compliance results in a comparable effectiveness.25–27
Gaining insight in pathophysiology and treatment of OSA becomes increasingly relevant, as OSA is a common disorder with a range of harmful sequelae. The estimated prevalence rates of OSA represent substantial increases (up to 55%) partly due to increasing awareness and the ongoing obesity epidemic.4 BP, EF, and LV function of the heart are frequently used to assess cardiovascular morbidity in association with OSA in literature.19 These objective parameters give an indication of cardiovascular changes during OAm therapy in comparison with baseline measurements, thus clarifying the possible beneficial effect of OAm therapy as an alternative for CPAP. Since the cardiovascular morbidity and mortality is an important feature in OSA, we performed a systematic review of articles studying cardiovascular changes during OAm therapy to expose the value of OAm.
METHODS
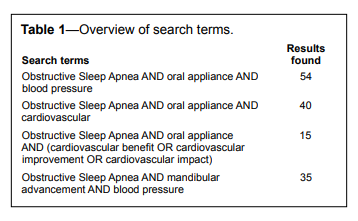
We searched 4 online databases: Pubmed, Web of Science, Medline and OvidSP. All relevant studies published prior to January 20, 2013, that examined the effects of OAm on any of the cardiovascular parameters were included. Using the results produced by the search terms listed in Table 1, a first selection was made based on the content of the title and abstract.
Table 1Overview of search terms. |
{kind=link}
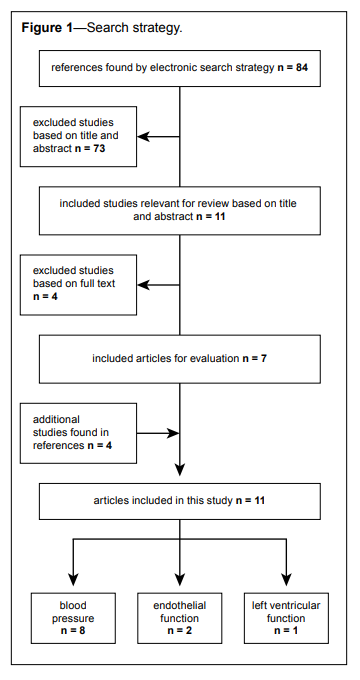
A second selection was then based on the evaluation of the content of the manuscripts. Studies that investigated noncardiovascular effects of OAm or studies that did not include any oral appliance arm were excluded. Figure 1 explains the search strategy in detail. Finally, a total of 11 studies could be included in the present review. Because the topic of this literature study is relatively new, no exclusions were made based on publication date; all studies were published after 2003.
Figure 1Search strategy. |
{kind=link}
Systematic Review
Apnea-Hypopnea Index (AHI)
One way to measure the outcome of OAm therapy is using the apnea-hypopnea index (AHI) that represents the number of apneas and hypopneas per hour of sleep. An obstructive apnea is defined as an interruption in nocturnal breathing ≥ 10 sec despite continued respiratory effort. Hypopneas are abnormal respiratory events lasting ≥ 10 sec with ≥ 30% reduction in thoracoabdominal movement or airflow, and with ≥ 4% oxygen desaturation.28 Therefore, several studies not only described the cardiovascular effect of OAm, but also the change in AHI after OAm therapy. Table 2 represents the mean AHI values of the different studies.
Table 2Summary of OAm treatment studies assessing blood pressure parameters. |
{kind=link}
Blood Pressure (BP)
As previously mentioned, there is a positive correlation between BP and OSA severity expressed in terms of AHI. The following studies investigated the effect of OAm therapy on a decrease in BP values.
