Reprinted Article 2, Issue 5.4
REPRINTED: Differences in Volume and Area of the Upper Airways in Children with OSA Compared to a Healthy Group
http://dx.doi.org/10.15331/jdsm.5992
Rosa Carrieri Rossi, DDS, PhD1 ; Nelson José Rossi, DDS, PhD2 ; Edson Illipront Filho, DDS, PhD3 ; Nelson José Carrieri Rossi, DDs, MS4 ; Israel Chilvarquer, DDS, PhD5 ; Reginaldo Raimundo Fujita6 ; Shirley Shizue Nagata Pignatari, MD, PhD6
1 Division of Pediatric Otolaryngology, Department of Otolaryngology and Head and Neck Surgery, Federal University of Sao Paulo-UNIFESP Brasil; 2Postgraduate of Orthodontics ,Educational Association of Brazil-FUNORTE/SOEBRAS; 3Division of Radiology, Sao Paulo State University-USP; 4Postgraduate of Orthodontics, Educational Association of Brazil-FUNORTE/SOEBRAS; 5Division of Radiology, Sao Paulo State University-USP; 6Division of Pediatric Otolaryngology, Department of Otolaryngology and Head and Neck Surgery, Federal University of Sao Paulo-UNIFESP Brasil
ABSTRACT
Study Objectives:
The cause of obstructive sleep apnea in children is not fully known. The many risks and predisposing associated factors challenge its diagnosis and treatment. The objective of this research was to verify the differences in the volume and areas of the upper airways between children submitted to adenotonsillectomy for the treatment of OSA, but with persistent/recurrent postoperative OSA complaints, and a sex-age matched healthy control group, assisted by cone beam computed tomographic images.
Methods:
The study included a group of 20 children of both sexes, with mean age of 9.5 years, diagnosed with OSA and primary snoring (PS) by polysomnographic exam (AHI ≥ 3), angle class II, and retruded mandible, and a control group of 20 healthy children of both sexes, mean age of 7.4 years, with the same characteristics, but without respiratory complaints. Both groups were submitted to otolaryngological and orthodontic clinical examinations, and to cone beam computed tomography exam (CBCT). Areas and volumes of the nasopharynx and oropharynx and lower axial area were measured. Mean, standard deviation, confidence interval, and Student t-test with a 5% significance between these groups were analyzed.
Results:
The results showed a significant difference (p < 0.05) in the volume and area of the nasopharynx of patients with OSAS compared to the same parameters in healthy patients. Children with OSA (SG) showed a significant narrowing in the nasopharynx and in the lower area of the upper airway (UA) compared to the control group (CG).
Conclusions:
Children with persistent OSA symptoms after adenotonsillectomy present with narrowing of the nasopharynx, and CBCT is a useful complementary test for orthodontic diagnostic and treatment planning of these patients.
Keywords:
apnea and hypopnea syndrome, habitual snoring, nasopharynx and oropharynx size, CBCT
Citation:
Rossi RC, Rossi NJ, Filho EI, Rossi NJ, Chilvarquer I, Fujita RR, Pignatari SS. Differences in volume and area of the upper airways in children with OSA compared to a healthy group. Journal of Dental Sleep Medicine 2016;3(3):81–87.
INTRODUCTION
Obstructive sleep apnea (OSA) is a respiratory sleep disorder (RSD) characterized by partial or complete upper airway (UA) obstruction that can affect children in their very early phase of development.1–6 Children between 2 and 6 years old are the most affected group for the occurrence of upper airway lymphoid tissue hypertrophy, usually presenting with the most severe aspects of OSA. Diagnostic delays of this condition may generate a negative influence on their adult life quality.3–8 The polysomnographic (PSG) evaluation is considered the gold standard method for the diagnosis of OSA,1–6,14–16 and surgical removal of lymphoid tissue has been the standard treatment in these cases.9–13
Recurrence of OSA can occur after adenotonsillectomy, and (among other causes) is believed to happen due to concomitant craniofacial disorders. Any condition that causes obstruction of the upper airway (UA) or reduces the pharyngeal muscles tonus can provide risk for OSA development.3,5–7 Some of these conditions may be recognized and treated by the orthodontist.
