Review Article 1, Issue 2.2
Home Sleep Testing and Sleep Apnea: A Review for Dentists
http://dx.doi.org/10.15331/jdsm.4632
Aileen L. Love, MD1 ; Samuel T. Kuna, MD1,2
ABSTRACT
Obstructive sleep apnea (OSA) is a prevalent disorder that increases the risk of hypertension, cardiovascular disease, and motor vehicle accidents. OSA is characterized by snoring, repetitive upper airway obstruction, oxygen desaturation, arousals from sleep, and daytime sleepiness. It is a condition that is underdiagnosed. OSA is most effectively treated with positive airway pressure therapy, but can alternatively be treated with oral appliance therapy for those patients with mild to moderate OSA or those intolerant of positive airway pressure. Until recently in the United States, in-laboratory polysomnography testing, a comprehensive recording of physiological signals to assess sleep stages and respiration during sleep, was the standard of care for diagnosis of OSA. Due to the demand for sleep testing and cost of in-laboratory polysomnography, unattended home sleep testing with portable monitors is increasingly being used to diagnose OSA. Evidence has shown that the use of portable monitors results in similar patient outcomes as in-laboratory testing in patients with a high pretest probability for OSA. Portable monitors are also increasingly being used in the management of patients being initiated on mandibular repositioning appliances to determine the amount of advancement needed to adequately control the sleep disordered breathing. Current guidelines recommend that home sleep testing should only be performed by sleep specialists.
Keywords:
portable monitors, obstructive sleep apnea
Citation:
Love AL, Kuna ST. Home sleep testing and sleep apnea: a review for dentists. Journal of Dental Sleep Medicine 2015;2(2):45–52.
sleep apnea (OSA) is a major public health issue. The prevalence of OSA and its associated risk for hypertension, cardiovascular disease, and motor vehicle accidents have resulted in increased demand for testing and treatment. It is currently estimated that 17% of men and 9% of women between the ages of 50 and 70 years have moderate-to-severe sleep disordered breathing.1–7 In-laboratory polysomnography (PSG) is considered the clinical standard for diagnosis of OSA, but it is expensive and requires specialized resources.8,9 Ambulatory management pathways for the diagnosis and treatment of OSA have become increasingly employed to meet this clinical demand.10–14 The American Academy of Sleep Medicine (AASM) recommends unattended home sleep testing (HST) using portable monitors (PM) for the diagnosis of OSA in conjunction with a comprehensive clinical evaluation and notes it may be used as an alternative to PSG for patients who have a high pretest probability of OSA.15 The Centers for Medicare and Medicaid Services (CMS) and private insurers are now providing coverage of continuous positive airway pressure (CPAP) and auto-titrating airway pressure (APAP) to their beneficiaries diagnosed with OSA via HST.16,17 The recent increased reliance on HST has raised important questions: Who should be tested for OSA with HST? What PM should be used? How should HST be used to evaluate management after diagnosis, e.g., adjustment of oral appliance device? Who should perform these tests?
WHO SHOULD BE TESTED FOR OSA WITH HST?
HST is a valid alternative to in-lab PSG for patients who have a high pretest probability of OSA, but is not a reliable general screening tool for OSA because it lacks sensitivity and would yield too many false negative results. In order to determine if patients are good candidates for HST, the AASM and American Academy of Dental Sleep Medicine (AADSM) recommend that patients undergo evaluation by a sleep physician prior to testing. The patient should be carefully assessed for risk factors that increase the likelihood of OSA including symptoms such as snoring, daytime sleepiness, and witnessed apneas. Other symptoms may include morning headaches, decreased concentration and memory, frequent urination during the night, sleep fragmentation, and daytime sleepiness as indicated by a score greater than 10 on the Epworth Sleepiness Scale (ESS).18 During an initial sleep evaluation, sleep physicians also screen for other sleep disorders, such as narcolepsy and periodic limb movement disorder, which can present with excessive daytime sleepiness and would not be detected on HST.A variety of questionnaires have been developed to screen patients for OSA, including the Berlin Questionnaire, Wisconsin Sleep Study questionnaire, Multivariable Apnea Prediction survey, STOP (snoring, tiredness, observed apnea, and high blood pressure) and STOP-BANG (BMI, age, neck circumference, gender) questionnaires with a moderate degree of sensitivity and specificity.19–21 Unfortunately, none of these have adequate discriminatory power to have gained widespread application in clinical medicine. Even patients who lack symptoms associated with OSA may be at increased risk. Clinicians should have a high index of suspicion of OSA in patients with obesity, an adjusted neck circumference score > 45 cm, cardiovascular diseases, type 2 diabetes, pulmonary hypertension, and a history of motor vehicle accidents. Screening should also be considered for commercial truck drivers as well as those referred for bariatric surgery.13,22 Patients who have cardiopulmonary comorbidities or morbid obesity with BMI > 50 kg/m2 may be better served by referral for PSG, since there is limited evidence to support the accuracy of HST in these specialized populations.
