Review Article 1, Issue 11.2
Risk Factors for OSA Observed During Orofacial Examination: A Review
http://dx.doi.org/10.15331/jdsm.7330Tanya Al-Talib, DDS, MSO, D. ABDSM1; Harmeet Chiang BDS, DDS, MS, FAGD2; Andres Pinto DMD, MPH, MSCE, MBA3; Isabel Moreno Hay DDS, PhD4; Reed Park, DDS5; Xan Goodman, SON, IHS, SPH, SDM6; Gregory Essick, DDS, PhD, D.ABDSM7
1 Associate Professor in Residence- Orthodontics, University of Nevada Las Vegas- School of Dental Medicine, 2 Associate professor- General Practice Division Chief, Department of General Practice, Virginia Commonwealth University, School of Dentistry; 3 Chair and Professor, Oral and Maxillofacial Medicine and Diagnostic Sciences Case Western School of Dental Medicine; 4 Associated Professor and Program Director, Division of Orofacial Pain, University of Kentucky ; 5 Clinical Assistant Professor Emeritus University of Iowa College of Dentistry; 6 Health Sciences Librarian, University of Nevada Las Vegas; 7 Adjunct Professor, Comprehensive Oral Health
UNC Adams School of Dentistry
ABSTRACT
The American Dental Association in 2017 and the American Academy of Dental Sleep Medicine in 2018 recommended that dentists screen all patients for sleep-related breathing disorders, such as obstructive sleep apnea (OSA). The recommendations advised proper referral of those at increased risk of OSA to a medical provider for follow-up evaluation and diagnosis. Although several approaches to screening based on validated questionnaires are recommended for clinical practice, none has been formally validated for use with dental patients. These questionnaires assess the presence of symptoms of untreated OSA, such as excessive daytime sleepiness, and of established signs of the disorder such as snoring. It is generally accepted by dentists who practice dental sleep medicine that screening should query not only symptoms and signs of untreated OSA, but also consider relevant findings from the patient’s medical history and orofacial examination. The purpose of this manuscript is to identify and review key findings in the orofacial clinical examination reportedly associated with an increased prevalence of OSA. Identification of these risk indicators may lead to the development and validation of informed screening paradigms for use in dental practice.
Keywords:
Obstructive sleep apnea(OSA), soft tissue risk factors; hard tissue risk factors
Citation:
Al-Talib T, Chiang H, Pinto A, et al. Risk factors for OSA observed during orofacial examination: A review. J Dent Sleep Med. 2024;11(2)
INTRODUCTION
The American Dental Association in 2017 and the American Academy of Dental Sleep Medicine in 2018 recommended that dentists screen all patients for sleep-related breathing disorders, such as obstructive sleep apnea (OSA). The recommendations advised proper referral of those at increased risk of OSA to a medical care professional for follow-up evaluation and diagnosis.1,2 Although several approaches to screening based on validated questionnaires are recommended for clinical practice, none has been formally validated for use with dental patients. These questionnaires assess the presence of symptoms of untreated OSA, such as excessive daytime sleepiness, and of established signs of the disorder such as snoring.3 It is generally accepted by dentists who practice dental sleep medicine that screening should query not only symptoms and signs of untreated OSA, but also consider relevant findings from the patient’s medical history and orofacial examination. The purpose of this manuscript is to identify and review key findings in the orofacial clinical examination reportedly associated with an increased prevalence of OSA. Identification of these risk indicators may lead to the development and validation of informed screening paradigms for use in dental practice.
The authors are faculty members of US dental schools and serve a role in promoting dental sleep medicine education, practice, and research at their respective institutions. Based on the literature reviewed by the authors, the parameters described in the next paragraphs are suggested as orofacial risk indicators of OSA useful in identifying individuals at increased risk of OSA. These parameters coexist with OSA, that is, their prevalence is reported to be higher in individuals with OSA than in individuals without OSA, without consideration of the cause of the association.
Soft-Tissue Risk Factors
Macroglossia
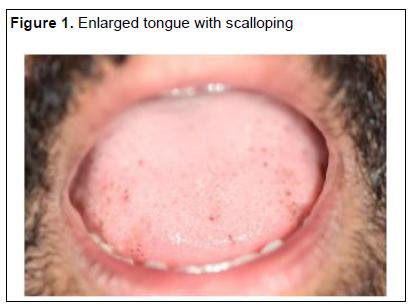
Multiple clinical and imaging studies report that macroglossia is associated with the presence and severity of OSA. Clinically, macroglossia is recognized by scalloping (indentations or crenations) along the side of the tongue, indicating that the tongue is anatomically too wide for the dental arch4 (Figure 1). Additionally, it also is identified by a "high" tongue that at rest extends onto or across the occlusal table, thus limiting the visibility of the uvula and soft palate (Mallampati score of 3 or 4)5.
In an early study, tongue scalloping (Figure 1) was more prevalent (70%) and more pronounced in patients with known or newly documented OSA in comparison with patients without documented OSA (58%).6 In two recent studies, dental school patients with tongue scalloping were three times more likely to be at risk of OSA based on the Berlin questionnaire7 or STOP questionnaire8 than patients without scalloping, after adjusting for confounding variables. A high tongue position consistent with Mallampati score of 3 was found to be an independent risk factor predicting OSA in men, but not in women.5
In place of visual examination, a recent investigation used digital morphometrics to assess tongue width and tongue thickness objectively.9 Based on standardized measurements, the authors found that a larger width and thickness were associated with an increased likelihood of OSA and a higher apnea-hypopnea index, independently of age, sex, and race. The associations were not statistically significant upon controlling for body mass index (BMI).9
The role of tongue adiposity, particularly in the posteroinferior part of the tongue, and the role of macroglossia in the pathogenesis of OSA have been studied using magnetic resonance imaging. Based on volumetric data, individuals with OSA have a larger tongue volume than individuals without OSA, independently of confounding factors.10-12 Kim et al. found that after adjusting for age, BMI, sex, and race, both tongue base volume and tongue base fat were increased significantly in patients with obesity and OSA in comparison with individuals with obesity without OSA.11 A similar result for tongue base size using ultrasonography was reported previously.13 A recent study found that reduction of tongue fat most strongly correlated with reduction in apnea-hypopnea index, before and after controlling for weight loss which indicates the role of the tongues in the pathogenesis of OSA.14 Reduction of the fat at multiple locations in the body from dieting or bariatric surgery was assessed in this landmark study.
