Review Article 1, Issue 7.4
Comparing a Sibilant Phoneme Denture Bite Position With an Anterior Protrusive Mandibular Positioning Device in Oral Appliance Therapy for Dental Treatment of Obstructive Sleep Apnea: A Systematic Review
http://dx.doi.org/10.15331/jdsm.7162Enoch T. Ng, DDS1; Pedro Mayoral, DDS, MSc, PhD2; Ivonne Hernandez, DDS, MSc3; Manuel O. Lagravere, DDS, MSc, PhD 3
1 Graduate Student, School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada; 2 University Católica de Murcia UCAM, Faculty of Medicine and Dentistry, School of Dentistry, Madrid Spain; 3 School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada
ABSTRACT
Objective:
The objective of this systematic review is to provide a summary of the published literature related to the use of a sibilant phoneme technique (SPT) for determining mandibular positioning in dental sleep appliances for the management of obstructive sleep apnea (OSA), and to summarize these findings into normative ranges and protocols similar to those already established for anterior protrusive mandibular positioning.
Methods:
A search was performed on five databases: MEDLINE, Embase, Cochrane Library, Scopus, and Web of Science Core Collection. Articles not related to sleep medicine and dentistry were excluded. Only articles with a high likelihood of using a sibilant phoneme/phonetic and/or biomimetic occlusal registration with presleep and postsleep testing were selected. Review of the selected articles did not justify a meta-analysis.
Results:
Six articles met the loose inclusion criteria, of which only three articles met strict inclusion criteria. Of these three articles, two included deliberate maxillary expansion precluding the results from comparability with other mandibular positioning techniques. The remaining article was a direct comparison of the number of titrations between a SPT and a George Gauge anterior protrusive technique for mandibular positioning for dental sleep appliances.
Conclusions:
Insufficient information exists on the use of the SPT for mandibular positioning in dental sleep appliances for the management of OSA. Because of the potential for a therapeutic outcome with minimal protrusion of the mandible and therefore lower risk of developing the side effects associated with dental sleep appliances, further research should be explored in this area.
Keywords:
dental appliance, obstructive sleep apnea, phonetic bite, sibilant phoneme
Citation:
Ng ET, Mayoral P, Hernandez I, Lagravère MO. Comparing a sibilant phoneme denture bite position with an anterior protrusive mandibular positioning device in oral appliance therapy for dental treatment of obstructive sleep apnea: A systematic review. J Dent Sleep Med. 2020;7(4)
BACKGROUND
Sleep-disordered breathing is a prevalent medical condition believed to affect more than 15% of the global population.1-3 Of the different types of sleep-disordered breathing, obstructive conditions (specifically, OSA) are of particular interest to dentists. OSA is characterized by repetitive partial or complete obstructions in the upper airway, usually along the pharyngeal segment, while maintaining the thoracic effort of breathing and with associated oxygen desaturations and/or neurologic arousals.4 This collapse along the pharyngeal segment usually occurs due to a loss of muscle tonus during sleep.5 The oxygen desaturations and neuroarousals from OSA have a cascading effect on health and function, with well-established correlations between OSA and cardiovascular disease, diabetes, and daytime sleepiness, for example.6-9
Though OSA is a medical condition, one of the treatments involves dentists fabricating custom-fit dental sleep appliances.10 This therapy is widely known by several names including oral appliance therapy, mandibular appliance therapy, dental sleep appliance, mandibular repositioning appliances, mandibular repositioning therapy, or mandibular advancement appliance. Though these devices do not have the same efficacy as positive airway pressure for treating OSA in terms of apnea-hypopnea index reduction, their overall treatment effectiveness is similar because of greater patient compliance.11,12 In this article, these devices will be referred to as “dental sleep appliances” in that they are dental appliances used for the treatment of sleep breathing disorders; specifically for OSA.
