Original Article, Issue 4.4
A Fully Digital Workflow and Device Manufacturing for Mandibular Repositioning Devices for the Treatment of Obstructive Sleep Apnea: A Feasibility Study
http://dx.doi.org/10.15331/jdsm.6742
Shouresh Charkhandeh, DDS1,2; David Kuhns, PhD3 ; Sung Kim, BS3
1The Snore Centre, Calgary, Canada; 2Zephyr Sleep Technologies, Calgary, Canada; 3ProSomnus Sleep Technologies, Dublin, California
ABSTRACT
Study Objectives:
The objective of this study was to examine the feasibility and patient preference of mandibular repositioning devices (MRDs) made from (1) a fully digital workflow including patient scanning, bite registration, and device manufacturing using an open platform intraoral scanner (iTero; Align Technology Inc., San Jose, California, United States) and a computer aided design/ computer aided manufacturing (CAD/CAM) MRD (MicrO2 Sleep Appliance; ProSomnus Sleep Technologies, Pleasanton, California, United States), and (2) a conventional workflow using polyvinyl siloxane (PVS) impressions as the source of patient data. The fit accuracy and comfort level of devices from each workflow were compared. A method for capturing a digital scan using a stable open bite technique is tested for accuracy and ease of implementation.
Methods:
This prospective feasibility study reports on selected patients (n = 5) recruited from a dental practice (ages 34 to 51 years; apnea-hypopnea index 1–32 events/h). Each patient received two MRDs. The first MRD was manufactured using a conventional workflow model (ie, PVS impressions, PVS bite registration, CAD/CAM of the MRD with quality control on physical stone models). The second MRD was manufactured using a digital workflow model (ie, digital intraoral scanning using an open platform intraoral scanner, digital open bite registration, and CAD/CAM of the MRD). All patients were then followed up using our standard clinical protocol set based on the American Academy of Dental Sleep Medicine guidelines. The dental fit (ie, the accuracy of the fit against the teeth), the occlusal fit (ie, the accuracy of the upper and lower splint fitting together), and the patient preference (ie, which appliance they preferred using) was recorded.
Results:
In the conventional workflow 2 appliances required minor dental adjustments and 3 appliances required occlusal adjustments. In the digital workflow, no dental or occlusal adjustments were required. All patients preferred the digital MRDs in terms of comfort.
Conclusions:
It is feasible to utilize a fully digital workflow for manufacturing of MRDs for treatment of obstructive sleep apnea with predictable outcomes. Devices from a full digital workflow are preferred by patients compared to the standard process. The full digital workflow using the CAD/CAM MRD required fewer adjustments and patient satisfaction with the device and the process could make for a better experience for the patient and the doctor. Follow-up studies are required using larger sample size and different intraoral scanners and MRDs.
Keywords:
bite registration, device manufacturing, digital workflow, intraoral scanning, mandibular repositioning devices, obstructive sleep apnea, oral appliance therapy
Citation:
Charkhandeh S, Kuhns D, Kim S. A fully digital workflow and device manufacturing for mandibular repositioning devices for the treatment of obstructive sleep apnea: a feasibility study. Journal of Dental Sleep Medicine. 2017;4(4):97–102.
INTRODUCTION
Obstructive sleep apnea (OSA) is a very common chronic disease with many adverse clinical consequences, affecting an estimated 10% to 20% of the United States population.1,2 The condition remains undiagnosed in most of these patients, and studies show the percentage of undiagnosed OSA could be as high as 80% to 90%.3,4 Untreated OSA is associated with higher risk of fatal cardiovascular and cerebrovascular events,5-8 hence, the importance of long-term treatment of patients. Currently, the most commonly prescribed treatment for patients with OSA is continuous positive airway pressure (CPAP) therapy. Although this treatment is efficacious and relatively safe with minor side effects, patient adherence is low and many patients refuse to start CPAP treatment. It is reported that patient adherence to CPAP could be as low as 50%; therefore, an alternative therapy is required.9,10 Based on published American Academy of Sleep Medicine guidelines, oral appliances are recommended as an alternative for patients with mild to moderate OSA and patients who cannot tolerate CPAP or are not adherent to the therapy.11 There has been tremendous growth in this area of dentistry over the past decade and many patients are now seeking this treatment modality. It is estimated that approximately 200,000 appliances are being made every year in North America and by the year 2023 this number will reach over 1 million. Although the growth seems to be very fast, it is worth noting that currently fewer than 10% of patients who could respond to oral appliance therapy (OAT) receive a mandibular repositioning device (MRD).12 Based on meta-analysis, 50% to 60% of all patients with OSA would respond to OAT,11 but MRDs are only prescribed in 5% to 10% of all diagnosed patients.