Macroglossia contributes to the oropharyngeal crowding that promotes airway closure during sleep.15 Because macroglossia results in inferior-posterior positioning of the hyoid, the tongue muscles that maintain airway patency are placed at a mechanical disadvantage.16,17 It has also been reported that the tongues of some patients with OSA exhibit increased electromyographic activity but decreased glucose uptake, suggesting chronic denervation and reinnervation pathology. This, in turn, impairs the responsiveness of the tongue muscles to increased airway resistance, thereby contributing to the loss of airway patency.11
Tongue Tie
Tongue tie or ankyloglossia is a congenital anomaly of the tongue characterized by a short or an abnormally attached lingual frenum that restricts tongue mobility. Methods to assess the severity of tongue tie include the Kotlow free-tongue measurement and the Marchesan tongue range of motion ratio (TRMR).18-20 The free-tongue measurement is the anatomic length of the ventral surface of the tongue from the insertion of the frenulum to the tongue tip. The TRMR is the ratio between two measurements taken between the edges of the upper and lower incisor teeth during function: maximum mouth opening while the tongue tip remains on the incisive papilla and maximum mouth opening. The TRMR provides a measurement of tongue mobility that captures restriction in tongue function. TRMR greater than 80%, 50% to 80%, less than 50%, and less than 25% define grades 1, 2, 3 and 4 ankyloglossia, respectively.20 Grades 3 and 4 represent significantly below average tongue mobility characteristic of the bottom 10% of patients reporting for orthodontic evaluation. In all age groups tested, decreases in the Kotlow free-tongue measurement and in the TRMR correlated with a reduction in palatal width (transverse maxillary hypoplasia) and elongation of the soft palate – risk factors for OSA as described elsewhere in this article.21
The assertions of a relationship between tongue tie and sleep-disordered breathing are based on systematic observations from nonsyndromic pediatric patients with tongue tie and OSA, coupled with the results of older animal studies.22,23 In the studies of children, a short lingual frenum was associated with the presence of OSA independent of the presence of tonsillar hypertrophy. Patients also tended to exhibit other orofacial anomalies such as a narrow palate, long soft palate, mouth breathing, and impediments in sucking, swallowing, or speech attributed to the tongue tie. Guilleminault and colleagues concluded that restricted tongue mobility in infancy results in developmental deficiency of the maxilla and in mouth breathing, contributing to an increased collapsibility of the upper airway that persists into adulthood.22,23 However, no studies to date have demonstrated an increased prevalence of OSA in adults with a restricted tongue position. This finding has not been investigated.
Limited Visibility of the Soft Palate
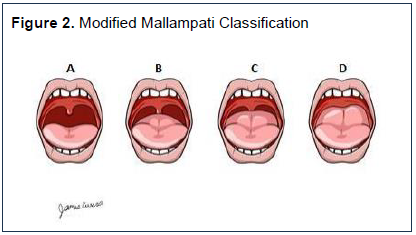
The visibility of the soft palate is commonly assessed using a modified Mallampati score. The original three-category scoring was introduced to determine the difficulty of tracheal intubation in surgery.24 The scoring was extended to four categories, as currently used, by Samsoon and Young.25 This classification accounts for the length of the soft palate and its appearance when the individual is sitting upright with the tongue protruded. A subsequent modification of the assessment with the tongue in its natural position was recommended by Friedman et al.26 In all versions, the higher the class, the less visible the uvula and soft palate. In individuals in class III, the soft palate is visible, but not the uvula, and in individuals in class IV, none of the soft palate is visible24,25 (Figure 2).
Because the Mallampati classification was originally developed to assess the difficulty of airway intubation, additional studies were conducted to determine its correlation with the severity of OSA. Mallampati class III and IV were significantly related to the presence and severity of OSA.27 It is known that a high Mallampati score in patients with OSA indicates the presence of a longer uvula and soft palate.28 Mallampati scoring has also been used to classify the tongue size: the higher the Mallampati score the larger the tongue, which in turn, may contribute to airway obstruction.29
The usefulness of the Mallampati score as an adjunct to screening for OSA with the STOP-Bang questionnaire has been demonstrated. The STOP-Bang questionnaire is a screening tool for OSA in adults that has high sensitivity but low specificity, with high potential for false-positive results.30 In one study, assessment of the modified Mallampati score (Figure 2) was shown to increase the specificity of the STOP-Bang questionnaire without changing its sensitivity. 31
Long, Broad, or Erythematous Uvula
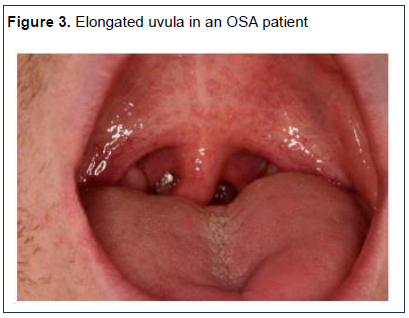
A long, broad, or erythematous uvula signifies mechanical trauma and/or inflammation and is a risk indicator for OSA. The uvula is evaluated by visual examination in the upright, or less commonly, supine position. The uvula is described as large if its length is longer than 15 mm and width is greater than 10 mm.32 Upon investigating multiple soft tissue areas, Schellenberg et al found that an enlarged uvula was a statistically significant risk factor for OSA with an odds ratio of 1.9 ( 95% CI, 1.2-2.9).33 In addition, a systematic review of 16 observational studies including data from 2604 patients found a direct relationship between an enlarged uvula and snoring and sleep-disordered breathing.32 Another study concluded that a thickened uvula may be a reliable indicator of OSA.34
The erythematous appearance of the uvula in patients with OSA is supported by histologic change associated with mechanical trauma and/or inflammation (Figure 3). These histologic changes include extensive edema of the lamina propria with vascular dilation,29 higher number of leukocytes in the lamina propria,35 and more intercellular space.36
Oropharyngeal Wall Constriction
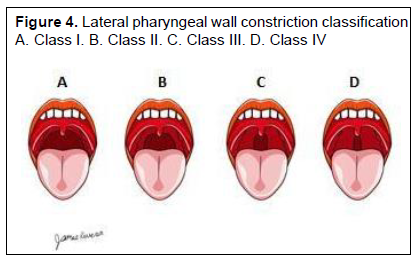
Multiple studies have assessed the role of the lateral pharyngeal wall in the risk for OSA. In one study the lateral pharyngeal wall was classified as either normal or narrow: normal when there is no soft tissue in the pharyngeal cavity and narrow when soft tissue invades the pharyngeal cavity. In this study it was found that pharyngeal narrowing was associated with the presence of OSA.28 Another study used a grading system based on the intersection of the palatopharyngeal arch with the base of the tongue to assess the extent of oropharyngeal wall constriction. In class I, the palatopharyngeal arch intersects at the lateral border of the tongue; in class II, at 25% or more of the tongue width on that side; class III, at 50% or more of the tongue width on that side; and class IV, at 75% or more of the tongue width on that side (Figure 4). The presence of class III and IV was predictive of OSA and thus found to be an anatomic risk indicator in screening individuals for OSA risk. 37
Large Tonsils
Large tonsils are often implicated as an etiologic factor underlying OSA. The Waldeyer ring is a ring of lymphoid tissue in the throat, divided into three parts: pharyngeal tonsils (adenoids in children), palatine or faucial tonsils including tubal tonsils, and lingual tonsils (submucosal lymphatic collections). Literature supports evidence that the lingual38 and/or palatine tonsil size and positioning are predictive of OSA risk in children.39 There is also some evidence that lingual and/or palatine tonsil size positioning are predictive of OSA risk in adults,33,40-42 although some studies refute this position for the lingual tonsils.43
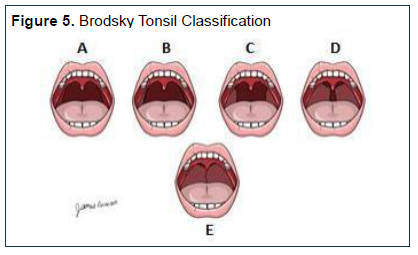
In dental practice, only the palatine tonsils are typically assessed and graded subjectively according to the oropharyngeal space obstructed by their presence as described by Brodsky: grade 0, in the fossa; grade 1+, 0– 25% obstruction; grade 2+, 25–50% obstruction; grade 3+, 51–75% obstruction; and grade 4+, 75–100% obstruction.44 Obstruction is estimated subjectively by the extent to which the tonsils extend out of its tonsillar fossa toward the uvula. The different grades of tonsillar enlargement are illustrated in Figure 5.
