Review Article, Issue 1.1
The Link between Sleep Bruxism, Sleep Disordered Breathing and Temporomandibular Disorders: An Evidence-based Review
http://dx.doi.org/10.15331/jdsm.3736
Ramesh Balasubramaniam, BDSc, MS1 ; Gary D. Klasser, DMD2 ; Peter A. Cistulli, MD, PhD3 ; Gilles J. Lavigne, DDS, PhD4
ABSTRACT
The potential link between sleep bruxism (SB), sleep disordered breathing (SDB), and temporomandibular disorders (TMD) is an area of intense interest in the dental sleep medicine field. There is a growing trend among some clinicians that treatment of SDB and hence SB may alleviate TMD related signs and symptoms. However the evidence base underpinning such a move in clinical practice is questionable. To date, we do not fully understand the relationship among these three entities and whether causality actually exists. This review examines the relationship(s) between SB, SDB, and TMD with the aim of defining whether these clinical disorders are concomitant, and the nature and direction of any causal relationships, with the ultimate goal of providing advice to clinicians about what to do when they identify this clinical cluster in a given patient. This review will provide a pathway for future research endeavors, which ultimately will be of great assistance in moving the field forward in an evidence-based manner.
Keywords:
Sleep bruxism, sleep disordered breathing, upper airway resistance syndrome, obstructive sleep apnea, temporomandibular disorders, comorbidity.
Citation:
Balasubramaniam R, Klasser GD, Cistulli PA, Lavigne GJ. The link between sleep bruxism, sleep disordered breathing and temporomandibular disorders: an evidence-based review. Journal of Dental Sleep Medicine. 2014;1(1):27–37.
There has been recent interest in the relationship between sleep bruxism (SB) and sleep disordered breathing (SDB). Some clinicians have advocated assessment for possible SDB in patients with temporomandibular disorders (TMD), with an underlying assumption that patients with TMD “caused” by SB may in fact have underlying SDB. In these patients, it is recommended that treatment of SDB which is assumed to be the “cause” of SB, will resolve TMD related signs and symptoms. This review will examine the relationship between sleep bruxism (SB), sleep disordered breathing (SDB), and temporomandibular disorders (TMD), with the aim of defining whether these clinical disorders are concomitant, the nature and direction of any causal relationships, with the ultimate goal of providing advice to clinicians about what to do when they identify this clinical cluster in a given patient.
OVERVIEW OF SLEEP BRUXISM, SLEEP DISORDERED BREATHING, AND TEMPOROMANDIBULAR DISORDERS
Sleep bruxism (SB) is defined as a stereotyped movement disorder characterized by rhythmic masticatory muscle activity (RMMA) associated with tooth grinding (TG) and occasional tooth clenching.1 The definition of bruxism was recently reviewed by an international group of experts,2 and this updated definition has been adopted for the International Classification of Sleep Disorders-3, to be published online in 2013. This consensus work: (1) recognized that bruxism has two distinct circadian manifestations: sleep (indicated as sleep bruxism) or wakefulness (indicated as awake bruxism) and (2) reinforced that SB is a repetitive jaw-muscle activity characterized by clenching or grinding of the teeth and/or by bracing or thrusting of the mandible. The prevalence of selfreports of tooth grinding to assess SB is about 8%.3 The gold standard for diagnosis of SB is a polysomnogram (PSG), and a one-night study is considered adequate for the diagnosis of moderate to high frequency SB. In some cases of low RMMA frequency, a second night study may be necessary to confirm the findings of the first night.4 A recent study involving 1,042 subjects who completed a questionnaire and underwent a PSG found that, based on the questionnaire alone, the prevalence was 12.5%. With the use of PSG alone regardless of the subjects report, the prevalence was 7.4%. The prevalence of SB when the questionnaire was combined with polysomnographic recording was 5.5%.5
Interest in SB has gained more attention due to a shift in the modern day employment environment and its putative recent association to sleep disorders such as insomnia and SDB.5 The word night or nocturnal as it relates to bruxism should no longer be used, since many workers sleep during the daytime due to flexible work schedules. Therefore, SB can occur anytime during a 24-h cycle. SB can be divided into two distinct categories. They are: (1) primary or idiopathic SB, which is without an identifiable cause or any associated sociopsychological or medical problem; and (2) secondary SB, which is related to sociopsychological and/or medical conditions (e.g., movement or sleep disorder, neurologic or psychiatric condition, drug/ chemical related). Practitioners must be aware that SB may occur concomitantly with many other sleep disorders such as insomnia, sleep epilepsy, REM behavior disorder (RBD), and SDB.
The etiology of SB is most likely multifactorial—the result of a combination of environmental, biological, and psychosocial influences; however, a causal association between these factors and SB has yet to be established. The various etiological factors reported in the literature over the last half-century range from nicotine, ethanol, recreational drugs, and caffeine intake to peripheral mechanisms such as occlusal discrepancies, to a variety of central factors such as stress and psychosocial influences, alterations in catecholamine levels and other neurochemicals, and cardiac-autonomic interactions related to airway patency and salivary flow. In addition, there appears to be some minor evidence of genetic and familial predisposition for developing chronic SB.6-12 Historically, convincing arguments existed for a direct relationship between SB and occlusal factors, as early studies seemed to indicate that occlusal corrections diminished or stopped SB activity.13-15 However, later studies challenged occlusal disharmony as a principal contributing factor; several also reported that SB activity was not reduced by occlusal therapy,16-20 thereby creating doubt as to the practice of this philosophy in relation to SB. Emotional stress was another etiological factor, that at one time, was considered to be highly responsible for SB. Early studies that monitored levels of SB looked for an association with stressful events, and some found that sleep masticatory muscle activity and periodic pain were increased during stressful periods.21-23 However, recent evidence has found this association to be true only in a small percentage of the population, thus minimizing the importance of this factor.5,7,8,24-26 There is, however, some degree of consensus that many SB individuals have an anxious personality (not an anxiety disorder) and are focused on successful performance.8,27-31
Sleep disordered breathing (SDB) may have several presentations. Two commonly identified conditions are obstructive sleep apnea and upper airway resistance syndrome (UARS).32-34 Classically, the prevalence of OSA has been reported to be 2% in women and 4% in men in the general population in the US. Among 50- to 60-year olds, 4% of women and 9.1% of men have OSA.35 However, a recent study has revealed that the prevalence of SDB has been increasing in tandem with the obesity epidemic. In the US, the prevalence rate for moderate-to-severe OSA is 10% and 3% among 30- to 49-year-old men and women, respectively, and 17% and 9% among 50- to 70-year-old men and women, respectively.36
Classically, UARS is diagnosed by observation of episodes of increased respiratory effort associated with abnormal breathing pattern that does not meet the criteria for hypopnea (duration > 10 seconds and drop in nasal flow amplitude of > 30%). Hence the arousals occur without evidence of OSA and are associated with excessive daytime sleepiness. Also, the lowest oxygen saturation at termination of the abnormal breathing event is > 92%, associated with well-defined cyclical alternating patterns (CAP) related to repetitive oscillations in autonomiccardiac and EEG activities towards a rise in arousal pressure.32,37 The AASM Task Force38 has provided a proxy to the clinical definition UARS, the respiratory effort related arousal. 39 In UARS the “S” is for syndrome and mandatory for sleepiness, which is not taken into account in RERA.39 RERA is clinically associated with increased inspiratory efforts reflected by more negative esophageal pressure, terminating with alpha wave or alpha and beta wave burst-related EEG arousals.40,41 OSA involves both obstructive apnea (cessation of airflow ≥ 90% compared to baseline with a duration ≥ 10 sec associated with continued or increased inspiratory effort throughout the entire period of absent airflow) and hypopnea (a reduction in airflow ≥ 30% compared to baseline with a duration ≥ 10 sec, and with ≥ 3% oxygen desaturation compared to baseline, or an arousal).42
Patients with SDB typically have a number of physiologic traits that may explain the disorder. Typically, a small pharyngeal airway combined with reduced pharyngeal dilator muscle activation during sleep may result in obstruction. The muscle responsiveness during sleep and arousal threshold in response to respiratory stimulation determines whether the individual develops SDB. Also the stability of ventilatory control determines if the individual develops SDB. That is, if the respiratory drive is unstable, the pharyngeal dilator muscle response will also be unstable and hence promote upper airway collapse.43,44 SDB is considered a heterogeneous disorder in which anatomy is an important factor. However, in 56% of OSA subjects, nonanatomical factors such as genioglossus muscle responsiveness, arousal threshold, and respiratory control stability and loop gain contribute to the condition.45
TMD as defined by the American Academy of Orofacial Pain encompass a group of musculoskeletal and neuromuscular conditions that involve the TMJs, the masticatory muscles, and all associated tissues.46 Based on a systematic review of studies that utilized the Research Diagnostic Criteria for TMD (RDC/TMD), the prevalence of TMD in the general population is 13% for muscle pain, 16% for disk derangement, and 9% for joint pain.47 These conditions primarily occur in the young and middle-aged adults and are twice as prevalent in females in the general population.48,49 Patients with TMD typically complain of masticatory muscle and TMJ pain, limited mandibular movements, and TMJ sounds associated with masticatory functions such as chewing.46 Although the etiology of TMD remains ambiguous, microtrauma is hypothesized to be a cause. It is reported that sustained and repetitious adverse loading of the masticatory system that occurs with SB can cause TMD.50-53 Based on the underlying assumption of some clinicians that SB is related to untreated SDB, it is posited that perhaps treatment of SDB will resolve signs and symptoms of TMD.
