Original Article, Issue 3.2
Treatment of Obstructive Sleep Apnea with a Tongue-Stabilizing Device at a Single Multidisciplinary Sleep Center
http://dx.doi.org/10.15331/jdsm.5716
Mariko Yanagihara, MD1,2,3; Satoru Tsuiki, PhD1,2,4; Yasuhiro Setoguchi, PhD3 ; Yuichi Inoue, PhD1,2,4
1Institute of Neuropsychiatry, Tokyo, Japan; 2Foundation of Sleep and Health Sciences, Tokyo, Japan; 3Department of Respiratory Medicine, Tokyo Medical University, Tokyo, Japan; 4Department of Somnology, Tokyo Medical University, Tokyo, Japan
ABSTRACT
Study Objectives:
Mandibular advancement devices (MADs) may not be acceptable for use in patients with obstructive sleep apnea (OSA) when dental and/or temporomandibular joint side effects are likely. Tongue-stabilizing devices (TSDs) are a potential alternative to MAD therapy. We aimed to document the outcome of TSD treatment at a single multidisciplinary sleep center.
Methods:
OSA patients for whom MAD treatment was contraindicated due to dental and/or temporomandibular joint problems were prescribed a TSD. Follow-up overnight polysomnography (PSG) was performed with a TSD in place. Responders were defined as patients with a reduction in the apnea-hypopnea index (AHI) to less than 5 events/h as well as more than a 50% reduction in baseline AHI.
Results:
Of 551 patients who were referred for oral appliance therapy, 76 (100%) were prescribed a TSD. There were patients who were acclimatizing to TSD (n = 6; 8%), intolerant (n = 22; 29%), lost to follow-up (n = 26; 34%), and stopped using TSD by other reasons (n = 6; 8%). Of the 16 subjects (21%) who completed follow-up testing of PSG, the mean baseline AHI was reduced from 21.8 ± 8.6 to 9.3 ± 5.8 events/h (p < 0.01) with a TSD in place. The TSD improved AHI from 14.2 ± 2.9 to 2.1 ± 1.3 events/h in 5 responders (7%) (p < 0.01).
Conclusions:
The efficacy of the TSD was similar to that reported for MADs as long as the TSD was tolerated, especially in mild OSA patients. However, the high percentage of treatment dropout and/or lost to follow-up suggests the potential need for appliance redesign or modification to improve patients’ adherence to therapy.
Keywords:
obstructive sleep apnea, oral appliance, tongue-stabilizing device
Citation:
Yanagihara M, Tsuiki S, Setoguchi Y, Inoue Y. Treatment of obstructive sleep apnea with a tongue-stabilizing device at a single multidisciplinary sleep center. Journal of Dental Sleep Medicine 2016;3(2):43–47.
INTRODUCTION
Obstructive sleep apnea (OSA) is a major public health problem that has been associated with long-term adverse health consequences including hypertension, metabolic dysfunction, and cardiovascular disease.1 Nasal continuous positive airway pressure (nCPAP) has been the standard treatment for OSA for more than three decades,2 while oral appliances (mandibular advancement devices [MADs]) and tongue-retaining devices have been prescribed for patients with mild to moderate OSA and/or who fail to use nCPAP.3,4 In clinical settings, both sleep dentists and physicians often encounter patients for whom MADs are contraindicated even for mild OSA and nCPAP failure due to compromised dentition, severe periodontal disease, or temporomandibular joint disorders.4
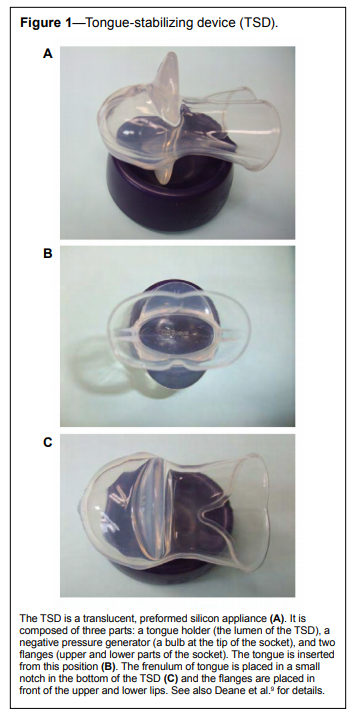