Schellenberg et al. found that tonsillar enlargement (grade 2 and higher) was associated with an increased risk of OSA even when the effects of BMI and neck circumference were taken into account.33 In addition, Dahlqvist et al. reported that large tonsils were significantly associated with moderate and severe OSA.5 Jara and Weaver reported that most patients with OSA with tonsils grade 1+ to 3+ and an increase in tonsil grade (Figure 5) was associated with an increase in the AHI.40
Hard Tissue Risk Factors
Noncarious Tooth Structure Loss
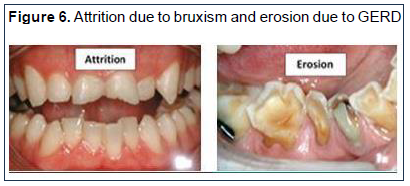
Loss of dental hard tissues including enamel, dentin, or cementum is known as tooth wear. The etiology can be multifactorial45 (Figure 6) including mechanical wear from tooth-to-tooth contact (attrition), or from extrinsic factors such as tooth brushing (abrasion), and chemical wear (erosion) from an acidic diet or gastric acid reflux (gastroesophageal reflux disease [GERD]).46
The association between noncarious tooth structure loss and sleep disorders including OSA and sleep bruxism has been widely investigated in the literature. Although attrition is commonly associated with sleep-related breathing disorders in clinical practice, only one study has established a correlation between the degree of tooth wear and the severity of the OSA. However, this study did not distinguish between mechanical and chemical tooth wear.47
It has been hypothesized that tooth wear and OSA can be indirectly associated due to the common coexistence of GERD and OSA.48,49 Therefore, it is recommended that patients with evidence of dental erosion be screened for GERD as well as OSA. In addition, a possible association between sleep bruxism and GERD has been suggested. An increase of rhythmic masticatory muscle activity is observed in patients with a decreased esophageal pH during sleep,49 and it has been hypothesized that sleep bruxism can play a protective role stimulating salivary flow in an attempt to restore the pH balance.45,50 Thus, the relationship between dental erosion, dental attrition, GERD, sleep bruxism, and OSA is complex, making it difficult, if not impossible, to evaluate the association between only two of these disorders in isolation.45
Last, the link between sleep bruxism and sleep-related breathing disorders is debated in the literature. Even though the two sleep disorders appear to coexist,51,52 no evidence of a temporal association53 or casualty between them has been clearly established.50,54 It is noteworthy that tooth wear has not proved to be a validated clinical sign of sleep bruxism, and that polysomnography is needed to establish a definitive diagnosis for sleep bruxism.45,51 Consistent with this conclusion, a recent systematic review by da Coste Lopes et al concluded that there is not enough evidence to support an association between sleep bruxism and OSA.55
Other recent studies, however, demonstrate an increased prevalence of sleep bruxism for a particular subset (endotype) of individuals with OSA.56 This work suggests that sleep bruxism may be more prevalent only in individuals who have milder forms of OSA, individuals for whom sleep bruxism is likely to be effective in maintaining or reestablishing airway patency.57 Accordingly, further studies are needed to better elucidate the association between sleep bruxism and distinct endotypes of OSA.
Large Mandibular Tori
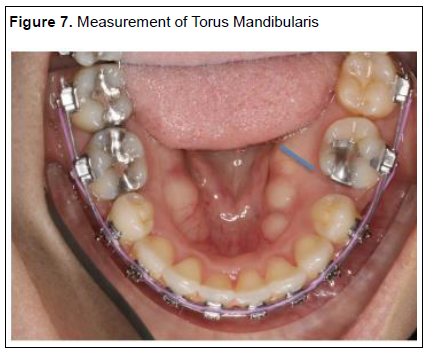
Mandibular tori are bony exostoses formed mostly by cortical bone with very limited bone marrow located on the lingual surface of the lower jaw.58,59 Different classifications of their size have been proposed. Agbaje et al characterized mandibular tori in three sizes: small (1 to 2 cm), medium (2 to 3 cm), and large (> 2 cm) and that can be solitary or multiple.60 In contrast, Ruangsri et al proposed six levels based on diameter and location: level 1 (<6 mm) unilateral, level 2 (<6 mm) bilateral, level 3 (6 mm-2 cm) unilateral, level 4 (6 mm-2 cm) bilateral, level 5 (>2 cm) unilateral, and level 6 (>2 cm) bilateral.28 Alternatively, torus size has been judged by its thickness (the greatest prominence)61 as measured on a study cast using a digital caliper (Figure 7).
Large mandibular tori have often been associated with the presence of OSA.28 Ruangsri reported that torus man-dibularis had a high prevalence among individuals with OSA in comparison with individuals without OSA. Large mandibular tori bilaterally were associated with the pres-ence of OSA. It was also emphasized in this study that dif-ferent ethnicities may exhibit different prevalence rates.62 Ahn et al concluded that the presence of mandibular tori influences the severity of OSA and increases the likelihood of positional OSA.62 In addition, Palm et al found that thick tori were more common in individuals who had mild to moderate OSA (respiratory disturbance index of <30) than in individuals with severe OSA. Moreover, in this study sample, thick tori predicted a complete response to oral appliance therapy independent of potentially confounding variables such as age, sex, and BMI.61
Steep Mandibular Plane Angle
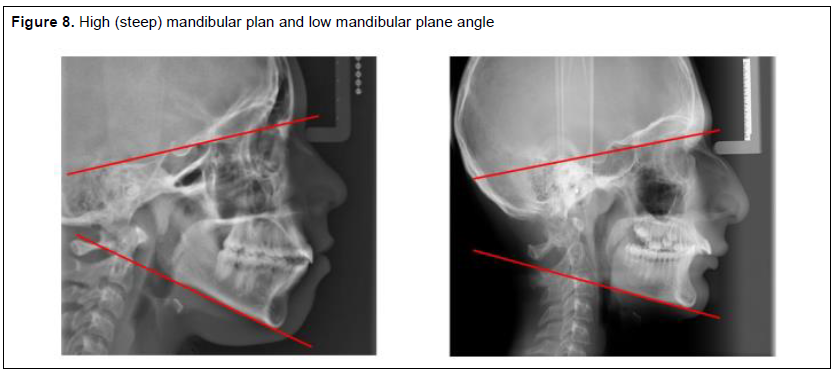
A steep mandibular plane angle (MPA) has often been associated with increased risk of OSA. The mandibular plane is tangent to the gonial angle and the lowest point of the symphysis.63 The MPA is calculated by relating the mandibular plane to the Frankfort horizontal plane.63 A steep MPA is present in hyperdivergent skeletal patterns with a long anterior lower facial height and open bite tendency, lip incompetence, and is often associated with class II malocclusion. These are typically classified as a “high angle case'' or “long face syndrome”.64 High (steep) MPAs can occur in both retrusive and protrusive faces. The range of readings range from 17° to 28° with an average of 21.9°.63
The MPA can be assessed clinically by placing the side of the index finger or a ruler along the lower border of the mandible and the Frankfort plane. When the angle is average, the point of intersection of the two planes should be just behind the back of the head. The location of this point of intersection can be seen more posteriorly in low versus high angle cases (Figure 8). In the presence of facial asymmetry, the right and left mandibular planes may differ and must be assessed separately. The MPA is reduced in short-faced individuals and increased in long-faced individuals, and the Frankfort plane may not be horizontal with the head in a natural head position. It is best to use a true horizontal line as a reference.
