Review Article 1, Issue 3.2
Health-Related Quality of Life Assessment Tools and SleepDisordered Breathing
http://dx.doi.org/10.15331/jdsm.5718
Rose D. Sheats, DMD, MPH
Orofacial Pain Group, University of North Carolina School of Dentistry, Chapel Hill, NC
ABSTRACT
Patients, providers, and third-party payers all have a stake in the outcomes of management of medical conditions. As part of the development of the 2015 update of clinical practice guidelines for the treatment of obstructive sleep apnea and snoring with oral appliance therapy (see reference 1), studies were reviewed that included assessments of quality of life outcomes. Patient perception of health-related quality of life has been recognized as important an outcome as the provider’s clinical assessment of treatment effectiveness. Tools have been developed to measure relevant domains that contribute to health-related quality of life. These tools may be generic or disease-specific. It is essential to note that assessments of sleep are not equivalent to assessments of health-related quality of life. This review offers for clinicians an introduction to examples of generic and obstructive sleep apnea-specific health-related quality of life instruments and also serves to distinguish such tools from those used to assess sleep.
Keywords:
health-related quality of life, sleep-disordered breathing, adult quality of life tools, pediatric quality of life tools, treatment outcomes
Citation:
Sheats RD. Health-related quality of life assessment tools and sleep-disordered breathing. Journal of Dental Sleep Medicine 2016;3(2):49–55
INTRODUCTION
In 2015 the American Academy of Sleep Medicine and the American Academy of Dental Sleep Medicine published a joint set of updated clinical practice guidelines for the use of oral appliance therapy (OAT) to treat obstructive sleep apnea and snoring.1 These guidelines were developed using a set of 11 PICO (patient, population or problem, intervention, comparison, and outcomes) questions that had arisen from previous guidelines and reviews. It is noteworthy that 4 of these 11 PICO questions (#1, 4, 5, & 10) included assessment of the impact of oral appliance therapy on quality of life measures. The final recommendations were based on extensive review of the best literature available and meta-analysis of the evidence. The evidence included outcomes from quality of life studies, signifying that quality of life assessments are considered important in judging therapeutic benefit from OAT.
Dentists who provide oral appliance therapy are familiar with the popular Epworth Sleepiness Scale2 and polysomnography but may confuse these tools with those that measure health-related quality of life. The distinction between them is important. Release of the new practice guidelines presents an opportunity for timely review of the process of formally measuring quality of life and health-related quality of life (HRQoL) and for distinguishing them from measurement of sleep quality and parameters.
Quality of life is composed of many standards including wealth, environment, happiness, social and community interactions, and physical and mental health. Many instruments or tools have been developed to measure these various dimensions that contribute to an individual’s quality of life. Health-related quality of life (HRQoL) instruments measure how a disease, disability, or disorder affects one’s life over time.3 They are also used to examine the impact of treatment on specific conditions. Physical, mental, and social health comprise important aspects of HRQoL.
Health-related quality of life tools have been developed and validated for use in both clinical and research settings. The best instruments have been rigorously studied to confirm good psychometric parameters such as validity, reliability, and internal consistency, all essential features of well-designed survey instruments.4 These instruments or tools measure multiple “domains” that refer to categories of health dimensions that compose health-related quality of life. Questions or statements, referred to as “items,” are grouped to assess each health dimension, and responses to each group of items are summarized to provide a score for that health dimension.
Responses to questions or statements are usually recorded as yes/no or scored on a Likert scale. A Likert scale is composed of ordered responses that indicate a progression such as worsening (or improvement) of symptoms. Likert scales typically have 3 to 7 options in HRQoL instruments. For example, a 4-point Likert scale measuring ability to perform a specific activity might have the following ordered categories:
- no difficulty
- a little difficulty
- moderate difficulty
- extreme difficulty.
- all the time
- a large amount of the time
- a moderate to large amount of the time
- a moderate amount of the time
- a small to moderate amount of time
- a small amount of time
- not at all.