The number of patients prescribed an MRD could increase because of many factors, such as the general public’s raised awareness of the importance of proper sleep, positive health outcomes associated with OAT, and prospective selection of patients who would respond to OAT.12,13 Although this is great news in terms of growth in the field of dental sleep medicine, the number of patients will increase our current clinical workflow models and device manufacturing may not be able to keep up with the increased demand. Therefore, having more efficient workflow systems and device manufacturing become crucial in delivery of care.
The use of intraoral scanners for digital impressions of the teeth and a fully digital workflow system, including the device manufacturing, could be a way to more efficiently produce MRDs. The use of digital scanners in dentistry is expected to grow by 13.9% (compound annual growth rate) from 2015 to 2022.14 Digital scanners have been used widely in the dental industry over the past decade and there seems to be a lot of inconsistent results in terms of being able to register the maxillomandibular occlusal relationship, when the teeth are not fully occluding (ie, “digital open bite registration”). This has been the main hurdle for many practitioners to make use of a fully digital workflow, and therefore, they still use a conventional “bite registration.” This creates inefficiencies in the workflow, and it has the potential to introduce inaccuracies in device manufacturing. The difference in the degree of accuracy between conventional bite registration using polyvinyl siloxane (PVS) and digital bite registration could result in improper articulation of the models. An additional benefit of a fully digital manufacturing process is the reduced need for physical models.
If a reliable, fully digital workflow can be established, it could improve patient care by providing more efficient and accurate care to the patient. The objective of the current study was to examine the feasibility and patient preference of MRDs made from a fully digital workflow versus the conventional workflow.
METHODS AND RESULTS
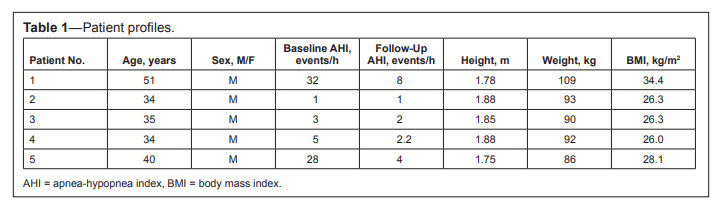
Five patients were selected to participate in this feasibility study. The patients’ characteristics and data are summarized in Table 1. They were all tested for sleep apnea using an at-home level 3 sleep recorder. The patients’ baseline apnea-hypopnea indexes are summarized in Table 1. After the baseline sleep study, all patients received full orthodontic records (ie, upper and lower PVS impressions, intraoral/extraoral photographs, and cone beam computed tomography). Proper medical history, dental history, and consent forms were signed. All patients were also examined by a dentist to determine the suitability for an MRD.
Table 1Patient profiles. |
{kind=link}
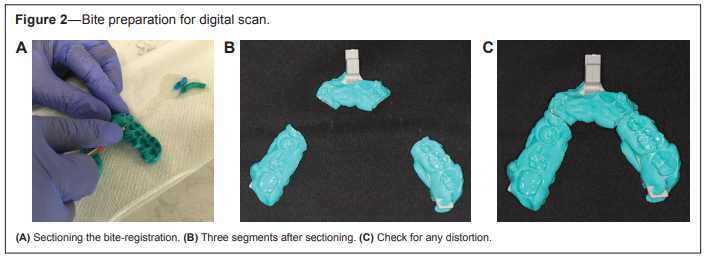
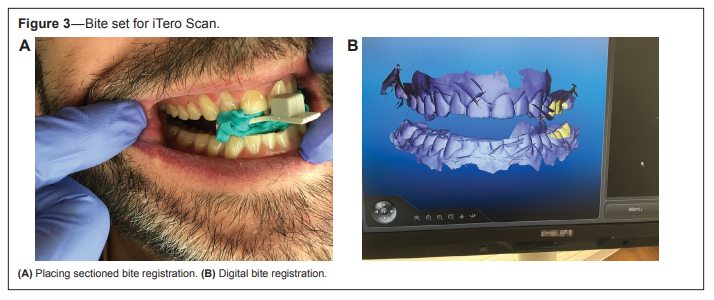
Each patient went through both MRD manufacturing workflow models. They first went through the conventional workflow (Figure 1) using a George Gauge (Great Lakes Orthodontics, New York, United States) to obtain a PVS bite registration. All patients then went through the digital workflow model (Figure 2). The digital workflow started with taking upper and lower intraoral scans using the Ortho Software Module on the iTero scanner (Align Technology Inc., San Jose, California, United States). The bite registration was taken using the initial bite and protrusion level as a reference. In order to stabilize the bite at the