Craniofacial abnormalities in individuals with OSA are present in both the lower and upper pharynx. The two most common lower pharyngeal changes include elongated pharyngeal structures and a propensity toward a narrow posterior airway space resulting from an inferiorly positioned hyoid bone and a steep MPA. These abnormalities may be genetic or may be secondary to prolonged or recurrent episodes of increased airway resistance, such as tonsillar hypertrophy leading to altered growth patterns. The end result is lower airway instability due to the inability to maintain tongue posture in the supine position.65
Johns et al compared lateral cephalometric radiographs of young individuals with OSA to those of patients without apnea who are snorers and control patients. Univariate logistic regression analysis of 19 craniofacial measurements revealed a significantly steeper MPA in the OSA group.65 A study by Lowe et al demonstrated that individuals with OSA have a steep MPA, which may reduce the upper airway dimensions and result in impaired upper airway stability.66 In yet another study that included cephalometric measurements, Tsuchiya et al classified OSA subtypes in 84 adult males using a cluster analysis on the basis of apnea index and BMI. The authors reported that the males with a high apnea index and low BMI ratio have a vertical skeletal discrepancy of a steep MPA as one of the contributors.67
Retrognathia/ Micrognathia
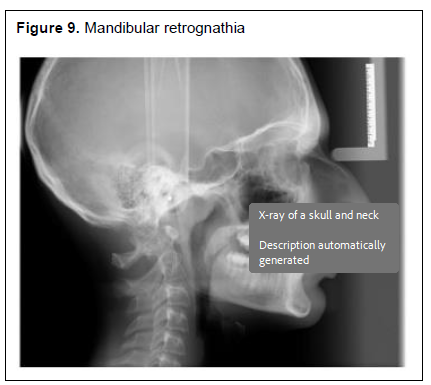
Retrognathia and micrognathia (Figure 9) are well recognized craniofacial risk factors for OSA. Both retrognathia and micrognathia are facial deformities related to the development or position of the fetal mandible. Retrognathia is characterized by an abnormal retrusive position of the mandible in relation to the maxilla, whereas micrognathia refers to a mandibular hypoplasia and is most often associated with craniofacial genetic syndromes.68 From a lateral view, individuals with retrognathia or micrognathia present an exaggerated convex facial profile. This often includes a skeletal deficiency, especially of the mandible in the anteroposterior plane of growth.69 On standard lateral cephalometry, retrognathia is defined as greater than 0.5 cm of retroposition of the gnathion (the most inferior point in the contour of the chin) relative to the plane of the nasion (the deepest point of the superior aspect of the nasal bone, ie, the base of the nose).69 Upon physical examination, in the patient with retrognathia, the thyromental distance will be less than the standard three fingers’ breadth, or approximately 7 mm.70-72
Retrognathia and micrognathia have been associated with an increased prevalence of OSA in both children and adults. The prevalence of sleep apnea in the pediatric population is between 1% and 4 %.73 Several studies have found retrognathia and micrognathia in cephalometric measurements of non-syndromic individuals with OSA.74 For example, Lowe et al showed that individuals with OSA had smaller and more posteriorly positioned mandibles, which decreased the overall airway space as seen on lateral cephalometry.75 In another study, significant differences in dentofacial morphology were reported between 12 individuals with obesity and 13 individuals without obesity. Particularly in individuals without obesity who have OSA, there were significant morphologic abnormalities that included retrognathia and micrognathia, possibly contributing to the pathogenesis of their OSA.72 Similar findings were reported in a larger Japanese, population- based study of 103 individuals with and without obesity and who had OSA.76
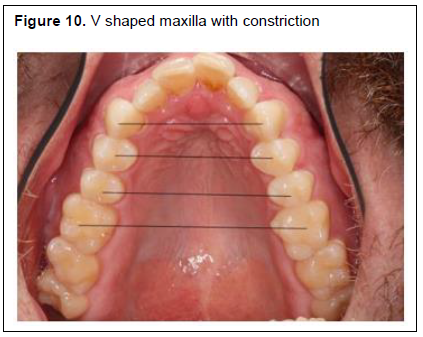
Maxillary Constriction With High Vaulted Palate
Maxillary constriction with a high vaulted palate is identified clinically by the presence of a high palatal vault and narrow and tapered maxillary arch (V-shaped). It may be associated with unilateral or bilateral posterior crossbite, or not associated with crossbite due to a compensatory constriction of the mandibular arch (lingually tipped mandibular molars).77
A quantitative characterization of maxillary constriction can be determined upon consideration of three orthodontic measurements without consideration of the palatal height (Figure 10):
1. Intercanine distance, defined as the distance between the centroids of the canines, as described by Moyers et al.78
2. Interpremolar distance at the first and second premolar regions, defined as the linear distance between the centroids of the first and second premolars.
