Review Article 1, Issue 10.2
Mandibular Advancement Device Effects on the Upper Airway Anatomy and Function: An Umbrella Review
http://dx.doi.org/10.15331/jdsm.7290Silvia Gianoni-Capenakas, DDS, MSC 1; Da In Kim, DDS 2; Pedro Mayoral, DDS, MSc, PhD 3; Manuel Lagravère Vich, DDS, MSc, PhD 4
1Oral Medicine Specialist, MSc, PhD candidate and Orthodontics resident - School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, Canada ; 2Orthodontics Resident, Faculty of Dentistry, University of British Columbia, Canada; 3Director of Master Program on Dental Sleep Medicine, Catholic University of Murcia UCAM, Madrid, Spain; 4Associate Professor, Orthodontic Graduate Program, School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, Canada
ABSTRACT
Study Objectives:
To summarize systematic reviews regarding function and anatomy of the upper airway and subjective evaluations on breathing capability depending on the advancement and/or opening of the mandible.
Methods:
Four databases were searched based on inclusion criteria. Two independent reviewers evaluated abstracts of all articles for phase 1 and full text in phase 2 of selection. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement was used as a guideline; weaknesses were assessed using the AMSTAR2 tool.
Results:
Twelve systematic reviews were included. Mandibular protrusion greater than 50% of maximum protrusion results in a decrease of apnea-hypopnea index (AHI) by an average of 62.3% and an increase in oxygen saturation (SaO2). These findings correlate with dimensional changes in the upper airway, tongue, soft palate, and hyoid positions. Changes in the nasopharynx are minimal; however, significant volumetric increase of the oropharynx after mandibular advancement device (MAD) use in growing patients was observed. Improved Epworth Sleepiness Scale scores were reported for all included studies in one review. All MAD designs reviewed in the study show the potential to reduce AHI and respiratory disturbance index, with slightly lower AHI levels with those devices favoring more anterior than vertical mandibular movement.
Conclusions:
Devices that favor progressive mandibular advancement with less vertical opening have the potential to decrease AHI and increase SaO2. Findings of this review can help clinicians determine titration amounts of mandibular advancement for specific patients and can help gauge the level of MAD efficacy on patients with sleep apnea.
Statement of Significance:
Approximately 80 million Americans have sleep disordered breathing (SDB); 1 of 5 have mild to moderate obstructive sleep apnea (OSA), and 1 of 15 have moderate to severe OSA. Part of the population in whom SDB/OSA has been diagnosed for any reason cannot use continuous positive airway pressure (CPAP). The alternate treatment is the mandibular advancement device (MAD). The MAD’s function is to protrude and help stabilize the mandible to maintain a patent upper airway during sleep. MAD accounts for approximately 5% of the total OSA therapy in the United States, and some patients have indications to use MAD rather than CPAP. Therefore, it is of utmost importance to summarize the literature about MAD use and its effects on the respiratory capability of patients in whom SDB is diagnosed.
Keywords:
mandibular advancement, upper airway, mandibular opening, MAD, sleep apnea, AHI, oxygen saturation
Citation:
Gianoni-Capenakas S, Kim DI, Mayoral P, Lagravère Vich. Mandibular advancement device effects on the upper airway anatomy and function: An umbrella review. J Dent Sleep Med. 2023;10(2)
INTRODUCTION
Obstructive sleep apnea (OSA) is a breathing disorder that results in repetitive breathing cessation during sleep.1,2 OSA has a high prevalence, affecting 9% to 38% of the adult population.3 The cause of OSA is a combination of multiple anatomic and nonanatomic factors.4,5 One of the common causes of OSA is related to upper airway collapse.6 Although the gold standard of treatment is continuous positive airway pressure (CPAP), low compliance rates between 30% to 60% 7 increase the need for alternative treatment methods.