There are multiple recommended treatments for OSA in adults. These include weight loss, positional therapy, positive airway pressure machines, dental sleep appliances, and surgical intervention.13-17 Although sleep physicians may make diagnoses and direct the treatments for patients with OSA, usually only licensed dentists are able to fabricate custom-fit dental sleep appliances when they are prescribed due to state and federal regulations and in accordance with American Academy of Sleep Medicine (AASM) and American Academy of Dental Sleep Medicine (AADSM) practice parameters.18-20 These appliances traditionally have been fabricated to position the mandible and tongue anteriorly to aid in maintaining patency of the pharyngeal airway.21 Although there are an assortment of different dental appliances varying in material and form, treatment parameters are generally focused around the position in which the mandible is held rather than the style of the device worn by the patient. Parameters for anterior protrusive positioning have become well established in regard to considerations such as habitual occlusion, retrusion, and protrusion.22,23 Vertical positioning has traditionally been primarily determined by material thicknesses required for the devices and/or measuring gauges, as some research indicates increased vertical dimension in appliance treatment does not correspond with increased treatment effectiveness.24-26 Anterior positioning has traditionally been primarily determined as 50% to 75% of maximum protrusion.27, 28 However, recent research has indicated minimal anterior protrusion of the mandible may be sufficient to achieve treatment success parameters for some patients.29 The conflicting article conclusions warrant further investigation to bring a consensus within the research in this area.
By necessity, most dental sleep appliances are designed to anchor off of existing dentition, an existing appliance, or dental implants. Reasonable retention may be possible for patients with an edentulous maxilla due to the prosthodontic principles related to postpalatal seal, but secured retention cannot be established on edentulous mandibles without the use of implants. However, the principles related to the fabrication of dental prosthesis may be of particular interest to dentists who provide appliance therapy for OSA. Principles in denture fabrication for the edentulous patient include the use of phonetics in determining mandibular position with the use of sibilant sounds to determine the closest speaking space in three dimensions (including corrections of pitch, roll, and yaw).30 This closest speaking space is generally considered the most anterior mandibular position beyond which may cause muscular dysfunction at rest, and may provide an alternative to the commonly accepted 50% to 75% maximum protrusion for dental sleep.31
The importance of exploring alternative mandibular positions for dental sleep appliances is vital due to common side effects associated with protrusive positioning used in oral appliance therapy and the current lack of consensus about the necessary degree of mandibular protrusion. These commonly accepted adverse effects are not all transient, and some of the long-term adverse effects include temporomandibular joint dysfunction, long-term changes to the craniofacial structure, dental occlusal changes, and other soft-tissue adverse effects.32-35 Of particular interest is that the greater the mandibular protrusive position, the greater the risks and changes associated with these long-term adverse effects. This, combined with research both for and against the need for significant mandibular protrusion, warrants further investigation into different mandibular positioning techniques.27-29 An initial mandibular position obtained with a SPT may provide the greatest therapeutic benefit for the management of OSA with the lowest risk of the accepted adverse effects commonly associated with dental sleep appliances.
METHODS
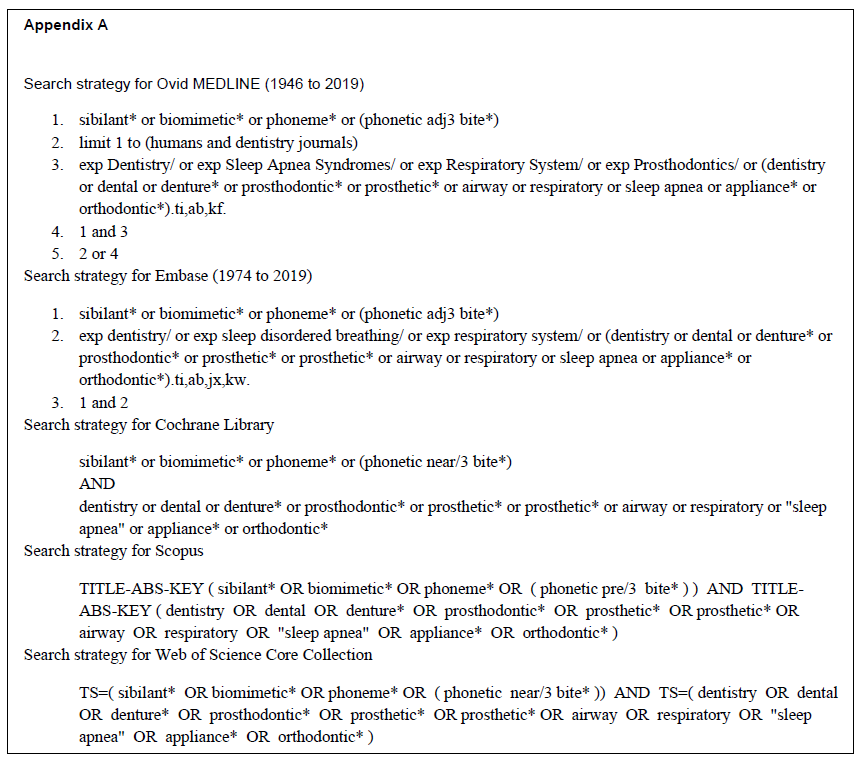
A computer-assisted literature search was done on the medical databases MEDLINE, Embase, Cochrane Library, Scopus, and Web of Science Core Collection. Determination of the appropriate syntax for each database was done with the help of a health sciences librarian. The systematic search was done on December 24, 2019. A combination of “sibilant”, “biomimetic”, “phoneme”, “phonetic bite”, “dentistry”, “denture”, “dental”, “prosthodontic”, “prosthetic”, “airway” “respiratory”, “sleep apnea”, “appliance”, “orthodontic” and their permutations were used with the appropriate syntax inputs for each database. The specific search parameters used for each database are listed in Appendix A.