3. Intermolar distance, defined as the linear measurement between the centroids of the first permanent molars.79
Forster et al studied several patients preorthodontically and concluded the average widths in the intercanine, interpremolar (first), interpremolar (second), and intermolar sites in a normal mandibular plane angle patients were 33.5 mm, 39.9 mm, 44.3 mm, and 45.8 mm, respectively. It is noteworthy that the authors found a weak but negative correlation between the MPA and the arch width; hence, individuals with a steeper MPA tended to present with a decreased arch width.80
In addition, a number of studies have suggested an association between maxillary constriction and sleep-disordered breathing. Seto et al suggested that individuals with OSA have narrower and more tapered arches as compared with individuals without OSA.79 A study of Japanese males with OSA found that maxillary constriction was associated with more severe OSA.81 Although the precise role of the constriction in the pathogenesis of OSA is not known,77 individuals with maxillary constrictions (Figure 10) seem to have greater nasal resistance leading to mouth breathing, both of which are related to OSA.82
Other studies have focused on posterior crossbite or a deep palate as a surrogate of maxillary constriction. One study reported an increased prevalence of posterior crossbite in children with OSA compared with control patients without OSA.83 Johal and Conaghan found that deep palate was an independent predictor of high risk for OSA in adults, the palate being significantly deeper in the OSA group than in the control group. 84
Craniofacial Syndromes
Craniofacial syndromes result from genetic variations that alter the normal development of facial structures. Altered growth and development of the face affect the mid to lower facial position in comparison with the cranial base. Therefore, any alteration of the normal growth and development of the craniofacial structures poses a risk for developing airway impairment. Mandibular micrognathia is a common risk factor present in several craniofacial syndromes. Dimensional or positional changes of the mandible have a significant effect on the position of the tongue, hence, a plausible risk for posterior airway collapse. A narrow palate also poses a challenge for tongue position and spacing, requiring the patient to move the tongue posteriorly in search of functional space.85 Changes in upper airway (nasal) anatomy in patients with maxillary clefts also affect adequate perfusion and may cause oral breathing habits, with deleterious effects on dental development and positioning.85
A dramatic example of these changes is the Pierre Robin sequence, among others. In children born with Pierre Robin syndrome, which includes genetically determined micrognathic /retrognathic changes, there is a 20-fold to 40-fold increase in sleep-disordered breathing prevalence.86 Similarly, children with Down syndrome are at a higher risk for the development of OSA, with reported wide prevalence between 20% and 80% in different cohorts. The phenotype in Down syndrome, with midface hypoplasia,87 macroglossia,88 and obesity,89 makes this disorder particularly susceptible to OSA. Further, case control studies of individuals with Down syndrome with and without OSA demonstrate a significant differential in cognitive performance and IQ. Children with syndromic craniofacial disorders are at increased risk for OSA and other breathing abnormalities, and pose a diagnostic challenge, as conducting sleep studies may not be practical in these individuals.90
Figure 1Enlarged tongue with scalloping |
{kind=link}
Figure 2Modified Mallampati Classification |
{kind=link}
Figure 3Elongated uvula in an OSA patient |
{kind=link}
Figure 4Lateral pharyngeal wall constriction classification A. Class I. B. Class II. C. Class III. D. Class IV |
{kind=link}
Figure 5Brodsky Tonsil Classification |
{kind=link}
Figure 6Attrition due to bruxism and erosion due to GERD |
{kind=link}
Figure 7Measurement of Torus Mandibularis |
{kind=link}
Figure 8High (steep) mandibular plan and low mandibular plane angle |
{kind=link}
Figure 9Mandibular retrognathia |
{kind=link}
Figure 10V shaped maxilla with constriction |
{kind=link}
Table 1Summary of soft and hard tissue risk factors with references |
{kind=link}
SUMMARY
Although several screening questionnaires for OSA have been validated for use in medical practice, clinicians should realize that these have not been validated for use in the dental setting in which patient demographics and health status differ. Using these questionnaires alone can result in false negative and positive outcomes and thus, in underreferral or overreferral of patients for further evaluation by medical providers. The lack of validation constitutes a barrier to the effective implementation of screening for OSA in the clinical practice of dentistry.
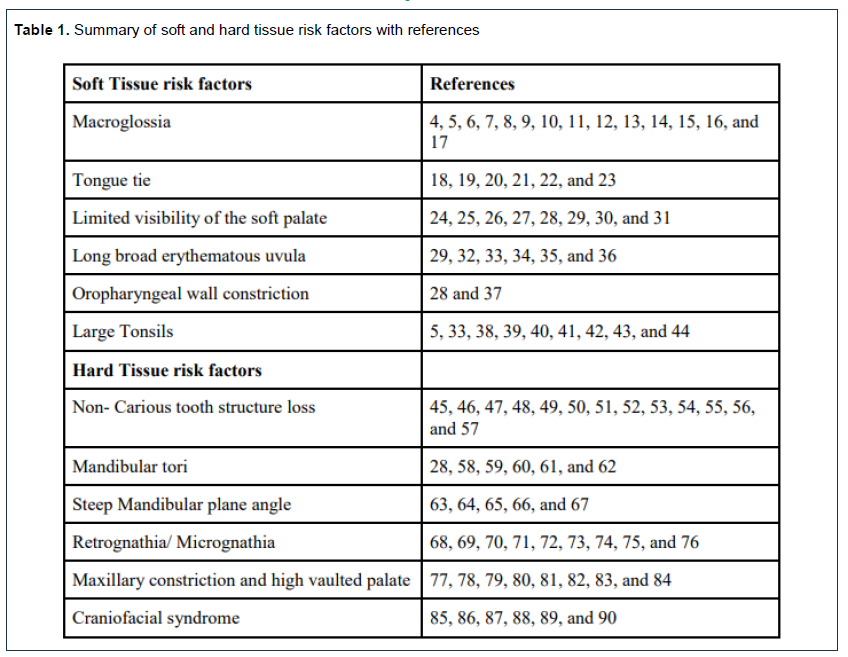
The premise of this review is that screening patients for OSA can be accomplished more accurately by combining the results from a screening questionnaire validated for nondental patient groups with information from the soft and hard tissue craniofacial examination. For example, the STOP-Bang screening questionnaire has been shown to have very high sensitivity in identifying individuals in nondental patient groups with OSA but mediocre to poor diagnostic specificity.1,2,30,31 In using this questionnaire alone to screen dental patients, there is potentially a high risk of false-positive outcomes resulting in the unnecessary and costly referral of these patients for follow-up evaluation by a medical provider and a diagnostic sleep study. For patients who screen with either three or four affirmative responses – consistent with an intermediate risk of OSA – the presence of orofacial risk factors for OSA would support the dentist’s decision to refer these patients for further evaluation rather than to wait and reevaluate later. The literature review highlighted craniofacial and soft tissue risk indicators that are observed during the clinical examination of dental patients (Table 1): macroglossia, tongue tie, limited visibility of soft palate, enlarged or erythematous uvula, oropharyngeal wall constriction, and large tonsils. Additionally, hard tissue risk indicators include noncarious tooth structure loss, large mandibular tori, steep mandibular plane angle, retrognathia/ micrognathia, maxillary constriction, and high vaulted palate. The evidence underlying these as risk indicators in adults varies from controversial (eg, for tongue tie) to very strong (e.g., for macroglossia). Research is needed to validate existing screening questionnaires for use with dental patients and to determine whether the sensitivity and specificity of the testing are improved upon inclusion of one or more of these risk indicators (refer to Table 1 summary).
ACKNOWLEDGEMENTS
The authors thank Dr. Rose Sheats for reviewing this manuscript and Mr. James Rivera for providing the artwork for the Brodsky tonsils classification, oropharyngeal wall constriction, and the modified Mallampati classifications.
REFERENCES
- Nagappa M, Liao P, Wong J, et al. Validation of the STOP-bang questionnaire as a screening tool for obstructive sleep apnea among different populations: A systematic review and meta-analysis. PLoS One. 2015;10(12):e0143697. doi: 10.1371/journal.pone.0143697 [doi].
- Farney RJ, Walker BS, Farney RM, Snow GL, Walker JM. The STOP-bang equivalent model and prediction of severity of obstructive sleep apnea: Relation to polysomnographic measurements of the apnea/hypopnea index. J Clin Sleep Med. 2011;7(5):459-65B. doi: 10.5664/JCSM.1306 [doi].
- Levine M, Bennett K, Cantwell M, Postol K, Schwartz D. Dental sleep medicine standards for screening, treating, and managing adults with sleep-related breathing disorders. J Dent Sleep Medicine. 2018;5(3):61-8.
- Yanagisawa K, Takagi I, Sakurai K. Influence of tongue pressure and width on tongue indentation formation. J Oral Rehabil. 2007;34(11):827-834. doi: JOR1734 [pii].