Health-related quality of life instruments are either generic or disease or condition-specific. Generic health-related quality of life instruments refer to those questionnaires or tools that can be used across populations and facilitate cross-disease comparisons.5 Because of their general nature, however, they are not sensitive enough to measure treatment outcomes for specific diseases. Many do not include a sleep domain.
Disease-specific health-related quality of life tools focus on particular features of a specific disease or condition and have been validated to examine the impact of specific diseases and their management on patients’ lives. They provide consistent and reliable assessments of impaired HRQoL and are sensitive enough to measure changes that occur as a result of treatment over time. Instruments have been developed for both adult and pediatric assessments.
The purpose of this review is to introduce clinicians to examples of generic as well as obstructive sleep apnea-specific health-related quality of life instruments. These examples were drawn from published studies of sleep-disordered breathing research and are not intended to be all-inclusive of the breadth of such instruments that have been developed. Readers seeking to compare psychometric properties of these instruments are encouraged to review source articles or one of several excellent review articles.4–8
When comparing the merits of the following instruments, consideration should be given to the length of the instrument, the administration (interview vs self-administration), the complexity of scoring, and the ease of comparing scores over time.
GENERIC HEALTH-RELATED QUALITY OF LIFE INSTRUMENTS
Sickness Impact Profile (SIP)
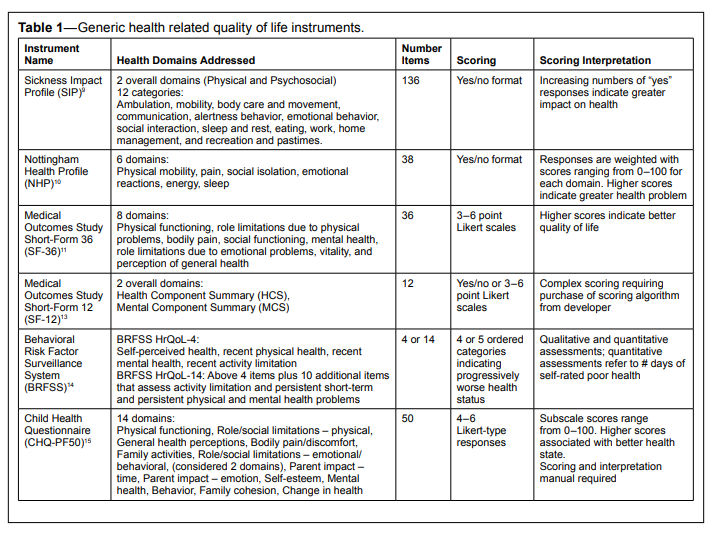
The Sickness Impact Profile (SIP) was among the earliest and most comprehensive of generic HRQoL instruments.9 It can be completed either by the patient or by an interviewer. At 136 items, it provides individual scores in each of 12 categories that it assesses: ambulation, mobility, body care and movement, communication, alertness behavior, emotional behavior, social interaction, sleep and rest, eating, work, home management, and recreation and pastimes. Response choices are binary (“Yes/No”). Individual category scores are calculated by a standardized weighting method of item responses. Summary scores for 2 domains, physical and psychosocial, are derived from the categories. A total score is also calculated and is reported as a percentage. Higher scores are associated with poorer level of health.The SIP has been used to validate subsequent HRQoL instrument development, but its length and complexity of scoring render it impractical for use in clinical practice.
The Nottingham Health Profile (NHP)
Another early instrument, the Nottingham Health Profile (NHP) was developed in Nottingham, England to include both patient perception of health as well as clinical assessment.10 It places equal or greater emphasis on the patient’s impression of the impact of disease or its treatment on health-related quality of life. The NHP measures 6 health domains via 38 self-administered yes/no questions: energy level, pain, emotional reactions, sleep, social isolation, and physical abilities. Its reliability and validity have been extensively demonstrated in a number of settings. Scores are weighted according to an algorithm and range from 0 to 100 for each domain, with higher scores representing greater perceived problems in that domain.Although patients may be amenable to completing a 38-item questionnaire, scoring of the instrument requires an algorithm that would likely be burdensome in a clinical practice.