Exclusion criteria included any articles not related to human subjects or dentistry.
Loose inclusion criteria included any articles related to OSA treatment in adults, probable use of a biomimetic or sibilant-type phoneme technique or device, and pretreatment and posttreatment sleep testing (in accordance with AASM and AADSM guidelines).
Strict inclusion criteria eliminated any articles that did not explicitly state the method of occlusal registration for mandibular positioning used, did not use a custom-fit titratable appliance (in accordance with AASM and AADSM guidelines), or where attempts to contact the authors for clarification on methodology were unsuccessful.
Potential references were first screened to remove all duplicates, then by title, and finally by abstracts to determine relevance. Only articles considered relevant were reviewed in full text. Articles were reviewed independently by two reviewers.
RESULTS
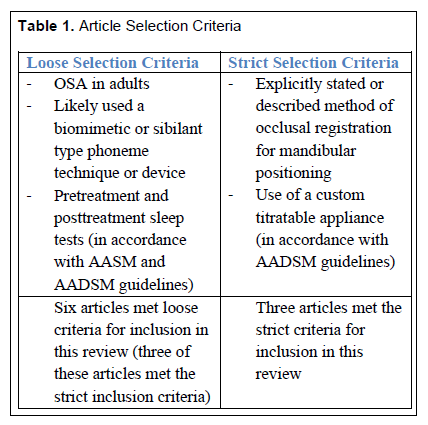
Our search yielded 1,645 articles and/or abstracts. An electronic search of duplicates in Refworks was conducted and duplicates removed, with 720 references remaining. After sorting through titles, 11 references remained. Of these 11 references, 6 were extended abstracts (such as for conference proceedings) and 5 were journal articles. The titles of the six extended abstracts were used as a search term in Google Scholar, with the first five pages of results reviewed for potentially relevant journal articles that did not appear within our original literature search. Six articles were selected from this Google Scholar search as relevant based on title and abstract. A total of 11 articles were reviewed in full text, and 6 were deemed relevant by loose inclusion criteria. Three of these articles were deemed relevant by strict inclusion criteria. Article selection criteria details are summarized in Table 1.
Table 1Article Selection Criteria |
{kind=link}
Descriptive Results
Of the three articles that met the loose inclusion criteria but not the strict inclusion criteria, two were case reports and one was a case series.36-38
Of the three articles that met the strict inclusion criteria, two were case series and one was a retrospective cohort study.39-41
Data Extractions
The collected data did not support a meta-analysis. Qualitative description of the relevant data for each study is provided in Table 2 and Table 3.
