Review Article 2, Issue 7.4
Rapid Maxillary Expansion Effects on the Upper Airway Dimensions and Function in Growing Patients: An Umbrella Review
http://dx.doi.org/10.15331/jdsm.7164Silvia Gianoni-Capenakas, DDS, MSc1; Karla Carpio Horta, DDS, MSc PhD2 ; Carlos Flores-Mir DDS, MSc, DSc., FRCD(c)1; Manuel O. Lagravère, DDS, MSc, Ph.D., FRCD(c)1; Camila Pacheco-Pereira, DDS, MBA, MSc1,3
1School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, Canada; 2 School of Dentistry of Ribeirao Preto, University of Sao Paulo, Brazil; 3 University of Texas Health Science at San Antonio, San Antonio, Texas
ABSTRACT
Objective:
Because numerous published systematic reviews have assessed the effect of rapid maxillary expansion (RME) over upper airway dimensional changes, it is important to map and summarize their conclusions. In addition, the accepted methods used to evaluate the upper airway across the different systematic reviews will be outlined and areas of strengths and weaknesses on the topic identified.
Methods:
Systematic reviews in which RME treatment outcomes as related to upper airway dimensional changes or breathing function in children and adolescents were included in this umbrella systematic review. Studies that investigated upper airway changes using three-dimensional imaging (cone beam computed tomography, computed tomography, magnetic resonance imaging), acoustic rhinometry, rhinomanometry, and polysomnography correlated with RME effects were included. Studies on expansion using palatal anchorage with miniscrews and surgically assisted maxillary expansions were excluded, as well as studies including syndromic patients.
Results:
Sixty-six studies were found from the database searches. After managing duplicates, 33 studies were assessed based on the titles and abstracts, but only 16 reviews were considered for the next assessment phase (full text). From then, only 10 systematic reviews were finally included in this umbrella review.
Conclusions:
A significant amount of research has been published linking RME changes to increases in nasal respiratory capability, nasal volume, and linear transverse enlargement. However, methodologic inconsistencies and disagreements between the included studies (especially on the oropharyngeal dimensional changes after RME) lead to significant uncertainties about the consistency of the effect of RME changes, especially on the oropharynx region dimensions. It is not clear that the upper airway dimensional changes necessarily imply an improvement in actual breathing function.
Keywords:
sleep apnea, maxillary expansion, upper airway obstruction, review
Citation:
Gianoni-Capenakas S, Horta KC, Flores-Mir C, Lagravère MO, Pacheco-Pereira C. Rapid maxillary expansion effects on the upper airway dimensions and function in growing patients: An umbrella review. J Dent Sleep Med. 2020;7(4)
INTRODUCTION
The upper airway is part of the respiratory system and comprises the nasal cavity and surrounding sinuses, oral cavity, and pharynx.1 Upper airway function includes air warming and humidification, defense against infection, protection from food aspiration, ventilation, swallowing, and speech.1 Upper airway volume variation after orthodontic treatment has been heavily studied, but still has shown several inconsistencies because of differences in methodologic approaches and a large number of orthodontic/orthopedic appliances tested.
Maxillary expansion is used to correct maxillary deficiencies commonly related to posterior crossbites and crowding.1 The most common technique used in mixed dentition is rapid maxillary expansion (RME) with a tooth-anchor expander (Hyrax and Haas appliances).1 After maxillary expansion, the separation of the maxillary halves occurs followed by the separation of the nasal walls and lowering of the middle part of the palate vault.2 Additional reported changes related to the maxillary expansion are stretching of the tensor palatine muscles and improving the drainage of the eustachian tubes, reducing otitis media and conductive hearing loss.2,3 In addition to those changes, nasal permeability may increase and nasal air resistance may reduce.2,4,5 RME has been associated with changes in upper airway dimensions; however, the extent of these changes, the long-term effectiveness, and the relationship between airway dimensional changes and breathing capacity is still controversial, especially those changes related to the oropharynx portion.6–10
Different methods for evaluating the upper airway dimensions and functions are available, although each has its advantages and drawbacks.10 Cone beam computed tomography (CBCT) allows the rendering of the upper airway volume in a three-dimensional view, permitting the assessment of certain upper airway volumetric, linear, and angular measurements. Although it usually has a higher ionizing radiation dose than cephalometric radiographs, CBCT is overall more accurate than two-dimensional imaging.11 For ear, nose, and throat specialists, the primary professionals who assess the upper airway, acoustic rhinometry (AR) is the first tool of choice, as it gathers volumetric and cross-sectional area data from reflected signals. This may be followed by direct visualization via nasoendoscopy and PSG.
There are several types of literature reviews. An umbrella review is justified in cases when there is contradictory evidence coming from multiple previously published reviews. An umbrella review focuses on highlighting the strengths and weaknesses of previous reviews that address interventions and their results for a specific condition. In this sense, because numerous published systematic reviews have assessed the effect of RME over upper airway dimensional changes, it is important to map and summarize their conclusions. In addition, it is helpful to outline the methods used to evaluate the upper airway across the different systematic reviews and to identify strengths and weaknesses on the topic to guide future research and to make the readership aware of how those findings shape clinical approaches.