Mandibular advancement devices (MADs) prevent upper airway collapse by moving the jaw forward and downward.8,9 This anterior titration has been reported to increase the anteroposterior diameter and the cross-sectional area of the upper airway.10,11 Several studies have shown that compared to non advancement appliances, oral appliances that include mandibular advancement, and subsequent mandibular opening due to the condylar hinge angle, have significant benefits in preventing upper airway collapse.9–13
Several published systematic reviews have assessed the effect of mandibular advancement on the upper airway, and it is important to map and summarize their conclusions. The objective of an umbrella review is to highlight the strengths and weaknesses of previously published systematic reviews. This umbrella review aimed to summarize the findings of the effect of MADs on airway function, upper airway dimensions, and subjective self-reported evaluations on breathing capability. Findings of this study can provide guidance when evaluating candidate profiles for patients in need of MAD treatment.
METHODS
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis, or PRISMA, was used as a guideline for the methodologic approach of this study.14
Eligibility Criteria
Systematic reviews about the effects of MADs on the upper airway anatomy and function were included in this umbrella review. The inclusion criteria consisted of any age-range group in which the upper airway anatomy and/or ventilation was evaluated after MAD therapy. Randomized clinical trials (RCTs) and nonrandomized clinical trials were included in this review. Selected keywords included: upper airway, pharynx, oropharynx, nasopharynx, respiratory tract, mandibular advancement, mandibular advancement devices, orthodontics. Observational studies and animal studies were excluded. No limitations to publication year or language were imposed.
Information Sources
The following databases were searched to identify systematic reviews related to the inclusion criteria: EMBASE, PubMed, Web of Science, and Scopus. Additionally, a hand search was conducted. The search was performed in May 2020, and an update was performed in January 2021. The search results were exported to Rayyan Software (Qatar Computing Research Institute, Doha, Qatar),15 in which the duplicates were excluded (Figure 1).
Search
The excluded articles in phase 2 of selection are displayed in Appendix 1.
Selection of Sources of Evidence, Data Charting Process, and Data Items
Two reviewers (SGC and DK) evaluated titles and abstracts independently, using a web-based citation management program (Rayyan, Qatar Computing Research Institute, Doha, Qatar). The articles were screened in full text in the second phase by the same two reviewers, and, in cases of disagreement, a third reviewer was consulted (ML). The data were extracted by the second examiner (DK) and checked by the first author (SGC), and each article was recorded. The key features were listed, such as authors, country, year, respiratory disturbance index (RDI), apnea/hypopnea index (AHI), oxygen saturation (SaO2), snoring index, Epworth Sleepiness Scale (ESS), upper airway dimension, mandibular advancement, main results, and AMSTAR results (Table 1).
Critical Appraisal of Individual Sources of Evidence
Critical and noncritical weaknesses were assessed using the AMSTAR 2 tool.16 This tool focuses on the methodologic quality of each systematic review.16 The systematic reviews are ranked as high quality, moderate quality, low quality, or critically low.16
Summary Measures and Synthesis of Results
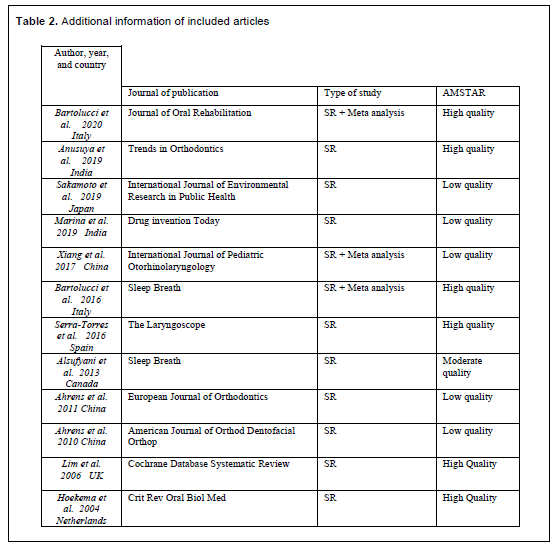
The studies were evaluated regarding changes in the upper airway, either dimensional or functional, such as respiratory function (AHI and RDI) and SaO2, as described in Table 1. Information on AMSTAR’s quality of evidence and journal of publication is displayed in Table 2.