On physical exam, obesity, large neck circumference (> 17 inches in men, > 16 inches in women), upper airway narrowing with a Mallampati score of 3 or 4, and the presence of retrognathia and macroglossia may offer clues that a patient is at increased risk for OSA.13 The oral examination performed by dentists provides an excellent opportunity for screening patients for OSA. Patients deemed at risk by dental professionals should be referred to a sleep expert for further evaluation and testing.23PSG: TECHNICALLY COMPLICATED AND EXPENSIVE
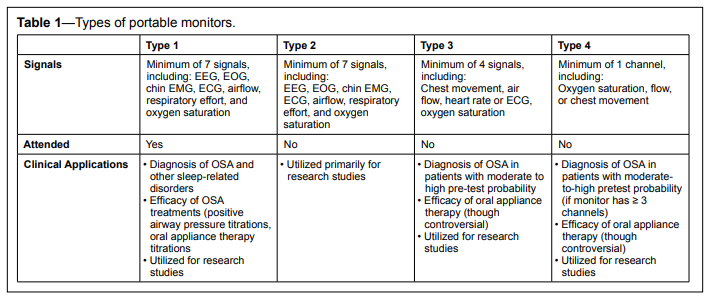
OSA is diagnosed through sleep testing.24 In-laboratory PSG has been the standard in clinical practice for the diagnosis and the initiation of PAP treatment in the United States. PSG is a complex physiological recording of neurological and respiratory signals that is typically administered in a sleep center by specially trained technologists. Patients typically spend one to two nights in a sleep center. The study records a minimum of 7 signals, including an electroencephalogram (EEG), bilateral electroculograms (EOG), chin electromyogram, airflow, oxygen saturation, respiratory effort, and electrocardiogram (ECG). Anterior tibialis EMG is also recorded to assess periodic limb movements (PLM). Video recording is also usually performed during full PSG. This is mandatory to diagnose and characterize parasomnias and periodic limb movement syndrome. An apnea-hypopnea index (AHI) is calculated by tallying the total number of apneas and hypopneas that occur throughout the recording, and then dividing by the total sleep time. OSA is diagnosed in patients with AHI > 15/h or with AHI > 5/h and associated symptoms.
If patients undergo PSG, they can have a full-night diagnostic study, and then return to the lab for a manual PAP titration study, or they may have a split-night study. During a split-night study, the first half is a devoted to diagnosis while the latter half focuses on PAP titration. The optimal PAP setting is typically defined as the lowest pressure that eliminates apneas and hypopneas in all sleep stages and body positions.
PSG can also play a role in determining the best candidates for oral appliances (OAs) used to treat OSA and evaluating their efficacy. OAs treat OSA by advancing the mandible forward and maintaining a patent airway. While AASM guidelines recommend OAs as an alternative to PAP therapy for patients with mild to moderate OSA,13 they are still not commonly used, in part because effective control of apneas and hypopneas cannot be ensured prior to device creation and adjustment. Remotely controlled mandibular positioners attached to disposable upper and lower dental trays have been developed, and these can now be used in conjunction with PSG to determine the best candidates for OAs and predict the effective protrusion position.25
Although PSG is considered the clinical standard for diagnosis of OSA, it is expensive and time consuming for patients and technical staff. Furthermore, the AHI cut points of 5, 15, and 30 for the diagnosis of mild, moderate, and severe OSA are based on expert consensus rather than evidence-based medicine,13 and the severity of AHI frequently does not correlate with the severity of a patient’s symptoms.26–30 The definition of hypopnea is also variable and can have a significant impact on PSG results. There can be a greater than 3-fold difference in the AHI, depending on whether the AASM (recommended), AASM (alternative), or Chicago definition of hypopnea is used to score events.31 To add further confusion, respiratory event related arousals (RERAs), events associated with a mild reduction in airflow followed by an arousal that do not meet the criteria for a hypopnea, are also sometimes scored, although these are not recognized by CMS.32,33 Although there is also confusion associated with scoring respiratory events on HST, considering the prevalence of OSA, demand for testing, and expense of PSG, HST is a reasonable alternative to help improve access to care.