Orthodontic planning and diagnosis include panoramic radiograph, lateral X-ray, and a X-ray series of the entire mouth, but these 2D tests fail to accurately assess the UA. Recent studies recommend 3D images as diagnostic tools to help identify obstructions in the UA, such as magnetic resonance imaging (MRI) and cone-beam computed tomography (CBCT).16,17
MRI is typically used for evaluating soft tissues, and there is a lack of standardized parameters for hard tissue evaluation.16 CBCT exposes the child to less ionizing radiation when compared to multiple detector-row spiral CT, but even so, radiation will still be higher than a 2D exam. The individual dose emitted by a single 2D test is low, but the collective dose of all exams that is usually recommended, is equal to or slightly higher than the dose emitted by a single 3D examination.18–24,26 Furthermore, the 3D image is more reliable than 2D to assess all the head and neck structures as well as the upper airways, and it can be useful to and serve a large multi-professional group.27–31
The objective of this research was to verify the differences in the volume and areas of the UA among children with OSA who have had adenotonsillectomy but continue to have persistent OSA, and a control group of healthy children, in order to plan the best orthodontic treatment.
METHODS
This observational case-control study was approved by the Ethics Committee of the Federal University Sao Paulo – UNIFESP under the number: 1739/11 02/12/2011, by the Ethics Committee of FOUSP-Dentistry College State University of Sao Paulo under the number 170/2010. Financed by the Research Foundation-FAPESP under the Protocol 2012/15715-2 November 2, 2012.
To accomplish this case-control study, a multidisciplinary team was enrolled. ENT examination was performed by an experienced otolaryngologist. Children suspected to have PS and OSA underwent a polysomnographic test to confirm the diagnosis, and the report was certified by a professional expert in sleep medicine. Orthodontic evaluations were carried out by 3 orthodontists in 2 different clinics. All selected patients underwent orthodontic planning examination with CBCT, and these images were evaluated by 2 imaging studies experts.
A total of 397 patients, ages ranging between 7–14 years, presenting with PS and OSA complaints were evaluated at the Oral breathing clinic at the Otorhinolaryngology Pediatric Division, Federal University of Sao Paulo (UNIFESP) from 2013 to 2014. All the patients had undergone adenotonsillectomy or had been excluded of having hypertrophic tonsils; but they all had OSA symptoms. After otorhinolaryngological and nasofibroscopic examinations, patients suspected of having OSA were referred for PSG. Patients with syndromes or obesity were excluded.
PSG was performed at the Sleep Apnea Institute-UNIFESP/ SP. Patients stayed overnight and were evaluated with an electroencephalogram (EEG), electrooculogram (EOG), electromyogram (EMG) mental and/or submental muscle, electrocardiogram (ECG), airflow (nasal and oral), respiratory effort (thoracic and abdominal), other body movements (tibial EMG), oxygen saturation, and carbon dioxide concentration (precision oximeter). The parameters evaluated in PSG are described in Table 1
Table 1PSG parameters. |
{kind=link}
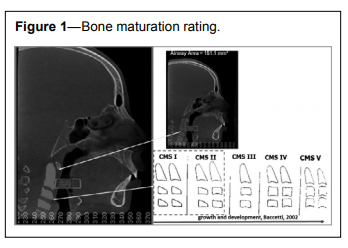
Twenty patients were selected for the study group (SG)—13 girls and 7 boys, with an average age of 9.5 years. The average apnea-hypopnea index of the patients included was 3.1, Angle Class II, short and retruded mandible and CMS I or II (Figure 1).14 Sexual dimorphism analysis in the PSG data was performed by Student t test, with 95% reliability.
Figure 1Bone maturation rating. |
{kind=link}
The control group (CG) consisted of 12 girls and 8 boys, mean age of 7.4 years old, CVMS I or II,14 without respiratory complaints, Class II malocclusion, and retruded mandible, who sought orthodontic treatment at the Dentistry College, State University of Sao Paulo-FOUSP, SP for other reasons. Children of both study and control groups were referred to orthodontic planning studies (cephalometric and study models) and CBCT examinations. The selected patients and legal guardians signed the consent form.