METHODS
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) was used as a guideline for the methodologic approach of this study.12
Eligibility Criteria
Systematic reviews in which RME treatment outcomes as related to upper airway dimensional changes or breathing function in children and adolescents were included in this umbrella systematic review. Studies that included healthy patients or patients with sleep-breathing disorders were listed. Studies that investigated upper airway changes using three-dimensional imaging (CBCT, CT, MRI), AR, rhinomanometry, and polysomnography (PSG) correlated to RME effects were included. Because the focus of this study is RME, studies on expansion using palatal anchorage with miniscrews surgically assisted maxillary expansions were excluded, as well as studies including patients exhibiting syndromic symptoms. No limitations of time or language were imposed.
Information Sources
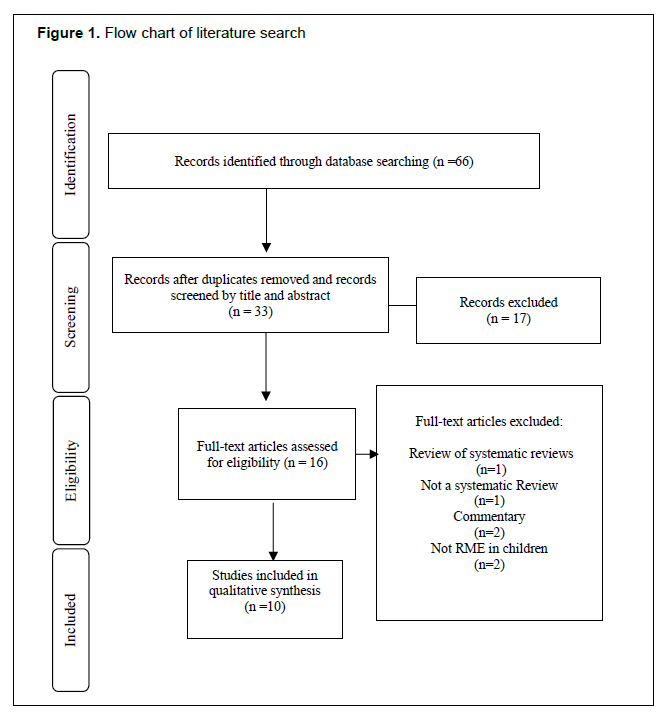
To identify systematic reviews related to our inclusion criteria, the following databases were searched: Cochrane, EMBASE, MEDLINE, and PubMed. Additionally, a hand search was performed. The search was carried out in April 2018, and an update was performed in April 2019. The search results were exported to Rayyan Software (Qatar Computing Research Institute, Doha, Qatar)13 in which the duplicates were excluded (Figure 1).
Search
The final search strategy displayed in Appendix 1 shows the search strategy and truncations used for each database.
Selection of Sources of Evidence, Data Charting Process and Data Items
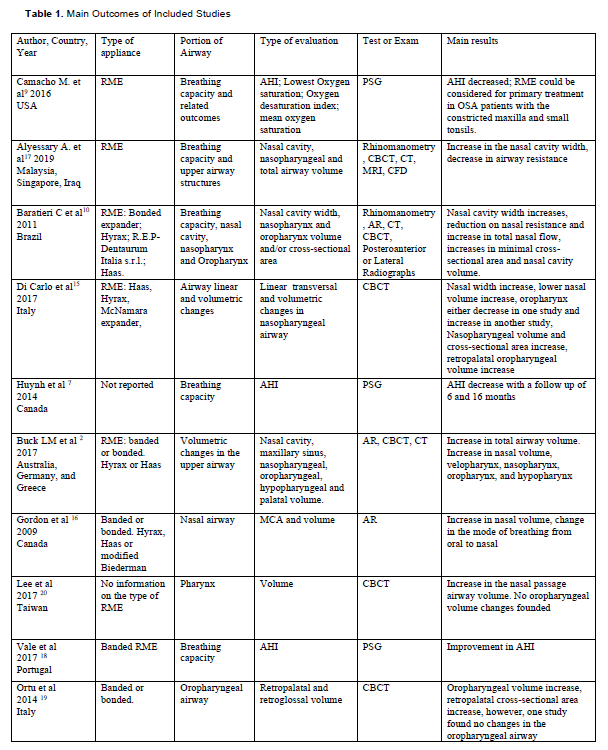
Two reviewers (SGC and KCH) independently evaluated the studies by screening the titles and abstracts, using a web-based citation management program (RefWorks, ProQuest LLC; and Rayyan, Qatar Computing Research Institute, Doha, Qatar). The articles were screened in full text in the second phase by the same two reviewers and, in cases of disagreement, a third reviewer was consulted (CPP). The data were extracted by the first examiner (SGC) and each article was charted. The key features were listed as authors, country, year, type of appliance, area of the airway evaluated, modalities of evaluation (e.g., volume, minimum cross-sectional area, apnea/hypopnea index (AHI), oxygen saturation), type of test to assess airway changes, and main results (Table 1). In addition, the data included in each systematic review are summarized in Table 2.