HOME SLEEP TESTING
HST with PMs has been shown to be reliable for patients with a high pretest probability of OSA, and the AASM supports the use of HST for the diagnosis of OSA in these patients.15 The AASM developed a classification system for HST, designated as type 2, 3, and 4 (Table 1).34 PMs are typically used to obtain unattended recordings at home, making sleep testing more widely available and potentially more economical. CMS and private health insurers cover the cost of HST and PAP therapy for patients with OSA diagnosed by HST, providing that at least 3 signals are recorded by the PM.16,17Table 1Types of portable monitors. |
{kind=link}
Type 2 PMs
Type 2 PMs collect the same signals that traditional PSGs record; however, they are designed to be used outside of the sleep laboratory. Some studies suggest they may be more cost-effective than attended PSG35,36 assuming that no overnight staff is required, but they are often not practical because technologists must travel to the patient’s home to set up the leads and then retrieve the monitor the next day. They are also not adequate to evaluate patients who may be suspected of having parasomnias or hypoventilation syndromes, since video and end-tidal CO2 monitoring are not performed. Type 2 studies, however, may be useful for testing hospitalized patients in their rooms and for subjects participating in clinical research studies; research participants have more flexibility in scheduling studies and are not burdened with traveling to sleep centers.37–41
Type 3 PMs
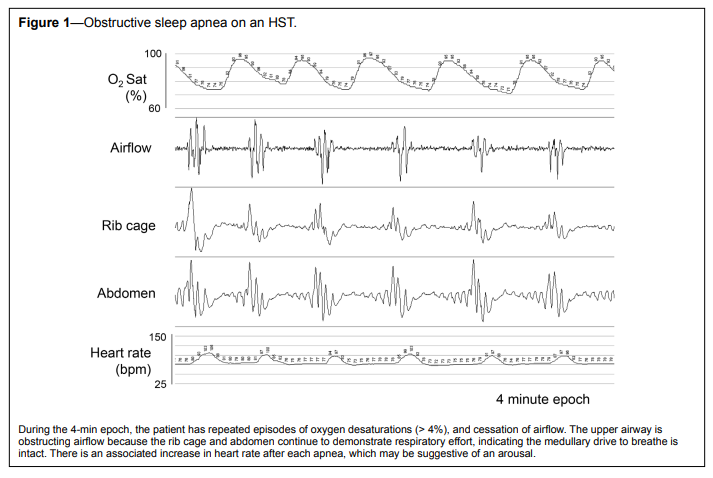
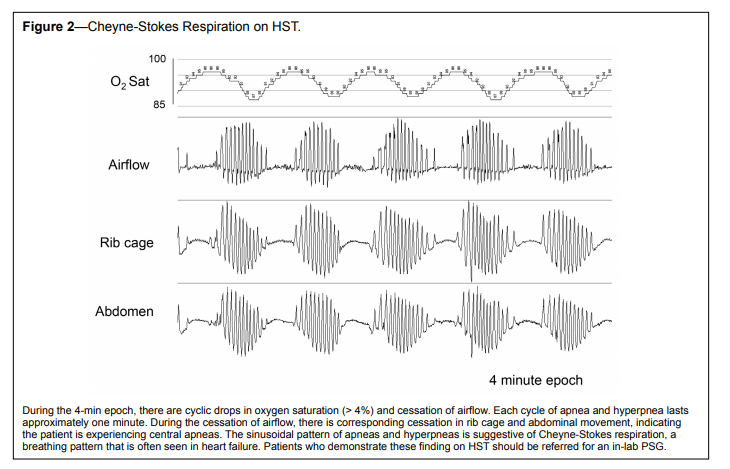
Type 3 monitors are designed to be unattended studies and are the most commonly used ambulatory monitors. They typically record between 4 and 7 signals, including oxygen saturation, 1–2 channels for respiratory movement, airflow, and heart rate. Most type 3 monitors also record body position, which is useful to detect positional sleep apnea. Patients can be instructed how to apply the sensors, and self-administration is not difficult. Since type 3 monitors (and type 4 monitors) do not record EEG, EOG, or chin muscle activity, one cannot determine when a patient is awake or asleep or the specific sleep stage. AHI is therefore calculated as the number of respiratory events per hour of recording rather than per hour of sleep. As a result, the AHI on these HSTs can underestimate the AHI on PSG. The average number of events per hour of recording on HST is sometimes referred to as the respiratory disturbance index, in order to distinguish it from the AHI calculated on a PSG. However, in this review, AHI will be used when referring to the results of both PSG and HST. The simultaneous use of wrist actigraphy, a surrogate measure of wake vs sleep states, during HST only slightly improves correlation of HST with PSG results and is not routinely used.42 Type 3 monitors, however, can distinguish between central and obstructive apneas because the monitors detect chest wall movement (Figure 1). Patients found on HST to have central sleep apnea or Cheyne-Stokes respiration, a breathing pattern frequently seen in severe heart failure, should be scheduled for a follow-up in-laboratory PSG (Figure 2).Figure 1Obstructive sleep apnea on an HST. |
{kind=link}
Figure 2Cheyne-Stokes Respiration on HST. |
{kind=link}
Type 4 PMs
Type 4 monitors typically only record 1–2 channels, usually oximetry and/or airflow. Type 4 monitors that record at least 3 channels are approved by CMS for the diagnosis of OSA. Similar to type 3 portable studies, type 4 tests tend to underestimate AHI. Type 4 tests also do not discern central from obstructive apneas and do not detect Cheyne-Stokes respiration unless they monitor respiratory effort and changes in airflow. There is some evidence that type 4 portable studies, specifically those that use a single-channel nasal airflow, may be as effective as in laboratory PSG in diagnosing OSA in a population with high pretest probability.43 Type 4 monitors seem to be the most popular type of PM used by dental practices that perform HST to confirm effectiveness of OAs.44Effectiveness of PMs
The utilization of HST presumes that it can accurately make the diagnosis of OSA without requiring an in-laboratory PSG. However, direct comparison studies between in-lab PSG and PMs are fraught with complications, primarily because differences in equipment and testing environments can significantly influence results.Technological advances have ushered in a wide variety of user-friendly PMs. At present, the current generation of devices can function as type 2–4 monitors, depending on the channels selected for recording. Studies using a particular PM cannot be generalized to other monitors—not even those in the same class—since the recording channels and sensors are often different. For instance, older studies comparing in-lab PSGs with type 3 monitor recordings relied on models that utilized an oro-nasal thermistor signal, known to be a less accurate measure of airflow than the nasal cannula pressure transducers currently used in more recent models.45,46 Even pulse oximetry can vary substantially between monitors, depending on the rate of sampling.47,48 This lack of standardization also limits the ability to perform evidence based reviews and meta-analyses of studies comparing in-lab PSG with HST. The AASM recommends that PMs use the same airflow, oximetry, and ideally, calibrated or uncalibrated inductance plethysmography for detection of respiratory effort that are conventionally used for in-laboratory PSG. Oro-nasal thermistor and nasal pressure signals to detect airflow can be used in tandem to improve testing sensitivity and protect against data loss if one signal is faulty.15 Due to technological advances in sleep medicine, however, not all PMs record airflow and chest wall movement, but rather rely on non-respiratory signals such as arterial tonometry to detect respiratory events associated with arousals.49,50 It difficult to know which combination of sensors and signals yield the most accurate results because there have not been head-to-head trials comparing PMs.