In a randomized clinical trial protocol, Gotsopoulos et al.29 examined the BP of 61 patients diagnosed with OSA (AHI ≥ 10/h) before and after 4 weeks of OAm treatment. The control group was treated with an OAm without mandibular protrusion. They found a significant reduction of 24-h diastolic blood pressure (DBP) after OAm therapy in comparison to the control group, mainly due to the effect of therapy on daytime DBP. Daytime BP values with OAm were significantly lower than those of the control group: systolic blood pressure (SBP) −3.3 ± 1.1 mm Hg, DBP −3.4 ± 0.9 mm Hg and mean arterial pressure (MAP) −3.6 ± 0.9 mm Hg. The 24-h heart rate (HR) was reduced in comparison to the control group, which was caused by a daytime HR reduction of 4 ± 1 beats per minute in comparison to the control group. The BP reduction after OAm therapy was most pronounced in the early morning, when the risk of a myocardial infarction is highest.23,30
Barnes et al.31 examined 114 patients with mild to moderate OSA (5/h < AHI ≤ 30/h). In this RCT, patients were treated with CPAP, OAm, and placebo for 3 months each. Eighty patients completed all 3 treatments. Patients treated with OAm showed a significant decrease in DBP at night (−2.2 ± 0.7 mm Hg). A significant number of the patients who did not show a BP dip at night prior to treatment—a sign associated with OSA—regained this BP dip after OAm therapy. This effect was not found with placebo or CPAP treatment.
Yoshida et al.32 examined 161 patients in a non-controlled study. These patients were treated for 2 months with OAm. Their BP values before and after treatment were compared. SBP (−4.5 ± 7.4 mm Hg), DBP (−3.0 ± 6.3 mm Hg), and MAP (−3.7 ± 6.1 mm Hg) all decreased significantly during OAm therapy. MAP response significantly correlated with baseline BP and AHI reduction. These results emphasize the importance of effective OSA therapy in the treatment of high BP.
Otsuka et al.33 studied 11 patients diagnosed with OSA. In this non-controlled study, all patients were treated with OAm, and their BP values were measured before and after titration up to two-thirds of maximum mandibular protrusion. The mean time between these 2 measurements was 5.2 months. They found significant changes in 20-h BP values after OAm therapy: 20-h DBP decreased from 79.5 ± 5.5 to 74.6 ± 6.0 mm Hg, and 20-h MAP decreased from 95.9 ± 5.4 to 91.2 ± 5.9 mm Hg. The 20-h SBP did not change significantly. BP values also changed significantly during sleep: SBP decreased from 118.4 ± 10.0 to 113.7 ± 9.1 mm Hg, DBP decreased from 71.6 ± 8.0 to 67.2 ± 7.9 mm Hg, and MAP decreased from 88.4 ± 8.0 to 83.9 ± 7.5 mm Hg. In this study, there also were decreases in early morning BP values, although these daytime changes were not significant.
Andrén et al.34 examined 29 patients diagnosed with OSA in a non-controlled study. BP was measured before OAm treatment, after 3 months of treatment and after 3 years of treatment. SBP showed a decrease from 154.9 ± 20.2 before treatment to 140.6 ± 15.9 after 3 months and 139.4 ± 17.5 mm Hg after 3 years of OAm use. DBP decreased from 88.4 ± 10.1 before treatment to 79.8 ± 9.9 after 3 months and 78.1 ± 8.9 after 3 years of OAm use. The changes after 3 months and 3 years of therapy were significantly different from baseline.
Andrén et al.35 examined 70 patients diagnosed with OSA and systemic hypertension in an RCT. The study group was treated for 3 months with an OAm with mandibular protrusion and the control group with an OAm without mandibular protrusion. The 24-h BP was measured before and after treatment. BP values of the study group decreased slightly but not significantly in comparison to the control group. The greatest change was seen in the 24-h SBP, with a mean reduction of 1.8 mm Hg in comparison to the control group. The BP changes were higher after exclusion of patients with normal baseline BP and also after exclusion of patients with AHI ≤ 15/h.
In the study by Lam et al.,36 101 patients were randomized in 3 groups: an OAm group, a CPAP group and a group in which only conservative measures were taken. All patients underwent a full polysomnographic examination before and after intervention, which was maintained for 10 weeks in each group. CPAP as well as OAm decreased early morning DBP significantly in comparison to baseline values, but there was no obvious difference between these 2 groups.
