Pro/Con Debate - PRO Issue 3.1
PRO: Upper Airway Resistance Syndrome Represents a Distinct Entity from Obstructive Sleep Apnea Syndrome
http://dx.doi.org/10.15331/jdsm.5366
Lauren Tobias, MD; Christine Won, MD, MS
Yale Centers for Sleep Medicine, Yale School of Medicine, New Haven, CT?
Controversy exists over whether the upper airway resistance syndrome (UARS) represents an entity whose pathophysiology and clinical characteristics are distinct from those of obstructive sleep apnea syndrome (OSAS). Many clinicians remain unconvinced of its clinical relevance as a unique disorder and instead believe it lies along the same spectrum as OSAS. We believe that ample evidence suggests UARS indeed represents a separate clinical phenomenon as opposed to simply a less severe form of OSAS, and that there is utility in considering it as a separate disorder.
UARS is a form of sleep disordered breathing characterized by repeated increases in upper airway resistance with concomitant increased respiratory effort, resulting in brief arousals. Such events are termed respiratory effort-related arousals or RERAs, where arousals are defined as a brief shift in alpha or fast theta frequency on the electroencephalogram (EEG) lasting from 3–10 seconds. RERAs are distinct from apneas or hypopneas in that they lack frank apneas or oxygen desaturation and are typically shorter (1 to 3 breaths), thereby failing to meet the generally accepted criteria for either apneas or hypopneas. RERAs are distinct from apneas or hypopneas in that they lack frank cessation of airflow or oxygen desaturation and are typically shorter (one to three breaths). By definition, the apneahypopnea index (AHI) in patients with UARS is less than five.
The gold standard measurement of RERAs in UARS is considered esophageal pressure monitoring (Pes), which detects progressive elevations in intrathoracic pressures with respiration leading up to an arousal. Most early publications of UARS utilized esophageal pressure monitoring and several abnormal forms of Pes tracings were described.1 Pes crescendo is characterized by a progressively increased negative peak inspiratory pressure in each breath, terminating with either an arousal or burst of delta wave on EEG. A second abnormality seen involves sustained continuous respiratory effort with a relatively stable and persistent negative peak inspiratory pressure seen on the Pes tracing to a degree greater than seen in baseline, non-obstructed breaths. The third form is Pes reversal, characterized by a sequence of increased respiratory efforts followed by a sudden decrement in respiratory effort indicated by a less negative peak inspiratory pressure.
Despite its utility, esophageal pressure monitoring has not been routinely adopted as part of standard polysomnographic setup in most sleep laboratories, since it involves the semi-invasive placement of a pediatric feeding catheter into the patient’s nostril down to the esophagus and the potential discomfort associated with this procedure. Ample evidence now suggests that RERAs may be adequately detected with nasal cannula pressure transducers (NCPTs) and this technology has been widely across the United States. We agree that sufficient data exists to accept NCPTs used in combination with respiratory inductive plethysmography (RIP) volume signals as an adequate substitute for esophageal pressure monitoring2,3 and certainly one with greater accuracy than a thermistor, for detecting flow-limited respiration in UARS.4 The superior tolerance of NCPTs by patients renders it a more convenient means of identifying subtle breathing abnormalities during sleep. The presence of flow limitation on the NCPT appears as a flattening of the normal bell-shaped curve of a normal breath with a drop in the amplitude by < 30% compared to normal breaths immediately preceding the drop.
Based on this definition alone, UARS would seem to potentially represent a milder degree of upper airway obstruction than is present in OSAS. If UARS existed simply on a spectrum with OSAS, however, we would expect to see the symptoms of this disorder on a continuum as well. Instead, research supports several symptoms unique/distinct to UARS and less predominant in OSAS (Table 1).