protruded position and enabling a scan of the “maxillomandibular” relation, the dentist segmented each bite into 3 pieces, using a surgical blade and a heat torch. The blade was used to cut through the PVS material, to minimize the chipping of the material and distortion of the bite. The heat torch was used to enable cutting through the plastic fork of the George Gauge without creating any distortion in the bite (Figure 2). The bite was then stabilized by asking the patient to bite into 2 out of the 3 pieces for each bite scan. When scanning the left side, the anterior and the right segments were seated (Figure 3). When scanning the right side, the anterior and the left segments were seated in patients’ mouths. This stabilization method was used to minimize the amount of distortion and inaccuracies in the bite registration by minimizing the possible cantilever effect and compression of retrodiscal tissue in the temporomandibular joint when no posterior support is present or there is movement of the mandible with respect to the maxilla. All scans were sent to the appliance manufacturer (ProSomnus Sleep Technologies, Pleasanton, California, United States).
Figure 1PVS and digital patient data capture. |
{kind=link}
Figure 2Bite preparation for digital scan. |
{kind=link}
Figure 3Bite set for iTero Scan. |
{kind=link}
Upon receipt by the manufacturer, each physical impression was poured and articulated with the bite. The bite was then inspected to ensure enough vertical gap (> 3 mm) to enable manufacture of the MicrO2 Sleep Appliance (ProSomnus Sleep Technologies, Pleasanton, California, United States).A technician measured the vertical gap between the upper and lower arches, and determined if any anatomical features are closer to each other than the required specification of 3 mm as described in the manufacturing technical work instructions. This could be the vertical gap between 2 opposing cusps, for example. All technicians were trained to the same work instructions and specifications. If the specification was not met, the data would be reviewed by quality personnel to determine if a new bite would be required. The models were scanned separately and together with the bite and the files were imported into the design software. Digital arches and bites were received through the vendor’s portal and imported into the design software. Once uploaded, the quality of the scans and bites were inspected digitally. The scan quality specification included evaluating that the digital mesh represents the physical model without holes in the mesh or missing data that would prohibit the manufacture of the device.
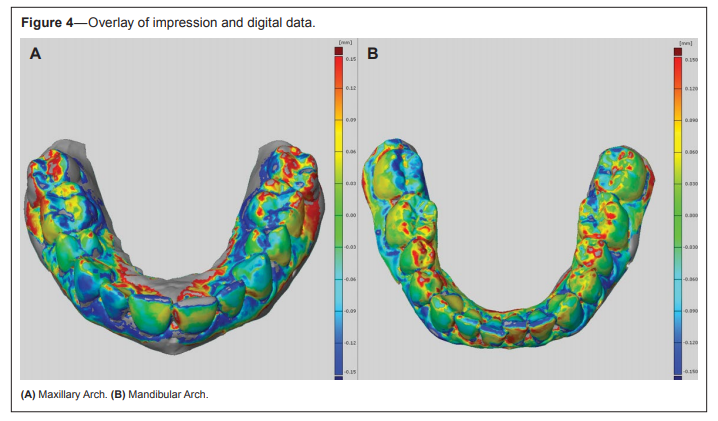
To complete the comparison of the physical impressions and digital impressions, both were loaded into the design software and set in place using the same coordinate system. With the models layered (Figure 4), a color map was generated showing the distance difference between each surface point for the 2 files. Figure 4 shows the upper arch overlay on the left and the lower arch overlay on the right, both with a scale of ± 150 microns. The gray reference portions of the overlay represent the scans of the poured impressions; the colorized map shows the delta intersection of the layered digital scan, with red above the reference surface and blue below the reference surface. The green areas describe areas of agreement between the scanned stone model and the iTero scan directly from the patient. However, many areas of deviation are denoted by blues and reds in the 2 images.