Critical Appraisal of Individual Sources of Evidence
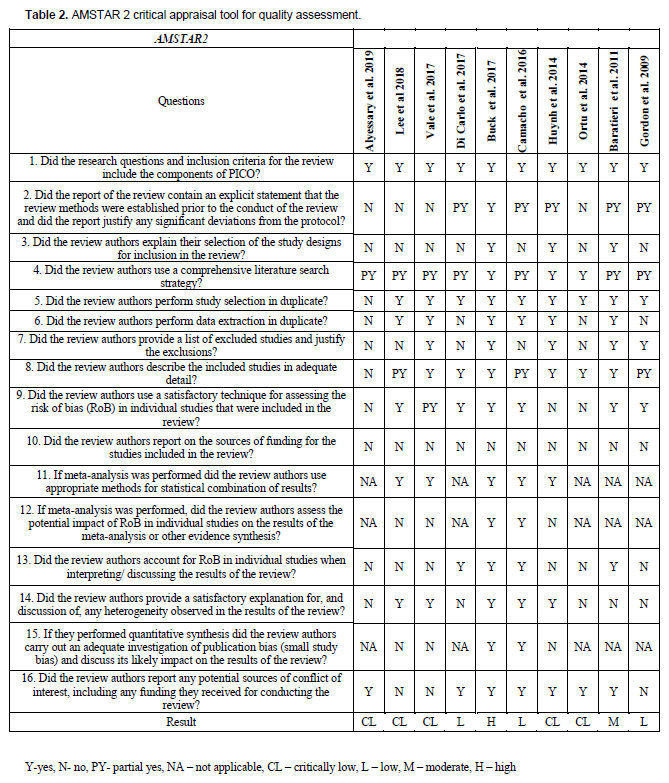
The assessment of the methodologic quality of each systematic review was executed using the AMSTAR 2 tool. This tool focuses on critical and noncritical weaknesses.14 It can be ranked as high quality, moderate quality, low quality, and critically low quality.14
Summary Measures and Synthesis of Results
The studies were evaluated regarding volumetric and minimal cross-sectional area changes in the upper airway (nasal cavity, nasopharynx, and oropharynx), respiratory function (AHI), and oxygen saturation. Also, the type of examinations (CBCT, AR, PSG) was assessed, as well as the type of RME and long-term effects of these variables.
The studies were grouped according to the analyzed airway section (nasal cavity, nasopharynx, oropharynx, and hypopharynx) and described in terms of the effects of RME in the upper airway.
Risk of Bias Across Studies
The risk of bias (RoB) across studies was evaluated, comparing the differences across studies such as type of RME, type of examinations, and type of outcome. In addition, a comparison of the RoB among individual reviews was considered. To date there is no published validated RoB assessment tool across included systematic reviews in cases of umbrella reviews.
Figure 1Flow chart of literature search |
{kind=link}
Table 1Main Outcomes of Included Studies |
{kind=link}
Table 2AMSTAR 2 critical appraisal tool for quality assessment. |
{kind=link}
RESULTS
Selection and Characteristics of Sources of Evidence
Sixty-six studies were identified from the database searches. After managing duplicates, 33 studies were assessed based on the titles and abstracts; 17 of them were excluded. The remaining 16 reviews were screened by assessing their full text. The references of the included studies were also screened for possible new inclusions. In total, 10 systematic reviews were included in this umbrella review.
The characteristics associated with the target group, number of articles included, main findings, databases searched, type of appliance, portion of airway analyzed, type of evaluation and tests or examinations used to evaluate upper airway dimensions and function are summarized in Tables 1.
Critical Appraisal Within Sources of Evidence
The AMSTAR 2 tool results shown in Table 2 are divided into 16 questions and the results displayed into 4 possible categories: high, moderate, low, and critically low quality of evidence. Only one systematic review was ranked with high quality of evidence,2 one received a moderate rating10; three were rated low9,15,16; and five received a critically low rating.7,17–20 The lack of a protocol registration was the most common critical domain across the studies. Although it is not possible to affirm the lack of registration or if the information was just not reported in the studies. Also, the lack of information about the study design and RoB assessment of individual studies was also noted in most of the systematic reviews.