For the CBCT, the participants were placed in the tomography room in a sitting position with their head parallel to the Frankfurt plane (FP), and the CBCT sensor was positioned in order to cover the entire head. Patients were instructed to remain still, with relaxed lips, avoiding swallowing, and keeping a smooth breathing pattern during image acquisition.31
The equipment used for CBCT was the i-Cat (Cone beam 3-D Dental Imaging System, Imaging Sciences International, Hatfield, PA). After capturing the X-rays, the tomography sensors attenuated and digitalized the images through algorithm reconstruction, converting the data in medicine digital image for communication (DICOM).30 After an accurate reconstructed digital image was obtained, participants were released.
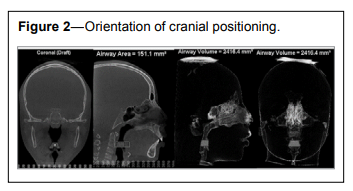
The reconstruction of the primary image was performed at the workstation. The Dolphin 3D software (Imaging Dolphin/ Patterson Dental, Chatsworth, CA, USA) was used for the proposed measurements. Before measuring the volume, area and lower area of the upper axial way, the pictures were standardized according to the orientation of the cranial positioning (Figure 2).26
Figure 2Orientation of cranial positioning. |
{kind=link}
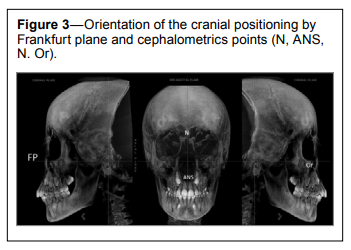
For the orientation of the cranial positioning, the axial plane coincides with the orbital points (Or); in the lateral, the coronal plane coincides with the porion (Po) on the left and right sides, and an axial plane is superimposed on the FP; the median sagittal plane joins the nasion (N) and the anterior nasal spine (ANS) (Figure 3).27,31
Figure 3Orientation of the cranial positioning by Frankfurt plane and cephalometrics points (N, ANS, N. Or). |
{kind=link}
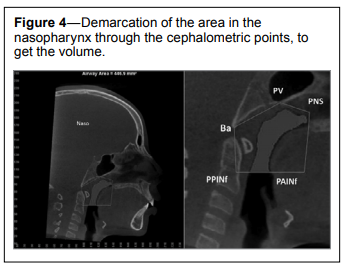
For evaluating the nasopharynx (NP) area and volume, the points were placed at the posterior nasal spine (PNS), posterior vomer (PV), point of horizontal and vertical extent of PV, point of PNS extension, basion (Ba), PPINf (located 15 mm after the lower limit of the uvula), and PAINf (marked 15 mm above the lower limit to the uvula) (Figure 4).31
Figure 4Demarcation of the area in the nasopharynx through the cephalometric points, to get the volume. |
{kind=link}
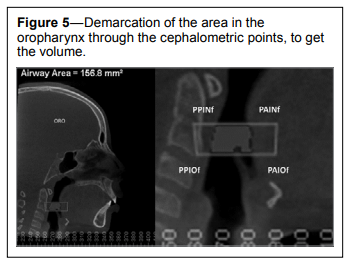
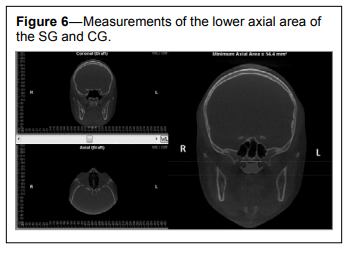
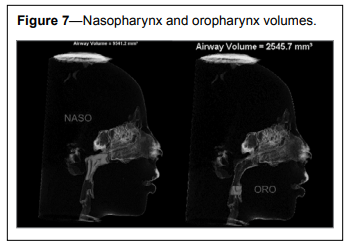
For the evaluation of the oropharynx (OP), the upper limit of the epiglottis was seen in the coronal plane, cut at its greatest length, and its highest portion was landmarked. In the image in sagittal view, this area was limited by the union of PPINf’ and PAINf’, and the points were created in PAIOf’ and PPIOf located 15 mm front and rear, respectively, of the uvula point. Sensitivity was determined using the same criteria that was used for the NP (Figures 5, 6).31 In Figure 7, regions of oropharynx are highlighted by software tools.