- Dahlqvist J, Dahlqvist A, Marklund M, Berggren D, Stenlund H, Franklin KA. Physical findings in the upper airways related to obstructive sleep apnea in men and women. Acta Otolaryngol. 2007;127(6):623-630. doi: 778652639 [pii].
- Weiss TM, Atanasov S, Calhoun KH. The association of tongue scalloping with obstructive sleep apnea and related sleep pathology. Otolaryngol Head Neck Surg. 2005;133(6):966-971. doi: S0194-5998(05)01504-4 [pii].
- Al-Jewair TS, Nazir MA, Al-Masoud NN, Alqahtani ND. Prevalence and risks of habitual snoring and obstructive sleep apnea symptoms in adult dental patients. Saudi Med J. 2016;37(2):183-190. doi: 10.15537/smj.2016.2.12852 [doi].
- Kale SS, Kakodkar P, Shetiya SH. Assessment of oral findings of dental patients who screen high and no risk for obstructive sleep apnea (OSA) reporting to a dental college - A cross sectional study. Sleep Sci. 2018;11(2):112-117. doi: 10.5935/1984-0063.20180021 [doi].
- Schwab RJ, Leinwand SE, Bearn CB, et al. Digital morphometrics: A new upper airway phenotyping paradigm in OSA. Chest. 2017;152(2):330-342. doi: S0012-3692(17)30925-X [pii].
- Schwab RJ, Pasirstein M, Pierson R, et al. Identification of upper airway anatomic risk factors for obstructive sleep apnea with volumetric magnetic resonance imaging. Am J Respir Crit Care Med. 2003;168(5):522-530. doi: 200208-866OC [pii].
- Kim AM, Keenan BT, Jackson N, et al. Metabolic activity of the tongue in obstructive sleep apnea. A novel application of FDG positron emission tomography imaging. Am J Respir Crit Care Med. 2014;189(11):1416-1425. doi: 10.1164/rccm.201310-1753OC [doi].
- Barrera JE, Pau CY, Forest VI, Holbrook AB, Popelka GR. Anatomic measures of upper airway structures in obstructive sleep apnea. World J Otorhinolaryngol Head Neck Surg. 2017;3(2):85-91. doi: 10.1016/j.wjorl.2017.05.002 [doi].
- Lahav Y, Rosenzweig E, Heyman Z, Doljansky J, Green A, Dagan Y. Tongue base ultrasound: A diagnostic tool for predicting obstructive sleep apnea. Ann Otol Rhinol Laryngol. 2009;118(3):179-184. doi: 10.1177/000348940911800304 [doi].
- Wang SH, Keenan BT, Wiemken A, et al. Effect of weight loss on upper airway anatomy and the apnea-hypopnea index. the importance of tongue fat. Am J Respir Crit Care Med. 2020;201(6):718-727. doi: 10.1164/rccm.201903-0692OC [doi].
- Ito E, Tsuiki S, Maeda K, Okajima I, Inoue Y. Oropharyngeal crowding closely relates to aggravation of OSA. Chest. 2016;150(2):346-352. doi: S0012-3692(16)41643-0 [pii].
- Chi L, Comyn FL, Mitra N, et al. Identification of craniofacial risk factors for obstructive sleep apnoea using three-dimensional MRI. Eur Respir J. 2011;38(2):348-358. doi: 10.1183/09031936.00119210 [doi].
- Kim AM, Keenan BT, Jackson N, et al. Tongue fat and its relationship to obstructive sleep apnea. Sleep. 2014;37(10):1639-1648. doi: 10.5665/sleep.4072 [doi].
- Kotlow LA. Ankyloglossia (tongue-tie): A diagnostic and treatment quandary. Quintessence Int. 1999;30(4):259-262.
- Marchesan IQ. Lingual frenulum: Quantitative evaluation proposal. Int J Orofacial Myology. 2005; 31:39-48.
- Yoon A, Zaghi S, Weitzman R, et al. Toward a functional definition of ankyloglossia: Validating current grading scales for lingual frenulum length and tongue mobility in 1052 subjects. Sleep Breath. 2017;21(3):767-775. doi: 10.1007/s11325-016-1452-7 [doi].
- Yoon AJ, Zaghi S, Ha S, Law CS, Guilleminault C, Liu SY. Ankyloglossia as a risk factor for maxillary hypoplasia and soft palate elongation: A functional - morphological study. Orthod Craniofac Res. 2017;20(4):237-244. doi: 10.1111/ocr.12206 [doi].
- Huang S, YS Q, Berkowski JA, Guilleminault C. Short lingual frenulum and obstructive sleep apnea in children. Int J Pediatr Res. 2015;1(1):1-4. https://clinmedjournals.org/articles/ijpr/ijpr-1-003.pdf.
- Guilleminault C, Huseni S, Lo L. A frequent phenotype for paediatric sleep apnoea: Short lingual frenulum. ERJ Open Res. 2016;2(3):00043-2016. eCollection 2016 Jul. doi: 00043-2016 [pii].
- Mallampati SR, Gatt SP, Gugino LD, et al. A clinical sign to predict difficult tracheal intubation: A prospective study. Can Anaesth Soc J. 1985;32(4):429-434. doi: 10.1007/BF03011357 [doi].
- Samsoon GL, Young JR. Difficult tracheal intubation: A retrospective study. Anaesthesia. 1987;42(5):487-490. doi: 10.1111/j.1365-2044.1987.tb04039.x [doi].
- Friedman M, Hamilton C, Samuelson CG, Lundgren ME, Pott T. Diagnostic value of the friedman tongue position and mallampati classification for obstructive sleep apnea: A meta-analysis. Otolaryngol Head Neck Surg. 2013;148(4):540-547. doi: 10.1177/0194599812473413 [doi].
- Karakoc O, Akcam T, Gerek M, Genc H, Ozgen F. The upper airway evaluation of habitual snorers and obstructive sleep apnea patients. ORL J Otorhinolaryngol Relat Spec. 2012;74(3):136-140. doi: 10.1159/000337134 [doi].
- Ruangsri S, Jorns TP, Puasiri S, Luecha T, Chaithap C, Sawanyawisuth K. Which oropharyngeal factors are significant risk factors for obstructive sleep apnea? an age-matched study and dentist perspectives. Nat Sci Sleep. 2016;8:215-219. doi: 10.2147/NSS.S96450 [doi].
- Woodson BT, Garancis JC, Toohill RJ. Histopathologic changes in snoring and obstructive sleep apnea syndrome. Laryngoscope. 1991;101(12 Pt 1):1318-1322. doi: 10.1002/lary.5541011211 [doi].
- Chung F, Abdullah HR, Liao P. STOP-bang questionnaire: A practical approach to screen for obstructive sleep apnea. Chest. 2016;149(3):631-638. doi: S0012-3692(15)00018-5 [pii].
- Avincsal MO, Dinc ME, Ulusoy S, Dalgic A, Ozdemir C, Develioglu ON. Modified mallampati score improves specificity of STOP-BANG questionnaire for obstructive sleep apnea. J Craniofac Surg. 2017;28(4):904-908. doi: 10.1097/SCS.0000000000003513 [doi].
- Chang ET, Baik G, Torre C, Brietzke SE, Camacho M. The relationship of the uvula with snoring and obstructive sleep apnea: A systematic review. Sleep Breath. 2018;22(4):955-961. doi: 10.1007/s11325-018-1651-5 [doi].