DOES THE LITERATURE SUPPORT AN ASSOCIATION BETWEEN SLEEP BRUXISM AND SLEEP DISORDERED BREATHING?
A relationship between SB and SDB has been previously suggested54; however, it is yet to be demonstrated whether both entities are coincidental, causally related, linked to some arousal reactivity, or under some physiological state, which involves the triggering of one or the other.
Currently, there is no evidence to support the association or causality of SB and OSA. However, there do appear to be clinical commonalties between SB and OSA. SB is a complex process that may have a role in maintaining normal physiology, or is perhaps a component of pathophysiology not yet fully elucidated. However, there appears to be an association between SB and sleep position.55 Furthermore, an association among OSA, sleep position, and parafunctional activities (clenching) has been expressed in some patients.56 A link between OSA and those individuals manifesting SB is a possibility, as these entities share the common finding of an alteration in muscle activity/tone.57-59 Observation during hypercapnia (rise in CO2 level) has revealed that the genioglossus and masseter muscles increase in activity by ventilatory stimuli.58 Activation of the masseter muscle is thought to stabilize the mandible; hence enabling the genioglossus to dilate the upper airway more efficiently.57,59,60
There are a number of questions that arise due to the commonalities existing between OSA and SB. Are these commonalities related to upper airway obstruction, whereby SB may be a normal physiologic reactive-protective mechanism? If so, could SB be utilized as a reliable and valid surrogate clinical marker for OSA? A detailed exploration of these questions utilizing an evidence-based narrative review approach will address these issues.
SB and SDB are of particular interest to practitioners who are involved in treating patients with either or both of these conditions. The coexistence, perhaps coincidental in terms of epidemiology (intersecting prevalence of SB decreasing and SDB increasing with age) and physiological mechanism triggering one or the other, has been reported in a number of pediatric and adult questionnaire- and PSG-based studies. For the purpose of this discussion, the pediatric population is considered subjects under the age of 17 years.
PEDIATRIC POPULATION
An investigation of the prevalence of sleep disorders based on a questionnaire telephone survey among 6- to 12-year-old healthy school children was carried out. The prevalence of sleep signs and symptoms, reported by parents, included descriptors related to habitual snoring (10.9%), cessation of breathing (1.5%), and TG (20.5%). Of interest, significant risk factors identified for habitual snoring comprised witnessed apnea, mouth breathing, snoring among first-degree relatives, morning headache, being male, allergic rhinitis, and witnessed sleep TG. Similarly, significant risk factors for witnessed sleep apnea comprised snoring, allergic rhinitis, morning tiredness, and daytime sleepiness. Among snorers, the odds ratios (OR) for witnessed sleep teeth grinding and morning headache were 1.56 and 1.53, respectively.61A multiple-choice questionnaire study involving 1,605 children in Turkey (819 boys and 786 girls) aged 7-13 years was administered.62 Based on a 72.5% response rate, the prevalence of occasional snoring and habitual snoring was 38.9% and 3.5%, respectively. Of interest, habitual snorers had more daytime signs and symptoms (such as mouth breathing, sleepiness, headache, and hyperactivity) and nighttime signs and symptoms (such as witnessed apnea, obstructed breathing, profuse sweating, restless sleep, enuresis, and TG). Also of significance, allergies, daytime mouth breathing, “shaking the child for apnea,” restless sleep, and hyperactivity were independent risk factors for habitual snoring. The prevalence of TG was 28.7% and 34.1% and significantly associated with occasional snoring and habitual snoring respectively.62 The validity of the questionnaire used in this study was tested on 38 patients prior to the study; however, it was not reported on. It is important to note that the use of questionnaires to capture epidemiological information regarding sleep apnea has limitations and requires improvement.63
In another study involving 119 snorers between ages 3 and 16, SB was evaluated via PSG. Seventy snorers (59%) were diagnosed with SB. The apnea index, apnea-hypopnea index (AHI), and REM sleep AHI were significantly greater among SB subjects than non-bruxers. The author suggested an association between SB and pediatric OSA.64
A PSG study involving 38 consecutive children with probable obstructive sleep apnea-hypopnea syndrome (OSAHS) was carried out. Thirty-five children (92.1%) diagnosed with OSAHS had excessive sleepiness (29.4%) and SB (34.3%) based on a questionnaire. All children (n = 8) with severe OSAHS were diagnosed with bruxism.65
ADULT POPULATION
Three groups of 25 patients with SDB were assessed for signs and symptoms consistent with functional somatic syndromes. All patients were clinically evaluated and had a PSG. The study revealed over 50% of patients with UARS (AHI < 10/h) reported SB; however, this finding was not clinically significant.66 It is important to note that the diagnosis of SB was based on observation of tooth grinding by the bed partner or dentist observation of teeth wear, which are both unreliable methods of assessing SB.5A telephone survey of 13,057 subjects over the age of 15 used the International Classification of Sleep Disorders minimal set criteria to assess the epidemiology of SB. This study revealed that snoring, choking/blocked breathing, breathing pauses, and OSA were significantly associated with the diagnosis SB and TG (not meeting criteria for SB). It also noted that subjects with OSA (OR = 1.8), loud snorers (OR = 1.4), and those with moderate daytime sleepiness (OR = 1.3) were at a higher probability but lower risk (i.e., low OR) of reporting SB.8 Obvious limitations of this study include use of telephone survey to assess SB and TG, as 20% of subjects did not have a bed partner and many were edentulous. Also subjects did not undergo a dental examination and PSG, which is the gold standard for assessing SB.5
In a full PSG study of 21 adult patients suspected of having SDB, 6 of 11 mild OSA patients (54%) and 4 of 10 moderate OSA patients (40%) were diagnosed with SB. Masseter muscle contraction episodes at the termination of an apneic event was noted in 3.5% in mild and 14.4% in moderate OSA patients.67 Critically, the diagnosis of SB was based on the combination of a questionnaire, clinical observation, and EMG measurement of masticatory muscles activity. Without the use of PSG and due to the small sample size of subjects for the diagnosis of SB, it is difficult to draw inference from this study.
In a study involving 24 sleep bruxers (15 females, age 23-67 years), sleep recordings revealed that only 4 subjects had a significant number of apnea-hypopnea events. A possible explanation for the lower prevalence may be related to the large age range and the predominantly female study population.68
A cross-sectional Japanese study of 1,930 residents (age 18-89 years) via a self-administered questionnaire and clinical examination, self-report SB was noted in 8% of individuals. It was higher among individuals between ages 30 and 49 years than those older than 60 years. SB was associated with snoring (OR: 2.58, p = 0.001).69 Limitations of this study include the subjective assessment of SB and inclusion of subjects missing some or all their teeth, and it did not take into account teeth contacts from use of prosthesis.
Based on the aforementioned studies, there appears to be a coexistence of SB and SDB in both pediatric and adult populations. However, in a recent publication involving 1,042 subjects, SB was assessed based upon questionnaire and polysomnographic recordings, there was no significant association between SB and AHI and mean oxygen saturation.5 Limitations of this study include the absence of dental examination, not utilizing audio-video recording to exclude non-RMMA related facial movements, and the influence of the first-night effect. Certainly, prospective epidemiological studies utilizing PSG over several nights in large populations are warranted to further investigate the relationship between SB and SDB.