RESULTS
Selection and Characteristics of Sources of Evidence
A total of 7,693 articles were found through a comprehensive database search. After managing duplicates, 4,359 studies were assessed based on the titles and abstracts. Thereafter, 4,340 were excluded. The remaining 19 reviews were screened by assessing their full text. The references of the included studies were also screened for possible new inclusions. Ultimately, 12 systematic reviews were included in this umbrella review.
Critical Appraisal Within Sources of Evidence
The AMSTAR 2 tool results shown in Table 1 are divided into 16 questions, and the results are displayed into 4 possible categories: high, moderate, low, and critically low quality of evidence. Six systematic reviews were ranked with high quality of evidence,17–22 one received a moderate rating,23 and five received a low rating.24–28
Results of Individual Sources of Evidence
Airway Functional Changes
Bartolucci et al discussed the amount of mandibular advancement and its effect on respiratory function measured basically with AHI.17 After evaluating 13 studies, they concluded that the mandibular advancement amount is not proportionate to the change in AHI.17 The mean success rate among the assessed studies was 62.3% and was related to mandibular advancements from 25% to 89% of the maximum mandibular protrusion.17 Sakamoto et al. also evaluated the amount of mandibular protrusion for effectiveness in respiratory pattern; they included only three studies in which 50% protrusion was compared to 75% mandibular protrusion.25 They concluded that 50% advancement could be more effective in patients with mild OSA, whereas 75% advancement is more prone to effectively ameliorate OSA symptoms in patients with severe OSA.25
Bartolucci et al., Hoekema et al., and Marina et al. evaluated the success rate of improving AHI and SaO2 when mono-block and duo-block MADs were used.18,21,24 Bartolucci et al. showed a better improvement in both indices when the monoblock MAD was used.18 Marina et al. corroborate with their results, showing a decrease in AHI values and an increase in SaO2.24 However, results from Hoekema et al. showed that not all studies verified a statistical difference in the efficacy of monoblock compared with duoblock designs.21
One systematic review focused on the design of the oral appliances and their effects on reducing OSA symptoms.28 It was concluded that all different designs effectively reduce AHI and RDI; the significant correlation seems to be with the mandible advancement.28
Hoekema et al evaluated MAD efficacy and effects on comorbidity linked to OSA symptoms.21 All included studies except two evaluated MAD with 50% to 87% of the maximum mandibular protrusion; the other two studies mentioned a mandibular protrusion of 2.4 mm to 6 mm.21 They verified that MAD is effective in decreasing AHI and increasing SaO2.