Table 1Clinical Features in upper airway resistance syndrome (UARS) and obstructive sleep apnea syndrome (OSAS). |
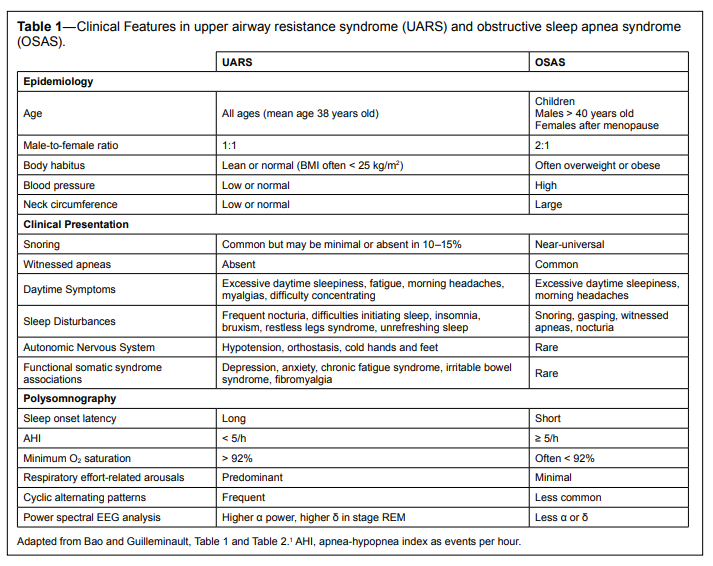{kind=link}
One of the central arguments in favor of UARS as a distinct entity stems from the differences in the population it affects. UARS patients tend to be leaner, with a mean BMI ≤ 25 kg/m2 , younger, with a mean age of 37.5 years, and equally present in males and females5 (although representing a greater proportion of sleep related breathing disorders in women6 ). Cephalometry has revealed craniofacial abnormalities in the upper airway anatomies of many UARS patients, including the presence of a long face, short and narrow chin with reduced mouth opening, retrolingual narrowing, increased overjet, high and narrow hard palate.7
A second argument in support of UARS as a distinct entity draws its support from the presenting complaints of these patients. UARS may occur in the absence of clinically significant snoring and may be an occult cause of excessive daytime sleepiness.8 UARS patients generally present with more subjective perception of daytime dysfunction in association with sleepiness than do OSAS patients.9 They complain of worse subjective sleep quality than OSAS patients as measured by standardized scales of insomnia, subjective sleepiness and sleep quality10 and higher rates of insomnia related to sleep initiation.6 Somatic complaints are more common and distinct personality characteristics are seen in these patients. Patients with UARS have been noted to complain more frequently of chronic insomnia and daytime sleepiness or fatigue than those with OSAS. Reports of headaches, vasomotor rhinitis, irritable bowel syndrome, difficulty in concentrating, and depressed mood have been described in association with UARS more frequently than OSAS. Patients with UARS tend to score more strongly toward neuroticism than OSAS patients on personality inventories8 and demonstrate increased somatic arousal as measured by self-report questionnaires.11 These observations have led to the suggestion that UARS may represent a functional somatic syndrome such as chronic fatigue syndrome and fibromyalgia. There are also objective measures suggesting that UARS is distinct from OSAS. Patients with UARS have been noted to perform more poorly than OSAS patients on tests of psychomotor vigilance,12 a proxy for daytime attentional function. In retrospective study of patients at an academic sleep center, a model fit to predict hypersomnolence among patients with both OSAS and UARS significantly underestimated hypersomnolence in UARS patients.13
A third line of argument comes from electroencephalographic spectral analysis, where EEG power is characterized for each sleep epoch on polysomnography. Patients with UARS are noted to have a general increase in alpha rhythm and relatively more delta power noted during stage REM sleep, in contrast to the reductions in both of these frequencies commonly observed in patients with OSAS.1 Furthermore, the presence of cyclic alternating pattern (CAP) on EEG has also been observed with higher frequency in patients with UARS than those with OSAS. In patients with UARS, CAP is a marker of sleep instability and poor sleep quality, and correlated with subjective symptoms of sleepiness and fatigue. Sleep disturbances in this population are often identifiable only with sensitive measures such as CAP analysis and not with traditional diagnostic scoring systems.14
Fourth, one of the pathologic lesions present in OSAS— local neurogenic lesions in the pharynx and upper larynx that interfere with maintenance of normal airway patency—does not appear to be present in patients with UARS.1 It has been hypothesized that this preservation of normal sensory input from the upper airways leads to faster arousal and recovery of normal breathing prior to the point of reaching levels of hypoxemia seen in OSAS.