Figure 4Overlay of impression and digital data. |
{kind=link}
Each patient then received both appliances and wore each appliance for 3 weeks. The dentist also recorded the amount of adjustment needed for each device in terms of adjustment made to the inside surface (to fit the teeth) and adjustment to the occlusal surfaces (to achieve properly balanced occlusion). The results are summarized in Table 2. After wearing each device for 3 weeks, each patient was asked which appliance they preferred in terms of comfort. The conventional device was worn first, followed by the digital device. There was no washout period between the 2 appliances. The results are shown in Table 2. A follow-up sleep study was performed to evaluate the efficacy of the treatment, and the patients’ followup apnea-hypopnea indexes are summarized in Table 1.
Table 2Fit adjustments and patient preference for each process. |
{kind=link}
DISCUSSION
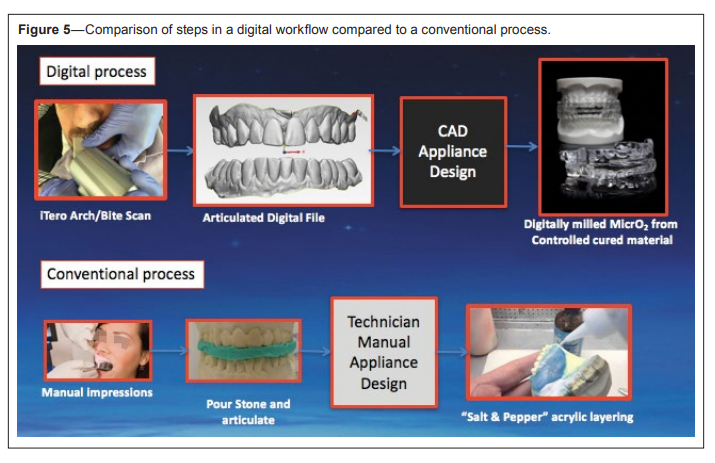
The results of the study suggest that it is feasible to implement a fully digital workflow using the existing technology in a dental practice and device manufacturing facilities, with no need for physical dental models. The digitally designed and manufactured devices had better accuracy in terms of dental fit and occlusal/bite fit as demonstrated by the digital file overlay and patient preference. All patients preferred the digital devices in terms of comfort. Although the sample size in this study was very small and further controlled double-blinded studies are required to reproduce the results, the possibility of having a fully digital workflow in dental sleep medicine is potentially beneficial for both the patient and the clinician. Digital scans seem to be preferred by most patients in terms of comfort.15 Dental clinicians using such technologies will minimize the chances of distortion and inaccuracies,and in case of a distorted scan,a full new impression will not be required. The distorted segment can easily be erased and re-scanned. Also,device manufacturing companies prefer the digital workflow due to the consistency,efficiency and in-office inspection of scan quality. Figure 5 illustrates the reduction in manual steps in a digital workflow. Each manual step adds error due to human touch that varies by technician. Additionally,manually designing and building up the device via the “salt and pepper” method also adds technique and material variance. The monomer/polymer mix, cure time, and resultant properties will also be varied. Milling from a controlled cured material reduces these errors, allowing better translation of data from the patient to the finished device. This results in less time being spent both in terms of the dental clinic and in manufacture of the device. A digital workflow model may also help provide faster turnaround time for the appliance delivery and hence provide more timely care for patients in need of an MRD. Currently,time to efficacious treatment for CPAP therapy can be very quick,whereas that for OAT appears to take more time. This can be caused by many factors such as lack of proper patient selection,subjective titration,and conventional device manufacturing. However,with better methods for patient selection for OAT and efficacious target protrusion,this time can be reduced significantly.
Figure 5Comparison of steps in a digital workflow compared to a conventional process. |
{kind=link}
The addition of fully digital device manufacturing could be a significant addition to this model by further reducing the time to efficacious treatment. Also, incorporating digital workflow in dental sleep medicine would allow better long-term monitoring of occlusal changes for patients with an MRD, as the digital scans can be readily stored, retrieved, and compared. As the demand for OAT and MRDs increases, we as clinicians and practice managers will require workflows and manufacturing technologies that are easily scalable. The full digital workflow model is aligned with the future need to treat the many patients who will soon receive a diagnosis.