The Medical Outcomes Study Short Form-36 (SF-36)
The Medical Outcomes Study Short Form-36 (SF-36) was developed as part of a multi-year, multi-site study to investigate variations in patient medical outcomes.11 This 36-item survey can be either interviewer- or self-administered and measures 8 health domains: physical functioning, role limitations due to physical problems, bodily pain, social functioning, mental health, role limitations due to emotional problems, vitality, and perception of general health. A score for each health domain is derived. A final question inquires about perception of change in health from the previous year. Most items are scored on a 3–6 point Likert-type scale. High scores are indicative of favorable responses in each scale.Because domains vary in the number of items from 2–10, interpretation of domain scores is not easily intuited and in clinical practice would be facilitated by the use of a table.11 The SF-36 is considered the gold standard of HRQoL instruments12 and is widely used in the validation of new HRQoL tools including each of the adult OSA-specific HRQoL instruments described below.
The Medical Outcomes Study Short Form-12 (SF-12)
The Medical Outcomes Study Short Form-12 was constructed by using regression methods to identify 12 items from the SF-36 to derive scores for a Physical Component Summary and Mental Component Summary of health-related quality of life.13 While loss of precision in assessing health occurs by reducing the number of items, the SF-12 can be administered in less than 2 minutes and is useful for population studies where cost and time may otherwise be prohibitive in the use of the SF-36. For assessments of an individual’s health, however, the 8 scales of the SF-36 are more reliable and offer a more precise representation of specific health domains. Thus is it more sensitive to changes that may occur over time or as the consequence of intervention in individual patients.Behavioral Risk Factor Surveillance System (BRFSS) Health-Related Quality of Life Module
The Centers for Disease Control (CDC) judged that the length of both the SF-36 and SF-12 rendered them impractical for large scale implementation. Thus the CDC developed a module on HRQoL composed of 4 questions to supplement the Statebased Behavioral Risk Factor Surveillance System (BRFSS). The module enabled local and State agencies to collect data on health related quality of life.14 The 4 questions on HRQoL were developed after the CDC convened several meetings, beginning in 1991, with experts in quality of life assessments, surveillance methodology, and public policy.14 The 4 questions address selfperceived general health, recent (past 30 days) physical health, recent mental health, and activity limitation. Responses are recorded as number of days in the past 30 that the respondent experienced problems in each item (except for self-perceived general health which is recorded on a 5-point Likert scale). The greater the number, the worse the perceived health.For those States that wish to collect more detailed HRQoL information, the CDC designed the HRQoL-14 as a supplemental optional 10-question module. These additional questions were validated using the SF-36 and assess Standard Activity Limitation and Healthy Days Symptoms to provide information on the burden of diseases and benefits of interventions.3
While it is tempting to utilize the CDC’s brief modules to assess HRQoL, the BRFSS health-related quality of life modules were specifically designed for population assessments, and, as such, are much too broad to be useful in evaluating individual patients. Nevertheless, the 2 modules are models with respect to desirable features of a simple, brief, and meaningful HRQoL survey.
Child Health Questionnaire - Parent Form 50 (CHQ-PF50)
This 50-item questionnaire is completed by the parent and was designed to measure HRQoL in children > 5 years of age.15 It assesses 14 physical and psychosocial domains and has been used to assess HRQoL in children with sleep disordered breathing.16 Item responses consist of 4 to 6 Likert-type choices. Subscale scores range from 0–100 with higher scores indicating better health state. This instrument does not lend itself to use in clinical practice as a scoring and interpretation manual are required.15Table 1 provides a comparison of these generic health-related quality of life instruments.