Phillips et al.25 studied the BP values of 102 OSA patients. Patients were divided into 2 equal groups and treated for 1 month with either OAm or CPAP. Thereafter, a 2-week washout period was scheduled and then patients were treated for 1 month with the other therapy. The authors found a reduction in MAP after 1 month of treatment for both therapies, but there was no significant difference between them. There was no significant reduction in mean BP after 1 month of therapy. These similar results were explained by the greater efficacy of CPAP and the greater compliance with OAm therapy.
A summary of OAm treatment studies assessing BP parameters is given in Table 2. In 8 studies, BP of 590 OSA patients was monitored, with a mean BP decrease of 4.2 mm Hg during OAm therapy.
Endothelial Function
Although OSA patients may not show signs of cardiovascular disease, they do show early signs of atherosclerosis, such as endothelial dysfunction (ED), increase in intima thickness, increased carotis diameter and increased biomarkers of oxidative stress and inflammation.8,37–41 These signs are significantly correlated with OSA severity.37,39,40,42–46Itzhaki et al.47 examined oxidative stress and EF after 3 months and after 1 year of OAm therapy in a controlled study. The study group consisted of 16 patients, 12 of whom completed the 1-year evaluation. The control group consisted of 9 patients, and the study also used a reference group of 10 patients without OSA (AHI ≤ 10/h). The reactive hyperemia peripheral arterial tonometry (RH-PAT) was measured and represents EF. This value improved from 1.77 ± 0.4 to 2.1 ± 0.4 after 3 months and to 2.0 ± 0.3 after 1 year of treatment. The results under OAm therapy did not differ significantly from those of the reference group. The thiobarbituric acid-reactive substance (TBARS) also was measured, representing the oxidative stress, and was expressed in nanomole malondialdehyde per milliliter plasma. The TBARS value decreased from 18.8 ± 6.2 to 15.8 ± 3.9 after 3 months and remained at 15.5 ± 3.2 after 1 year. There was a correlation between the change in AHI, EF, and TBARS values.
Trzepizur et al.48 examined the microvascular endothelial function (MVEF) in a study group of 12 patients and a control group of 9 patients (AHI < 15/h). MVEF was measured with laser Doppler flowmetry combined with acetylcholine (ACh) and sodium nitroprusside (SNP) iontophoresis. Cutaneous vascular conductance (CVC) was expressed in AU/mm Hg. CVC values were measured before OAm and CPAP treatment and were compared to control group values and posttreatment values. Baseline CVC did not differ between the control group and the study group before OAm treatment. CVC measurements with ACh showed a significantly higher CVC peak in the control group being 3.8 multiple of baseline conductance (MBC) in comparison to the study group for OAm treatment (2.3 MBC). Correlation analysis of the study and control groups showed that ACh-induced CVC peak was negatively correlated to AHI. CVC values of the study group increased in comparison to baseline after OAm treatment. There was a significant increase in ACh-induced CVC peak after OAm treatment. An increase in SNP-induced CVC peak was also found but was not significant.
Both studies show that EF is correlated to AHI, which emphasizes the importance of an optimal treatment of OSA patients.
Left Ventricle
In patients without cardiovascular diseases, OSA is associated with an elevated incidence of both diastolic and systolic dysfunction and left ventricular hypertrophy.Hoekema et al.49 examined the left ventricle (LV) function of 28 patients with mild to moderate OSA (AHI < 20/h) before and after 2–3 months of OAm (15 patients) or CPAP (13 patients) therapy. They evaluated LV function with echocardiography and measurements of the amino-terminal fragment of the pro-brain natriuretic peptide (NT-pro-BNP). The echocardiographic values after OAm treatment were not significantly different from the values before treatment. The concentration NP, which reflects left ventricular wall stress, decreased significantly after OAm treatment; this value increased after CPAP treatment. The changes in these values suggest improved cardiac function after OAm therapy.