Figure 5Demarcation of the area in the oropharynx through the cephalometric points, to get the volume. |
{kind=link}
Figure 6Measurements of the lower axial area of the SG and CG. |
{kind=link}
Figure 7Nasopharynx and oropharynx volumes. |
{kind=link}
Data from all measurements, the areas of the nasopharynx and oropharynx, the volumes of the oropharynx and nasopharynx, and lower axial area of the SG and CG, were measured with CBCT tools, and registered in a 2007 Excel table. The means, standard deviations, confidence intervals, and Student t-test with a 95% confidence level were calculated for all the obtained values.
RESULTS
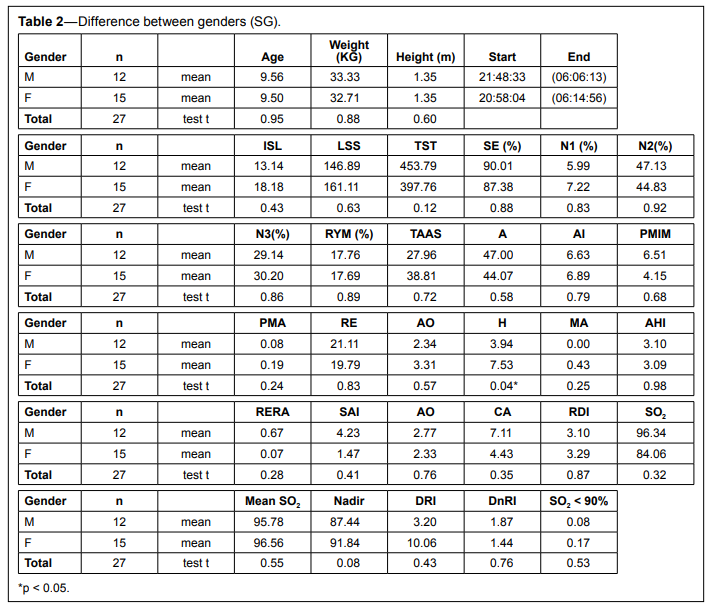
No significant differences of the major values obtained in the PSG examination were observed between genders. A significant difference (p = 0.04) was only found for the hypopnea parameter (H): girls had a higher number of events than boys. The remaining parameters did not show significant differences between genders (Table 2).
Table 2Difference between genders (SG). |
{kind=link}
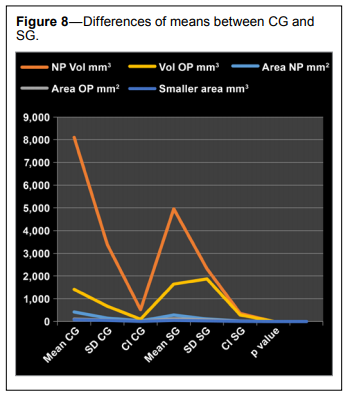
Regarding the CBCT measurements, the NP volume (4,949.85 mm3 ) and NP area (284.79 mm2 ) were significantly lower in the SG than in the CG (p = 0.001 and p = 0.002) (8,100.93 mm3 and 417.87 mm2 ), respectively. The OP volume and area of the SG (1,645.43 mm3 and 112.88 mm2 ) and CG (1,410.81 mm3 and 100.18 mm2 ) did not show significant differences. Clinical measures of OP were slightly higher in the SG (Table 2).
The CTCB cross-sectional areas of the nasopharynx, oropharynx, and hypopharynx in apneic patients were significantly reduced (p < 0.05) compared with those in the CG. The lower axial area of the NP was significantly lower (p = 0.01) in SG (74.48 mm2 ) than CG (44.03 mm2 ). The mean, standard deviation, confidence interval, and Student t-test with a 95% significance between these groups can be seem in Table 3.
Table 3Mean, standard deviation, confidence interval, and student test-t between control group and study group. |
{kind=link}
There was a significant difference between the volume and area of the NP of patients with OSA in comparison to the same parameters of healthy patients, but for OP no significant differences were found. The results can be observed in Figure 8.