Table 1Generic health related quality of life instruments. |
{kind=link}
DISEASE-SPECIFIC HEALTH-RELATED QUALITY OF LIFE INSTRUMENTS
Surveys developed specifically to evaluate the impact of obstructive sleep apnea on HRQoL include questionnaires that have been designed separately for adult and pediatric patients. Such instruments are specific for features of obstructive sleep apnea and are thus more sensitive to changes in disease condition that occur over time. They are useful for measuring the effect of treatment and therefore are more appropriate than generic health-related quality of life tools to document therapeutic outcomes on HRQoL of individual patients. Obstructive sleep apnea-specific HRQoL tools that have been identified by review of the literature are described below. They are grouped by suitability for either adult or pediatric patients.
Adult Disease-Specific Health-Related Quality of Life Instruments
Functional Outcomes of Sleep Quality (FOSQ)
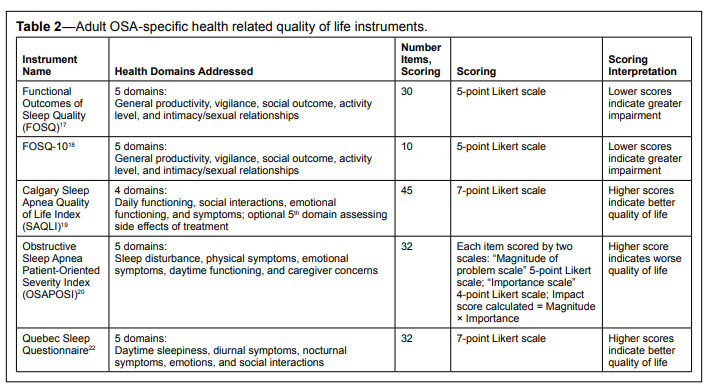
This widely-used instrument was the first disease-specific HRQoL survey that met rigorous psychometric criteria which confirmed its utility in clinical and research settings.17 First described in 1997, the FOSQ measures the impact of excessive sleepiness on functional activities of daily living. This 30-item self-administered survey measures 5 domains of health that are affected by quality of sleep and has been demonstrated to have excellent validity. The health domains assess general productivity, vigilance, social outcome, activity level, and intimacy/sexual relationships. Scores from the 5 components are used to calculate a global score.
Scoring algorithms are included with the survey and describe how to weight subscale scores and to use these weighted scores to arrive at a total score, which can range from 5 to 20. The lower the score, the greater the impact of excessive sleepiness.
FOSQ-10
A shorter version of the 30-item FOSQ was developed to facilitate implementation into clinical practices.18 This 10-item self-administered version measures the same 5 domains as the longer version and is capable of measuring meaningful changes in disease impact. The FOSQ-10 has been demonstrated to have similar psychometric properties as the longer version and is thus suitable for assessing the HRQoL impairment resulting from excessive sleepiness.
As in the original FOSQ instrument, mean weighted subscale scores are calculated to derive a total score according to the scoring algorithm. While not an arithmetically complex algorithm, effort must be expended to compute the total score.
Calgary Sleep Apnea Quality of Life Index
The Calgary Sleep Apnea Quality of Life Index (SAQLI) is an interview-administered instrument that assesses patients’ health-related quality of life over the previous 4 weeks.19 This 45-item survey assesses 4 domains: daily functioning, social interactions, emotional functioning, and symptoms. Furthermore, patients also rank the impact of each item on their functioning. The SAQLI is unique in that a fifth domain, treatment-related symptoms, can be assessed after treatment has been initiated, thus rendering this instrument especially attractive to clinicians seeking to evaluate not only patientperceived treatment effectiveness and but also side effects of treatment.
Patients rate each item on a 7-point Likert scale. Responses are weighted according to the importance of the problem that the patient assigns to each item. The somewhat elaborate scoring algorithm, however, may pose a challenge to efficient implementation in clinical practice.