SCOPER Categorization
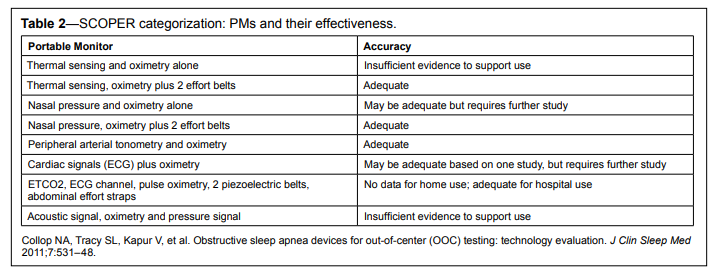
Given the plethora of PMs on the market, a novel way of evaluating HST has been devised, known as the SCOPER categorization (Sleep, Cardiovascular, Oximetry, Position, Effort and Respiratory).51 PMs were evaluated individually based on each category of SCOPER; all devices reviewed contained oximetry; devices deemed acceptable for the diagnosis of OSA had a sensitivity of 0.825 or greater when compared with an in-lab PSG (Table 2).Table 2SCOPER categorization: PMs and their effectiveness. |
{kind=link}
IN-LAB PSG VERSUS HST
The correlation between in-lab PSG and type 3 portable testing is greatest when both are carried out simultaneously in a sleep lab (i.e., in the same environment and on the same night). However, studies that utilize PMs in a sleep lab setting do not validate their use in a home environment, since correlation between in lab PSG and at-home portable studies are less robust for several important reasons. First, any study comparing in-lab PSG and home sleep studies must take into account the differences of environment (sleeping in one’s own bed as opposed to a laboratory bed, otherwise known as the “first-night effect”) and its impact on study results. Second, the method of testing itself influences the patient’s sleeping position. Patients are more likely to sleep supine during an in-lab PSG than home study because EEG lead placement and additional recording channels interfere with sleeping on one’s side or stomach.52 Since respiratory events are more likely to occur in the supine position, it is not surprising that the AHI may be higher during an in-lab study. Third, a general complication with sleep testing is the well-known night-to-night variability of AHI that is seen in all sleep testing, even with repeated in-lab PSGs.53–57 On some nights, patients may have minimal respiratory events, while on other evenings they have enough events to diagnose OSA. Therefore, studies that directly compare performance between in-lab PSG and HST should include multiple nights of both at home and in-lab testing to correct for this expected variability.TYPES OF SCORING
The scoring of a HST may be manual, totally automated, or a combination of both. In general, the scoring of sleep studies is problematic for both in-lab PSG and portable monitors. It is based on pattern recognition of uncalibrated signals, resulting in inter-scorer variability both within and between sleep laboratories. The AASM does not recognize automatic scoring without manual editing for the diagnosis of OSA. Evidence supports that manual scoring or manual editing of automated scoring is more accurate.13,58–62 Manual review of data protects against artifact mimicking respiratory events. The differences between manual and automated scoring become more significant in cases of milder OSA as opposed to those with more severe disease.63 In an effort to standardize sleep study results, the AASM recommends that (1) manual scoring assisted by computer software be performed by a qualified sleep technologist and (2) accredited comprehensive sleep medicine programs implement a quality/performance improvement program for PSG and HST to ensure inter-scorer reliability.64 Dental practices performing HST to help titrate OAs to an effective fit tend to use PM systems that provide automated scoring. There is no evidence to strongly support or discourage this practice, although, results of automated scoring should be interpreted with caution and patients should follow-up with their sleep physician once the appliance’s final fit has been established.APNEAS, HYPOPNEAS, AND SEVERITY OF OSA
Ideally, the metric for scoring apneas and hypopneas should be consistent for both in-lab PSG and HST in order to validly compare methods of testing. However, the technology and the scoring criteria used may result in a significantly different AHI for the same patient on the same night. Currently, there are no standardized guidelines for scoring HSTs. PSG results based on scoring criteria that use arousals to score hypopneas are likely to be particularly discrepant from HST results because most PMs cannot detect arousals. Although the PMs are more likely to underestimate the AHI, there are scenarios when the converse is true. For instance, short arousals following periodic limb movements are often associated with brief increases in breathing amplitude. The periods between these increases in breathing amplitude may be falsely considered as hypopneas on an HST because PMs do not have limb lead recordings. Without the EEG leads, there can also be a surprising overestimation of AHI when respiratory events are wrongly scored during awake periods. Therefore, a close collaboration with a fully equipped sleep lab should be considered mandatory for those who perform HSTs. This way, a full PSG can be ordered if the results of an HST are negative in a patient with a moderate to high pretest probability of OSA or in cases when another sleep disorder is suspected. A PSG may also be ordered if the patient is not able to perform HST due to either disability or failed attempts.PORTABLE MONITORS: CLINICAL OUTCOMES FOR OSA