COMMON FEATURES OF SLEEP BRUXISM AND SLEEP DISORDERED BREATHING
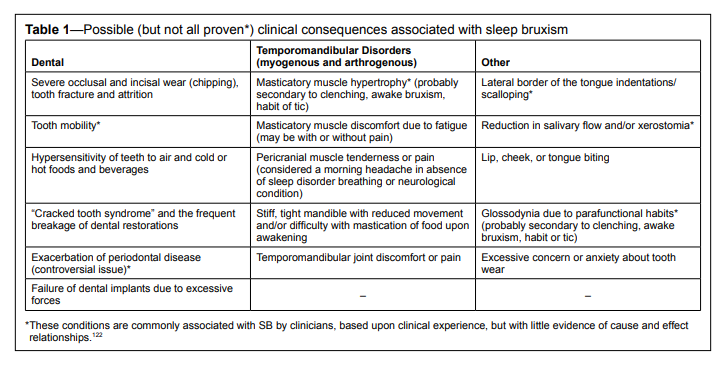
Patients suspected of SB may present to the practitioner with signs and symptoms of tooth wear or damage, fractured dental restorations, dental implant failure, tooth hypersensitivity, tongue indentation, masticatory muscle pain, TMJ pain, and tension-type headache (Table 1). As stated previously, there is uncertainty as to when SB is considered a normal physiologic behavior found in the healthy adult population or considered to be a pathophysiologic disorder highlighted by the abovementioned signs and symptoms.6 However, there appear to be common features in adult patients with SB and SDB related to sleep positions, oropharyngeal muscle activity, sleep arousal, and gastroesophageal reflux.
Table 1Possible (but not all proven*) clinical consequences associated with sleep bruxism |
{kind=link}
INFLUENCE OF SLEEP POSITION
Both OSA and SB patients spend 50% to 58% of their sleeping time in the supine position.70,71 In several studies investigating the relationship between OSA and SB, there was either no statistical significance or only a slight trend toward an increased frequency of SB episodes among OSA patients in the supine position as compared to other sleep positions (side or mixed).54,56,72,73 However, these studies did not assess the relationship between SB and UARS. Miyawaki et al.55 reported that among SB adult patients, 74% of RMMA and swallowing events occurred in the supine position compared to 23% in the lateral decubitus position, suggesting that sleep position may be a factor in the frequency of oromotor events. The authors suggested that future studies might investigate the potential of postural modification in management of SB.Based on limited studies, it appears that both SB and SDB can occur in the supine position. SB episodes do not exclusively occur in the supine position; however, studies on the effect of postural therapy on SB have not been carried out. In the case of SDB, sleep position appears to be related to the influence of gravity on the oropharyngeal tissues promoting upper airway obstruction.
OROPHARYNGEAL MUSCLE ACTIVITY
Masticatory and tongue muscle activity during sleep is thought to play an important role during SDB. In OSA the influence of gravity on the mandible, especially in the supine position, combined with masticatory and tongue muscle hypotonia results in a posterior shift of the mandible and tongue creating oropharyngeal narrowing and increased upper airway resistance. Yoshida assessed 14 adult apnea subjects and 6 snorers with PSG recordings, which included EMG of the genioglossus, masseter, and inferior lateral pterygoid muscles before, during, and after apneic events.57 The EMG amplitude was lower during an obstructive apnea event than before the event. The amplitudes were significantly higher after the apnea event. It was also found that EMG amplitude did not decrease during central apnea events. This study provided evidence that hypotonia of masticatory and tongue muscles during sleep resulted in obstructive apnea events. Other studies support the suggestion that genioglossus, submental, and masseter muscle activation in OSA patients may occur in an attempt to stabilize the mandible and prevent collapse of the upper airway.59,60,74Jaw opening at the end of inspiratory effort through submental muscle activation and tracheal tug has been shown to open the airway to allow mouth breathing; this is in contrast to jaw opening at the end of expiratory effort, which is known to narrow the airway.60 Similarly, increased distance between the tongue and posterior wall (from 11 to 17.5 mm) in subjects with neck extension in a jaw-closed position has been reported.75 These studies suggest that the combination of muscle tone and elasticity contribute to maintain the patency of the upper airway.
Based on the above studies, it appears the oropharyngeal and masticatory muscles activate and maintain tone during apneic events to maintain the patency of the upper airway. Although speculative, masticatory muscle activation during these apneic events combined with inadvertent tooth contacts may be diagnosed as SB.
SLEEP AROUSAL
A common sign of SDB is arousal from sleep after an episode of upper airway obstruction. Similarly, SB is reported to occur within a microarousal, whereby there is a cluster of arousals during an abrupt shift of 3 to 10-15 seconds in EEG activity along with increased heart rate and muscle tone. Of interest, in otherwise healthy young SB patients, there is an increase in sympathetic activity 8 minutes preceding the SB-related electromyographic (EMG) event; more specifically, RMMA. Also, as described below, 2 big breaths were observed in the physiological sequence preceding RMMA with a small but significant increase in blood pressure.76-79In a prospective age- and sex-matched controlled pilot study, SB-RMMA events in children were reported to occur with arousals in 66% of cases. Also, 40% of SB patients had significant attention and behavior problems. Of interest, light snoring was associated with only 9% of SB episodes.39 In adults, a large sample size PSG study revealed no difference in OSA between SB and non-SB subjects; however, the study found that 52% of RMMA events were associated with sleep arousal.5
An association between SB and rise in respiration within arousal has been reported in a study assessing changes in respiration of 20 young healthy SB subjects without apnea-hypopnea manifestations. The results revealed increased respiratory amplitude of 8% to 23%, four seconds before RMMA. The respiratory amplitude was 60% to 82% one second before RMMA, which is at the onset of suprahyoid muscle activity, in the window before RMMA/TG being activated. Significantly, during RMMA, respiratory amplitude is maximal (108% to 206%). A rapid return of respiratory amplitude to baseline is noted after RMMA. When arousal was associated with RMMA, the amplitude was 11 times higher than when arousal occurred without RMMA.79
In a recent study, 19 subjects (age 53.1 ± 13.7) with OSA without SB were analyzed to assess masseter muscle contractions during sleep in association with arousals and apnea-hypopnea events. Respiratory events with arousals were significantly associated with longer event duration and/or larger transient oxygen desaturation. Masseter muscle contraction increased significantly with increased duration of arousal. Of interest, the anterior tibialis muscle had a similar response pattern. The authors suggested that the muscle activity (i.e., both masseter and anterior tibialis) after respiratory events is a nonspecific motor phenomenon influenced by duration of arousals and not the presence of respiratory events.80
Arousals associated with SB and arousals associated with upper airway obstruction are well documented in the literature. It appears that in some cases these arousals are the same entity when SB is associated with upper airway obstruction, and other cases it appears to be related to a nonspecific motor phenomenon. The question remains as to the purpose of these arousals, given their association with sleep fragmentation.
GASTROESOPHAGEAL REFLUX
Similarly, gastroesophageal reflux symptoms and events are more prevalent among subjects with OSA.81-83 Current evidence suggests an association between gastroesophageal reflux and SB. It has been noted that RMMA episodes occur when esophageal pH is reduced.84,85 Interestingly, the prevalence of TMD among patients diagnosed with gastroesophageal reflux disease was 37%.86 As a proof of concept (i.e., SB stimulating salivary secretion), Ohmure et al. infused 5 mL of 0.1N HCl or saline into the esophagus of 12 healthy adult males without SB.87 It was noted that the frequency of EMG bursts, jaw muscle activation (presumptive to be RMMA) episodes, grinding noise, and RMMA/microarousal ratio was significantly higher during the 20-min period after acid infusion. Subjects who complained of heartburn did not reveal jaw muscle activation episodes 20 minutes after acid infusion, suggesting that jaw muscle activation and SB stimulate salivary secretion, thus enabling neutralization of esophageal acid.88-90 The acidic reflux content is thought to be cleared by a protective response involving arousal and swallowing to prevent mucosal injury and aspiration.91,92ASSOCIATION BETWEEN TEMPOROMANDIBULAR DISORDERS AND SLEEP DISORDERED BREATHING
It is likely that patients with low-frequency SB may present with painful TMD. Given that there is a relationship between SB and SDB, TMD may be diagnosed in patients with SDB. Petit et al.93 evaluated 100 adult patients diagnosed with OSA and found 2% of patients had significant signs and symptoms of TMD. In another study, Cunali et al.94 evaluated 87 adult patients with mild to moderate OSA and found 52% had TMD based on the RCD/TMD.The OPPERA cohort and case-control studies found that signs and symptoms of OSA were associated with occurrence of TMD. In the cohort study, high probability of OSA was associated with increased incidence of first-onset TMD (adjusted hazard ratio = 1.73). Similarly, in the case-control study, high probability of OSA was associated with increase of chronic TMD (adjusted OR = 3.63).95 Further studies utilizing large case-control designs are warranted to explore the relationship between TMD and SDB.