Obstructive Sleep Apnea Patient-Oriented Severity Index (OSAPOSI)
The Obstructive Sleep Apnea Patient-Oriented Severity Index (OSAPOSI) was developed to measure, from the patient’s perspective, pre-treatment and post-treatment physical, functional, and emotional aspects of obstructive sleep apnea (OSA) on health-related quality of life.20 This self-administered 32-item survey is organized into 5 subscales: sleep, awake, medical, emotional and personal, and occupational impact. Each item is scored twice: once to indicate the magnitude of the problem and a second time to record the patient’s judgment of how significantly the problem affects the patient’s HRQoL. The product of these 2 scores generates a symptomimpact score for each item. The symptom-impact score for each item ranges from 0 to 20 with a maximum total score on the entire instrument ranging from 0 to 640. Higher scores indicate worse HRQoL.
In 2000 a modified version of this instrument was described and renamed the Symptoms of Nocturnal Obstruction and Related Events-25 (SNORE-25).21 Seven items were removed, and the scoring was simplified to eliminate the need for patients to provide a second scoring of importance of the problem. Instead, after recording the magnitude of each problem, patients may list up to 5 of the most significant items that they hope will improve with treatment.
Quebec Sleep Questionnaire
The Quebec Sleep Questionnaire (QSQ) utilizes 32 items to measure 5 HRQoL domains: daytime sleepiness, diurnal symptoms, nocturnal symptoms, emotions, and social interactions.22 This self-administered instrument was developed specifically to capture changes that occur in quality of life as a consequence of treatment for OSA and has been demonstrated to be sufficiently sensitive to treatment impact. The authors acknowledge the similarity of the QSQ and the SAQLI in that both instruments were designed with the specific intent of evaluating the impact of treatment on sleep disordered breathing. However, the selection of items that compose the 2 instruments was determined by different methods. The SAQLI items were identified by the “factor analysis method” (a statistical method) while the QSQ items were chosen based on the “clinical impact method” whereby clinical judgment is used to select the items that compose the different domains. Both methods are deemed valid, and while the domains significantly overlap, the specific items that are assessed differ.
Item scores range from 1 to 7. Mean scores for each domain are calculated, and a total score is derived by calculating the mean of all items. Higher scores are associated with better HRQoL.
Table 2 summarizes these adult disease specific healthrelated quality of life instruments.
Table 2Adult OSA-specific health related quality of life instruments. |
{kind=link}
Pediatric Disease-Specific Health-Related Quality Of Life Instruments
Obstructive Sleep Apnea-18 (OSA-18)
The OSA-18 is a caregiver-administered health-related quality of life assessment tool for pediatric patients with OSA.23 Its 18 items assess 5 domains: sleep disturbance, physical symptoms, emotional symptoms, daytime functioning, and caregiver concerns. Its validity and reliability have been demonstrated for pediatric OSA patients between 6 months and 12 years of age. Higher scores are associated with larger impact of OSA on HRQoL. Scores < 60 suggest a small impact on HRQoL.
Cohen’s Pediatric OSA Surgery Quality of Life Questionnaire
Cohen’s Pediatric OSA Surgery Quality of Life Questionnaire is a survey of 76 items completed by parents of children 2 to 7 years old who underwent either tracheostomy or sleep apnea surgery.24 This instrument is unique in its inclusion of a cost domain. Designed to capture pre- and post-treatment impact on HRQoL, it assesses 3 domains: physical symptoms, psychosocial function, and costs which are measured both in numbers of medical visits as well as by out-of-pocket expenses. Items are scored on a 5-point Likert scale with lower rankings being associated with better outcomes.
Table 3 summarizes these pediatric disease specific health-related quality of life instruments.