- Schellenberg JB, Maislin G, Schwab RJ. Physical findings and the risk for obstructive sleep apnea. the importance of oropharyngeal structures. Am J Respir Crit Care Med. 2000;162(2 Pt 1):740-748. doi: 10.1164/ajrccm.162.2.9908123 [doi].
- Araz O, Karaman A, Esdur V, et al. The association of OSAS and uvula: The role of MRI in this egg-chicken problem in OSAS. Sleep Breath. 2020;24(2):465-470. doi: 10.1007/s11325-019-01879-3 [doi].
- Sekosan M, Zakkar M, Wenig BL, Olopade CO, Rubinstein I. Inflammation in the uvula mucosa of patients with obstructive sleep apnea. Laryngoscope. 1996;106(8):1018-1020. doi: 10.1097/00005537-199608000-00021 [doi].
- Hamans EP, Van Marck EA, De Backer WA, Creten W, Van de Heyning PH. Morphometric analysis of the uvula in patients with sleep-related breathing disorders. Eur Arch Otorhinolaryngol. 2000;257(4):232-236. doi: 10.1007/s004050050229 [doi].
- Tsai WH, Remmers JE, Brant R, Flemons WW, Davies J, Macarthur CA. A decision rule for diagnostic testing in obstructive sleep apnea. Am J Respir Crit Care Med. 2003;167(10):1427-1432.
- DeMarcantonio MA, Senser E, Meinzen-Derr J, Roetting N, Shott S, Ishman SL. The safety and efficacy of pediatric lingual tonsillectomy. Int J Pediatr Otorhinolaryngol. 2016;91:6-10. doi: S0165-5876(16)30337-8 [pii].
- Nolan J, Brietzke SE. Systematic review of pediatric tonsil size and polysomnogram-measured obstructive sleep apnea severity. Otolaryngol Head Neck Surg. 2011;144(6):844-850. doi: 10.1177/0194599811400683 [doi].
- Jara SM, Weaver EM. Association of palatine tonsil size and obstructive sleep apnea in adults. Laryngoscope. 2018;128(4):1002-1006. doi: 10.1002/lary.26928 [doi].
- Smith MM, Peterson E, Yaremchuk KL. The role of tonsillectomy in adults with tonsillar hypertrophy and obstructive sleep apnea. Otolaryngol Head Neck Surg. 2017;157(2):331-335. doi: 10.1177/0194599817698671 [doi].
- Camacho M, Li D, Kawai M, et al. Tonsillectomy for adult obstructive sleep apnea: A systematic review and meta-analysis. Laryngoscope. 2016;126(9):2176-2186. doi: 10.1002/lary.25931 [doi].
- Tang JA, Friedman M. Incidence of lingual tonsil hypertrophy in adults with and without obstructive sleep apnea. Otolaryngol Head Neck Surg. 2018;158(2):391-394. doi: 10.1177/0194599817740333 [doi].
- Brodsky L. Modern assessment of tonsils and adenoids. Pediatr Clin North Am. 1989;36(6):1551-1569. doi: S0031-3955(16)36806-7 [pii].
- Wetselaar P, Manfredini D, Ahlberg J, et al. Associations between tooth wear and dental sleep disorders: A narrative overview. J Oral Rehabil. 2019;46(8):765-775. doi: 10.1111/joor.12807 [doi].
- Marsicano JA, de Moura-Grec PG, Bonato RC, Sales-Peres Mde C, Sales-Peres A, Sales-Peres SH. Gastroesophageal reflux, dental erosion, and halitosis in epidemiological surveys: A systematic review. Eur J Gastroenterol Hepatol. 2013;25(2):135-141. doi: 10.1097/MEG.0b013e32835ae8f7 [doi].
- Durán-Cantolla J, Alkhraisat MH, Martínez-Null C, Aguirre JJ, Guinea ER, Anitua E. Frequency of obstructive sleep apnea syndrome in dental patients with tooth wear. J Clin Sleep Med. 2015;11(4):445-450. doi: 10.5664/jcsm.4602 [doi].
- Teklu M, Gouveia CJ, Yalamanchili A, et al. Predicting obstructive sleep apnea status with the reflux symptom index in a sleep study population. Laryngoscope. 2020;130(12):E952-E957. doi: 10.1002/lary.28592 [doi].
- Erdem D, Yılmaz YF, Özcan M, Titiz A, Özlügedik S, Ünal A. Correlation of sleep-disordered breathing and laryngopharyngeal reflux: A two-channel triple-sensor pHmetry catheter study. Eur Arch Otorhinolaryngol. 2018;275(10):2585-2592. doi: 10.1007/s00405-018-5107-0 [doi].
- Balasubramaniam R, Klasser GD, Cistulli PA, Lavigne GJ. The link between sleep bruxism, sleep disordered breathing and temporomandibular disorders: An evidence-based review. J Dent Sleep Med. 2014;1(1):27-37.
- Tan MWY, Yap AU, Chua AP, Wong JCM, Parot MVJ, Tan KBC. Prevalence of sleep bruxism and its association with obstructive sleep apnea in adult patients: A retrospective polysomnographic investigation. J Oral Facial Pain Headache. 2019;33(3):269–277. doi: 10.11607/ofph.2068 [doi].
- Saito M, Yamaguchi T, Mikami S, et al. Weak association between sleep bruxism and obstructive sleep apnea. A sleep laboratory study. Sleep Breath. 2016;20(2):703-709. doi: 10.1007/s11325-015-1284-x [doi].
- Manfredini D, Guarda-Nardini L, Marchese-Ragona R, Lobbezoo F. Theories on possible temporal relationships between sleep bruxism and obstructive sleep apnea events. an expert opinion. Sleep Breath. 2015;19(4):1459-1465. doi: 10.1007/s11325-015-1163-5 [doi].
- Jokubauskas L, Baltrušaityt A. Relationship between obstructive sleep apnoea syndrome and sleep bruxism: A systematic review. J Oral Rehabil. 2017;44(2):144-153. doi: 10.1111/joor.12468 [doi].
- da Costa Lopes AJ, Cunha TCA, Monteiro MCM, Serra-Negra JM, Cabral LC, Júnior PCS. Is there an association between sleep bruxism and obstructive sleep apnea syndrome? A systematic review. Sleep Breath. 2020;24(3):913-921
- Martynowicz H, Gac P, Brzecka A, et al. The relationship between sleep bruxism and obstructive sleep apnea based on polysomnographic findings. J Clin Med. 2019;8(10):1653. doi: 10.3390/jcm8101653. doi: 10.3390/jcm8101653 [doi].
- Essick GC, Raphael K, Sanders AE, Lavigne GL. Orofacial pain/temporomandibular disorders in relation to sleep disordered breathing and sleep bruxism. In: Principles and Practice of Sleep Medicine, ed 6. Elsevier; 2017:1435-1444.e5. https://www.sciencedirect.com/science/article/pii/B978032324288200146X.
- Drennan MR. The torus mandibularis in the bushman. J Anat. 1937;72(Pt 1):66.