Given the differences between AHI calculation on in-lab PSG and HST, there continues to be a debate if different cutoffs should be used for the diagnosis of OSA based on method of testing. In practical terms, patients at moderate to high risk for OSA who have a negative HST should be referred for an in-lab PSG to confirm the finding. Since there are inherent flaws in comparing in-lab PSG and HST, comparative effectiveness research is now helping to determine if patient-centered outcomes differ between patients diagnosed through the different testing methods.65 Several recent randomized controlled trials, using a non-inferiority design, have demonstrated that there are no clinically significant differences in PAP use and functional outcomes between the two testing pathways in patients with a high pretest probability of OSA.66–68 These studies may have limited generalizability to the population as a whole, but their design offers an alternative method for comparing diagnostic modalities. The use of PMs has recently been evaluated in patients with a mild-to-moderate probability of OSA. Masa et al. performed a randomized crossover trial comparing 3 nights of portable testing versus in-lab PSG for subjects with only a mildto-moderate suspicion of OSA. Their study found that if a PSG AHI > 5 events/h was considered diagnostic for OSA, a 3-night PM AHI of 5 events/h would effectively exclude or confirm the diagnosis of OSA.69 The 3 nights of PM testing was also found to be more cost-effective than in-lab PSG. Future studies might utilize other parameters, such as cardiovascular risks (24-h blood pressure, ECG rhythm) to evaluate the comparative effectiveness of the diagnostic pathways.HOME SLEEP TESTING IN SPECIAL POPULATIONS
HST should not be performed in patients with moderate-to-severe COPD, chronic heart failure, or chronic hypoventilation syndromes, given the lack of evidence-based medicine evaluating the use of HST to diagnosis OSA in patients with those comorbid disorders. However, type 2 or type 3 testing may be helpful in hospitalized patients who would not otherwise be able to obtain a sleep study. Patients suspected of having periodic limb movement disorder, parasomnias, circadian rhythm disorders, or narcolepsy should be referred for in-lab PSG, since PMs do not have the necessary channels to detect these sleep disorders. Although HST may be used in an elderly population for whom there is a high index of suspicion for OSA, some caution is warranted since the vast majority of patient-centered outcome studies utilizing HST enrolled a mostly male, middle-aged patient population.ROLE OF HST IN ORAL APPLIANCE MANAGEMENT
The AASM supports the use of type 3 PM to determine the effectiveness of non-PAP treatments, including OA use, upper airway surgery, and weight loss.14 Some dentists are using HST to diagnose patients with OSA, but the AASM discourages this practice. Rather, these patients should be referred to a sleep specialist for initial evaluation and testing. HST, however, is often used in tandem with clinical evaluations to determine if an OA is effectively titrated. A patient’s subjective symptoms and the objective data provided from an auto-scored PM are both used to guide advancement of device. One study suggests that a combination of monitoring a patient’s subjective symptoms and overnight oximetric scores improves the effectiveness of the OA fitting.70 Ideally, when an HST is performed with the patient using a OA, the AHI should be < 5 events/h and the patient should maintain an oxygen saturation > 90% for nearly 100% of the night. The AADSM does not officially recommend the use of HST for titration of OA as part of its treatment protocol, but the society is interested exploring its use in dental practices.71Given the flaws with auto-scoring and the adverse health outcomes that may be associated with even mild OSA, the AADSM recommends that all patients who receive OAs be scheduled for follow-up with their sleep physician after final fit has been established. The physician may order an in-lab PSG or type 3 portable test to ensure that the AHI is < 5 events/h, desaturations have been eradicated, and that additional OA adjustments are not required. The AADSM also recommends that once a final fit has been determined, that patients follow up with their dentist every 6 months for the first year, and annually thereafter, so that adherence, fit, and potential complications associated with OAs, such as TMJ and dental misalignment may be monitored. Patients with OAs should also periodically follow-up with their referring sleep physician to assess for symptoms of OSA. There are currently no data to support the use of PM by dentists to reassess the efficacy of an OA if OSA symptoms recur or to determine if a replacement OA provides adequate therapeutic benefit.
COST-EFFECTIVENESS OF HST
Several studies have demonstrated that HST has reduced costs when compared to PSG, based on the assumption that home studies do not require overnight staff or laboratory expenses. However, HST should not be assumed to be the more cost-effective simply because the upfront costs are less. If HSTs are associated with a high failure rate and missed diagnoses, cost-effectiveness would be reduced. Poor quality signals or data loss are more likely to occur with HST. To minimize failure rates, experienced sleep technologists as part of a comprehensive sleep medicine program should instruct patients about the self-application of sensors for HST.15The potential increased failure rate associated with HST would impact on the efficiency and cost-savings of the test. Simulated cost-effective analyses based on hypothetical cohorts of patients have demonstrated conflicting results. One study compared three hypothetical cohorts of patients: full night PSG versus split-night PSG and titration versus unattended portable home monitoring.72 Surprisingly, the full-night PSG was considered most cost-effective because there were fewer false negative and false positive studies. This study and others that rely on economic models, however, are based on assumptions that do not necessarily play out in the real world. Recently, a cost-effectiveness trial performed within the Veterans Healthcare System demonstrated that ambulatory management of patients with OSA using home testing measured over 2.75 years reduced sleep related costs of care by $564 when compared to in-lab management.73 There were no differences in pharmaceutical, laboratory, hospital, or other costs of care.