Table 3Pediatric OSA-specific health related quality of life instruments. |
{kind=link}
SLEEP ASSESSMENTS DO NOT MEASURE HEALTH-RELATED QUALITY OF LIFE
Quality of sleep is an important contributor to daytime functioning and long-term health, but the sleep domain by itself does not encompass the many dimensions that comprise HRQoL. Tools to evaluate sleep physiology, sleepiness, and sleep quality are briefly described in this review in an effort to clarify the distinction between instruments that assess sleep and those that measure HRQoL.Evaluation of sleepiness and sleep parameters provides useful information on the effectiveness of treatment in improving the sleep domain and thus sleep-associated outcomes. Dentists will recognize these tools as they are routinely included in medical referrals and patient follow-up exams. Common instruments to evaluate sleep physiology and sleepiness include polysomnography25 and the Epworth Sleepiness Scale.2 The Pittsburgh Sleep Quality Index26 is also discussed to demonstrate that sleep quality includes more domains than just sleepiness.
Polysomnography
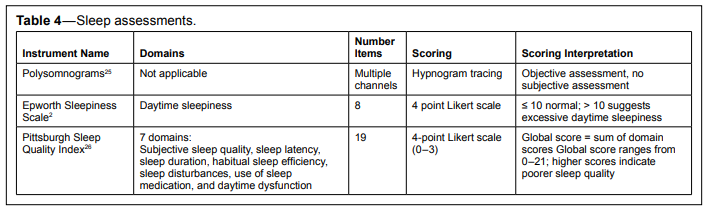
Polysomnography (PSG) provides information on sleep physiology (e.g. sleep stages, sleep architecture, sleep efficiency, oxygen levels) and is limited to documenting, in great detail, objective parameters of sleep,25 one domain among many that compose health-related quality of life. PSG parameters such as the apnea-hypopnea index, oxygen saturation levels, sleep efficiency, and sleep stages lend themselves to easy comparisons over time as long as one recognizes the limitation of night-to-night variability that occurs in subjects. PSG is useful for documenting changes in objective sleep parameters secondary to treatment intervention but does not measure changes in daytime functioning or health-related quality of life.Epworth Sleepiness Scale (ESS)
The Epworth Sleepiness Scale (ESS) is a widely used tool to measure excessive daytime sleepiness (EDS) because of its simplicity of use.2 This 8-question survey is self-administered, poses little burden to the practice, and provides a single score that can be compared over multiple visits. Scores range from 0 to 24; scores > 10 indicate the presence of EDS. While this questionnaire assesses the impact of sleepiness on daytime functioning, it is not specific for sleep disordered breathing. Other causes of EDS such as chronic or acute pain and emotional distress may better explain EDS in some patients.Pittsburgh Sleep Quality Index (PSQI)
The Pittsburgh Sleep Quality Index (PSQI) is a tool that was developed to evaluate the quality of sleep over a one-month period in psychiatric patients.26 This survey was validated using both healthy patients (“good sleepers”) and depressed patients (“poor sleepers”) and is composed of 19 self-rated items that evaluate both quantitative and qualitative information. Seven domains are assessed: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction. Item scores range from 0 to 3 per item, and a summary component score of 0–3 is determined according to the scoring algorithm for each component. The sum of the 7 component scores generates a single global score which can be used for easy longitudinal comparisons of changes in a patient’s sleep quality. Global scores range from 0–21. Higher scores indicate poorer sleep quality.Table 4 provides a summary of these sleep assessment tools. While evaluation of sleep provides useful information on a critical component of health-related quality of life, by themselves such tools are not suitable as global assessments of health-related quality of life.