Figure 8Differences of means between CG and SG. |
{kind=link}
DISCUSSION
Sleep apnea is a relatively well understood disorder in adults, but in children it remains controversial, particularly due to the multifactorial nature of the disease in addition to the differences in response to each child growth phase. Our results may have implications to children from 7 to 14 years of age, who had already received some treatment for OSA such as tonsillectomy in early childhood but still present with OSA complaints, as demonstrated by other authors in previous studies.3–14 Our goal was to understand which sites the upper airways could be involved with the persistence of the disease, in order to develop an effective orthodontic treatment.
The results of our study showed that the upper airway was significantly smaller in SG when compared to healthy subjects mainly at the nasopharynx.13,14 Regarding the oropharynx, we observed that healthy patients (CG) had a smaller area and volume than the OSA patients; the differences however, were not statistically significant. The axial lower area of the OSA patients was significantly lower than the CG, as already observed by many others.18–25
Reports in the literature showed that severe OSA is associated with younger ages (pre-adolescence) due to the increased lymphoid tissues, causing a narrowed pharynx.1–6,16 In the present study, the OSA patients were slightly older (average age of 9.5 years old), having already undergone a surgical treatment when younger, and mostly had no tonsils at all; even so, they presented with reduced NP volume. This observation demonstrated that other factors, such as craniofacial abnormalities, could play a role in the installation of OSA, in agreement with other studies.7–12 The CG patients did not have respiratory complaints and had no hypertrophic tonsils, despite their young age.
In addition, chronological age may not represent the real growth phase that can be best evaluated by bone age measurements.14 In our study, both groups were at the same stage of pubertal maturation (CVM I and II), and in the same age group (5–12 years old).27 Maybe OSA studies in children assessing also the real phase of growth and children development, determined by bone ossification age, could minimize the chance of erroneous conclusions.
In this study, no differences in AHI were found between males and females of the study group, and the patients were not divided by gender (Table 1).
In general, male patients have shown to have an increased risk for OSA; the mechanisms underlying this predisposition are unclear.13 At least one previous study demonstrated a difference, and proposed that to be due to the usual more enlarged UA sizes in adult males than in females, this anatomical feature could let the male UA more likely to collapse.13
Recent studies of CBCT, have demonstrated that patients with retruded mandible and class II tend to have the OP volume reduced when compared to patients Class I and III malocclusion, with advanced or standard mandible. According to the authors, the mandibular position may have influence on the volume of the OP. Regarding the NP, significant differences have been shown only in patients presenting with Class I and Class II malocclusion; the volume is usually lower in Class II patients.17,22,25 We included Class II patients with retruded mandible in both CG and the SG groups, and our results showed a greater and significantly reduced area and volume of the NP in patients with OSA and PS. The nasopharynx is not a region of the airway particularly related to mandible retrusion, but it could be associated with class II malocclusion, oral breathing, or allergic diseases.8,19,27 The SG patients were all oral breathers, which may have caused the narrowing of NP, even after they had been submitted to a surgical ENT treatment. This agrees with some authors who have shown the influence of the breathing mode on the anatomy of the upper airways.8,19,27
The causes of the OSA disorder has not been totally established, particularly in the pediatric population, in which the growth and developmental events, and external factors, such as allergic diseases and habits, can influence the development of the sleep disorders, confusing the correct diagnosis. Due to such a complexity of OSA in children, the treatment should be planned in conjunction with various professionals simultaneously.3–14 The PSG diagnosis may not be enough for understanding the cause of disease, in order to achieve the best treatment. We should have tools to evaluate the anatomical obstructive site of the patient to plan for the possible treatment.1–7,15,16
The MRI17 and CBCT exams18–24 have shown to be of good assistance for the OSA understanding. Recent studies recommend considering the cone-beam computed tomographic (CBCT) to identify obstructions in the airways,18 due to the many advantages, including that as the 3D image is more reliable than 2D.18–22 CBCT exams3,15,16 are safely used for diagnosis in orthodontics because they can replace all routinely requested tests in the diagnosis and orthodontic planning, with the same or even lower ionizing radiation than tests routinely ordered.17,23,24
Our goal was to understand and build parameters that could help the diagnosis and treatment of the recurrent PS and OSAS. Our sample was just large enough for statistical analysis, but not enough for definitive conclusions. The multifactorial aspects of the disorder and aspects related to childhood growth are a great obstacle in standardizing population samples. The observation of the sites where there is a decrease of size in the upper airways gives us an opportunity to offer the most appropriate orthodontic treatment. Studies involving patients with all patterns of malocclusion such as class I and III angle malocclusion should also be conducted for a comparison with our results.