SUMMARY
Ambulatory monitoring using HST is now accepted as a reasonable alternative in patients with a high pretest probability of OSA. It helps expand accessibility of testing to patients, and may be more cost-effective. Current guidelines and reimbursement requirements specify that HST must be supervised by a physician and should not be performed by a dentist. The use of HST in addition to assessment of subjective symptoms may be reasonable for the use of titration of OA to ensure an adequate adjustment of the device. Once a final adjustment has been determined, patients should be referred for an in-lab PSG or HST to ensure adequacy of the OA. More research is needed comparing portable monitoring systems, cost-effectiveness of HST, and use of HST in adjusting OA to attain treatment efficacy.
REFERENCES
2. Terán-Santos J, Jiménez-Gómez A, Cordero-Guevara J. The association between sleep apnea and the risk of traffic accidents. Cooperative Group Burgos-Santander. New Eng J Med 1999;340:847–51.
3. Masa JF, Rubio M, Findley LJ. Habitually sleepy drivers have a high frequency of automobile crashes associated with respiratory disorders during sleep. Am J Respir Crit Care Med 2000;162:1407–12.
4. Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med 2000;342:1378–84.
5. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 2005;365:1046–53.
6. Parra O, Arboix A, Bechich S, et al. Time course of sleep-related breathing disorders in first-ever stroke or transient ischemic attack. Am J Respir Crit Care Med 2000;161:375–80.
7. Young T, Finn L, Peppard PE, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep 2008;31:1071–8.
8. Flemons WW, Douglas NJ, Kuna ST, et al. Access to diagnosis and treatment of patients with suspected sleep apnea. Am J Respir Crit Care Med 2004;169:668–72.
9. Pack AI. Sleep-disordered breathing: access is the issue. Am J Respir Crit Care Med 2004;169:666–7.
10. Ballester E, Solans M, Vila X, et al. Evaluation of a portable respiratory recording device for detecting apnoeas and hypopnoeas in subjects from a general population. Eur Respir J 2000;16:123–7.
11. Douglas NJ, Thomas S, Jan MA. Clinical value of polysomnography. Lancet 1992;339:347–50.
12. Calleja JM, Esnaola S, Rubio R, Duran J. Comparison of a cardiorespiratory device versus polysomnography for diagnosis of sleep apnoea. Eur Respir J 2002;20:1505–10.
13. Epstein LJ, Kristo D, Strollo PJ Jr., et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med 2009;5:263–76.
14. Trikalinos TA, Ip S, Raman G, et al. Home diagnosis of obstructive sleep apnea-hypopnea syndrome. Department of Health and Human Services, Agency for Healthcare Research and Quality, 2007. www.cms. gov/Medicare/Coverage/DeterminationProcess/dowloads/id48TA.pdf
15. Collop NA, Anderson WM, Boehlecke B, et al. Clinical guidelines for the use of unattended portable monitors in the diagnosis of obstructive sleep apnea in adult patients. Portable Monitoring Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med 2007;3:737–47.
16. Centers for Medicare and Medicaid Services. Decision memo for continuous positive airway pressure (CPAP) therapy for obstructive sleep apnea (OSA) (CAG-00093R2). March 13, 2008.
17. Centers for Medicare and Medicaid Services, Decision Memo for sleep testing for obstructive sleep apnea (OSA) (CAG-00405N). March 3, 2009.
18. Johns MW. A new method for measuring daytime sleepiness: the Epworth Sleepiness scale. Sleep 1991:14:540–5.
19. Boynton G, Vahabzadeh A, Hammoud S, Ruzicka DL, Chervin RD. Validation of the STOP-BANG Questionnaire among patients referred for suspected obstructive sleep apnea. J Sleep Disord Treat Care 2013;2(4).
20. Cowan DC, Allardice G, Macfarlane D, et al. Predicting sleep disordered breathing in outpatients with suspected OSA. BMJ Open 2014;4:e004519.
21. Maislin G, Pack AI, Kribbs NB, et al. A survey screen for prediction of apnea. Sleep 1995;18:158–66.
22. Pineda E, Fitelson D, Rahill J, et al. Assessing the adjusted neck circumference sleep apnea screening score in patients undergoing polysomnography for suspected sleep apnea. Chest 2011;140(4_ MeetingAbstracts):812A.
23. Collop N, Shafazand S. Primary vs. specialist care in management of sleep apnea. J Clin Sleep Med 2013;9:625–7.
24. Kushida CA, Littner MR, Morgenthaler T, et al. Practice parameters for the indications for polysomnography and related procedures: an update for 2005. Sleep 2005;28:499–521.
25. Remmers J, Charkhandeh S, Grosse J, et al. Remotely controlled mandibular protrusion during sleep predicts therapeutic success with oral appliances in patients with obstructive sleep apnea. Sleep 2013;36:1517–25.