In a large case-control study involving a web-based registry of 1,511 adult TMD patients, approximately 10% of TMD patients had OSA, although this was not significantly different from controls.96 In another study utilizing the Douglass disorders questionnaire, 6% of 100 adult TMD patients had OSA compared to 4% of 100 age- and sex-matched controls, which was not clinically different.97 Of note, excessive daytime sleepiness was more frequent among masticatory myofascial pain patients.98
In a 3-month prospective study, 51 adult TMD patients were assessed by PSG, Beck Depression Index, and Brief Pain Inventory. The study revealed a trajectory increase in daily pain rating predicted by the presence of SDB. The authors postulated that treatment of SDB may minimize pain and suffering.99 Similarly, in a study assessing sleep disorders and their association with pain sensitivity, 53 masticatory myofascial pain adult patients were assessed: 43% had two or more sleep disorders such as insomnia and OSA; 28% of these patients were diagnosed with OSA. The author concluded that TMD patients complaining of sleep disturbances should have a sleep study.100
A commonly cited etiology for masticatory myofascial pain is SB. In a study involving 2-night PSG monitoring, 124 female patients with masticatory myofascial pain and 46 female controls, did not find a statistical significant difference in SB rates among patients (9.7%) and controls (10.9%). Of interest, self-reported rates for SB was 55.3% among masticatory myofascial pain cases compared to 15.2% among controls, hence bringing into question the validity of self-report of SB in clinical practice.101 However, further analysis of this study revealed that TMD patients have increased daytime dysfunction, increased sleep stage N1 percentage, increased RERA, and increased respiratory arousal index compared to controls. The authors concluded that TMD is associated with sleep disturbances and mild sleep breathing dysfunction.102 As discussed previously, a recent study did not report a significant association between SB and AHI and mean oxygen saturation.5
A similar study compared jaw-muscle EMG activity utilizing portable single-channel device for 4 nights in patients with craniofacial pain, pain-free conditions, tension-type headache, and healthy controls. There was no significant difference in EMG activity among the 4 groups. Of interest, pain related conditions had significantly greater night-to-night variability. It is important not to confuse the presence of jaw muscle EMG activity as diagnostic of SB-RMMA events as discussed previously.103
In a recently accepted paper for publication in the Journal of Sleep Research, PSG recordings of 10 patients with both OSA and SB were analyzed. Reportedly, significantly more SB-RMMA events followed the apnea-hypopnea events (i.e., occurred after the respiratory event [55%]), suggesting that SB-RMMA events occurring close to apnea-hypopnea events are a secondary form of sleep bruxism.104
Although speculative, underlying sleep disturbances and SDB may be associated with SB and to a lesser degree to TMD. On balance of the available literature, this relationship is equivocal. Also, oral parafunctional activity (SB) may not be the etiology for TMD as traditionally assumed. Further research is required to better elucidate these relationships.
MANAGEMENT OF SB AND ITS EFFECTS ON SLEEP DISORDERED BREATHING
The effect of SB treatment and its influence on SDB has been noted in a few studies. The notion that SB serves as a reactiveprotective mechanism against upper airway collapse has been posited in the past.8,31,79,105,106 It is common dental practice to utilize oral appliance therapy when treating SB; however, its effect on SDB remains an enigma.Twenty-eight moderate-to-severe SB adult subjects were treated with a thermoplastic mandibular advancement appliance (MAA) at 75% advancement and assessed by Bite Strip (EMG electrodes) for 30 days. Owing to limitation of the recording method (low specificity for RMMA from other orofacial motor activities), significant improvement of masseter muscle activity was observed and responses based on the Sleep Assessment Questionnaire were noted (p < 0.05). Also there was significant reduction of TMJ sounds and masseter muscle and temporalis muscle tenderness.107 The reliability of the use of Bite Strip for assessing SB over recorded masseter muscle activity is questionable, as its use has not been fully validated by independent investigators.
In a short term PSG, randomized, crossover, controlled but experimental study (not designed to asses efficacy), 13 adult SB subjects were fitted with a temporary thermoplastic custom fit MAA in 3 different positions: with freedom of movement, slightly advanced (< 40%), or more advanced (> 75%). The maxillary occlusal splint (MxOS-no advancement of the mandible) was used as the control device. The results revealed a 42% reduction in SB episodes per hour with the MxOS. The MAA in the freedom, < 40%, and > 75% advancement positions revealed 44%, 77%, and 83% reduction in SB episodes per hour, respectively. The authors hypothesized that the mechanism at which MAA reduces SB may be related to the dimension and configuration of the device, presence of pain, reduced freedom of movement, or upper airway patency.108
A subsequent experimental study from the same group was carried out in adult subjects randomized in a crossover, shortterm study among 3 groups—25% protrusion of the MAA, 75% protrusion of the MAA, or mandibular occlusal splint (MdOS). The aim was to investigate the effect of a custom fitted adjustable MAA on SB. Mean SB episodes per hour significantly were reduced by 39% and 47% with the MAA at 25% and 75% protrusion, respectively (p < 0.04), during a one-night PSG. The MdOS reduced the mean SB episodes by 34%; however, this was not statistically significant (p < 0.07). The authors concluded that short-term use of a reinforced MAA resulted in reduction of SB motor activity. Thus MAA may be a treatment option for patients with concomitant SB and SDB.109
In another short-term PSG study, 16 adolescents with SB, snoring, and headache underwent MAA therapy. PSGs were carried out at baseline and 3 positions (without connectors between upper and lower portions, maximum intercuspation, and 50% mandibular advancement) for 1 week in random order. Short-term use of a MAA reduced SB, snoring, and headache.110 Further investigation is necessary to assess the long-term effectiveness and safety of the MAA in adolescents with SB, SDB, and headache.
A pilot study involving 10 adult patients with snoring and OSA was carried out to assess the effects of MxOS on sleep. There was no statistical difference in median AHI62 between baseline and MxOS use at night. Of interest, 4 patients had aggravation of OSA with the use of the MxOS. Five of 10 of subjects had a 50% increase in AHI. Overall, the respiratory disturbance index (RDI) demonstrated a 30% increase when the MxOS was used at night. The split-night study showed a 40% increase in sleeping time with snoring. The authors suggested that patients who are candidates for oral appliances should be questioned about snoring and OSA prior to recommending oral appliance therapy.111
In a randomized, crossover, controlled study, 10 adult patients with snoring and OSA underwent 3 PSG recordings with their MxOS and 3 PSG recordings without their MxOS. There was a small increase in the mean AHI with MxOS, which was significantly higher than without MxOS. However, there was no difference in the Epworth Sleepiness Scale score. The authors concluded that MxOS was associated with OSA aggravation; however, the small size of the study limits its clinical relevance. It was suggested that the mechanism for increase AHI with MxOS could be related to reduced tongue space and rotation and anterior translation of the condyles, which consequently reduces the upper airway size.112 Further studies with larger sample sizes are warranted. Also the effect of the MdOS on snoring and OSA needs to be investigated.
It is routine for practitioners to increase the vertical dimension for certain dental procedures. For example, oral appliances are used in dental practices often to treat patients with SB, TMD, and as an interim for dental rehabilitation. These procedures modify the space between maxillary and mandibular occlusal surfaces. Eighteen mild to severe adult OSA (AHI 5 to 45) patients completed a study assessing the effect of increasing the vertical dimension by 6 mm (interincisal) with MAA without protrusion and its effects on AHI. Increase of the AHI was noted in 9 patients, with 2 patients reaching statistical significance. The authors concluded that increasing the vertical dimension without mandibular protrusion might aggravate OSA in some patients. Therefore practitioners should screen patients for OSA prior to fabricating an oral appliance, which increase the vertical dimension without mandibular protrusion.113
Based on the above-mentioned studies, it appears that MAA is more efficacious than a non-protruding conventional oral appliance in reducing SB. However, the mechanism for this reduction may not be related only to improvement in airway patency. Also, the short-term studies assessing the use of MxOS in SB suggest that this type of oral appliance may increase AHI in subjects with OSA, although the increase in AHI may not be clinically significant. Caution is advised when drawing conclusions from the above studies, as oral appliances may independently improve both SB and SDB; hence a causal relationship cannot be assumed. The effects of other non-dental treatments for OSA such as CPAP therapy and its effects on SB would provide better insight on whether such a relationship exists.