CONCLUSIONS
Children diagnosed with primary snoring and persistent obstructive sleep apnea after tonsillectomy showed a significant and important narrowing of the upper airway, especially at the nasopharynx region. The sagittal lower area of the upper airway also showed significant reduction. CBCT proved to be a complementary test for diagnostic and treatment planning purposes, and it is available to health professionals of many areas, avoiding the need for potentially harmful orthodontic exams.ABBREVIATIONS
AHI, apnea-hypopnea indexANS, anterior nasion spine
AT, adenotonsillectomy
Ba, basion
CBCT, cone bean tomography
CG, control group
DICOM, digital image for communication
FAPESP, Research Foundation of Sao Paolo State
FOUSP, Dentistry College, State University of Sao Paolo
FP, Frankfurt plane
i-Cat, cone beam 3-D dental imaging system
N, nasion
NP, nasopharynx
OP, oropharynx
OSA, obstructive sleep apnea
PAINF, pharynx anterior inferior (15 mm after the lower limit of the uvula)
PAIOF, pharynx anterior (15 mm front of the uvula point)
PNS, posterior nasion spine
PPINF, pharynx posterior inferior (15 mm after the lower limit of the uvula)
PPIOF, pharynx posterior (15 mm rear of the uvula point)
Po, porion
PS, primary snoring
PSG, polysomnography
PV, posterior vomer
RSD, respiratory sleep disorder
SG, study group
UA, upper airway
UARS, upper airway syndrome
UNIFESP, Federal University Sao Paulo
REFERENCES
2. Powell S, Kubba H, O’Brien C, Tremlett M. Paediatric obstructive sleep apnoea. BMJ 2010;340:c1918.
3. Bhattacharjee R, Kheirandish-Gozal L, Spruyt K, et al. Adenotonsillectomy outcomes in treatment of obstructive sleep apnea in children: a multicenter retrospective study. Am J Respir Crit Care Med 2010;182:676–83.
4. Valera FC, Demarco RC, Anselmo-Lima WT. Apnea syndrome and obstructive sleep hypopnea (OSAS) in children. Rev Bras Otorrinolaringol 2004;70:232–7.
5. Don MD, Geller KA, Koempel JA, Ward SD. Age specific differences in pediatric obstructive sleep apnea. Int J Pediatr Otorhinolaryngol 2009;73:1025–8.
6. Brietzke SE, Katz ES, Roberson DW. Can history and physical examination reliably diagnose pediatric obstructive sleep apnea / hypopnea syndrome. A systematic review of the literature. Otolaryngol Head Neck Surg 2004;131:827–32.
7. American Academy of Pediatrics (AAP). Subcommittee on Obstructive Sleep Apnea Syndrome. Clinical practice guideline: diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2002;109:704–12.
8. Gregor PB, Athanazio RA, Bittencourt AG, Neves FB, Terse R, Time F. Symptoms of obstructive sleep apnea-hypopnea syndrome in children. J Bras Pneumol 2008;34:356–61.
9. Pirelli P, Saponara M, De Rosa C, Fanucci E. Orthodontics and obstructive sleep apnea in children. Med Clin North Am 2010;94:517– 29.
10. Guilleminault C, Pelayo R, Leger D, Clerk A, Bocian RC. Recognition of sleep-disordered breathing in children. Pediatrics 1996;98:871–82.
11. Zucconi M, Caprioglio A, Calori G, et al. Craniofacial modifications in children with habitual snoring and obstructive sleep apnea: a casecontrol study. Eur Respir J 1999;13:411–7.
12. Live E, Stefini S, Annibale G, Pedercini R, Zucconi M, Strambi LF. Aspects of prevention of obstructive sleep apnea syndrome in developing children. Adv Otorhinolaryngol 1992;47:284.