Upper Airway Dimensional Changes
Four systematic reviews evaluated the effect of functional appliance therapy on airway dimensions in growing patients.19,20,22,23 Their conclusions showed that functional appliance therapy allows the forward repositioning of the mandible, leading to an increase in airway dimensions.19,20,23 There is a change in the tongue, soft palate, and hyoid positions.19,20 These effects also seem to be related to a reduction in AHI and increase in SaO2.19 Anusuya et al20 reported the findings of some of the included studies, showing that the change in the nasopharynx was minimal. However, the difference in the oropharynx was significant after the use of mandibular advancement treatment in growing patients.20
Alsufyani et al evaluated the usability of cone-beam CT in evaluating dimensional changes of the upper airway after mandibular advancement.22 They reported results based on surgical advancement of the mandible and mandibular advancement using appliance therapy. Due to the aim of this study, only the data available related to the use of appliance therapy were included and that were not based on just a one-case description. Therefore, only the data from two studies were included in this umbrella review. Their protrusion amounts were 75% of the maximum mandibular protrusion and 4 mm (±3.6 mm). The authors reported a low quality of evidence, showing a volumetric increase after using the Twin-block and Herbst appliances.22
Subjectively Perceived Symptoms
One systematic review reported subjective evaluations only.26 Fourteen studies were included in which the perceived treatment efficacy was analyzed.26 ESS was used in most of the included studies in the systematic review by Ahrens et al; 12 studies showed improved ESS scores using MAD.26 Other subjective tools were also used, such as the fatigue severity scale, sleep disorder questionnaire, visual analog scale, and health-related quality of life questionnaires.26 Most of the patients reported MAD to be more efficient for treating OSA symptoms.26
Synthesis of Results
Twelve systematic reviews were included in this study; all of them were written in English and published between 2004 and 2020. One study each was from the United Kingdom, Canada,22 Spain,19 Netherlands,21 and Japan;25 two from Italy;17,18 two from India;20,24 and three from China.23,26,27 Six systematic reviews only included RCTs.17,18,20,21,25, 28
Figure 1Flowchart of literature search and study selection. |
Table 1Summary of characteristics of included articles |
Table 2Additional information of included articles |
{kind=link}
|
DISCUSSION
The objective of this umbrella review was to summarize the findings of the effect of MADs on airway function, upper airway dimensions, and subjective self-reported evaluations on breathing capability. The findings of this umbrella review can provide guidance and awareness on how much of an effect MAD treatment can have on patients with sleep apnea.
Airway Functional Changes
Bartolucci et al., reporting results of 13 studies and Sakamoto et al, based on three RCTs, agree that advances of approximately 50% would benefit patients with mild to moderate OSA, both in terms of AHI improvement.17,25 Few studies have evaluated whether less than 50% of mandibular advancement based on the maximum protrusion is correlated with improved rates of AHI.17 Mandibular advancement of 75% of the maximum mandibular protrusion could benefit patients with severe OSA. However, it is possible to conclude that the improvement of AHI is not proportionate to the amount of mandibular advancement. Therefore, the amount of mandibular advancement could not be the only factor to affect AHI and improve OSA. The progressive mandible protrusion seems to be more suitable to titrate treatment according to each patient.
After reviewing 50 RCTs, Bartolucci et al. discussed improving the AHI and SaO2 indices by comparing monoblock to duoblock MADs.18 They reported that most of the studies included in their systematic review described better results in improving the AHI and SaO2 when the mono-block device was used.18 Their explanation for the better results with the monoblock device is related to the lower vertical increase, which generates a smaller rotation of the mandible and consequently greater mandibular advancement. This idea is in agreement with findings by Mayoral et al.13 However, the lack of control in vertical opening with the duoblock device could be mitigated with the use of elastics. Conversely, Hoekema et al.21 reported one study that showed no difference in AHI and SaO2 between mono-block and duoblock devices.
Hoekema et al.21 evaluated MAD efficacy, and their results also showed an improvement in SaO2 compared to the placebo. Yet, no difference was found in AHI and ESS when different vertical heights were tested, although the tendency was that patients prefer the ones with lower vertical dimension.21 Their findings are contrary to the idea that the greater the vertical opening, the greater the decrease in the dimension of the oropharynx, due to the posterior rotation of the mandible, which could compromise the AHI.
Marina et al.24 compared the custom-made and prefabricated MADs. Throughout six included studies, four of them concluded that both types improve AHI and oxygen saturation, also agreeing with Ahrens et al.27 One other study did not show a difference in AHI with both types of appliances, whereas one showed that both types improved AHI. However, the custom-made appliance had a better result than the prefabricated one. In agreement with Marina et al.,24 Serra-Torres et al.,19 and Ahrens et al.27 also reported better outcomes with the custom-made appliances. The individualized selection of an oral appliance accounting for the MAD characteristics such as fabrication material, tooth anatomy and angulation, number of teeth present, device extension, and propulsion system is crucial. Possible allergies to some materials, retention, and strength and thickness are important factors for the patient’s comfort and health. Materials, retention, device extension, and propulsion systems are interconnected and should be taken into account when choosing a MAD. For instance, the propulsion system affects the force vectors, and therefore also the retention. Moreover, the propulsion system will affect the comfort of the patient according to their sleep position.