Less research was performed in the domain of heart function, which can be monitored by echocardiography. Only 1 study compared the left ventricle function of 15 patients before and after 2–3 months of OAm therapy.
DISCUSSION
In this article we have performed a systematic review of the current evidence regarding the cardiovascular benefits of oral appliance therapy in obstructive sleep apnea patients. After online database research we analyzed 11 relevant articles.
This systematic review demonstrates that the evolution of BP after OAm therapy is studied in detail. BP decreased significantly during OAm therapy in 7 of 8 studies. The two studies comparing OAm with CPAP therapy showed no significant difference in BP results during both therapies. The results during OAm therapy were in the same order of magnitude as after CPAP therapy.33,38 Phillips et al.25 explained these similar results by the greater efficacy of CPAP and the greater compliance with OAm therapy.32,37,38 A clear variability in treatment response rate between the 8 different studies, evaluating BP changes, can be seen in Table 2, with 34% as lowest and 75% as highest treatment response rate. This treatment response is not correlated with the baseline AHI and probably correlated with the decrease in BP. Thereby we assume that the benefit on the heart will be the greatest in optimal OSA treatment.
Less research was performed in the domain of heart function, which can be monitored by echocardiography. Only 1 study compared the left ventricle function of 15 patients before and after 2–3 months of OAm therapy,49 more extensive research in this topic would be interesting. Both articles studying EF show that EF is correlated to AHI, which emphasizes the importance of an optimal treatment of OSA patients.
In this systematic review, only 3 of 11 studies evaluated their patients after a treatment period longer than 3 months as seen in Table 2. The washout period, which is the period without OSA therapy to eliminate the effects of previous therapy, was not always documented. There are no absolute recommendations on how long OSA therapy should be employed to achieve maximal beneficial cardiac effects or how quickly the beneficial cardiac effects are reversed after discontinuation of the treatment. Cardiac evaluation of patients, with a washout period of at least 3 months and an OAm treatment period of 6 months to 1 year may be worth studying.
Following current recommendations OAm therapy is prescribed for a select group of OSA patients with an AHI < 20/h or in patients for whom CPAP does not work or is not tolerated.22 Given this recommendation, it would be interesting to study cardiovascular benefit in a patient group with an AHI ≥ 20/h or to make a subanalysis of this group. Secondly only 3 of 11 studies compared cardiovascular effects during OAm therapy with cardiovascular effects during CPAP therapy. Since the cardiovascular morbidity and mortality is an important feature in treating OSA, more evidence comparing these two different treatment modalities is necessary. Large scale studies have demonstrated that CPAP reduces the risk of fatal and non-fatal cardiovascular events in severe OSA.50,51 In an observational study, Anandam et al.52,53 examined the cardiovascular mortality in 570 patients with severe OSA treated with either CPAP or OAm. Untreated severe OSA was a strong predictor of cardiovascular death. Cardiovascular death rates of CPAP- and OAm-treated patients were similar (compared to each other) and both significantly lower than the untreated OSA patients. Although residual AHI for OAm-treated patients was significantly higher than CPAP-treated patients, there was no difference in cardiovascular death rate between the two groups. Some studies included in this review demonstrate that patients under OAm therapy report higher subjective compliance than CPAP therapy.25,36 Objective measurement of compliance of OAm therapy has become feasible using an incorporated sensor in the OAm.54 Consequently, compliance will become more accurately assessable and will become an important variable in the comparison between CPAP and OAm therapy outcome. Not only efficacy, but also compliance is an important factor in comparing different treatment modalities. The product of efficacy and compliance can be formulated as the mean disease alleviation (MDA), as described by Vanderveken et al.54 MDA can be a measure for the net effectiveness of a therapy. Even if CPAP is superior to OAm in reducing AHI, in terms of efficacy the MDA values of both CPAP and OAm therapy are in the same order of magnitude due to the higher compliance to OAm.
All this could be elucidated further by studying the cardiovascular benefits between 6 and 12 months of OAm therapy, including implementation of objective compliance measurement, as well as extensive cardiovascular follow-up of patients, and in patients with more severe OSA and in comparison with CPAP treatment.