MANAGEMENT OF TEMPOROMANDIBULAR DISORDERS AND ITS EFFECTS ON SLEEP DISORDERED BREATHING
Twelve adult subjects with complaints of morning headache but without SBD and SB history were studied. Subjects underwent 4 PSG studies; a habituation study, a baseline study, neutral position MAA study, and 50% advancement MAA study. Both the neutral MAA and 50% MAA were associated with ≥ 70% morning headache reduction and ≥ 42% orofacial pain reduction (p < 0.01). Also RMMA was significantly reduced with both the neutral MAA and 50% MAA (p < 0.05). Two subjects without previous SDB complaints had AHI > 5. Both subjects had beneficial reduction of AHI with 50% MAA. One subject with an initial AHI of 5.3 had reduction of the AHI to 2 with the use of both the neutral MAA and 50% MAA. Perhaps the neutral MAA was sufficient to prevent the retruded jaw position that typically occurs during sleep; however, this remains to be proven. The authors concluded that the reductions in orofacial pain and morning headache may partially be linked to reduction in RMMA; however, this cannot be assumed as the only explanation for a causal link.114 Certainly, further studies on orofacial pain and headache patients with mild SDB are warranted, as a recent study reported an increase in the presence of RERA among female TMD subjects.102NON-DENTAL THERAPIES FOR SLEEP DISORDERED BREATHING AND ITS EFFECTS ON SLEEP BRUXISM
Continuous positive airway pressure (CPAP) is the gold standard treatment for snoring and OSA.115 In a published case report, a 47-year-old male with severe SB and severe OSA (RDI = 47.6) was observed before and after CPAP therapy. Sixty-seven SB-related motor activity events (RMMA with TG sounds) were induced by apnea/hypopnea events, and only 6 occurred spontaneously. With CPAP, the RDI decreased to 4.1 and SB was undetectable. It was suggested that in a patient with severe SB and OSA, where oral appliance therapy is contraindicated, that CPAP may be an effective therapy in managing both conditions.116 Of interest, in patients with SB and SDB, perhaps the use of CPAP may be adequate, and hence there may be no need for the use of an occlusal splint to protect teeth from wear. Obviously, large sample size randomized controlled trials are needed to further investigate such a suggestion.In an open label study, the records of 571 adult CPAP treated patients were reviewed. One hundred thirty nine patients (24%) were identified as sleep bruxers, based on a history of tooth grinding and examination of tooth wear.117 Of note, two recent publications raised concerns about tooth grinding diagnosis by history and clinical examination alone in absence of sleep recording, whereby the history of tooth grinding and the clinical estimations were inaccurate.5,118 That is, not all subjects that report tooth grinding based on history alone, were found to have SB during a PSG. The interest in this open study is the use of esophageal pressure to monitor UARS, which would be otherwise missed, given that SB is postulated to reduce airway obstruction. Of 95 SB patients who presented for follow-up, 69 used CPAP (56 nightly). SB identified by history and examination alone was improved in 35 patients (50%). In the absence of RMMA index to diagnose SB, strong conclusions cannot yet be drawn. Also SB-RMMA and tooth grinding sounds are known to have night-to-night variability, a factor to consider during data interpretation.119
In a retrospective study by the same researchers of the abovereported study, the records of 729 CPAP treated adult patients were reviewed. The authors identified 102 OSA/UARS patients by PSG and esophageal pressure monitoring and SB patients via the history and examination alone. Also CPAP compliance was assessed based on patient self-report. A multivariate analysis revealed statistically significant relationships between CPAP use and improvement in SB (p = 0.0054). Of interest, 25 patients had UARS, of whom 14 used CPAP nightly. Of these patients, 12 patients (86%) had improvement in SB. Also, the authors believe that esophageal pressure monitoring is essential to assess UARS, as SB may mask upper airway obstruction. Otherwise, RERA will not be identified and the threshold for the RDI may not be reached to identify underlying UARS or OSA. This study observed that using CPAP to treat OSA, i.e., maintenance of airway patency, also resulted in decreased SB.106 Significant limitations in this study are related to the assessment of SB being based solely upon history and examination, and RMMA not directly measured but rather assumed to have occurred. Also the temporal association between RMMA and decrease in AHI needs to be closely analyzed for individual subjects before firm conclusions can be drawn about such stimulating findings.
Another unexplored avenue is the benefit and efficiency of upper airway surgery to manage snoring and OSA in cases with SB. The incidence of SB was assessed in a study before and after adenotonsillectomy in children with SDB. Sixty-nine children with tonsillar hyperplasia and SDB were provided a questionnaire and examination to determine the presence of SDB and SB before and after surgery.120 All 69 children were noted to have OSA, and 45.6% presented with SB. At 3-month follow-up, OSA was resolved in all patients, and only 11.8% continued to have SB. The authors concluded that there is a “positive correlation” between SDB and SB and noted that SB was associated with airway obstruction in children. A major limitation of this study is that SDB and SB were assessed by unvalidated questionnaire and examination. Also, it is unclear if observation of tooth grinding sounds and tooth wear were utilized as the method for assessing SB. Similar concerns are raised on the diagnosis of SDB, as PSG was not performed.120
In another study, 140 children (aged 4-12 years) were evaluated for obstructive symptoms secondary to adenotonsillar hypertrophy pre- and post-adenotonsillectomy. The prevalence of SB based on a questionnaire completed by observant parents was 25.7% and 7.1% pre- and post-surgery, respectively. The authors concluded that SB-tooth grinding improved with adenotonsillectomy.121 It is obvious that blind and randomized assessments are needed before firm conclusions can be drawn from these two studies. Moreover, studies regarding the benefits and efficacy of mandibular advancement (orthognathic) surgery and palatal expansion surgery in teenagers and adults with SDB and SB are scarce. The effect of treatment on SB, SDB, and TMD is summarized in Table 2.
Table 2Effect of treatment on sleep bruxism, sleep disordered breathing, and temporomandibular disorders |
{kind=link}
CONCLUSION
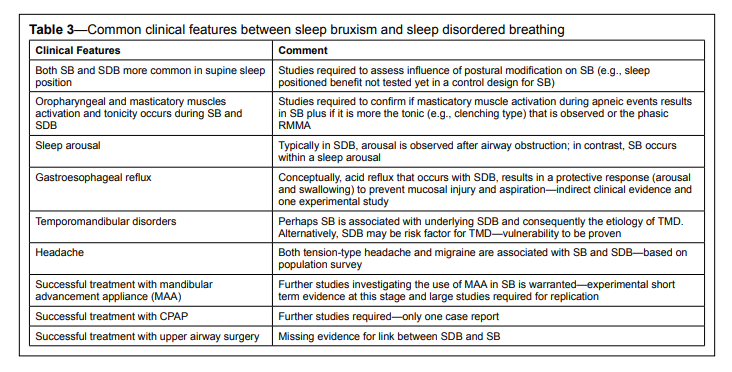
It appears that SB and SDB often coexist (Table 3). Both entities appear to share common risk factors, with intersecting prevalences across the life span, and clinical features that influence their clinical presentation. Hence this may challenge the clinical decision-making for diagnosis, comorbidities, and management of SB and SDB. The clinician has to be cautious in assuming causality just because treatment of SDB improves SB-TG in some patients. Individual differences in the era of personalized medicine prevent us from rapidly concluding on cause-and-effect relationships to be generalized to the whole population.
Table 3Common clinical features between sleep bruxism and sleep disordered breathing |
{kind=link}
Vulnerability or predisposition to SDB and SB, respectively, needs to be identified, as indirect evidence is now emerging that perhaps SB may serve as a “reactive or protective mechanism” against upper airway obstruction. It appears that when patients with SB and/or painful TMD complain about insomnia, snoring and/or cessation of breathing during sleep, sleepiness of unidentified causes, or uncontrolled blood pressure, it is prudent to screen for the presence of SDB. Such is done in collaboration with sleep medicine specialists using either sleep laboratory or home recording systems with electromyography analysis of masseter/temporal muscle activity.