Table 4Sleep assessments. |
{kind=link}
DISCUSSION
Patients, providers, and third-party payers all have a stake in the outcomes of management of medical conditions, especially with the advent of the Affordable Care Act. The Centers for Medicaid and Medicare Services (CMS) has developed a set of quality metrics to improve patient care and outcomes of many diseases.27 Quality metrics are reported to CMS via the Physician Quality Reporting System (PQRS), a program that was first implemented in 2006 as a temporary measure under the Physician Quality Reporting Initiative. In 2010 the Affordable Care Act made the program permanent, and the name was changed to the Physician Quality Reporting System. Although the reporting requirement is considered voluntary, beginning in 2015, Medicare reimbursement rates are being “negatively adjusted” for providers of Part B covered services who do not satisfactorily report quality metrics to CMS.28
The American Academy of Sleep Medicine (AASM) spearheaded the effort to develop for CMS appropriate outcome measures for the sleep apnea quality metrics.29 The AASM acknowledged that although health-related quality of life measurements are not typically collected during routine clinical evaluations, such evaluations provide one of the best assessments of effective patient treatment. The AASM report did not mandate use of a specific HRQoL tool and instead deferred to clinician choice in order to minimize the burden to the practice.
At present, no PQRS measures have been established for oral appliance therapy (OAT), thus dentists who provide this treatment to Medicare recipients are not currently required to report data to CMS on quality measures for OAT. However, the changing healthcare climate may lead to incorporation of such outcomes into future practice guidelines or reimbursement policies. At that time, it would behoove dental sleep medicine practitioners to be prepared to identify what instruments are available and to understand features of HRQoL tools that would expedite compliance with such guidelines.
SUMMARY
Of the currently available obstructive sleep apnea specific health-related quality of life instruments, dentists will likely find that the following are most user-friendly: the Functional Outcomes of Sleep Quality-10 (FOSQ-10), the Calgary Sleep Apnea Quality of Life Index (SAQLI), or the Quebec Sleep Questionnaire (QSQ). Clinicians should note, however, that scoring for all three tools necessitates calculations which may constitute a barrier to facile implementation in clinical practice.Measurement of HRQoL outcomes of OAT may be facilitated by development of a brief and clinically useful tool that can be rapidly deployed in a busy dental practice. Desirable features of such an OSA-specific HRQoL instrument with acceptable psychometric parameters include the ability to be self-administered, ease of patient completion, straightforward scoring, and a single overall score for comparison across time.
It is clear from review of these generic and OSA-specific health-related quality of life instruments that common dimensions emerge that are deemed to be important aspects of a favorable health-related quality of life. As health care providers, we should aspire not only to diminishing the unfavorable medical sequelae of sleep disordered breathing but also to enhancing our patients’ energy levels and vitality, social and community interactions, work productivity, mental alertness, and overall general well-being.
REFERENCES
2. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep 1991;14:540–5.
3. Centers for Disease Control and Prevention. Measuring healthy days: Population assessment of health-related quality of life. Atlanta, GA: Centers for Disease Control and Prevention, 2000.
4. Guyatt GH, Naylor CD, Juniper E, Heyland DK, Jaeschke R, Cook DJ. Users’ guides to the medical literature. XII. How to use articles about health-related quality of life. Evidence-Based Medicine Working Group. JAMA 1997;277:1232–7.
5. Reimer MA, Flemons WW. Quality of life in sleep disorders. Sleep Med Rev 2003;7:335–49.
6. Coons SJ, Rao S, Keininger DL, Hays RD. A comparative review of generic quality-of-life instruments. PharmacoEconomics 2000;17:13–35.
7. Moyer CA, Sonnad SS, Garetz SL, Helman JI, Chervin RD. Quality of life in obstructive sleep apnea: a systematic review of the literature. Sleep Med 2001;2:477–91.
8. Hullmann SE, Ryan JL, Ramsey RR, Chaney JM, Mullins LL. Measures of general pediatric quality of life: Child Health Questionnaire (CHQ), DISABKIDS Chronic Generic Measure (DCGM), KINDL-R, Pediatric Quality of Life Inventory (PedsQL) 4.0 Generic Core Scales, and Quality of My Life Questionnaire (QoML). Arthritis Care Res 2011;63:S420–S430.
9. Bergner M, Bobbitt RA, Carter WB, Gilson BS. The Sickness Impact Profile: development and final revision of a health status measure. Med Care 1981;19:787–805.