CONCLUSIONS
The results of this concise review indicate that OAm therapy provides a beneficial effect on the cardiovascular comorbidity in OSA patients. Improvement in BP, EF, and left ventricular function are proven in several independent studies. The studies comparing OAm therapy to CPAP therapy even illustrate that the reduction in BP values after both therapies might be of the same order of magnitude. This finding contrasts with the current recommendations for OSA treatment in which OAm therapy is prescribed for a select group of OSA patients with an AHI < 20/h or in patients for whom CPAP does not work or is not tolerated and calls for further research in this field.22
REFERENCES
2. Somers VK, White DP, Amin R, et al. Sleep apnea and cardiovascular disease: an American Heart Association/American College of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council on Cardiovascular Nursing. Circulation 2008;118:1080–111.
3. Shah NA, Yaggi HK, Concato J, Mohsenin V. Obstructive sleep apnea as a risk factor for coronary events or cardiovascular death. Sleep Breath 2010;14:131–6.
4. Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol 2013;177:1006–14.
5. Bradley TD, Floras JS. Sleep apnea and heart failure: Part I: obstructive sleep apnea. Circulation 2003;107:1671–8.
6. Bradley TD, Floras JS. Obstructive sleep apnoea and its cardiovascular consequences. Lancet 2009;373:82–93.
7. Stoohs R, Guilleminault C. Cardiovascular changes associated with obstructive sleep apnea syndrome. J Appl Physiol 1992;72:583–9.
8. Dyugovskaya L, Lavie P, Lavie L. Increased adhesion molecules expression and production of reactive oxygen species in leukocytes of sleep apnea patients. Am J Respir Crit Care Med 2002;165:934–9.
9. Ryan S, Taylor CT, McNicholas WT. Selective activation of inflammatory pathways by intermittent hypoxia in obstructive sleep apnea syndrome. Circulation 2005;112:2660–7.
10. Narkiewicz K, Montano N, Cogliati C, van de Borne PJ, Dyken ME, Somers VK. Altered cardiovascular variability in obstructive sleep apnea. Circulation 1998;98:1071–7.
11. Vanderveken OM, Boudewyns A, Ni Q, et al. Cardiovascular implications in the treatment of obstructive sleep apnea. J Cardiovasc Transl Res 2011;4:53–60.
12. Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med 2000;342:1378–84.
13. Lavie P, Herer P, Hoffstein V. Obstructive sleep apnoea syndrome as a risk factor for hypertension: population study. BMJ 2000;320:479–82.
14. Nieto FJ, Young TB, Lind BK, et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study. JAMA 2000;283:1829–36.
15. Davies RJO, Belt PJ, Roberts SJ, Ali NJ, Stradling JR. Arterial bloodpressure responses to graded transient arousal from sleep in normal humans. J Appl Pysiol 1993;74:1123–30.
16. Sullivan CE, Issa FG, Berthon-Jones M, Eves L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet 1981;1:862–5.
17. Grote L, Hedner J, Grunstein R, Kraiczi H. Therapy with nCPAP: incomplete elimination of sleep related breathing disorder. Eur Respir J 2000;16:921–7.
18. Vanderveken OM. How to treat patients that do not tolerate continuous positive airway pressure. Breathe 2010;7:1–11.
19. Sutherland K, Vanderveken OM, Tsuda H, et al. Oral appliance treatment for obstructive sleep apnea: an update. J Clin Sleep Med 2014;10:215–27.
20. Marklund M, Verbraecken J, Randerath W. Non-CPAP therapies in obstructive sleep apnoea: mandibular advancement device therapy. Eur Respir J 2012;39:1241–7.
21. Schwarting S, Huebers U, Heise M, Schlieper J, Hauschild A. Position paper on the use of mandibular advancement devices in adults with sleep-related breathing disorders. A position paper of the German Society of Dental Sleep Medicine (Deutsche Gesellschaft Zahnaerztliche Schlafmedizin, DGZS). Sleep Breath 2007;11:125–6.