Summary Description
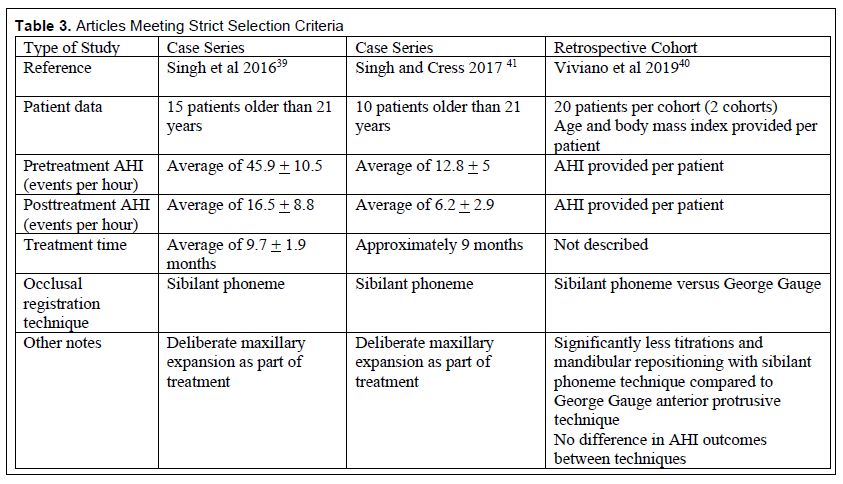
Of the three articles that met the strict inclusion criteria, two were case series and one was a retrospective cohort. Both case series included deliberate maxillary expansion and no direct comparisons with a control group. For the retrospective cohort, a direct comparison was made between the SPT and the APT for mandibular positioning in relation to the number of titrations necessary to reach treatment efficacy (defined as an AHI reduction of 50% and below 10 events per hour). Due to the deliberate maxillary expansion, data extracted from the case series studies could not be used for direct comparison between different mandibular positioning techniques.
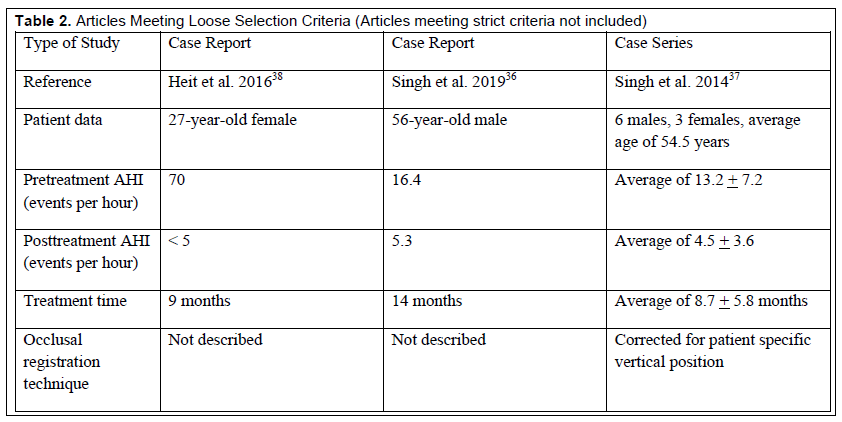
Of the three articles that met the loose inclusion criteria but not the strict inclusion criteria, two were case reports and one was a case series. The use of a biomimetic bite registration technique is noted but not described. For all three of these studies, no control group is present.
The retrospective cohort study is the only study to directly compare the SPT and the APT for mandibular positioning for dental sleep appliances. This study appears to be a pilot study and focuses on comparing the number of titrations needed to successfully manage a patient’s OSA by AHI numbers, and the results indicated that the SPT required less titration than the APT.
Table 2Articles Meeting Loose Selection Criteria (Articles meeting strict criteria not included) |
{kind=link}
Table 3Articles Meeting Strict Selection Criteria |
{kind=link}
DISCUSSION
Of the three studies we found that specifically noted the use of SPT for mandibular positioning used for dental sleep appliances in the treatment of OSA, two studies involved deliberate permanent orthopedic changes (maxillary expansion). Though it should be noted that there is nothing within the current AASM and AADSM guidelines that would explicitly exclude deliberate orthopedic remodeling (including maxillary expansion), deliberate orthopedic changes to the maxilla are a complicating factor for the study of the sibilant phoneme technique alone. Furthermore, those two studies are not comparative with other techniques due to no control group and are case series in nature. Only one article directly compared the SPT to the APT for mandibular positioning for oral appliance therapy. This study does not include deliberate orthopedic remodeling as a compounding variable of treatment.