26. Flemons WW, Littner MR, Rowley JA, et al. Home diagnosis of sleep apnea: a systematic review of the literature. An evidence review cosponsored by the American Academy of Sleep Medicine, the American College of Chest Physicians, and the American Thoracic Society. Chest 2003;124:1543–79.
27. Whitelaw WA, Brant RF, Flemons WW. Clinical usefulness of home oximetry compared with polysomnography for assessment of sleep apnea. Am J Respir Crit Care Med 2005;171:188–93.
28. Bennett LS, Barbour C, Langford B, Stradling JR, Davies RJ. Health status in obstructive sleep apnea: relationship with sleep fragmentation and daytime sleepiness, and effects of continuous positive airway pressure treatment. Am J Respir Crit Care Med 1999;159:1884–90.
29. Kingshott RN, Engleman HM, Deary IJ, Douglas NJ. Does arousal frequency predict daytime function? Eur Respir J 1998;12:1264–70.
30. Lloberes P, Marti S, Sampol G, et al. Predictive factors of qualityof-life improvement and continuous positive airway pressure use in patients with sleep apnea-hypopnea syndrome: study at 1 year. Chest 2004;126:1241–7.
31. Kuna ST, Benca R, Kushida CA, et al. Agreement in computer-assisted manual scoring of polysomnograms across sleep centers. Sleep 2013;36:583–9.
32. Rueland WR, Rochford PD, O’Donoghue FJ, et al. The new AASM criteria for scoring hypopneas: impact on the apnea hypopnea index. Sleep 2009;32:150–7.
33. Redline S, Kapur V, Sanders MH, et al. Effects of varying approaches for identifying respiratory disturbances on sleep apnea assessment. Am J Respir Crit Care Med 2000;161:369–74.
34. Ferber R, Millman R, Coppola M, et al. Portable recording in the assessment of obstructive sleep apnea. ASDA standards of practice. Sleep 1994;17:378–92.
35. Fry JM, DiPhillipo MA, Curran K, Goldberg R, Baran AS. Full polysomnography in the home. Sleep 1998;21:635–42.
36. Campbell AJ, Neill AM. Home set-up polysomnography in the assessment of suspected obstructive sleep apnea. J Sleep Res 2011;20:207–13.
37. Portier F, Portmann A, Czernichow P, et al. Evaluation of home versus laboratory polysomnography in the diagnosis of sleep apnea syndrome. Am J Repir Crit Care Med 2000;162:814–8.
38. Foster GD, Borradaile KE, Sanders MH, et al. A randomized study on the effect of weight loss on obstructive sleep apnea among obese patients with type 2 diabetes: the Sleep AHEAD study. Arch Intern Med 2009;169:1619–26.
39. Foster GD, Sanders MH, Millman R, et al. Obstructive sleep apnea among obese patients with type 2 diabetes. Diabetes Care 2009;32:1017–19.
40. Goodwin JL, Kaemingk KL, Fregosi RF, et al. Clinical outcomes associated with sleep-disordered breathing Caucasian and Hispanic children-- the Tucson children’s assessment of sleep apnea stud (TuCASA). Sleep 2003;26:587–91.
41. Redline S, Sanders MH, Lind BK, et al. Methods for obtaining and analyzing unattended polysomnography data for a multicenter study. Sleep Heart Health Research Group. Sleep 1998;21:759–67.
42. Garcia-Diaz E, Quintana-Gallego E, Ruiz A, et al. Respiratory polygraphy with actigraphy in the diagnosis of sleep apnea-hypopnea syndrome. Chest 2007;131:725–32.
43. Makarie Rofail L, Wong KK, Unger G, Marks GB, Grunstein RR. The role of single-channel nasal airflow pressure transducer in the diagnosis of OSA in the sleep laboratory. J Clin Sleep Med 2010;6:349–56
44. Levendowski DJ, Morgan TD, Patrickus JE, et al. In-home evaluation of efficacy and titration of a mandibular advancement device for obstructive sleep apnea. Sleep Breath 2007;11:139–47.
45. Ballester E, Badia JR, Hernández L, et al. Nasal prongs in the detection of sleep-related disordered breathing in the sleep apnoea/hypopnoea syndrome. Eur Respir J 1998;11:880–3.
46. Norman RG, Ahmed MM, Walsleben JA, et al. Detection of respiratory eventsduring NPSG: nasal cannula/pressure sensor versus thermistor. Sleep 1997;12:1175–84.
47. Davila DG, Richards KC, Marshall BL, et al. Oximeter’s acquisition parameter influences the profile of respiratory disturbances. Sleep 2003;26:91–5.
48. Davila DG, Richards KC, Marshall BL, et al. Oximeter performance: the influence of acquisition parameters. Chest 2002;122:1654–60.
49. Popovic D, King C, Guerrero M, et al. Validation of forehead venous pressure as a measure of respiratory effort for the diagnosis of sleep apnea. J Clin Monit Comput 2009;23:1–10.
50. Yalamanchali S, Farajian V, Hamilton C, et al. Diagnosis of obstructive sleep apnea by peripheral arterial tonometry: meta-analysis. JAMA Otolaryngol Head Neck Surg 2013;139:1343–50.