- Garcia AS, Gonzalez JM, Rivadeneira AS, Roladan LO. Current status of the torus palatinus and torus mandibularis. Med Oral Patol Oral Cir Bucal. 2010;15(2):e353-360.
- Agbaje JO, Arwojolu MO, Kolude B, Lawoyin JO. Torus palatinus and torus mandibularis in a Nigerian population. African Journal of Oral Health. 2005;2(1-2):30-36. https://www.ajol.info/index.php/ajoh/article/view/57001.
- Palm E, Franklin KA, Marklund M. Mandibular tori size is related to obstructive sleep apnea and treatment success with an oral appliance. Sleep Breath. 2014;18(2):431-438. https://doi.org/10.1007/s11325-013-0905-5. doi: 10.1007/s11325-013-0905-5.
- Ahn SH, Ha JG, Kim JW, et al. Torus mandibularis affects the severity and position-dependent sleep apnoea in non-obese patients. Clin Otolaryngol. 2019;44(3):279-285. doi: 10.1111/coa.13286 [doi].
- Jacobson A. Radiographic cephalometry: from basics to videoimaging. 1995.
- Ayoub A, Khambay B, Benington P, Green L, Moos K, Walker F. Handbook of Orthognathic Treatment: A Team Approach. John Wiley & Sons; 2013.
- Johns FR, Strollo PJ Jr, Buckley M, Constantino J. The influence of craniofacial structure on obstructive sleep apnea in young adults. J Oral Maxillofac Surg. 1998;56(5):596-602. doi: S0278-2391(98)90459-1 [pii].
- Lowe AA, Santamaria JD, Fleetham JA, Price C. Facial morphology and obstructive sleep apnea. Am J Orthod Dentofacial Orthop. 1986;90(6):484-491. doi: 0889-5406(86)90108-3 [pii].
- Tsuchiya M, Lowe AA, Pae EK, Fleetham JA. Obstructive sleep apnea subtypes by cluster analysis. Am J Orthod Dentofacial Orthop. 1992;101(6):533-542. doi: 0889-5406(92)70128-W [pii].
- Sanz-Cortés M, Gómez O, Puerto B. Micrognathia and retrognathia. In: Obstetric Imaging: Fetal Diagnosis and Care. Elsevier, 2018, pp 321-327. e1.
- Jenzer AC, Schlam M. Retrognathia. In: StatPearls StatPearls Publishing LLC, 2022. NBK538303 [bookaccession].
- Cattano D, Killoran PV, Cai C, et al. Difficult mask ventilation in general surgical population: Observation of risk factors and predictors. F1000Research. 2014(3):204. https://f1000research.com/articles/3-204/v1.
- Shah PN, Sundaram V. Incidence and predictors of difficult mask ventilation and intubation. J Anaesthesiol Clin Pharmacol. 2012;28(4):451-455. doi: 10.4103/0970-9185.101901 [doi].
- Peterson GN, Domino KB, Caplan RA, Posner KL, Lee LA, Cheney FW. Management of the difficult airway: A closed claims analysis. Anesthesiology. 2005;103(1):33-39. doi: 00000542-200507000-00009 [pii].
- Lumeng JC, Chervin RD. Epidemiology of pediatric obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):242-252.
- Koubayashi S, Nishida A, Nakagawa M, Shoda, Wada K, Susami R. Dentofacial morphology of obstructive sleep apnea syndrome patients. Nihon Kyosei Shika Gakkai Zasshi. 1989;48(4):391-403.
- Lowe AA, Ozbek MM, Miyamoto K, Pae EK, Fleetham JA. Cephalometric and demographic characteristics of obstructive sleep apnea: An evaluation with partial least squares analysis. Angle Orthod. 1997;67(2):143-153. doi: 10.1043/0003-3219(1997)0672.3.CO;2 [doi].
- Endo S, Mataki S, Kurosaki N. Cephalometric evaluation of craniofacial and upper airway structures in japanese patients with obstructive sleep apnea. J Med Dent Sci. 2003;50(1):109-120. doi: 10.11480/jmds.500115.
- Cistulli PA, Palmisano RG, Poole MD. Treatment of obstructive sleep apnea syndrome by rapid maxillary expansion. Sleep. 1998;21(8):831-835. doi: 10.1093/sleep/21.8.831 [doi].
- Moyers, RE. Standards of human occlusal development. 1976.
- Seto BH, Gotsopoulos H, Sims MR, Cistulli PA. Maxillary morphology in obstructive sleep apnoea syndrome. Eur J Orthod. 2001;23(6):703-714. doi: 10.1093/ejo/23.6.703 [doi].
- Forster CM, Sunga E, Chung CH. Relationship between dental arch width and vertical facial morphology in untreated adults. Eur J Orthod. 2008;30(3):288-294. doi: 10.1093/ejo/cjm113 [doi].
- Maeda K, Tsuiki S, Fukuda T, Takise Y, Inoue Y. Is maxillary dental arch constriction common in japanese male adult patients with obstructive sleep apnoea? Eur J Orthod. 2014;36(4):403-408. doi: 10.1093/ejo/cjt058 [doi].
- Hershey HG, Stewart BL, Warren DW. Changes in nasal airway resistance associated with rapid maxillary expansion. Am J Orthod. 1976;69(3):274-284. doi: 10.1016/0002-9416(76)90076-2 [doi].
- Galeotti A, Festa P, Viarani V, et al. Prevalence of malocclusion in children with obstructive sleep apnoea. Orthod Craniofac Res. 2018;21(4):242-247. doi: 10.1111/ocr.12242 [doi].
- Johal A, Conaghan C. Maxillary morphology in obstructive sleep apnea: A cephalometric and model study. Angle Orthod. 2004;74(5):648-656. doi: 10.1043/0003-3219(2004)0742.0.CO;2 [doi].
- ElMallah M, Bailey E, Trivedi M, Kremer T, Rhein LM. Pediatric obstructive sleep apnea in high-risk populations: Clinical implications. Pediatr Ann. 2017;46(9):e336-e339. doi: 10.3928/19382359-20170815-01 [doi].
- Robison JG, Otteson TD. Increased prevalence of obstructive sleep apnea in patients with cleft palate. Arch Otolaryngol Head Neck Surg. 2011;137(3):269-274.
- Suri S, Tompson BD, Cornfoot L. Cranial base, maxillary and mandibular morphology in Down syndrome. Angle Orthod. 2010;80(5):861-869.
- Guimaraes CV, Donnelly LF, Shott SR, Amin RS, Kalra M. Relative rather than absolute macroglossia in patients with Down syndrome: implications for treatment of obstructive sleep apnea. Pediatr Radiol. 2008;38(10):1062-1067.
- Cronk C, Crocker AC, Pueschel SM, et al. Growth charts for children with Down syndrome: 1 month to 18 years of age. Pediatrics. 1988;81(1):102-110.
- Cielo CM, Silvestre J, Paliga JT, et al. Utility of screening for obstructive sleep apnea syndrome in children with craniofacial disorders. Plast Reconstr Surg. 2014;134(3):434e-441e.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted October 3, 2023
Accepted for publication January 5, 2024
Address correspondence to: Tanya Al-Talib, DDS, MSO, D. ABDSM. Associate Professor in Residence- Orthodontics; Email: tanya.al-talib@unlv.edu.