Of the two studies that included deliberate maxillary expansion, the Daytime Nighttime Appliance was used (this is a removable appliance that is now under the brand name Vivos Therapeutics). Details on how the expansion was conducted (rate, intervals, recommended force levels, frequency of adjustments, types of adjustments, specialized materials, etc.) are not described. As well, selection criteria and/or criteria for why these particular patients were candidates for this appliance as opposed to more traditional dental sleep appliance therapy is not provided. Because this expansion device is not widely used, the lack of details severely limits the ability for nonaffiliated third-party clinicians and researchers to replicate the results of these studies and could potentially make the results questionable.
Of the cohort study directly comparing the SPT and the APT, no power analysis is provided. The study primarily focuses on comparing the number of titrations necessary to reach successful AHI management, with success being defined as an AHI reduction of 50% and below 10 events per hour. Although all clinicians were board certified and no statistical differences were found between the two cohorts pre-operatively, without a power calculation it is difficult to determine whether the sample size for this study was sufficient to draw generalized conclusions. Other limitations within this study include no description of the adjustment/titration protocols used, no description of the appliances used, and a lack of specific methodology description or references for the George Gauge and sibilant phoneme techniques. Although the difference in starting points between the two methods is briefly discussed in general terms, specifics are not described. Based on these limitations, this study appears to be a pilot study. Nevertheless, the primary result that the SPT requires less titrations to reach successful AHI management compared to the APT is compelling as this is the only study we could find that provides any direct comparisons between the APT and SPT for dental sleep appliances. From this study, despite its many limitations, one would assume that the SPT would require less mandibular advancement. However, this study does not explicitly investigate this measure.
In all three studies, OSA was diagnosed by sleep specialist physicians. Although patients within the cohort study were treated in accordance with AASM and AADSM guidelines, which emphasize an interdisciplinary collaborative approach, for the case series studies it is unknown whether patients were also evaluated for potential nasal obstructions by qualified personnel (usually otolaryngologists) and whether radiographic imaging studies were properly interpreted by qualified personnel (usually medical or dental radiologists). It is recommended for all dentists that a team approach be taken when providing dental sleep appliance therapy and that communication between the treating dentist, physician, and other clinicians involved in the patient’s care occur on a regular basis.
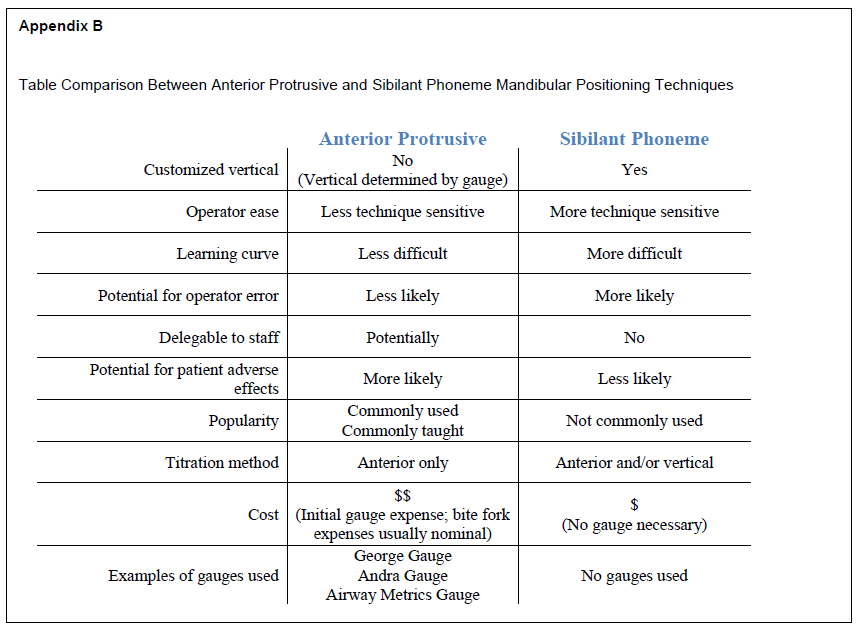
None of these studies describe the differences between the SPT and the APT in practical terms for clinicians. Although the APT generally requires a protrusive gauge, the SPT requires the use of a round bite stick. Although most protrusive gauges have a set thickness, the round bite sticks can be selected at any thickness. In both techniques, an excellent occlusal registration is vital as is recording the details of the technique and bitefork or bitestick used. Reproducing the mandibular position for the SPT requires using the same technique (having the patient repeating the same sibilant sounds) with the same dimension bitestick as originally used. Similarly, reproducing the mandibular position for the APT requires that the same gauge (for example, a George Gauge) be used with the same original technique (% or mm protrusion, based on habitual bite, maximum retrusive, or incisal edge-to-edge). A breakdown of advantages and disadvantages between the two techniques is included in Appendix B.