In patients with confirmed SB and concomitant SDB, after nasal examination to exclude obstruction, either a MMA or CPAP may be prescribed. The same is also suggested for TMD patients with SDB. Dentists need to be aware that current standard maxillary oral appliances (occlusal splints) to protect teeth from attrition may not be appropriate treatment in the presence of SDB. That is, in some cases, occlusal splints may aggravate the underlying SDB. Also, in some cases, MAA may initiate or aggravate preexisting painful TMD in patients with SDB. Further prospective studies looking at the relationship between SB and SDB, and painful TMD and SDB are warranted before it may be translated into clinical guidelines and standards of practice.
REFERENCES
2. Lobbezoo F, Ahlberg J, Glaros AG, et al. Bruxism defined and graded: an international consensus. J Oral Rehabil 2013;40:2-4.
3. Lavigne GJ, Montplaisir JY. Restless legs syndrome and sleep bruxism: prevalence and association among Canadians. Sleep 1994;17:739-43.
4. Hasegawa Y, Lavigne G, Rompre P, Kato T, Urade M, Huynh N. Is there a first night effect on sleep bruxism a sleep laboratory study. J Clin Sleep Med 2013;9:1139-45.
5. Maluly M, Andersen ML, Dal-Fabbro C, et al. Polysomnographic study of the prevalence of sleep bruxism in a population sample. J Dent Res 2013;92:97S-103S.
6. Lavigne GJ, Khoury S, Abe S, Yamaguchi T, Raphael K. Bruxism physiology and pathology: an overview for clinicians. J Oral Rehabil 2008;35:476-94.
7. Manfredini D, Lobbezoo F. Role of psychosocial factors in the etiology of bruxism. J Orofac Pain 2009;23:153-66.
8. Ohayon MM, Li KK, Guilleminault C. Risk factors for sleep bruxism in the general population. Chest 2001;119:53-61.
9. Ahlberg J, Savolainen A, Rantala M, Lindholm H, Kononen M. Reported bruxism and biopsychosocial symptoms: a longitudinal study. Community Dent Oral Epidemiol 2004;32:307-11.
10. Lavigne GL, Lobbezoo F, Rompre PH, Nielsen TA, Montplaisir J. Cigarette smoking as a risk factor or an exacerbating factor for restless legs syndrome and sleep bruxism. Sleep 1997;20:290-3.
11. Hojo A, Haketa T, Baba K, Igarashi Y. Association between the amount of alcohol intake and masseter muscle activity levels recorded during sleep in healthy young women. Int J Prosthodont 2007;20:251-5.
12. Abe Y, Suganuma T, Ishii M, et al. Association of genetic, psychological and behavioral factors with sleep bruxism in a Japanese population. J Sleep Res 2012;21:289-96.
13. Ramfjord SP. Bruxism, a clinical and electromyographic study. J Am Dent Assoc 1961;62:21-44.
14. Ash MM, Ramfjord SP. Occlusion. 4th ed. Philadelphia: W.B. Saunders, 1995.
15. Guichet NE. Occlusion: a teaching manual. Anaheim: The Denar Corporation, 1977.
16. Rugh JD, Barghi N, Drago CJ. Experimental occlusal discrepancies and nocturnal bruxism. J Prosthet Dent 1984;51:548-53.
17. Kardachi BJ, Bailey JO, Ash MM. A comparison of biofeedback and occlusal adjustment on bruxism. J Periodontol 1978;49:367-72.
18. Tsukiyama Y, Baba K, Clark GT. An evidence-based assessment of occlusal adjustment as a treatment for temporomandibular disorders. J Prosthet Dent 2001;86:57-66.
19. Clark GT, Tsukiyama Y, Baba K, Watanabe T. Sixty-eight years of experimental occlusal interference studies: what have we learned? J Prosthet Dent 1999;82:704-13.
20. Manfredini D, Visscher CM, Guarda-Nardini L, Lobbezoo F. Occlusal factors are not related to self-reported bruxism. J Orofac Pain 2012;26:163-7.
21. Rugh JD, Solberg WK. Electromyographic studies of bruxist behavior before and during treatment. J Calif Dent Assoc 1975;3:56-9.
22. Solberg WK, Clark GT, Rugh JD. Nocturnal electromyographic evaluation of bruxism patients undergoing short term splint therapy. J Oral Rehabil 1975;2:215-23.
23. Clark GT, Beemsterboer PL, Solberg WK, Rugh JD. Nocturnal electromyographic evaluation of myofascial pain dysfunction in patients undergoing occlusal splint therapy. J Am Dent Assoc 1979;99:607-11.
24. Pierce CJ, Chrisman K, Bennett ME, Close JM. Stress, anticipatory stress, and psychologic measures related to sleep bruxism. J Orofac Pain 1995;9:51-6.
25. Dao TT, Lavigne GJ, Charbonneau A, Feine JS, Lund JP. The efficacy of oral splints in the treatment of myofascial pain of the jaw muscles: a controlled clinical trial. Pain 1994;56:85-94.
26. Watanabe T, Ichikawa K, Clark GT. Bruxism levels and daily behaviors: 3 weeks of measurement and correlation. J Orofac Pain 2003;17:65-73.
27. Lavigne GJ, Manzini C, Kato T. Sleep bruxism. In: Kryger MH, Roth T, Dement WC, eds. Principles and practice of sleep medicine. Philadelphia: Elsevier, 2005.
28. Biondi M, Picardi A. Temporomandibular joint pain-dysfunction syndrome and bruxism: etiopathogenesis and treatment from a psychosomatic integrative viewpoint. Psychother Psychosom 1993;59:84-98.
29. Kampe T, Tagdae T, Bader G, Edman G, Karlsson S. Reported symptoms and clinical findings in a group of subjects with longstanding bruxing behaviour. J Oral Rehabil 1997;24:581-7.
30. Pingitore G, Chrobak V, Petrie J. The social and psychologic factors of bruxism. J Prosthet Dent 1991;65:443-6.
31. Bader GG, Kampe T, Tagdae T, Karlsson S, Blomqvist M. Descriptive physiological data on a sleep bruxism population. Sleep 1997;20:982-90.
32. Terzano MG, Parrino L, Sherieri A, et al. Atlas, rules, and recording techniques for the scoring of cyclic alternating pattern (CAP) in human sleep. Sleep Med 2001;2:537-53.
33. Guilleminault C, Stoohs R, Clerk A, Simmons J, Labanowski M. From obstructive sleep apnea syndrome to upper airway resistance syndrome: consistency of daytime sleepiness. Sleep 1992;15:S13-6.
34. Guilleminault C, Stoohs R, Clerk A, Cetel M, Maistros P. A cause of excessive daytime sleepiness. The upper airway resistance syndrome. Chest 1993;104:781-7.
35. Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med 1993;328:1230-5.
36. Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol 2013 Apr 14 [Epub ahead of print].
37. Bao G, Guilleminault C. Upper airway resistance syndrome--one decade later. Curr Opin Pulm Med 2004;10:461-7.
38. Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. Sleep 1999;22:667-89.
39. Herrera M, Valencia I, Grant M, Metroka D, Chialastri A, Kothare SV. Bruxism in children: effect on sleep architecture and daytime cognitive performance and behavior. Sleep 2006;29:1143-8.
40. Guilleminault C, Stoohs R, Kim YD, Chervin R, Black J, Clerk A. Upper airway sleep-disordered breathing in women. Ann Intern Med 1995;122:493-501.
41. Black JE, Guilleminault C, Colrain IM, Carrillo O. Upper airway resistance syndrome. Central electroencephalographic power and changes in breathing effort. Am J Respir Crit Care Med 2000;162:406-11.
42. Berry RB, Brooks R, Gamaldo CE, Harding SM, Marcus CL, Vaughn BV. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications. Version 2.0.1. www.aasmnet.org. Darien, IL: American Academy of Sleep Medicine, 2013.