A tongue-retaining device that maintains the tongue in a protruding position by suction was first documented by Cartwright and Samelson in 1982.5 The device can be recommended for OSA patients when MADs are contraindicated, although these devices are generally less common and less efficacious than MADs.6–8 A tongue-stabilizing device (TSD) is a type of tongueretaining device that is now commercially available (Aveo-TSD, Innovative Health Technologies, New Zealand) (Figure 1).9–11 The great differences between the earlier design of the tongueretaining device reported in 1982 and the TSD are their design and fabrication. The tongue-retaining device is custom made from dental casts since the appliance entirely covers the upper and lower dental arches for appliance retention. Conversely, TSD is a preformed silicone appliance without dental coverage but still has the anterior bulb being retained in place only by tongue suction.9,10 Therefore, patients need no dental impression undertaken for TSD fabrication; it could be assumed that TSD has succeeded in reducing bulk in comparison with the original tongue-retaining device. Because of this simplicity, TSD was used to prevent snoring at temporary refuges after the earthquake and nuclear power plant accident in Japan in 2011.11
Figure 1Tongue-stabilizing device (TSD). |
{kind=link}
Several studies have demonstrated that the TSD is as efficacious as a titratable oral appliance for improving OSA.9,10 The results of research and the advantage of its simplicity in the field suggest that the TSD may be underused in the treatment of OSA. However, to date, there have been no observational reports on its prescription, effectiveness, or tolerance in a clinical setting. The purpose of this study was to document patient flow and the outcome of TSD treatment at a single multidisciplinary sleep center. This is the first report of TSD use in a clinical setting.
METHODS
Patients
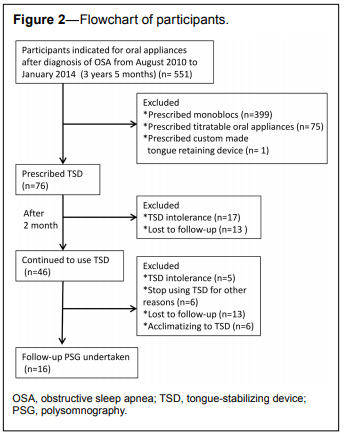
The protocol of this investigation was approved by the ethics committee of the Foundation of Sleep and Health Sciences, Tokyo, Japan. Figure 2 shows the flow of participants. The prospective recruitment of eligible patients was conducted over a period of 41 months (3 years 5 months) from August 2010, when the first TSD was prescribed at the Yoyogi Sleep Disorder Center, Tokyo, to January 2014. Patients who were indicated for oral appliance therapy after a diagnosis of OSA (n = 551) were referred to the sleep apnea dental clinic at the Yoyogi Sleep Disorder Center. This patient recruitment was also performed consecutively. Inclusion criteria were: Japanese of both genders who were diagnosed with OSA (apnea-hypopnea index [AHI] > 5 events/h) by initial overnight polysomnography (PSG) performed at the center; OSA patients for whom MADs were contraindicated because of severe periodontitis, insufficient number of teeth, denture use, and/or temporomandibular joint dysfunction. Both mild-to-moderate OSA patients who did not require nCPAP and moderate-to-severe OSA patients who failed to use nCPAP were included. Patients who met one or more of the following exclusion criteria were excluded: severe cardiovascular disease, medically complicated, or medically unstable. Patients who were prescribed monoblocs (ASO International, Tokyo, Japan) (n = 399), titratable oral appliances (SomnoDent, SomnoMed Japan, Japan) (n = 75), or custom-made tongue-retaining devices (ASO International, Tokyo, Japan) (n = 1) were also excluded.12,13 Consequently, 76 patients were prescribed a TSD during the study period. All of these patients agreed that their PSG results could be used for research purposes, and provided written informed consent with respect to the anonymous use of their data.13
Figure 2Flowchart of participants. |
{kind=link}
Polysomnographic Evaluation
Episodes of hypopnea were determined based on the American Academy of Sleep Medicine criteria of a reduction in airflow amplitude ≥ 50% from baseline persisting for ≥ 10 s, or some level of reduction in airflow amplitude persisting ≥ 10 s with the presence of respiratory-associated arousal and/or oxygen desaturation ≥ 3% (Chicago criteria).14 The severity of OSA was assessed in terms of AHI (mild [AHI ≥ 5 to < 15 events/h], moderate [AHI ≥ 15 to < 30 events/h], and severe [AHI ≥ 30 events/h]).