Although a review of the literature provides some insight on the use of phonetics in determining initial mandibular position for treatment of OSA by dental appliances, the limited number of articles published makes generalized conclusions impossible. Our results are indicative of a field in which minimal research has been done, and therefore a field ripe with opportunities for primary research to be conducted. It seems puzzling that so little information exists regarding the use of this technique, a staple in removable prosthodontics for determining a reproducible mandibular position regardless of tooth position.30, 31 Perhaps most interesting is that the use of a SPT in removable prosthodontics consistently places the mandible in the most anterior and superior position while optimizing oral muscular stability for retention of removable dentures.30 This muscular stability would potentially translate to greater muscular tonus in the oropharynx and, if the oral structures were maintained in such a position, may translate into maintained oropharyngeal muscular tonus during sleep (decreased oropharyngeal muscular collapsibility during sleep).31 This would potentially mean that significantly less mandibular protrusion may be necessary in the use of dental sleep appliances for the management of OSA, thereby decreasing the incidence and severity of adverse effects commonly associated with dental sleep appliances. Primary research into this area of study should be conducted to determine whether a SPT should be considered as an alternative to an APT for determining the initial mandibular position for dental sleep appliances.
CONCLUSION
Minimal research exists on the use of a sibilant phoneme technique for mandibular positioning for dental appliances in the treatment of OSA. Furthermore, for this limited number of studies most are confounded by deliberate maxillary expansion as part of the treatment protocols within the study, making direct comparisons with other mandibular positioning techniques for dental sleep appliances untenable. Because of the potential for a therapeutic outcome with minimal protrusion of the mandible and therefore much lower risk of developing common adverse effects associated with dental sleep appliances, further research should be conducted in this area.
ABBREVIATIONS
AASM: American Academy of Sleep Medicine
AADSM: American Academy of Dental Sleep Medicine
AHI: apnea-hypopnea index
APT: anterior protrusive technique
BMI: body mass index
OSA: obstructive sleep apnea
SPT: sibilant phoneme technique
ACKNOWLEDGMENTS
This research was conducted in part at the University of Alberta School of Dentistry and Faculty of Graduate Studies and Research.
REFERENCES
Franklin KA, Lindberg E. Obstructive sleep apnea is a common disorder in the population-a review on the epidemiology of sleep apnea. J Thorac Dis. 2015;7(8):1311-1322. doi: 10.3978/j.issn.2072-1439.2015.06.11.
Frost & Sulliven. Darien, IL: American Academy of Sleep Medicine;2016. Hidden health crisis costing America billions. Underdiagnosing and undertreating obstructive sleep apnea draining healthcare system. American Academy of Sleep Medicine. Available from: http://www.aasmnet.org/sleep-apnea-economic-impact.aspx. Accessed December 24, 2019.
Frost & Sulliven. Darien, IL: American Academy of Sleep Medicine;2016. In an age of constant activity, the solution to improving the nation’s health may lie in helping it sleep better. What benefits to patients experience in treating their obstructive sleep apnea? Available from: http://www.aasmnet.org/sleep-apnea-economic-impact.aspx. Accessed December 24, 2019.
Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an american academy of sleep medicine clinical practice guideline. J Clin Sleep Med. 2017;13(3):479-504. doi: 10.5664/jcsm.6506.
Eckert DJ. Phenotypic approaches to obstructive sleep apnoea - new pathways for targeted therapy. Sleep Med Rev. 2018;37:45-59. doi: 10.1016/j.smrv.2016.12.003.
Anker SD, von Haehling S, Germany R. Sleep-disordered breathing and cardiovascular disease. Indian Heart J. 2016;68 Suppl 1: S69-76. doi: 10.1016/j.ihj.2015.11.018.
Wang X, Bi Y, Zhang Q, Pan F. Obstructive sleep apnoea and the risk of type 2 diabetes: a meta-analysis of prospective cohort studies. Respirology. 2013;18(1):140-146. doi: 10.1111/j.1440-1843.2012.02267.x.