22. Kushida CA, Morgenthaler TI, Littner MR, et al. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances: an update for 2005. Sleep 2006;29:240–3.
23. Elliott WJ. Circadian variation in the timing of stroke onset: a meta-analysis. Stroke 1998;29:992–6.
24. Cistulli PA, Gotsopoulos H, Marklund M, Lowe AA. Treatment of snoring and obstructive sleep apnea with mandibular repositioning appliances. Sleep Med Rev 2004;8:443–57.
25. Phillips CL, Grunstein RR, Darendeliler MA, et al. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea. Am J Respir Crit Care Med 2013;187:879–87.
26. Dieltjens M, Braem MJ, Vroegop AV, et al. Objectively measured vs selfreported compliance during oral appliance therapy for sleep-disordered breathing. Chest 2013;144:1495–502.
27. Vanderveken OM, Braem MJ, Dieltjens M, De Backer WA, Van de Heyning PH. Objective measurement of the therapeutic effectiveness of continuous positive airway pressure versus oral appliance therapy for the treatment of obstructive sleep apnea. Am J Respir Crit Care Med 2013;188:1162.
28. Meoli AL, Casey KR, Clark RW, et al. Hypopnea in sleep-disordered breathing in adults. Sleep 2001;24:469–70.
29. Gotsopoulos H, Kelly JJ, Cistulli PA. Oral appliance therapy reduces blood pressure in obstructive sleep apnea: a randomized, controlled trial. Sleep 2004;27:934–41.
30. Cohen BL. Lung cancer risk from residential radon: meta-analysis of eight epidemiologic studies. J Natl Cancer Inst 1997;89:664; author reply 664–5.
31. Barnes M, McEvoy RD, Banks S, et al. Efficacy of positive airway pressure and oral appliance in mild to moderate obstructive sleep apnea. Am J Respir Crit Care Med 2004;170:656–64.
32. Yoshida K. Effect on blood pressure of oral appliance therapy for sleep apnea syndrome. Int J Prosthodont 2006;19:61–6.
33. Otsuka R, de Almeida FR, Lowe AA, Linden W, Ryan F. The effect of oral appliance therapy on blood pressure in patients with obstructive sleep apnea. Sleep Breath 2006;10:29–36.
34. Andren A, Sjoquist M, Tegelberg A. Effects on blood pressure after treatment of obstructive sleep apnoea with a mandibular advancement appliance - a three-year follow-up. J Oral Rehab 2009;36:719–25.
35. Andren A, Hedberg P, Walker-Engstrom ML, Wahlen P, Tegelberg A. Effects of treatment with oral appliance on 24-h blood pressure in patients with obstructive sleep apnea and hypertension: a randomized clinical trial. Sleep Breath 2013;17:705–12.
36. Lam B, Sam K, Mok WY, et al. Randomised study of three non-surgical treatments in mild to moderate obstructive sleep apnoea. Thorax 2007;62:354–9.
37. Lavie L, Vishnevsky A, Lavie P. Evidence for lipid peroxidation in obstructive sleep apnea. Sleep 2004;27:123–8.
38. Christou K, Moulas AN, Pastaka C, Gourgoulianis KI. Antioxidant capacity in obstructive sleep apnea patients. Sleep Med 2003;4:225–8.
39. Yamauchi M, Nakano H, Maekawa J, et al. Oxidative stress in obstructive sleep apnea. Chest 2005;127:1674–9.
40. Carpagnano GE, Kharitonov SA, Resta O, Foschino-Barbaro MP, Gramiccioni E, Barnes PJ. 8-Isoprostane, a marker of oxidative stress, is increased in exhaled breath condensate of patients with obstructive sleep apnea after night and is reduced by continuous positive airway pressure therapy. Chest 2003;124:1386–92.
41. Schulz R, Mahmoudi S, Hattar K, et al. Enhanced release of superoxide from polymorphonuclear neutrophils in obstructive sleep apnea. Impact of continuous positive airway pressure therapy. Am J Respir Crit Care Med 2000;162:566–70.