Tongue-Stabilizing Device
Detailed information on the TSD and its indications have been reported previously.9,10 Briefly, the tongue is inserted into the anterior bulb and sucked by the negative pressure generated by squeezing the bulb. Potential risks of the TSD include soreness and/or discomfort of the tongue, excessive saliva or dry mouth, and discomfort of the lips, teeth, and gums.9,10 Use of a TSD is associated with minimal side effects in the temporomandibular joint.
Protocol and Treatment Outcome
A TSD was prescribed after the methods were explained in detail. Patients were advised to increase the suction level as necessary to maintain sufficient retention, or to decrease suction if they felt excessive discomfort on their tongue. A second overnight PSG was undertaken with the TSD in place when patients had used the TSD regularly and experienced subjective improvements in OSA symptoms, such as with regard to snoring, morning headache, or sleep quality. Changes in daytime sleepiness were evaluated with the Japanese version of the Epworth Sleepiness Scale (JESS).15 Responders to TSD treatment were defined as patients who showed a reduction in AHI to < 5 events/h with a > 50% reduction in baseline AHI.12Statistical Analysis
The normality of the data distribution was assessed using the Kolmogorov-Smirnov test. Paired t-tests were used to compare the differences in PSG variables between baseline and follow-up, whereas unpaired t-tests were used to compare the difference in each PSG variable between responders and non-responders. Sensitivity, specificity, and positive and negative predictive values were also assessed based on a 2 × 2 cross table that was used to investigate the effect of baseline AHI on the responder-nonresponder distribution. Finally, in order to describe any differences in those patients who continued and who discontinued treatment (excluding subjects who were lost to followup), a univariate logistic regression followed by a multivariate logistic regression analysis was performed to investigate contributions to the likelihood of continuation of TSD therapy by incorporating gender, age, JESS, BMI, and baseline AHI. A p value of < 0.05 was considered to be statistically significant.RESULTS
A total of 76 subjects were prescribed a TSD (Figure 2). Thirty patients dropped out of TSD treatment within 2 months. Of these 30 subjects, 17 patients complained of tongue soreness and/or dry mouth and/or increased salivation and/or disturbed sleep due to irritation of the tongue and soft tissues. All 17 patients also complained that TSD came off easily. The remaining 13 patients were lost to follow-up. After 2 months, 5 patients dropped out because of the same reasons as the above 17 patients. Six patients stopped using TSD because of falling off (n = 3), appliance broken (n = 1), dental treatment required (n = 1), and decease (n = 1). In addition, there were 13 patients lost to follow-up and 6 patients who were acclimatizing to TSD.
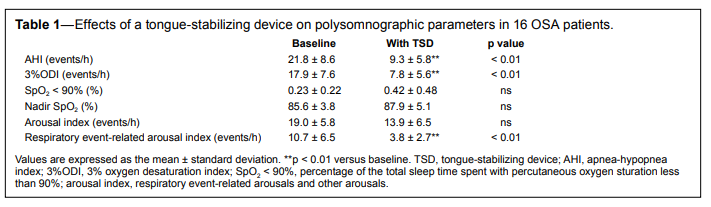
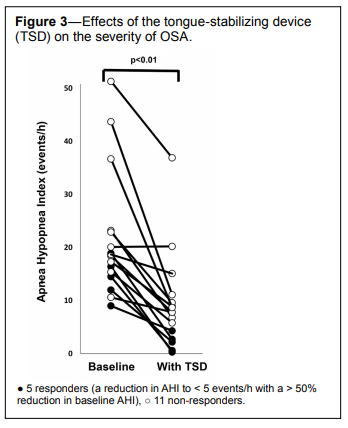
Sixteen of the 76 OSA patients (7 males and 9 females) completed a follow-up PSG with a TSD in place (Table 1). The mean ± standard deviation (SD) of age, BMI, and JESS at baseline in these 16 patients were 63.6 ± 9.2 years, 24.0 ± 2.9 kg/m2 , and 12.0 ± 5.3 points, compared to 64.6 ± 9.2 years, 24.1 ± 3.0 kg/m2 , and 9.8 ± 4.8 points at follow-up PSG with a TSD in place. There were no significant changes in BMI or JESS throughout the study. TSD significantly reduced AHI (p < 0.01), 3% oxygen desaturation index (3%ODI) (p < 0.01), and respiratory event-related arousal index (p < 0.01), while no significant changes were seen in the percentage of total sleep time spent with percutaneous oxygen saturation less than 90% (SpO2 < 90%), nadir SpO2, and arousal index (Figure 3).