Gami AS, Howard DE, Olson EJ, Somers VK. Day-night pattern of sudden death in obstructive sleep apnea. N Engl J Med. 2005;352(12):1206-1214.
Young T, Finn L, Peppard PE, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep. 2008;31(8):1071-8.
Ramar K, Dort L, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: an update for 2015. J Clin Sleep Med. 2015;11(7):773-827.
Chan AS, Cistulli PA. Oral appliance treatment of obstructive sleep apnea: an update. Curr Opin Pulm Med. 2009;15(6):591-6. doi: 10.1097/MCP.0b013e3283319b12.
Sutherland K, Phillips CL, Cistulli PA. Efficacy versus effectiveness in the treatment of obstructive sleep apnea: CPAP and oral appliances. J Dent Sleep Med. 2015;2(4):175-181.
Epstein LJ, Kristo D, Strollo PJ Jr, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;15;5(3):263-76.
American Sleep Apnea Association. Sleep apnea treatment options. Available at: https://www.sleepapnea.org/treat/sleep-apnea-treatment-options. Accessed December 24, 2019.
Veasey SC, Guilleminault C, Strohl KP, Sanders MH, Ballard RD, Magalang UJ. Medical therapy for obstructive sleep apnea: a review by the medical therapy for obstructive sleep apnea task force of the standards of practice committee of the American Academy of Sleep Medicine. Sleep. 2006;29(8):1036-1044.
Caples SM, Rowley JA, Prinsell JR, et al. Surgical modifications of the upper airway for obstructive sleep apnea in adults: a systematic review and meta-analysis. Sleep. 2010;33(10):1396-1407.
Patil SP, Ayappa IA, Caples SM, Kimoff RJ, Patel SR, Harrod CG. Treatment of adult obstructive sleep apnea with positive airway pressure: an American academy of sleep medicine systematic review, meta-analysis, and GRADE assessment. J Clin Sleep Med. 2019;15(2):301-334. doi: 10.5664/jcsm.7638.
Gauthier L, Almeida F, Arcache JP, et al. Position paper by Canadian dental sleep medicine professionals regarding the role of different health care professionals in managing obstructive sleep apnea and snoring with oral appliances. Can Respir J. 2012;19(5):307-309. doi.org/10.1155/2012/631803.
Gianoni-Capenakas S, Gomes AC, Mayoral P, Miguez M, Pliska B, Lagravère M. Sleep-disordered breathing: the dentists’ role – a systematic review. J Dent Sleep Med. 2020;7(1). Available at: https://aadsm.org/journal/review_article_1_issue_71.php.
Kushida CA, Morgenthaler TI, Littner MR et al. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances: an update for 2005. Sleep. 2006;29(2):240-3.
Brown EC, Cheng S, McKenzie DK, Butler JE, Gandevia SC, Bilston LE. Tongue and lateral upper airway movement with mandibular advancement. Sleep. 2013;36(3):397-404. doi: 10.5665/sleep.2458.
Mayoral P, Lagravère MO, Míguez-Contreras M, Garcia M. Antero-posterior mandibular position at different vertical levels for mandibular advancing device design. BCM Oral Health. 2019;19(1):85. doi: 10.1186/s12903-019-0783-8.
Ippolito DR, Stipa C, Cameli M, Sorrenti G, Pelligra I, Alessandri-Bonetti G. Maximum voluntary retrusion or habitual bite position for mandibular advancement assessment in the treatment of obstructive sleep apnoea patients. J Oral Rehabil. 2019. doi: 10.1111/joor.12902. [Epub ahead of print]
Vroegop AV, Vanderveken OM, Van de Heyning PH, Braem MJ. Effects of vertical opening on pharyngeal dimensions in patients with obstructive sleep apnoea. Sleep Med. 2012;13(3):314-316. doi: 10.1016/j.sleep.2011.08.005.
Piskin B, Karakoc O, Genc H, et al. Effects of varying mandibular protrusion and degrees of vertical opening on upper airway dimensions in apneic dentate subjects. J Orofac Orthop. 2015;76(1):51-65. doi: 10.1007/s00056-014-0259-z.