42. Imadojemu VA, Gleeson K, Quraishi SA, Kunselman AR, Sinoway LI, Leuenberger UA. Impaired vasodilator responses in obstructive sleep apnea are improved with continuous positive airway pressure therapy. Am J Respir Crit Care Med 2002;165:950–3.
43. Ip MS, Tse HF, Lam B, Tsang KW, Lam WK. Endothelial function in obstructive sleep apnea and response to treatment. Am J Respir Crit Care Med 2004;169:348–53.
44. Itzhaki S, Lavie L, Pillar G, Tal G, Lavie P. Endothelial dysfunction in obstructive sleep apnea measured by peripheral arterial tone response in the finger to reactive hyperemia. Sleep 2005;28:594–600.
45. Drager LF, Bortolotto LA, Lorenzi MC, Figueiredo AC, Krieger EM, Lorenzi-Filho G. Early signs of atherosclerosis in obstructive sleep apnea. Am J Respir Crit Care Med 2005;172:613–8.
46. Minoguchi K, Yokoe T, Tazaki T, et al. Increased carotid intima-media thickness and serum inflammatory markers in obstructive sleep apnea. Am J Respir Crit Care Med 2005;172:625–30.
47. Itzhaki S, Dorchin H, Clark G, Lavie L, Lavie P, Pillar G. The effects of 1-year treatment with a herbst mandibular advancement splint on obstructive sleep apnea, oxidative stress, and endothelial function. Chest 2007;131:740–9.
48. Trzepizur W, Gagnadoux F, Abraham P, et al. Microvascular endothelial function in obstructive sleep apnea: impact of continuous positive airway pressure and mandibular advancement. Sleep Med 2009;10:746–52.
49. Hoekema A, Voors AA, Wijkstra PJ, et al. Effects of oral appliances and CPAP on the left ventricle and natriuretic peptides. Int J Cardiol 2008;128:232–9.
50. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 2005;365:1046–53.
51. Sanders MH, Montserrat JM, Farre R, Givelber RJ. Positive pressure therapy: a perspective on evidence-based outcomes and methods of application. Proc Am Thorac Soc 2008;5:161–72.
52. Anandam A, Patil M, Akinnusi M, Jaoude P, El-Solh AA. Cardiovascular mortality in obstructive sleep apnoea treated with continuous positive airway pressure or oral appliance: an observational study. Respirology 2013;18:1184–90.
53. Vanderveken OM. Perspectives on the reduction in cardiovascular mortality with oral appliance therapy for patients with severe obstructive sleep apnoea intolerant to continuous positive airway pressure. Respirology 2013;18:1161–2.
54. Vanderveken OM, Dieltjens M, Wouters K, De Backer WA, Van de Heyning PH, Braem MJ. Objective measurement of compliance during oral appliance therapy for sleep-disordered breathing. Thorax 2013;68:91–6.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication June, 2014
Submitted in final revised form September, 2014
Accepted for publication October, 2014
Address correspondence to: Gilles Van Haesendonck, Faculty of Medicine and Health Sciences, University of Antwerp, Department of ENT, Head and Neck Surgery, Antwerp University Hospital, Wilrijkstraat 10, B-2650 Edegem, Belgium; Tel: +32 3 821 33 85; Email: gvanhaesendonck@gmail.com
DISCLOSURE STATEMENT
This was not an industry supported study. Dr. Braem has received research support from Somnomed. Dr. Vanderveken is a co-investigator for a study supported by Inspire Medical Systems Inc., and he consults for Inspire Medical Systems Inc. and for Philips Electronics B.V. He is co-promoter of a Research Grant from SomnoMed Ltd. at Antwerp University Hospital (2013–2015). His department received support in the form of free devices for a RCT with sleep position trainer in 20 patients from Nightbalance NV, Delft, the Netherlands. The other authors have indicated no financial conflicts of interest.