Upper Airway Dimensional Changes
Anusuya et al.20 reported no increase in the nasopharynx region after the use of functional appliance for the mandibular advancement in growing patients. However, they found an increase in the oropharynx region. Likewise, Xiang et al.23 reported an increase in the oropharynx region after using a functional mandibular advancement appliance in growing patients in whom dimensional changes were measured without the appliance in place before and after therapy. Conversely, Serra-Torres et al.19 reported an increase in the velopharynx area in adult patients. Mandibular advancement increases antero and lateral dimensions of the velopharynx and oropharynx by displacing the suprahyoid and genioglossus muscles anteriorly; increasing tension on the palatoglossal and palatopharyngeal muscles of the soft palate; and lateral movement of the pharyngeal arches, which would influence airway space. Xiang et al.’s review assessed growing patients without sleep disordered breathing.
Subjectively Perceived Symptoms
Hoekema et al. reported some studies showing an improvement in the ESS score compared to a placebo device,21 but others showed no difference. However, one systematic review mentioned a subjective improvement in breathing even with the inactive appliance (no mandibular protrusion) in place.26 This could be due to the placebo effect or a slight vertical opening increase due to splint thickness. However, Hoekema et al. mentioned that the control devices are created to minimally increase the vertical mandibular opening.21 Regarding monoblock or duoblock, Hoekema et al.21 reported no differences in the ESS according to one study.
Conclusion of Studies Graded as High Quality Through AMSTAR
Six studies were graded high quality according to AMSTAR; five of them were based on adult patients and one on children.17-21,28 Three of them were based only on RCTs. 17,18,28 Their main conclusions are: (1) According to 50 articles, the monoblock device showed higher effectiveness than the duoblock; however, the authors reported this conclusion as having very low quality of evidence.18 (2) According to 8 articles, functional appliances enlarge the oropharynx in children.20 (3) AHI improvement is not proportionate to the amount of mandibular advancement, based on 13 articles.17 (4) AHI, oxygen saturation, snoring, and daytime sleepiness improve with MAD therapy. There is an increase in the upper airway area; these results were based on 22 articles.19 (5) Based on 17 studies, another systematic review described improvement in AHI and daytime sleep with MAD therapy.28
Additional Information
Hoekema et al. suggested that MAD treatment did not significantly change the maximum mouth opening, lateral movement, or protrusion.21 However, one study in their systematic review showed an increased mouth opening in 28% of patients.21 Among the systematic reviews included in this study, a significant variability was seen in the results of individual studies.27 Differences in study design, sample size, type of MAD, amount of advancement or opening, patient compliance, and long-term effect studies lead to the conclusion that no one appliance fits all patients and symptoms.29
The material of the devices (thermoplastic, acrylic, acrylic-metal, printed nylon), the retention mode, and the design of the devices (attached bilateral compression, attached bilateral traction, attached midline traction, attached bilateral interlocking, unattached bilateral interlocking) were not described. However, all of them could contribute to the efficiency (efficacy + adherence) of the MAD.
Future Directions
Because compliance is a crucial characteristic of this therapy, more studies in this area are necessary. The effectiveness of MADs in edentulous patients is still unclear. Moreover, studies evaluating MADs long-term effects and adverse effects are needed.
In addition, imaging studies with evaluation of ventilation rather than AHI might be of great interest. Lately, authors have reported the importance of not only evaluation of OSA through one index – AHI – instead, the variability of severity of OSA is also linked to oxygen saturation, for example.30 Therefore, future studies need to take into consideration a list of parameters such as oximetry, sleep stage shifts, arousal, sleep efficiency, and snoring.