Results of Individual Sources of Evidence: General Information
Lee et al.20 analyzed the pharyngeal changes after RME or protraction, but the current study focused only on the results related to RME alone. Di Carlo et al. evaluated the upper airway changes comparing CBCT protocols.15 Vale et al. evaluated the available studies examining patients with obstructive sleep apnea (OSA) treated with RME for posterior crossbites and analyzing the AHI rates after the RME treatment.18 Ortu et al. evaluated changes in oropharyngeal airway volume and minimal cross-sectional area (MCA) after the use of RME.19 Huynh et al. and Camacho et al. evaluated upper airway changes after RME in children in whom OSA was diagnosed.7,9 Gordon et al. evaluated nasal dimensional changes through AR after RME treatment.16 Buck et al. described the volumetric changes in the upper airway after RME.2
Upper Airway Function
Huynh et al., Camacho et al., and Vale et al. evaluated the efficacy of RME in pediatric patients in whom OSA was diagnosed.7,9,18 Their principal findings were a decrease of AHI after RME, and improved mean oxygen saturation and higher oxygen saturation after RME. Camacho et al. stated that RME could be a primary treatment option for children with small tonsils or the second option in patients in whom adenotonsillectomy failed and OSA persisted thereafter, in children with the constricted maxilla.9 Nonetheless, according to Camacho et al., the patients with residual OSA after adenotonsillectomy and RME treatment could have considered multiple oropharyngeal sites of collapsibility (epiglottis, supraepiglottis, and tongue base sites).9 The reduction in the obstruction could be a secondary factor associated with post-RME treatment such as an increase in nasal cavity size and consequently improvement in nasal flow; better tongue position after maxillary width expansion; and a stimulus for normal positioning of the mandible after the maxillary teeth repositioning.9
An immediate overall decrease of 70% in the AHI was found, with a reduction from a mean of 8.9 ± 7/h to 2.7 ± 3.3/h after the treatment with RME; aside from two studies, the other 15 showed at least 50% reduction in AHI after the RME.9 According to Vale et al. the mean decrease for AHI was 3.24 at a 95% confidence interval [0.34-6.15].18 A more significant reduction of the AHI levels was seen in children with small tonsils or no tonsils.9
Regarding oxygen saturation, studies reported an improvement between 0.4% to 5.7% in the mean oxygen saturation and a 9% improvement of lowest oxygen saturation.9 Nasal flow increase was also reported (P<0.05).10 Although all the aforementioned results seem consistent, one study emphasized the possibility of some of the changes being related to normal growth and spontaneous remission of OSA.9 Huynh et al. reported a high heterogeneity (I2=98.4%, P<0.001), as did Vale et al. (I2= 98.02%, P<0.0001 for AHI improvement, and I2=95.53% P<0.0001 for AHI normalization).7,18 According to Vale et al., this is a likely finding because a small number of studies included belonged to a few research author groups.18 Although RME can positively influence the breathing capacity of patients with OSA, RME treatment is an auxiliary method18 and should be used only when orthodontically indicated.21
Upper Airway Dimensional Changes
Alyessary et al. showed that most of the results indicated an increase in the anterior nasal cavity area, from pretreatment to posttreatment (11.7%), postexpansion to postretention (22.2%), and pre-expansion to postretention (35.7%).17 Similar results were found in the middle and posterior nasal cavity areas (10% and 15%, respectively).17 Nasal width increase was found in several studies and its volume was reported to have increased dimensions after RME treatment.15,22,23 An increase in the nasal volume (11.3%) was reported.17 Lee et al. reported changes in the nasal passage airway volume (P=0.004).20 However, no changes were seen in the lower airway and the airway below the palatal plane (P>0.05) in the same study.20 Gordon et al. reported an increase in the nasal volume and MCA; one study demonstrated MCA increase after RME in two groups, one before the pubertal growing peak and the other after the pubertal growing peak.16 However, a higher decrease in the MCA was seen after the retention phase in the group after the pubertal growing peak.16 Buck et al.2 found that overall total airway volume increased; when evaluated via AR, studies showed a statistically significant increase in nasal volume (P<0.001) with an increase from 2 mm3 to 6 mm3. An increase in volume of the velopharynx, nasopharynx, oropharynx and hypopharynx was found; however, there was a decrease in the remaining volume gain after the retention when compared to the volume results right after the expansion in the nasopharynx and oropharynx.2
Regarding the oropharynx, one study found differences in the oropharyngeal volume; however, those changes were not statistically significant. Other studies showed a statistically significant increase in oropharyngeal volume after RME.22,24 Conversely, one study showed a decrease in the oropharyngeal volume although not statistically significant,15,23 and another three studies found no differences in the oropharyngeal volume.15,25–27 Out of five studies analyzed by Ortu et al., two did not find changes in the oropharynx volume after RME; the other three found increases, one in the retropalatal cross-sectional area, one in the retropalatal plane, and one in oropharyngeal volume.19 One author stated that the improvement of airway ventilation was related to the “new” lower position of the tongue.15,25 The reduction of upper airway resistance was linked to the changes in the nasal valves, the widening of the nasopharyngeal cavity, and the increase in the total airway volume.17 Baratieri et al. noted in their study a moderate level of evidence showing that RME increases nasal cavity width and posterior nasal airway according to the quality of evidence tool assessed.10
Long-term Effects
An overall decrease in AHI results after RME treatment was described by Huynh et al (P=0.005 from baseline to follow-up of 6 to 12 months in one study, and P=0.046 from baseline to follow-up at 10 to 16 months in another study).7 Baratieri et al. evaluated the long-term effects of RME on upper airway dimensions.10 They stated an indication of the stability of the results for at least 11 months after treatment with RME, although one study concluded that there was stability up to 5 years.10
Type of RME and Diagnostic Examinations
Hyrax and Haas appliances, reported as banded or bonded, were used in the studies included in each systematic review.11,18 The activation protocol that was most commonly reported was two turns a day.11 However, the type of appliance was poorly described by some authors. Huynh et al.’s description of studies was limited; there was no information on the type of appliances used, only vague descriptions such as “fixed”, “in situ”, or “ex-situ”.7 All the articles evaluated by Vale et al. reported the use of banded RME appliances.18 Camacho et al., Alyessary et al., Lee et al., and Ortu et al. did not mention the type of RME used in the included articles.9,17,19,20 The reported examinations used to appraise the breathing capacity were PSG, AR,,11,20 and rhinomanometry.11,20 The upper airway dimensional changes were assessed with either CBCT,11,18,20,22,23 CT,3,20 or MRI.20
Synthesis of Results
Ten systematic reviews were included in this study; all of them were written in English and published between 2009 and 2019. One study was from a group from the United States, Portugal, and Italy9; one from Malaysia and Singapore17; one from Brazil10; two from Canada7,16; one from Taiwan20; one from Portugal18; one from a group from Australia, Germany, and Greece2; and two from Italy.15,19 Of the 10 systematic reviews, 3 studies focused on patients with OSA.7,9,18
The reviews were critically appraised for quality of evidence using the AMSTAR 2 tool14; the results showed only one2 systematic review scored as high quality of evidence. From the included systematic reviews, it was possible to retrieve 53 articles in total that studied upper airway changes after orthodontic treatment using RME in patients with a constricted maxilla (bilateral or unilateral crossbites). Nineteen of them reported results related to breathing capacity, 2 related to the oral cavity or the palatal volume, 29 related to the nasal volume, 11 related to nasopharynx, and 9 related to oropharynx. The mean age of the assessed patients ranged from 5.9 to 14 years.