A key question in this discussion is whether our current definition of OSAS, which allows for the scoring of hypopneas (reduced airflow or flow limitation) terminating not only in desaturation, but also in arousals, sufficiently captures all of those patients with clinical symptoms resulting from said arousals. We argue that it likely does not. OSAS is characterized by multiple pathologic perturbations including hypoxemia and re-oxygenation, increased intra-thoracic pressure and mechanical load, sympathetic activation, elevations of inflammatory markers, and arousals. The degree to which of each of these pathologic events contributes to adverse clinical outcomes likely differs and growing research is beginning to elucidate these differences. Indeed, evidence suggests that the arousals and associated sleep disruption which are central to the pathophysiology of UARS may be sufficient in themselves to cause adverse outcomes, even in the absence of hypoxemia. Human studies have reported associations between arousals and subjective sleepiness, changes in hormone secretion patterns, increased metabolic rate and increased sensory arousal threshold.15 Several studies have demonstrated a positive association between the number of arousals and awakenings seen on polysomnogram (PSG) and presence of hypertension. Evidence suggests that brief arousals from sleep, even for a single night, may affect levels of sleepiness the following day. For example, Philip et al. produced nocturnal auditory stimuli to elicit arousals and demonstrated a significant reduction in mean sleep latency on next-day multiple sleep latency testing (MSLT).16 In a similar experiment, Martin and colleagues demonstrated effects of such stimulation on mood and cognitive function.17
Most initial descriptions of disease began with clinical observations of the most pronounced, easily identifiable examples of a disorder. Over time, as the less “classic” manifestations of a disease are characterized and its prevalence explored in other populations, it is often recognized that the initial ontology was oversimplified. A disease’s expression in some populations may not be recognized until later on. This was in fact the case with obstructive sleep apnea, where reports of fatigue, headache, and mood disturbance rather than “classic” symptoms of snoring and witnessed apneas,18 were observed more commonly in women, and were not recognized for several years after its initial description. Once this realization occurred, OSAS was recognized to be more widely prevalent in women than was previously believed. Particularly in the case of UARS, we believe that erring in the direction of over- as opposed to under-diagnosis is prudent. The former risks needlessly treating some additional patients with a virtually harmless therapy that may be withdrawn at any point; the latter risks missing an opportunity to improve patients’ quality of life significantly. If we fail to acknowledge that UARS may represent a distinct clinical syndrome, we may less vigilantly ensure the scoring of RERAs and therefore miss opportunities to correlate these events with clinical outcomes in the future.6
We acknowledge that there are limitations in the current research on UARS, but view these as constructive starting points for further investigations as opposed to justification to dismiss the entity altogether. As the Greek playwright Sophocles stated, “Look and you will find it—what is unsought will go undetected.” One limitation of research to date on UARS involves the absence of a standardized definition across research groups and even within the same groups over time, as well as heterogeneity in the characterization of events that have been considered to meet criteria as RERAs. A second limitation is that much of the research on UARS has been conducted by only a few research groups and not yet replicated by other teams in different patient populations. Finally, a third limitation is the potential of sample bias in existing literature to have influenced the description of this entity. Specifically, most of the initial investigations by Guilleminault and colleagues occurred in a population of patients who had presented to sleep clinics. It stands to reason that such patients differ from the population of patients at large, and even from those who might have been randomly recruited from primary care clinics, in that they suffered symptoms stereotypical enough to result in subspecialty referral. This issue of sample bias may be even more relevant to sleep disorders than other medical disorders, since detailed sleep histories are not routinely elicited in primary care settings.19 Without comparison to the general population, it is therefore impossible to estimate the true risk conferred by polysomnographic findings of UARS as they relate to specific complaints or clinical outcomes. The first step to classification of any disease requires its recognition in a narrow patient population, but future work should more rigorously evaluate the prevalence of UARS symptoms and PSG findings in all patients, not simply in those with easily identifiable symptoms that drive them to seek care at a sleep clinic.
Even if the above definition of UARS evolves over time, as occurs with many disorders, it remains useful as a starting point. Indeed, our understanding of the pathophysiology of OSAS continues to evolve, with recent work suggesting the existence of multiple phenotypes of OSAS, characterized by the presence or absence of hypoxemia,20 genioglossus muscle responsiveness during sleep, arousal threshold, and presence of loop gain.21 A recent application of cluster analysis from the Icelandic Sleep Apnea Cohort has yielded a further classification scheme based on clinical subtypes that may eventually help us to identify patients with sleep apnea based on predominant presenting symptoms.22 We anticipate that these lines of inquiry will be further pursued in coming years, leading to a refined understanding and revised definitions of the sleep-related breathing disorders, their variable clinical and pathophysiologic profiles, and in turn, to modified treatment pathways for managing these patients. The true prevalence of UARS in the general population is not known, but we suspect it is substantial, and therefore feel it warrants further study.
In summary, we feel that UARS indeed represents a unique sleep-related breathing disorder distinct from OSAS, the heterogenous nature of which has only recently begun to be elucidated. If the disorder truly existed along a continuum with OSAS, we would expect to see a dose-dependent response between the degree of sleep disordered breathing and clinical symptomatology. As the aforementioned studies make clear, such a relationship has not been consistently seen. Rather, several symptoms appear to occur with increased frequency among patients with UARS and not in those with OSAS. Further work is needed in order to advance our understanding of UARS and its relationship to the more conventionally accepted sleep breathing disorders so that symptomatic patients do not continue to go untreated.
CITATION
Tobias L, Won C. PRO: Upper airway resistance syndrome represents a distinct entity from obstructive sleep apnea syndrome. Journal of Dental Sleep Medicine 2016;3(1):21–24.