CONCLUSION
- A titratable custom-made MAD seems to be the best appliance for decreasing AHI and increasing SaO2. Moreover, the lowest vertical increase possible and control of mouth opening seems to improve the patient’s subjective Multiple factors influence the efficacy of the MAD, including the severity of OSA, degree of protrusion, appliance design, and fabrication materials. Therefore, the best MAD is the one that matches all of these requirements for each particular patient.
- The compilation of the information from 12 systematic reviews suggests that:
- A decrease in AHI and an increase in SaO2 is related to mandibular protrusion of at least 50% of the maximum mandible protrusion rate. The progressive mandible protrusion seems to be more suitable to titrate treatment according to each patient.
- All device designs have the potential to reduce AHI and RDI.
- An improvement in the subjective respiratory efficiency using ESS was seen.
- There is strong evidence suggesting that the oropharynx space is increased, and there is a change in the position of the tongue, hyoid bone, and soft palate.
- Functional appliance therapy results showed significant improvement in oropharyngeal dimensions in class II malocclusion patients with retrognathic mandibles.
AppendixExcluded articles for Umbrella Review |
REFERENCES
- Park J, Ramar K, Olson E. Updates on definition, consequences, and management of obstructive sleep apnea. Mayo Clin Proc. 2011;86(6):549-554.
- Spicuzza L, Caruso D, Di Maria G. Obstructive sleep apnoea syndrome and its management. Ther Adv Chronic Dis. 2015;6(5):273-285.
- Senaratna CV, Perret JL, Lodge CJ, et al. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med Rev. 2017 Aug;34:70-81.
- Eckert DJ, Malhotra A, Jordan AS. Mechanisms of Apnea. Prog Cardiovasc Dis. 2009;51:313-323.
- Eckert DJ. Phenotypic approaches to obstructive sleep apnoea – New pathways for targeted therapy. Sleep Med Rev. 2018;37:45-59.
- Owens RL, Eckert D, Yeh S, Malhotra A. Upper airway function in the pathogenesis of obstructive sleep apnea: A review of the current literature. Curr Opin Pulm Med. 2008;14(6):519-524.
- Rotenberg B, Murariu D, Pang K. Trends in Cpap adherence over twenty years of data collection: A flattened curve. J Otolaryngol Head Neck Surg. 2016;45(1).
- Basyuni S, Barabas M, Quinnell T. An update on mandibular advancement devices for the treatment of obstructive sleep apnoea hypopnoea syndrome. J Thorac Dis. 2018;10 (Suppl 1):S48-S56.
- Kim D, Lagravère Vich M, Mayoral P, Miguez M. Three-dimensional changes in skeletal/ dental landmarks with use of mandibular advancement device. J Dent Sleep Med. 2020;7(2).
- Ryan CF, Love LL, Peat D, Fleetham JA, Lowe AA. Mandibular advancement oral appliance therapy for obstructive sleep apnoea: Effect on awake calibre of the velopharynx. Thorax. 1999;54(11):972-977.
- Petri N, Svanholt P, Solow B, Wildschiodtz G, Winkel P. Mandibular advancement appliance for obstructive sleep apnoea: Results of a randomised placebo controlled trial using parallel group design. J Sleep Res. 2008;17(2):221-229.
- Tsuiki S, Hiyama S, Ono T, et al. Effects of a titratable oral appliance on supine airway size in awake non-apneic individuals. Sleep. 2001;24(5):554-560.
- Mayoral P, Lagravère MO, Míguez-Contreras M, Garcia M. Antero-posterior mandibular position at different vertical levels for mandibular advancing device design. BMC Oral Health. 2019;19(1):85.
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic review and meta-analysis protocols: The PRISMA Statement. PLoS Med. 2009;6(6): e1000097.
- Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210.
- Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008.