The overall conclusion of these included systematic reviews is that an increase in the nasal cavity volume, a decrease in airway resistance, and a decrease in AHI among children in whom OSA is diagnosed are usually observed immediately after the treatment with RME. Nasopharyngeal volume and minimal cross-sectional area increases were shown with seven articles claiming an increase after RME and three claiming no change was apparent. The major uncertainty regarding the results was focused on the oropharynx, where three studies reported an increase in the oropharynx, four reported no changes, and two reported a decrease in oropharynx after RME treatment.22–26,28–31 The relative lack of long-term follow-up studies has to be noted. How much of the decrease in airway resistance and AHI is only temporary?
Risk of Bias Across Studies
A large number of dissimilarities were seen across the studies. The studies differ regarding the area of the airway analyzed, which could be interesting to have results focused on just one area.22 However, the upper airway’s boundaries used in the included studies in each review for times were different. The retropalatal plane described in one study was at the same anatomic boundary as the nasopharyngeal space of another included study and was the same boundary of the oropharyngeal space in another. This discrepancy leads to uncertainties among the results.
In addition, the differences in types of examinations made the comparator factor impossible. It is not possible to compare the dimensional changes found via AR to those found with CBCT. The lack of more studies evaluating the long-term effects of RME on the upper airway still should raise some degree of skepticism. The main RoB limitation within studies was the lack of a registered protocol, and sometimes the authors mentioned that there was a protocol; however, there was no registration number described. Only two studies reported a previous plan for the meta-analysis and investigation of the heterogeneity causes.2,9 Four studies did not describe the included studies in detail.9,16,17,20
DISCUSSION
The objective of this umbrella review was to summarize the findings on the effect of the RME on the upper airway. Methodologic flaws and differences did not support a direct comparison between some results. Moreover, such superficial comparison can lead to inaccuracies, especially concerning nasopharynx, oropharynx, and retropalatal pharynx boundaries and nomenclatures, as reported by the included studies.
The increased nasal cavity volume after RME treatment seems to be consistently reported by several systematic reviews.2,7,10,15–17 Overall their results showed an increase in the nasal cavity by approximately 10% to 12%.2,15,20,32 Supporting articles associated these volumetric changes with a decrease in nasal resistance and some degree of AHI normalization tendency.7,9,18 The decrease ranged from 8% to 95%.9,15,16,18 However, caution is needed because it is not possible to automatically imply improved breathing function only by AHI changes.
In regard to nasopharynx dimensional changes, several studies have found increases in volume and/or MCA, demonstrating increases of up to 29%.2,15,28,30,33,34
However, few studies have evaluated the effects of RME in the oropharynx and the results are controversial: three studies reported an increase (retropalatal plane; retropalatal airway; oropharyngeal sagittal and axial area), four studies reported no changes, and two studies reported decreases of oropharynx dimensions.22–26,28–31
In general, the heterogeneity was found to be high,18,21,23 although not all the systematic reviews performed a meta-analysis. The systematic reviews that evaluated upper airway dimensions were rated with a high level of evidence,2 moderate level of evidence,11 low level of evidence,18,19 and critically low level of evidence.20,22,23 The systematic reviews that analyzed AHI were scored with critically low7,21 and low10 quality of evidence. Although the study by Huynh et al. was fully organized and complete, the RoB was not individually reported or discussed; for this reason, according to the AMSTAR 2 tool their rating dropped off to the critically low quality of evidence.7 An increase in the palatal volume may be related to a better repositioning of the tongue posture, increasing the airway space in the oropharynx level.3,35 The tongue might be positioned closer to the roof of the palate, displacing the tongue away from the oropharynx, possibly leading to more consistent nasal breathing.7 However, caution is needed to correlate findings in this sense because the difference in tongue position can be related to swallowing or breathing phases during the CBCT examinations in children; even when the radiology technician uses a strict protocol, tongue movement is not unlikely to occur.18
The transverse changes in the maxillary halves and consequently on the nasal walls after the maxillary expansion procedure seem to be directly related to the nasal cavity dimensional changes.3–6 Furthermore, these changes might be related to the findings on reduced nasal resistance and normalization of AHI.7 Based on linear measurements, Lagravère et al. reported transverse maxillary statistically significant changes in the nasal cavity width (intercondylar width) and inter-alveolar width.1 Concerning vertical changes, the changes in the mandibular plane in relation to the palatal plane and sella nasion plane were relatively minor (1.65º and 1.97º respectively).1 However, some studies have found no significant changes in transversal skeletal width, although changes in transversal molar and premolar width were found, suggesting dental tipping.1 Although others have supported significant transversal findings, important increases to the maxillary alveolar width were found but the clinical significance is still questionable.1 Nonsignificant anteroposterior skeletal changes were found, but significant vertical changes were confirmed in the mandibular plane angulation (P<0.05). However, those findings may not be clinically significant.1,11
Regarding the tools utilized, a nocturnal PSG gives a reliable and objective assessment of nocturnal breathing capacity.35 However, because RME anatomic changes might occur at different upper airway levels, it is impossible to know to which part of the upper airway the changes are related. The AR is an interesting examination approach that provides cross-sectional area and volume of the nasal cavity and pharynx through the reflection of sound waves. Nasal decongestants can be used to remove short-term pathologic constriction effects and acute inflammation.19 However, it is also not possible to know which part of the upper airway has increased in regard to the RME effect. Both PSG and AR require special equipment and analysis by an ear, nose, and throat specialist.