43. White DP. Pathogenesis of obstructive and central sleep apnea. Am J Respir Crit Care Med 2005;172:1363-70.
44. Eckert DJ, Malhotra A. Pathophysiology of adult obstructive sleep apnea. Proc Am Thorac Soc 2008;5:144-53.
45. Eckert DJ, White DP, Jordan AS, Malhotra A, Wellman A. Defining phenotypic causes of obstructive sleep apnea: identification of novel therapeutic targets. Am J Respir Crit Care Med 2013;188:996-1004.
46. Leeuw Rd, Klasser GD, American Academy of Orofacial Pain. Orofacial pain: guidelines for assessment, diagnosis, and management. 5th ed. Quintessence Pub Co, 2013.
47. Manfredini D, Guarda-Nardini L, Winocur E, Piccotti F, Ahlberg J, Lobbezoo F. Research diagnostic criteria for temporomandibular disorders: a systematic review of axis I epidemiologic findings. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;112:453-62.
48. LeResche L. Epidemiology of temporomandibular disorders: implications for the investigation of etiologic factors. Crit Rev Oral Biol Med 1997;8:291-305.
49. Kohler AA. On temporomandibular disorders. Time trends, associated factors, treatment need and treatment outcome. Swed Dent J Suppl 2012:8 p preceding 11-119.
50. Carlsson GE, Egermark I, Magnusson T. Predictors of signs and symptoms of temporomandibular disorders: a 20-year follow-up study from childhood to adulthood. Acta Odontol Scand 2002;60:180-5.
51. Camparis CM, Siqueira JT. Sleep bruxism: clinical aspects and characteristics in patients with and without chronic orofacial pain. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:188-93.
52. Ahlberg K, Ahlberg J, Kononen M, Alakuijala A, Partinen M, Savolainen A. Perceived orofacial pain and its associations with reported bruxism and insomnia symptoms in media personnel with or without irregular shift work. Acta Odontol Scand 2005;63:213-7.
53. Johansson A, Unell L, Carlsson GE, Soderfeldt B, Halling A. Risk factors associated with symptoms of temporomandibular disorders in a population of 50- and 60-year-old subjects. J Oral Rehabil 2006;33:473-81.
54. Okeson JP, Phillips BA, Berry DT, Cook YR, Cabelka JF. Nocturnal bruxing events in subjects with sleep-disordered breathing and control subjects. J Craniomandib Disord 1991;5:258-64.
55. Miyawaki S, Lavigne GJ, Pierre M, Guitard F, Montplaisir JY, Kato T. Association between sleep bruxism, swallowing-related laryngeal movement, and sleep positions. Sleep 2003;26:461-5.
56. Phillips BA, Okeson J, Paesani D, Gilmore R. Effect of sleep position on sleep apnea and parafunctional activity. Chest 1986;90:424-9.
57. Yoshida K. A polysomnographic study on masticatory and tongue muscle activity during obstructive and central sleep apnea. J Oral Rehabil 1998;25:603-9.
58. Hollowell DE, Bhandary PR, Funsten AW, Suratt PM. Respiratoryrelated recruitment of the masseter: response to hypercapnia and loading. J Appl Physiol 1991;70:2508-13.
59. Hollowell DE, Suratt PM. Activation of masseter muscles with inspiratory resistance loading. J Appl Physiol 1989;67:270-5.
60. Hollowell DE, Suratt PM. Mandible position and activation of submental and masseter muscles during sleep. J Appl Physiol 1991;71:2267-73.
61. Ng DK, Kwok KL, Cheung JM, et al. Prevalence of sleep problems in Hong Kong primary school children: a community-based telephone survey. Chest 2005;128:1315-23.
62. Sahin U, Ozturk O, Ozturk M, Songur N, Bircan A, Akkaya A. Habitual snoring in primary school children: prevalence and association with sleeprelated disorders and school performance. Med Princ Pract 2009;18:458-65.
63. Fedson AC, Pack AI, Gislason T. Frequently used sleep questionnaires in epidemiological and genetic research for obstructive sleep apnea: a review. Sleep Med Rev 2012;16:529-37.
64. Sheldon SH. Obstructive sleep apnea and bruxism in children. In: Bailey DR, ed. Sleep Med Clin 2010;5:163-88.
65. Gregorio PB, Athanazio RA, Bitencourt AG, Neves FB, Terse R, Hora F. [Symptoms of obstructive sleep apnea-hypopnea syndrome in children]. J Bras Pneumol 2008;34:356-61.
66. Gold AR, Dipalo F, Gold MS, O’Hearn D. The symptoms and signs of upper airway resistance syndrome: a link to the functional somatic syndromes. Chest 2003;123:87-95.
67. Sjoholm TT, Lowe AA, Miyamoto K, Fleetham JA, Ryan CF. Sleep bruxism in patients with sleep-disordered breathing. Arch Oral Biol 2000;45:889-96.
68. Bader G, Lavigne G. Sleep bruxism; an overview of an oromandibular sleep movement disorder. Sleep Med Rev 2000;4:27-43.
69. Kato T, Velly AM, Nakane T, Masuda Y, Maki S. Age is associated with self-reported sleep bruxism, independently of tooth loss. Sleep Breath 2012;16:1159-65.
70. Yoshida K. Influence of sleep posture on response to oral appliance therapy for sleep apnea syndrome. Sleep 2001;24:538-44.
71. Metersky ML, Castriotta RJ. The effect of polysomnography on sleep position: possible implications on the diagnosis of positional obstructive sleep apnea. Respiration 1996;63:283-7.
72. Okeson JP, Phillips BA, Berry DT, Baldwin RM. Nocturnal bruxing events: a report of normative data and cardiovascular response. J Oral Rehabil 1994;21:623-30.
73. Okeson JP, Phillips BA, Berry DT, Cook Y, Paesani D, Galante J. Nocturnal bruxing events in healthy geriatric subjects. J Oral Rehabil 1990;17:411-8.
74. Remmers JE, deGroot WJ, Sauerland EK, Anch AM. Pathogenesis of upper airway occlusion during sleep. J Appl Physiol 1978;44:931-8.
75. Morikawa S, Safar P, Decarlo J. Influence of the headjaw position upon upper airway patency. Anesthesiology 1961;22:265-70.
76. Huynh N, Kato T, Rompre PH, et al. Sleep bruxism is associated to micro-arousals and an increase in cardiac sympathetic activity. J Sleep Res 2006;15:339-46.
77. Kato T, Rompre P, Montplaisir JY, Sessle BJ, Lavigne GJ. Sleep bruxism: an oromotor activity secondary to micro-arousal. J Dent Res 2001;80:1940-4.
78. Nashed A, Lanfranchi P, Rompre P, et al. Sleep bruxism is associated with a rise in arterial blood pressure. Sleep 2012;35:529-36.
79. Khoury S, Rouleau GA, Rompre PH, Mayer P, Montplaisir JY, Lavigne GJ. A significant increase in breathing amplitude precedes sleep bruxism. Chest 2008;134:332-7.
80. Hida A, Kitamura S, Ohsawa Y, et al. In vitro circadian period is associated with circadian/sleep preference. Sci Rep 2013;3:2074.
81. Shepherd K, Hillman D, Holloway R, Eastwood P. Mechanisms of nocturnal gastroesophageal reflux events in obstructive sleep apnea. Sleep Breath 2011;15:561-70.
82. Green BT, Broughton WA, O’Connor JB. Marked improvement in nocturnal gastroesophageal reflux in a large cohort of patients with obstructive sleep apnea treated with continuous positive airway pressure. Arch Intern Med 2003;163:41-5.
83. Ing AJ, Ngu MC, Breslin AB. Obstructive sleep apnea and gastroesophageal reflux. Am J Med 2000;108 Suppl 4a:120S-125S.
84. Miyawaki S, Tanimoto Y, Araki Y, Katayama A, Fujii A, Takano-Yamamoto T. Association between nocturnal bruxism and gastroesophageal reflux. Sleep 2003;26:888-92.
85. Miyawaki S, Tanimoto Y, Araki Y, Katayama A, Imai M, TakanoYamamoto T. Relationships among nocturnal jaw muscle activities, decreased esophageal pH, and sleep positions. Am J Orthod Dentofacial Orthop 2004;126:615-9.
86. Gharaibeh TM, Jadallah K, Jadayel FA. Prevalence of temporomandibular disorders in patients with gastroesophageal reflux disease: a casecontrolled study. J Oral Maxillofac Surg 2010;68:1560-4.
87. Ohmure H, Oikawa K, Kanematsu K, et al. Influence of experimental esophageal acidification on sleep bruxism: a randomized trial. J Dent Res 2011;90:665-71.