51. Collop NA, Tracy SL, Kapur V, et al. Obstructive sleep apnea devices for out-of-center (OOC) testing: technology evaluation. J Clin Sleep Med 2011;7:531–48
52. Metersky ML, Castriotta RJ. The effect of polysomnography on sleep position: possible implications on the diagnosis of positional obstructive sleep apnea. Respiration 1996;63:283–7.
53. Aber WR, Block AJ, Hellard DW, Webb WB. Consistency of respiratory measurements from night to night during the sleep of elderly men. Chest 1989;96:747–51.
54. Bliwise DL, Benkert RE, Ingham RH. Factors associated with nightly variability in sleep-disordered breathing in the elderly. Chest 1991;100:973–6.
55. Chediak AD, Acevedo-Crespo JC, Seiden DJ, Kim HH, Kiel MH. Nightly variability in the indices of sleep-disordered breathing in men being evaluated for impotence with consecutive night polysomnograms. Sleep 1996;19:589–92.
56. Lord S, Sawyer B, O’Connell D, et al. Night-to-night variability of disturbed breathing during sleep in an elderly community sample. Sleep 1991;14:252–8.
57. Quan SF, Griswold ME, Iber C, et al. Short-term variability of respiration and sleep during unattended nonlaboratory polysomnography--the Sleep Heart Health Study. [corrected]. Sleep 2002;25:843–9.
58. Dingli K, Coleman EL, Vennelle M, et al. Evaluation of a portable device for diagnosing the sleep apnoea/hypopnoea syndrome. Eur Respir J 2003;21:253–9.
59. Overland B, Bruskeland G, Akre H, Skatvedt O. Evaluation of a portable recording device (Reggie) with actimeter and nasopharyngeal/esophagus catheter incorporated. Respiration 2005;72:600–5.
60. Ancoli-Israel S, Mason W, Coy TV, Stepnowsky C, Clausen JL, Dimsdale J. Evaluation of sleep disordered breathing with unattended recording: the Nightwatch System. J Med Eng Tech 1997;21:10–14.
61. Cirignotta F, Mondini S, Gerardi R, Mostacci B, Sancisi E. Unreliability of automatic scoring of MESAM 4 in assessing patients with complicated obstructive sleep apnea syndrome. Chest 2001;119:1387–92.
62. Esnaola S, Duran J, Infante-Rivard C, Rubio R, Fernandez A. Diagnostic accuracy of a portable recording device (MESAM IV) in suspected obstructive sleep apnoea. Eur Respir J 1996;9:2597–605.
63. Yin M, Miyazaki S, Itasaka Y, et al. A preliminary study on application of portable monitoring for diagnosis of obstructive sleep apnea. Auris Nasus Larynx 2005;32:151–6.
64. Iber C, Ancoli-Israel S, Chesson AL, Quan SF. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications. Westchester, IL: American Academy of Sleep Medicine, 2007.
65. Chai-Coetzer CL, Antic NA, Mcevoy, RD. Ambulatory models of care for obstructive sleep apnoea: diagnosis and management. Respirology 2013;18:605–15.
66. Antic NA, Buchan C, Esterman A, et al. A randomized controlled trial of nurse-led care for symptomatic moderate-severe obstructive sleep apnea. Am J Respir Crit Care Med 2009;179:501–8.
67. Berry RB, Hill G, Thompson L, McLaurin V. Portable monitoring and auto titration versus polysomnography for the diagnosis and treatment of sleep apnea. Sleep 2008;31:1423–31
68. Mulgrew AT, Fox N, Ayas NT, Ryan CF. Diagnosis and initial management of obstructive sleep apnea without polysomnography: a randomized validation study. Ann Intern Med 2007;146:157–66.
69. Guerrero A, Embid C, Isetta V, et al. Management of sleep apnea without high pre-test probability or with comorbidities by three nights of portable sleep monitoring. Sleep 2014;37:1363–73.
70. Fleury B, Rakotonanahary D, Petelle B, et al. Mandibular advancement titration for obstructive sleep apnea: optimization of the procedure by combining clinical and oximetric parameters. Chest 2004;125:1761–7.
71. ADSM position paper: dental sleep medicine and portable monitoring. August 2005. http://www.aadsm.org/resources/pdf/ADSMPosition_ PMAug2005.pdf
72. Pietzsch JB, Garner A, Cipriano LE, Linehan JH. An integrated health-economic analysis of diagnostic and therapeutic strategies in the treatment of moderate-to-severe obstructive sleep apnea. Sleep 2011;34:695–709.
73. Atwood C, Kuna ST, Little KC. Cost Effectiveness of home management of obstructive sleep apnea: the veteran sleep apnea treatment trial. Am J Respir Crit Care Med 2014;179:501–8.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication October, 2014
Submitted in final revised form February, 2015
Accepted for publication February, 2015
Address correspondence to: Aileen L. Love, MD, Center for Sleep and Circadian Neurobiology, University of Pennsylvania, 3624 Market Street, Ste 201, Philadelphia, PA 19104
DISCLOSURE STATEMENT
This was not an industry supported study. Dr. Love has received grant support through NIH T32 HL007713. Dr. Kuna has received grant support through NIH 1P01-1HL094307, HSR&D I01, and HX000833-01.
PDF