Few studies evaluated the long-term effects of RME on upper airway dimensions7,10; one of them implied higher stability in a group of adolescents if RME was done before the pubertal peak of growth.16 The higher stability in the group treated before the peak of growth could be related to less palatal suture calcification at the time of expansion and a lower resistance against the expansion forces.6 In agreement with stability results, Pirelli et al. found the RME results to be stable after 12 years in a group of children in whom OSA was diagnosed.36 Additionally, the long-term effect is not an easy matter of debate considering the Scammon growth curve and craniofacial growth, and the various ages are going to process the long-term effects differently. In addition, several studies did not consider samples of untreated growing study patients.
During craniofacial growth, the nasopharynx volume can reach rates of up to 80% of the increase.37 Hence, not only can orthodontic treatment influence size, but lymphoid tissue growth related to the Scammon growth curve will influence the relative upper airway dimensions at the oropharyngeal and nasopharyngeal levels as well.38 Tonsil and adenoid tissues quickly increase during in younger patients, with a slower development after that, a peak before adolescence, and a decrease approaching adulthood.37,38 Therefore, it is possible that the increase in the nasopharyngeal airway is related to the spontaneous reduction of the lymphoid tissue due to age or normal craniofacial growth changes. In contrast to a previous systematic review of systematic reviews on the same RME treatment and its effects on upper airway subject, the decision was made to include studies that focused on patients with sleep-breathing disorders and also those that were performed in healthy patients.6 Because the intention was to summarize the findings in this area, and because those patients underwent RMT, the results of pharyngeal and nasal dimensions, breathing capacity, AHI, and oxygen patency are extremely valid to be analyzed. Because two-dimensional imaging studies have been related to the superimposition of structures and magnification and low accuracy to visualize the upper airway, the decision was made not to include studies based on lateral two-dimensional cephalometric radiographs.37,39,40
In line with the proposal for this systematic review, more studies that measure breathing function on the oropharyngeal changes related to RME are necessary to understand the real effects of RME in the cited region of the pharynx. Although according to some authors, RME can positively influence the breathing capacity of patients with OSA.7,9,18 RME treatment is an auxiliary method18 and should be used only when orthodontically indicated.
Limitations
The authors of this umbrella review acknowledge that one included study22 was not a systematic review, but a narrative review. Hence, that review failed to provide information commonly reported in systematic reviews. Nevertheless, the decision to include this study was based on the fact that it is a relevant review addressing this topic.
Overall the value of an umbrella review greatly depends on the quality and risk of bias of the included primary studies. For this topic, several methodologic, clinical, and statistical issues were identified that would preclude stronger conclusions.
Future Directions
In line with the proposal for this systematic review, further studies with enhanced methods on the upper airway volumetric changes related to RME are needed to improve understanding of the real effects of RME on airway function. Also, future studies should analyze airway function to correlate the volumetric changes to actual breathing capacity and functional performance after maxillary expansion treatment. In addition, subjective analysis of patient’s perceptions of breathing improvement after orthodontic therapy should be made.
Finally, efforts should be made to identify which phenotypic characteristics are associated with better functional breathing responses. It is becoming more clear that not all the individuals with OSA respond similarly to any given management therapy.
CONCLUSION
A significant amount of research has been published linking RME changes to an increase in nasal respiratory capability, nasal volume, and linear transverse enlargement. However, inconsistencies and disagreements among the included study results, especially the oropharyngeal dimensional changes after RME, lead to uncertainties about the effect of RME on the oropharynx region.
It is not clear that upper airway dimensional changes necessarily imply an improvement in actual breathing function. Having stated this, some studies have measured a decrease in upper airway resistance associated with the dimensional changes. If this decrease automatically implies improvements in breathing function as objectively or subjectively qualified is unknown.
Finally, any portrayed dimensional changes would be important for patients with a maxillary constriction to start with. Those cases would need to have a maxillary expansion regardless of breathing changes or not. Although according to some authors RME can positively influence the breathing capacity of patients with OSA, RME treatment is an auxiliary method and should be used only when orthodontically indicated. Hence, RME could be considered a positive adjunctive sleep breathing management tool for a specific subgroup of children with maxillary constriction. So far, such subgroup has not been identified.
REFERENCES
- Lagravère M, Carey J, Heo G, Toogood R, Major P. Transverse, vertical, and anteroposterior changes from bone-anchored maxillary expansion vs traditional rapid maxillary expansion: A randomized clinical trial. Am J Orthod Dentofac Orthop. 2010;137(3):304.e1-304.e12.