REFERENCES
2. Epstein MD, Chicoine SA, Hanumara RC. Detection of upper airway resistance syndrome using a nasal cannula/pressure transducer. Chest 2000;117:1073–7.
3. Ayappa I, Norman RG, Krieger AC, Rosen A, O’Malley RL, Rapoport DM. Non-Invasive detection of respiratory effort-related arousals (REras) by a nasal cannula/pressure transducer system. Sleep 2000;23:763–71.
4. Montserrat JM, Badia JR. Upper airway resistance syndrome. Sleep Med Rev 1999;3:5–21.
5. Exar EN, Collop NA. The upper airway resistance syndrome. Chest 1999;115:1127–39.
6. Guilleminault C, Kirisoglu C, Poyares D, et al. Upper airway resistance syndrome: a long-term outcome study. J Psychiatr Res 2006;40:273–9.
7. Pépin JL, Guillot M, Tamisier R, Lévy P. The upper airway resistance syndrome. Respir Int Rev Thorac Dis 2012;83:559–66.
8. Kristo DA, Lettieri CJ, Andrada T, Taylor Y, Eliasson AH. Silent upper airway resistance syndrome: prevalence in a mixed military population. Chest 2005;127:1654–7.
9. Deary V, Ellis JG, Wilson JA, Coulter C, Barclay NL. Simple snoring: not quite so simple after all? Sleep Med Rev 2014;18:453–62.
10. So SJ, Lee HJ, Kang SG, Cho CH, Yoon HK, Kim L. A comparison of personality characteristics and psychiatric symptomatology between upper airway resistance syndrome and obstructive sleep apnea syndrome. Psychiatry Investig 2015;12:183–9.
11. Broderick JE, Gold MS, Amin MM, Gold AR. The association of somatic arousal with the symptoms of upper airway resistance syndrome. Sleep Med 2014;15:436–43.
12. Stoohs RA, Knaack L, Blum HC, Janicki J, Hohenhorst W. Differences in clinical features of upper airway resistance syndrome, primary snoring, and obstructive sleep apnea/hypopnea syndrome. Sleep Med 2008;9:121–8.
13. Gold AR, Gold MS, Harris KW, Espeleta VJ, Amin MM, Broderick JE. Hypersomnolence, insomnia and the pathophysiology of upper airway resistance syndrome. Sleep Med 2008;9:675–83.
14. Guilleminault C, Lopes MC, Hagen CC, da Rosa A. The cyclic alternating pattern demonstrates increased sleep instability and correlates with fatigue and sleepiness in adults with upper airway resistance syndrome. Sleep 2007;30:641–7.
15. Jaimchariyatam N, Rodriguez CL, Budur K. Sleep-related cortical arousals in adult subjects with negative polysomnography. Sleep Breath 2014;19:989–96.
16. Philip P, Stoohs R, Guilleminault C. Sleep fragmentation in normals: a model for sleepiness associated with upper airway resistance syndrome. Sleep 1994;17:242–7.
17. Martin SE, Engleman HM, Deary IJ, Douglas NJ. The effect of sleep fragmentation on daytime function. Am J Respir Crit Care Med 1996;153:1328–32.
18. Redline S, Kump K, Tishler PV, Browner I, Ferrette V. Gender differences in sleep disordered breathing in a community-based sample. Am J Respir Crit Care Med 1994;149:722–6.
19. Senthilvel E, Auckley D, Dasarathy J. Evaluation of sleep disorders in the primary care setting: history taking compared to questionnaires. J Clin Sleep Med 2011;7:41–8.
20. Palma J-A, Iriarte J, Fernandez S, et al. Characterizing the phenotypes of obstructive sleep apnea: clinical, sleep, and autonomic features of obstructive sleep apnea with and without hypoxia. Clin Neurophysiol 2014;125:1783–91.
21. Eckert DJ, White DP, Jordan AS, Malhotra A, Wellman A. Defining phenotypic causes of obstructive sleep apnea. Identification of novel therapeutic targets. Am J Respir Crit Care Med 2013;188:996–1004.
22. Ye L, Pien GW, Ratcliffe SJ, et al. The different clinical faces of obstructive sleep apnoea: a cluster analysis. Eur Respir J 2014;44:1600–7.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication October, 2015
Accepted for publication October, 2015
Address correspondence to: Christine Won, MD, PO Box 208057, 333 Cedar St, New Haven, CT 06520-8057; Tel: (203) 785-4163; Fax: (203) 785-3634; Email: Christine.won@yale.edu
DISCLOSURE STATEMENT
The authors have indicated no financial conflicts of interest.
PDF