- Bartolucci ML, Bortolotti F, Raffaelli E, D’Antò V, Michelotti A, Alessandri Bonetti G. The effectiveness of different mandibular advancement amounts in OSA patients: a systematic review and meta-regression analysis. Sleep Breath. 2016;20(3):911-919.
- Bartolucci ML, Bortolotti F, Corazza G, Incerti Parenti S, Paganelli C, Alessandri Bonetti G. Effectiveness of different mandibular advancement device designs in obstructive sleep apnoea therapy: A systematic review of randomised controlled trials with meta-analysis. J Oral Rehabil. 2021;48(4):469-486.
- Serra-Torres S, Bellot-Arcís C, Montiel-Company JM, Marco-Algarra J, Almerich-Silla JM. Effectiveness of mandibular advancement appliances in treating obstructive sleep apnea syndrome: A systematic review. Laryngoscope. 2016;126(2):507-514.
- Anusuya V, Ashok Kumar J, Sharan J. Effects of functional appliance treatment on pharyngeal airway passage dimensions in Class II malocclusion subjects with retrognathic mandibles: A systematic review. APOS Trends Orthod. 2019;9(3):138-148.
- Hoekema A, Stegenga B, de Bont LG. Efficacy and co-morbidity of oral appliances in the treatment of obstructive sleep apnea-hypopnea: A systematic review. Crit Rev Oral Biol Med. 2004;15(3):137-155.
- Ahrens A, McGrath C, Hägg U. A systematic review of the efficacy of oral appliance design in the management of obstructive sleep apnoea. Eur J Orthod. 2011;33(3):318-324.
- Alsufyani NA, Al-Saleh MAQ, Major PW. CBCT assessment of upper airway changes and treatment outcomes of obstructive sleep apnoea: A systematic review. Sleep Breath. 2013;17(3):911-923. doi:10.1007/s11325-012-0799-7
- Xiang ML, Hu B, Liu Y, Sun J, Song J. Changes in airway dimensions following functional appliances in growing patients with skeletal class II malocclusion: A systematic review and meta-analysis. Int J Pediatr Otorhinolaryngol. 2017;97:170-180.
- Marina M, Ariga P, Ganapathy DM, Vadaguru Mallikarjuna A. Efficacy of two mandibular advancement appliances in the treatment of obstructive sleep apnea-hypopnea syndrome: A systematic review. Drug Invent Today. 2019;11(3):698-702.
- Sakamoto Y, Furuhashi A, Komori E, et al. The most effective amount of forward movement for oral appliances for obstructive sleep apnea: A systematic review. Int J Environ Res Public Health. 2019;16(18):3248.
- Ahrens A, McGrath C, Hägg U. Subjective efficacy of oral appliance design features in the management of obstructive sleep apnea: A systematic review. Am J Orthod Dentofacial Orthop. 2010;138(5):559-576.
- Lim J, Lasserson TJ, Fleetham J, Wright J. Oral appliances for obstructive sleep apnoea. Cochrane Database Syst Rev. 2006(1):CD00435.
- Pliska BT, Nam H, Chen H, Lowe AA, Almeida FR. Obstructive sleep apnea and mandibular advancement splints: occlusal effects and progression of changes associated with a decade of treatment. J Clin Sleep Med. 2014;10(12):1285-1291.
- Kapur VK, Donovan LM. Why a single index to measure sleep apnea is not enough. J Clin Sleep Med. 2019;15(5):683-684. Published 2019 May 15.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted April 11, 2022
Submitted in final revised form July 3, 2022
Accepted for publication September 8, 2021
Address correspondence to: Silvia Gianoni-Capenakas, DDS, MSC; Address: School of Dentistry, Faculty of Medicine and Dentistry, 5-488 Edmonton Clinic Health Academy, 11405-87 Avenue NW, University of Alberta, Edmonton, AB, Canada T6G 1C9; Email: capenaka@ualberta.ca