- Buck LM, Dalci O, Ali Darendeliler M, Papageorgiou SN, Papadopoulou AK. Volumetric upper airway changes after rapid maxillary expansion: A systematic review and meta-analysis. Eur J Orthod. 2017;39(5):463-473. doi:10.1093/ejo/cjw048
- Taşpinar F, Uçüncü H, Bishara SE. Rapid maxillary expansion and conductive hearing loss. Angle Orthod. 2003;73:669-673.
- Hartgerink D V., Vig PS, Orth D, Abbott DW. The effect of rapid maxillary expansion on nasal airway resistance. Am J Orthod Dentofac Orthop. 1987;92(5):381-389. doi:10.1016/0889-5406(87)90258-7
- Pirelli P, Saponara M, Attanasio G. Obstructive sleep apnoea syndrome (OSAS) and rhino-tubaric dysfunction in children: therapeutic effects of RME therapy. Prog Orthod. 2005;6(1):48-61.
- Bucci R, Montanaro D, Rongo R, Valletta R, Michelotti A, D’Antò V. Effects of maxillary expansion on the upper airways: Evidence from systematic reviews and meta-analyses. J Oral Rehabil. 2019;46(4):377-387. doi:10.1111/joor.12766
- Huynh NT, Desplats E, Almeida FR. Orthodontics treatments for managing obstructive sleep apnea syndrome in children: A systematic review and meta-analysis. Sleep Med Rev. 2016;25:84-94. doi:10.1016/j.smrv.2015.02.002
- Abdullatif J, Certal V, Zaghi S, et al. Maxillary expansion and maxillomandibular expansion for adult OSA: A systematic review and meta-analysis. J Craniomaxillofac Surg. 2016;44(5):574-578. doi:10.1016/j.jcms.2016.02.001
- Camacho M, Chang ET, Song SA, et al. Rapid maxillary expansion for pediatric obstructive sleep apnea: A systematic review and meta-analysis. Laryngoscope. 2017;127(7):1712-1719. doi:10.1002/lary.26352
- Baratieri C, Alves M, De Souza MMG, De Souza Araújo MT, Maia LC. Does rapid maxillary expansion have long-term effects on airway dimensions and breathing? Am J Orthod Dentofac Orthop. 2011;140(2):146-156. doi:10.1016/j.ajodo.2011.02.019
- Alsufyani NA, Noga ML, Witmans M, Major PW. Upper airway imaging in sleep-disordered breathing: role of cone-beam computed tomography. Oral Radiol. 2017;33(3):161-169. doi:10.1007/s11282-017-0280-1
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred Reporting Items for Systematic review and Meta-Analysis Protocols: The PRISMA Statement. PLoS Med. 2009;6(6):e-10.
- Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210. doi:10.1186/s13643-016-0384-4
- Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomized or non-randomized studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008
- Di Carlo G, Saccucci M, Ierardo G, et al. Rapid maxillary expansion and upper airway morphology: a systematic review on the role of cone beam computed tomography. Biomed Res Int. 2017; Article ID 5460429
2017:1-10. doi:10.1155/2017/5460429 - Gordon JM, Rosenblatta M, Witmans M, et al. Rapid palatal expansion effects on nasal airway dimensions as measured by acoustic rhinometry. Angle Orthod. 2009;79(5):1000-1007. doi:10.2319/082108-441.1
- Alyessary AS, Othman SA, Yap AUJ, Radzi Z, Rahman MT. Effects of non-surgical rapid maxillary expansion on nasal structures and breathing: A systematic review. Int Orthod. 2019;17(1):12-19. doi:10.1016/j.ortho.2019.01.001
- Vale F, Albergaria M, Carrilho E, et al. Efficacy of rapid maxillary expansion in the treatment of obstructive sleep apnea syndrome: a systematic review with meta-analysis. J Evid Based Dent Pract. 2017;17(3):159-168.
- Ortu E, Giannoni M, Ortu M, Gatto R, Monaco A. Oropharyngeal airway changes after rapid maxillary expansion: the state of the art. Int J Clin Exp Med. 2014;7(7):1632-1638. doi:10.1016/j.ajodo.2012.11.019
- Lee W, Tu Y, Huang C, Chen R, Fu M, Fu E. Pharyngeal airway changes following maxillary expansion or protraction: A meta- analysis. Orthod Craniofac Res. 2018;21:4-11. doi:10.1111/ocr.12208
- American Association of Orthodontics TF. White Paper: Obstructive Sleep Apnea and Orthodontics.; 2019. https://www1.aaoinfo.org/wp-content/uploads/2019/03/sleep-apnea-white-paper-amended-March-2019.pdf.
- El H, Palomo JM. Three-dimensional evaluation of upper airway following rapid maxillary expansion: A CBCT study. Angle Orthod. 2014;84(2):265-273. doi:10.2319/012313-71.1
- Zeng J, Gao X. A prospective CBCT study of upper airway changes after rapid maxillary expansion. Int J Pediatr Otorhinolaryngol. 2013;77(11):1805-1810. doi:10.1016/j.ijporl.2013.07.028
- Ribeiro ANC, De Paiva JB, Rino-Neto J, Illipronti-Filho E, Trivino T, Fantini SM. Upper airway expansion after rapid maxillary expansion evaluated with cone beam computed tomography. Angle Orthod. 2012;82(3):458-463. doi:10.2319/030411-157.1
- Iwasaki T, Saitoh I, Takemoto Y, et al. Tongue posture improvement and pharyngeal airway enlargement as secondary effects of rapid maxillary expansion: A cone-beam computed tomography study. Am J Orthod Dentofac Orthop. 2013;143(2):235-245. http://dx.doi.org/10.1016/j.ajodo.2012.09.014. Accessed January 8, 2019.