Pitsis A, Darendeliler M, Gotsopoulos H, Petocz P, Cistulli P. Effect of Vertical Dimension on Efficacy of Oral Appliance Therapy in Obstructive Sleep Apnea. Am J Respir Crit Care Med.. 2002;166(6):860–864. doi: 10.1164/rccm.200204-342oc
Tegelberg A, Walker-Engström ML, Vestling O, Wilhelmsson B. Two different degrees of mandibular advancement with a dental appliance in treatment of patients with mild to moderate obstructive sleep apnea. Acta Odontol Scan. 2003;61(6):356-362.
Aarab G, Lobbezoo F, Hamburger HL, Naeije M. Effects of an oral appliance with different mandibular protrusion positions at a constant vertical dimension on obstructive sleep apnea. Clin Oral Investig. 2010;14(3):339-345. doi: 10.1007/s00784-009-0298-9.
Anitua E, Durán-Cantolla J, Almeida GZ, Alkhraisat MH. Minimizing the mandibular advancement in an oral appliance for the treatment of obstructive sleep apnea. Sleep Med. 2017;34:226-231. doi: 10.1016/j.sleep.2016.12.019.
Pound E. Let /S/ be your guide. J Prosthet Dent. 1977;38(5):482-489.
Singh GD, Olmos S. Use of a sibilant phoneme registration protocol to prevent upper airway collapse in patients with TMD. Sleep Breath. 2007;11(4):209-216.
Pliska BT, Nam H, Chen H, Lowe AA, Almeida FR. obstructive sleep apnea and mandibular advancement splints: occlusal effects and progression of changes associated with a decade of treatment. J Clin Sleep Med. 2014;10(12):1285-1291. doi: 10.5664/jcsm.4278.
Sanders AE, Essick GK, Fillingim R, et al. Sleep apnea symptoms and risk of temporomandibular disorder: OPPERA cohort. J Dent Res. 2013;97(7 Suppl):S70-S77. Doi: 10.1177/0022034513488140.
Perez CV, de Leeuw R, Okeson JP, et al. The incidence and prevalence of temporomandibular disorders and posterior open bite in patients receiving mandibular advancement device therapy for obstructive sleep apnea. Sleep Breath. 2013;17(1):323-332. doi: 10.1007/s11325-012-0695-1.
Sheats RD, Schell TG, Blanton AO, et al. Management of side effects of oral appliance therapy for sleep-disordered breathing. J Dent Sleep Med. 2017;4(4):111-125. doi:10.15331/jdsm.6746.
Singh GD, Kraver M, Chernyshev O. Restoration of sleep using a novel biomimetic protocol for adult OSA: clinical case report. Cranio. 2019;37(2):136-139. doi: 10.1080/08869634.2018.1425235.
Singh GD, Griffin TM, Chandrashekhar R. Biomimetic oral appliance therapy in adults with mild to moderate obstructive sleep apnea. Austin J Sleep Disord. 2014;1(1):5.
Heit TC, Sebastian J, Singh GD. A novel combined protocol for the resolution of severe obstructive sleep apnea. J Sleep Disord Ther. 2016;5(5). Doi: 10.4172/2167-0277.1000251
Singh GD, Griffin T, Cress SE. Biomimetic oral appliance therapy in adults with severe obstructive sleep apnea. J Sleep Disord Ther. 2016;5:1-5. doi:10.4172/2167-0277.1000227
Viviano J, Klauer D, Olmos S, Viviano JD. Retrospective comparison of the George GaugeTM registration and the sibilant phoneme registration for constructing OSA oral appliances. Cranio. 2019;26:1-9. doi: 10.1080/08869634.2019.1694776.
Singh GD, Cress SE. Biomimetic oral appliance therapy in adults with mild to moderate obstructive sleep apnea using combined maxillo-mandibular correction. J Sleep Disord Manag. 2017;3(1):1-7. doi.org/10.23937/2572-4053.1510014.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication February 4, 2020
Submitted in final revised form March 26, 2020
Accepted for publication March 27, 2020
Address correspondence to: Dr. Enoch Ng, Graduate Student, School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, 11405 - 87th Avenue, Edmonton, Alberta Canada, T6G 1C9; Email: enoch@ualberta.ca
DISCLOSURE STATEMENT
The authors have no conflicts of interest to disclose.
APPENDICES
Appendix A |
{kind=link}
Appendix B |
{kind=link}