10. Hunt SM, McEwen J, McKenna SP. Measuring health status: a new tool for clinicians and epidemiologists. J R Coll Gen Pract 1985;35:185–8.
11. Ware JE Jr., Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992;30:473–83.
12. Weaver TE. Outcome measurement in sleep medicine practice and research. Part 1: assessment of symptoms, subjective and objective daytime sleepiness, health-related quality of life and functional status. Sleep Med Rev 2001;5:103–28.
13. Ware JE, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care 1996;34:220–33.
14. Hennessy CH, Moriarty DG, Zack MM, Scherr PA, Brackbill R. Measuring health-related quality of life for public health surveillance. Public Health Rep 1994;109:665–72.
15. HealthActCHQ. CHQ: Child Health Questionnaire (n.d.). Retrieved from http://www.healthact.com/chq.php.
16. Rosen CL, Palermo TM, Larkin EK, Redline S. Health-related quality of life and sleep-disordered breathing in children. Sleep 2002;25:657–66.
17. Weaver TE, Laizner AM, Evans LK, et al. An instrument to measure functional status outcomes for disorders of excessive sleepiness. Sleep 1997;20:835–43.
18. Chasens ER, Ratcliffe SJ, Weaver TE. Development of the FOSQ-10: a short version of the Functional Outcomes of Sleep Questionnaire. Sleep 2009;32:915–9.
19. Flemons WW, Reimer MA. Development of a disease-specific healthrelated quality of life questionnaire for sleep apnea. Am J Respir Crit Care Med 1998;158:494–503.
20. Piccirillo JF, Gates GA, White DL, Schectman KB. Obstructive sleep apnea treatment outcomes pilot study. Otolaryngol Head Neck Surg 1998;118:833–44.
21. Piccirillo JF Outcomes research and obstructive sleep apnea. Laryngoscope 2000;110:16–20.
22. Lacasse Y, Bureau MP, Series F. A new standardised and selfadministered quality of life questionnaire specific to obstructive sleep apnoea. Thorax 2004;59:494–9.
23. Franco RA Jr., Rosenfeld RM, Rao M. First place--resident clinical science award 1999. Quality of life for children with obstructive sleep apnea. Otolaryngol Head Neck Surg 2000;123:9–16.
24. Cohen SR, Suzman K, Simms C, Burstein FD, Riski J, Montgomery G. Sleep apnea surgery versus tracheostomy in children: an exploratory study of the comparative effects on quality of life. Plast Reconstr Surg 1998;102:1855–64.
25. Berry RB, Brooks R, Gamaldo CE, Harding SM, Lloyd RM, Marcus CL, Vaughn BV; for the American Academy of Sleep Medicine. AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications, Version 2.2. www.aasmnet.org. Darien, IL: American Academy of Sleep Medicine, 2015.
26. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 1989;28:193–213.
27. Centers for Medicare and Medicaid Services. Physician Quality Reporting System: Measures Codes. July 10, 2015. Retrieved from: http://www.cms.gov/Medicare/Quality-Initiatives-PatientAssessment-Instruments/PQRS/MeasuresCodes.html
28. Centers for Medicare and Medicaid Services. Physician Quality Reporting System. (n.d.) Retrieved from: http://www.cms.gov/ Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/ Payment-Adjustment-Information.html
29. Aurora RN, Collop NA, Jacobowitz O, Thomas SM, Quan SF, Aronsky AJ. Quality measures for the care of adult patients with obstructive sleep apnea. J Clin Sleep Med 2015;11:357–83.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication August, 2015
Submitted in final revised form February, 2016
Accepted for publication February, 2016
Address correspondence to: Rose D. Sheats, University of North Carolina, School of Dentistry, CB 7450, Chapel Hill, NC 27599; Email: Rose_Sheats@unc.edu
DISCLOSURE STATEMENT
This was not an industry supported study. Dr. Sheats has indicated no financial conflicts of interest.
PDF