- Pangrazio-Kulbersh V, Wine P, Haughey M, Pajtas B, Kaczynski R. Cone beam computed tomography evaluation of changes in the naso-maxillary complex associated with two types of maxillary expanders. Angle Orthod. 2012;82(3):448-457. doi:10.2319/072211-464.1
- Zhao Y, Nguyen M, Gohl E, Mah JK, Sameshima G, Enciso R. Oropharyngeal airway changes after rapid palatal expansion evaluated with cone-beam computed tomography. Am J Orthod Dentofac Orthop. 2010;137(4):S71-S78. doi:10.1016/j.ajodo.2008.08.026
- Almuzian M, Ju X, Almukhtar A, Ayoub A, Al-Muzian L, McDonald JP. Does rapid maxillary expansion affect nasopharyngeal airway? A prospective Cone Beam Computerised Tomography (CBCT) based study. Surgeon. 2018;16(1):1-11. doi:10.1016/j.surge.2015.12.006
- Li L, Qi S, Wang H, Ren S, Ban J. Cone-beam CT evaluation of nasomaxillary complex and upper airway following rapid maxillary expansion. Zhonghua Kou Qiang Yi Xue Za Zhi. 2015;50(7):403-407. http://www.ncbi.nlm.nih.gov/pubmed/26564743.
- Smith T, Ghoneima A, Stewart K, et al. Three-dimensional computed tomography analysis of airway volume changes after rapid maxillary expansion. Am J Orthod Dentofac Orthop. 2012;141:618-626. doi:10.1016/j.ajodo.2011.12.017
- Chang Y, Koenig LJ, Pruszynski JE, Bradley TG, Bosio JA, Liu D. Dimensional changes of upper airway after rapid maxillary expansion: A prospective cone-beam computed tomography study. Am J Orthod Dentofac Orthop. 2013;143(4):462-470. doi:10.1016/j.ajodo.2012.11.019
- Bicakci AA, Agar U, Sökücü O, Babacan H, Doruk C. Nasal airway changes due to rapid maxillary expansion timing. Angle Orthod. 2005;75(1):1-6. doi:10.1043/0003-3219(2005)075<0001:NACDTR>2.0.CO;2
- Izuka EN, Feres MFN, Pignatari SSN. Immediate impact of rapid maxillary expansion on upper airway dimensions and on the quality of life of mouth breathers. Dental Press J Orthod. 2015;20(3):43-49. doi:10.1590/2176-9451.20.3.043-049.oar
- Tecco S, Tetè S, Perillo L, Chimenti C, Festa F. Maxillary arch width changes during orthodontic treatment with fixed self-ligating and traditional straight-wire appliances. World J Orthod. 2009;10(4):290-294. http://www.ncbi.nlm.nih.gov/pubmed/20072744. Accessed February 18, 2019.
- Perlis M, Lichstein KI. Treating Sleep Disorders: Principles and Practice of Behavioral Sleep Medicine. Hoboken, New Jersey: Wiley, 2003
- Pirelli P, Saponara M, Guilleminault C. Rapid maxillary expansion (RME) for pediatric obstructive sleep apnea: a 12-year follow-up. Sleep Med. 2015;16(8):933-935. doi:10.1016/j.sleep.2015.04.012
- Kapila SD. Cone Beam Computed Tomography in Orthodontics: Indications, Insights, and Innovations. Ames, Iowa: Wiley-Blackwell; 2014. doi:10.1002/9781118674888
- Pirelli P, Saponara M, Guilleminault C. Rapid maxillary expansion in children with obstructive sleep apnea syndrome. Sleep. 2004;27(4):761-766.
- Rossini G, Cavallini C, Cassetta M, Barbato E. 3D cephalometric analysis obtained from computed tomography. Review of the literature. Ann Stomatol (Roma). 2011;2(3-4):31-39. http://www.ncbi.nlm.nih.gov/pubmed/22545187. Accessed March 23, 2019.
- Lenza MG, de O Lenza MM, Dalstra M, Melsen B, Cattaneo PM. An analysis of different approaches to the assessment of upper airway morphology: a CBCT study. Orthod Craniofac Res. 2010;13(2):96-105. doi:10.1111/j.1601-6343.2010.01482.x
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication January 22, 2020
Submitted in final revised form May 18, 2020
Accepted for publication May 29, 2020
Address correspondence to: Dr. Silvia Gianoni-Capenakas, School of Dentistry Faculty of Medicine and Dentistry, 5-488 Edmonton Clinic Health Academy, 11405-87 Avenue NW, University of Alberta, Edmonton, AB, Canada T6G 1C9; Phone: (587) 594 9947; Email: capenaka@ualberta.ca
DISCLOSURE STATEMENT
The authors have no conflicts of interest to disclose.
APPENDICES
Appendix 1Studies included in the systematic reviews |