In terms of the bite registration and the translation of a conventional bite to a digital bite registration, the investigators found that this procedure is very technique sensitive at this stage and depends heavily on the expertise of the clinician and their level of experience with digital scanners. An important aspect is to have proper stabilization of the protrusive bite to prevent any unwanted movement of the mandible and the dentition during the scanning. Another very important aspect is to maintain the proper vertical dimension both in anterior and posterior region. Failure to provide such posterior support may result in unwanted compression of the soft tissue around the temporomandibular joint, thus resulting in an inaccurate bite registration. Keeping this in mind, a properly designed gauge specifically designed for digital open bite registration could be very helpful in overcoming discrepancies.
The sample size was very small for this study and the process was limited to one type of scanner and device type. Investigators believe more testing with higher numbers of patients and utilizing different scanners and appliance designs would be beneficial. Because of the small number of participants, the statistical significance of the results is unknown and a followup randomized study with a larger sample size would be necessary for better statistical analysis of the results. In addition, randomizing the sequence of conventional versus digital MRDs with a washout period added in between would be important for a more accurate comparison. Also, an easier and less technique-sensitive bite registration process needs to be established to avoid segmenting the bite and creating possible issues. With the increasing number of patients requiring MRD, such an approach could result in more efficient workflow models with faster turnaround time, and more accurate and more costeffective and scalable workflows. More follow-up studies would be useful to understand how such digital workflow, in combination with other available technologies for patient selection, would affect the general efficiency of clinical care delivery for OAT, including time to efficacious treatment, avoidance of OAT nonresponders, number of appointments required for OAT, cost of total treatment, and patient satisfaction.
REFERENCES
2. Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328(17):1230–1235.
3. Kapur V, Strohl KP, Redline S, Iber C, O’Connor G, Nieto J. Underdiagnosis of sleep apnea syndrome in U.S. communities. Sleep Breath. 2002;6(2):49–54.
4. Young T, Skatrud J, Peppard PE. Risk factors for obstructive sleep apnea in adults. JAMA. 2004;291(16):2013–2016.
5. Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342(19):1378–1384.
6. Peker Y, Carlson J, Hedner J. Increased incidence of coronary artery disease in sleep apnoea: a long-term follow-up. Eur Respir J. 2006;28(3):596–602.
7. Punjabi NM, Polotsky VY. Disorders of glucose metabolism in sleep apnea. J Appl Physiol. 2005;99(5):1998–2007.
8. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoeahypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046–1053.
9. Engleman HM, Wild MR. Improving CPAP use by patients with the sleep apnoea/hypopnoea syndrome (SAHS). Sleep Med Rev. 2003;7(1):81-89.
10. McArdle N, Devereux G, Heidarnejad H, Mackay T, Douglas N. Long term use of CPAP therapy for sleep apnea/hypopnea syndrome. Am J Respir Crit Care Med. 1999;159(4 Pt 1):1108-1114.
11. Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: an update for 2015. J Clin Sleep Med. 2015;11(7):773–827.
12. Frost & Sullivan. Hidden health crisis costing America billions. Underdiagnosing and undertreating obstructive sleep apnea draining healthcare system. American Academy of Sleep Medicine website. http://www.aasmnet.org/sleep-apnea-economic-impact.aspx. Published 2016. Accessed August 24, 2017.
13. Remmers J, Charkhandeh S, Grosse J, et al. Remotely controlled mandibular protrusion during sleep predicts therapeutic success with oral appliances in patients with obstructive sleep apnea. Sleep. 2013;36(10):1517-1525.
14. News & Trends/Industry News. Dentistry Today. 2016;35(9):48.
15. Yuzbasioglu E, Kurt H, Turunc R, Bilir H. Comparison of digital and conventional impression techniques: evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral Health. 2014;14(10):7.
ACKNOWLEDGMENTS
The authors thank the clinical staff at The Snore Centre (Amanda Duffy and Ava McLellan) and the iTero Regional Manager, John Martin for their clinical support. We also thank the ProSomnus Sleep Technologies team for their support.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication February 2, 2017
Submitted in final revised form June 24, 2017
Accepted for publication July 12, 2017
DISCLOSURE STATEMENT
This study was funded by ProSomnus Sleep Technologies. Dr. Kuhns is VP of Technology and Sung Kim is VP of Engineering at ProSomnus. Dr. Charkhandeh is the Clinical Director at The Snore Centre and the Chief Dental Officer at Zephyr Sleep Technologies.