13. Linder-Aronson S. Adenoids: Their effect on mode of breathing and nasal airflow and their relationship to characteristics of the facial skeleton and the dentition. The biometric, rhino-manometric and radiographic study cephalometric on children with and without adenoids. Acta Otolaryngol 1970;265:1–132.
14. Marcus CL, Brooks LJ, Ward SD, et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2012;130:714–55.
15. Carroll JL, McColley SA, Marcus GB Curtis S, Loughlin GM. Inability of clinical history to distinguish primary snoring from obstructive sleep apnea syndrome in children. Chest J 1995;108:610–8.
16. Erazo L, Ríos SA. Benchmark on obstructive sleep apnea screening automatic algorithms in children. Proc Comput Sci 2014;35:739–46.
17. Zhou M, Jiang M, Cheng Y, Li Z, Huang W, Xue F, Wang Q. Diagnosis of obstructive level in obstructive sleep apnea pharynx with hypopnea syndrome with multiple detector-row spiral CT. J Clin Otorhinolaryngol Head Neck Surg 2008;22:600–2.
18. De Moraes MEL, Hollender LG, Chen CS, Moraes LC, Balducci I. Evaluating craniofacial asymmetry with digital cephalometric images and cone-beam computed tomography. Am J Orthod Dentofacial Orthop 2011;139:E523–31.
19. El H, Palomo MJ. Measuring the airway in 3 dimensions: the reliability and accuracy study. Am J Orthod Dentofacial Orthop 2010;137:S50. e1–9; discussion S50–2.
20. Abramson ZR, Susarla S, Tagoni JR, Kaban L. Three-dimensional computed tomographic analysis of airway anatomy. J Oral Maxillofac Surg 2010;68:363–71.
21. Zinsly SR, Moraes LC, Moura P, Ursi W. Assessment of pharyngeal airway space using Cone-Beam Computed Tomography. Dental Press J Orthod 2010;15:150–8.
22. El H, Palomo, MJ. Airway volume is different dentofacial skeletal patterns. Am J Orthod Dentofacial Orthop 2011;139:E511–21.
23. Baccetti T, Franchi L. The fourth dimension in dentofacial orthopedics: treatment: timing for class II and class III malocclusions. World J Orthod 2001;2:159–67
24. Vos W, Backer JD, Devolder A, et al. Correlation between severity of sleep apnea and upper airway morphology based on advanced anatomical and functional imaging. J Biomech 2007;40:2207–13.
25. Kyung-Min O, Ji-Suk H, Yoon-Ji K, Cevidanes LS, Yang-Ho P. Threedimensional analysis of pharyngeal airway form in children with facial patterns anteroposterior. Angle Orthod 2011;81:1075–82.
26. Grauer D, Cevidanes LS, Proffit WR. Working with DICOM craniofacial images. Am J Orthod Dentofacial Orthop 2009;136:460–70.
27. Ribeiro AN, de Paiva JB, Rino-Neto J., Illipronti-Filho E, Trivino T, Fantini, SM. Upper airway expansion after rapid maxillary expansion. Evaluated with cone beam computed tomography. Angle Orthod 2012;82:458.
ACKNOWLEDGMENTS
The authors thank FAPESP foundation for the help given to research.SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication May, 2015
Submitted in final revised form April, 2016
Accepted for publication April, 2016
Address correspondence to: Rosa Carrieri Rossi, DDS, PhD, Division of Pediatric Otolaryngology, Federal University of Sao Paulo- UNIFESP Brasil, Rua Tijuco preto 1694, Tatuapé São Paulo BR, CEP: 03319000; Tel: 5511 29413629; Email: rosacrossi@gmail.com
DISCLOSURE STATEMENT
This was not an industry supported study. This study was Financed by FAPESP research foundation. FAPESP under the Protocol 2012/15715-2 November 2, 2012 http://www.fapesp.br/en/. This observational case-control study was approved by the Ethics Committee of The Federal University Sao Paulo - UNIFESP under the number: 1739/11 02/12/2011. The authors acknowledge the financial support by FAPEP for this project. The institution where the work was performed was UNIFESP – Federal University of São Paulo. All authors have reported no financial conflicts of interest.