88. Helm JF, Dodds WJ, Hogan WJ, Soergel KH, Egide MS, Wood CM. Acid neutralizing capacity of human saliva. Gastroenterology 1982;83:69-74.
89. Allen ML, Orr WC, Woodruff DM, Duke JC, Robinson MG. The effects of swallowing frequency and transdermal scopolamine on esophageal acid clearance. Am J Gastroenterol 1985;80:669-72.
90. Mandel ID. The functions of saliva. J Dent Res 1987;66 Spec No:623-7.
91. Orr WC, Robinson MG, Johnson LF. The effect of esophageal acid volume on arousals from sleep and acid clearance. Chest 1991;99:351-4.
92. Orr WC, Elsenbruch S, Harnish MJ, Johnson LF. Proximal migration of esophageal acid perfusions during waking and sleep. Am J Gastroenterol 2000;95:37-42.
93. Petit FX, Pepin JL, Bettega G, Sadek H, Raphael B, Levy P. Mandibular advancement devices: rate of contraindications in 100 consecutive obstructive sleep apnea patients. Am J Respir Crit Care Med 2002;166:274-8.
94. Cunali PA, Almeida FR, Santos CD, et al. Prevalence of temporomandibular disorders in obstructive sleep apnea patients referred for oral appliance therapy. J Orofac Pain 2009;23:339-44.
95. Sanders AE, Essick GK, Fillingim R, et al. Sleep apnea symptoms and risk of temporomandibular disorder: OPPERA Cohort. J Dent Res 2013;92:S70-7.
96. Hoffmann RG, Kotchen JM, Kotchen TA, Temporomandibular disorders and associated clinical comorbidities. Clin J Pain 2011;27:268-74.
97. Douglass AB, Bornstein R, Nino-Murcia G, et al. The Sleep Disorders Questionnaire. I: Creation and multivariate structure of SDQ. Sleep 1994;17:160-7.
98. Collesano V, Segu M, Masseroli C, Manni R. Temporomandibular disorders and sleep disorders: which relationship? Minerva Stomatol 2004;53:661-8.
99. McInrue E, Hoehn J, Klick B, et al. Sleep disordered breathing is associated with a trajectory of increase pain in temporomandibular joint disorder (TMD): A three month prospective study. Sleep 2009;32(abstract suppl):A399.
100. Smith MT, Wickwire EM, Grace EG, et al. Sleep disorders and their association with laboratory pain sensitivity in temporomandibular joint disorder. Sleep 2009;32:779-90.
101. Vendrame M, Kaleyias J, Valencia I, Legido A, Kothare SV. Polysomnographic findings in children with headaches. Pediatr Neurol 2008;39:6-11.
102. Raphael KG, Sirois DA, Janal MN, et al. Temporomandibular pain disorders are associated with sleep disturbance and sleep disordered breathing in women: A controlled study. Sleep 2013;36(abstract suppl):A289.
103. Yachida W, Castrillon EE, Baad-Hansen L, et al. Craniofacial pain and jaw-muscle activity during sleep. J Dent Res 2012;91:562-7.
104. Saito M, Yamaguchi T, Mikami S, et al. Temporal association between sleep apnea-hypopnea and sleep bruxism events. J Sleep Res 4 Nov 2013. [Epub ahead of print].
105. Lavigne GJ, Kato T, Kolta A, Sessle BJ. Neurobiological mechanisms involved in sleep bruxism. Crit Rev Oral Biol Med 2003;14:30-46.
106. Simmons JH, Prehn R. Airway Protection: the missing link between nocturnal bruxism and obstructive sleep apnea. Sleep 2009;32(abstract suppl):A218.
107. Saueressig AC, Mainieri VC, Grossi PK, et al. Analysis of the influence of a mandibular advancement device on sleep and sleep bruxism scores by means of the BiteStrip and the Sleep Assessment Questionnaire. Int J Prosthodont 2010;23:204-13.
108. Landry ML, Rompre PH, Manzini C, Guitard F, de Grandmont P, Lavigne GJ. Reduction of sleep bruxism using a mandibular advancement device: an experimental controlled study. Int J Prosthodont 2006;19:549-56.
109. Landry-Schonbeck A, de Grandmont P, Rompre PH, Lavigne GJ. Effect of an adjustable mandibular advancement appliance on sleep bruxism: a crossover sleep laboratory study. Int J Prosthodont 2009;22:251-9.
110. Carra MC, Huynh NT, El-Khatib H, Remise C, Lavigne GJ. Sleep bruxism, snoring, and headaches in adolescents: short-term effects of a mandibular advancement appliance. Sleep Med 2013;14:656-61.
111. Gagnon Y, Mayer P, Morisson F, Rompre PH, Lavigne GJ. Aggravation of respiratory disturbances by the use of an occlusal splint in apneic patients: a pilot study. Int J Prosthodont 2004;17:447-53.
112. Nikolopoulou M, Ahlberg J, Visscher CM, Hamburger HL, Naeije M, Lobbezoo F. Effects of occlusal stabilization splints on obstructive sleep apnea: a randomized controlled trial. J Orofac Pain 2013;27:199-205.
113. Nikolopoulou M, Naeije M, Aarab G, Hamburger HL, Visscher CM, Lobbezoo F. The effect of raising the bite without mandibular protrusion on obstructive sleep apnoea. J Oral Rehabil 2011;38:643-7.
114. Franco L, Rompre PH, de Grandmont P, Abe S, Lavigne GJ. A mandibular advancement appliance reduces pain and rhythmic masticatory muscle activity in patients with morning headache. J Orofac Pain 2011;25:240-9.
115. Loube DI, Gay PC, Strohl KP, Pack AI, White DP, Collop NA. Indications for positive airway pressure treatment of adult obstructive sleep apnea patients: a consensus statement. Chest 1999;115:863-6.
116. Oksenberg A, Arons E. Sleep bruxism related to obstructive sleep apnea: the effect of continuous positive airway pressure. Sleep Med 2002;3:513-5.
117. Simmons JH, Prehn R. Nocturnal bruxism as a protective mechanism against obstructive breathing during sleep. Sleep 2008;31(abstract suppl):A199.
118. Raphael KG, Sirois DA, Janal MN, Wigren PE, Dubrovsky B, Nemelivsky LV, et al. Sleep bruxism and myofascial temporomandibular disorders: A laboratory-based polysomnographic investigation. J Am Dent Assoc 2012;143:1223-31.
119. Lavigne GJ, Guitard F, Rompre PH, Montplaisir JY. Variability in sleep bruxism activity over time. J Sleep Res 2001;10:237-44.
120. DiFrancesco RC, Junqueira PA, Trezza PM, de Faria ME, Frizzarini R, Zerati FE. Improvement of bruxism after T & A surgery. Int J Pediatr Otorhinolaryngol 2004;68:441-5.
121. Eftekharian A, Raad N, Gholami-Ghasri N. Bruxism and adenotonsillectomy. Int J Pediatr Otorhinolaryngol 2008;72:509-11.
122. Lobbezoo F, Lavigne GJ. Do bruxism and temporomandibular disorders have a cause-and-effect relationship? J Orofac Pain 1997;11:15-23.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication September, 2013
Submitted in final revised form December, 2013
Accepted for publication January, 2014
Address correspondence to: Ramesh Balasubramaniam, Perth Oral Medicine & Dental Sleep Centre, St John of God Hospital, Subiaco Clinic, Suite 311, 25 McCourt Street, Subiaco, WA 6008, Australia; Tel: +618 9382 2325; Fax: +618 9382 2328; Email: ramesh.balasubramaniam@uwa.edu.au
DISCLOSURE STATEMENT
This was not an industry supported study. The protocol of this research project was approved by the Human Research Ethics Committee at the University of Western Australia, Perth, Australia. All authors have contributed significantly and are in agreement with the content of the manuscript. Dr. Cistulli is a chief investigator on sponsored clinical trials in obstructive sleep apnea for ResMed Inc and Exploramed Inc. His department receives equipment support for oral appliance research from SomnoMed Ltd, and he has a pecuniary interest in the company from previous involvement in product development. He is a medical advisor to Exploramed Inc (a US medical device incubator) and Zephyr Sleep Technologies. He has received speaker fees / travel support from ResMed Inc Fisher & Paykel Healthcare. The other authors have indicated no financial conflicts of interest.