Table 1Effects of a tongue-stabilizing device on polysomnographic parameters in 16 OSA patients. |
{kind=link}
Figure 3Effects of the tongue-stabilizing device (TSD) on the severity of OSA. |
{kind=link}
Among the 16 patients who completed a follow-up PSG with a TSD in place, there were 5 responders (31.3%) and 11 non-responders (Table 2). Among the responders, TSD treatment reduced 3%ODI from 11.0% ± 4.8% to 2.2% ± 1.6% (p = 0.04) and increased the nadir SpO2 value from 84.2% ± 3.7% to 93.0% ± 1.6% (p = 0.03). No significant changes were found in the arousal index or the respiratory arousal index. In non-responders, TSD reduced AHI (p < 0.01), 3%ODI (p < 0.01), and the respiratory arousal index (p = 0.02). Moreover, the mean baseline AHI of non-responders (AHI = 25.3 ± 10.1 events/h) was significantly higher than that of responders (AHI = 14.2 ± 2.9 events/h) (p = 0.02).
Table 2Comparison of each parameter between responders and non-responders to TSD. |
{kind=link}
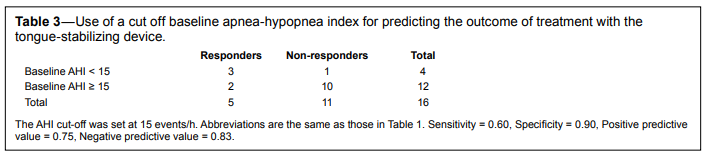
When the 16 patients were divided into a mild OSA group (baseline AHI < 15) and a moderate to severe OSA group (baseline AHI > 15 events/h), this cutoff value gave a sensitivity/ specificity and positive predictive value/negative predictive values of 0.60/0.90 and 0.75/0.83, respectively. Accordingly, 3 of 4 (75%) patients with mild OSA responded whereas only 2 of 12 (17%) patients with moderate to severe OSA responded to TSD.
A univariate logistic regression analysis revealed that continuation of TSD treatment was not associated with gender (odds ratio [95% confidence interval]) (0.417 [0.095–1.830], p = 0.417), age (1.023 [0.951–1.101], p = 0.536), BMI (1.002 [0.791–1.271], p = 0.986), JESS (1.076 [0.927–1.249], p = 0.337), and baseline AHI (1.049 [0.973–1.132], p = 0.210). No significant observation was also found when multivariate logistic regression analysis was applied (data not shown).
DISCUSSION
This is the first report to document TSD use in a single multidisciplinary sleep center. Of the 16 subjects who completed the protocol, only 5 patients had an AHI on TSD treatment that met criteria for an acceptable response used in previous reports.12,13
The treatment success rate with MADs has been reported to range from 19% to 57% when treatment success was defined as follow-up AHI < 5 events/h.4 In 16 patients who completed follow-up PSG with TSD in place, the treatment success rate with a TSD was 31%, which was slightly better than the 22.7% reported by Deane et al.9 under the same responder criterion. Therefore, we speculate that TSD could also be recommended for OSA patients for whom MADs are indicated. Lazard et al.7 reported that the conventional tongue-retaining device provided a complete success (post-treatment AHI < 10) rate of 47% and a partial response (10 < follow-up AHI < 20 with > 50% reduction from baseline AHI) rate of 24%. Under the same definition of responder as Lazard et al.,6 the complete and partial response rates in our study were 75% and 12.5%, respectively. A balanced combination of positive predictive value and negative predictive value of 0.75/0.83 supports the notion that a TSD is efficacious, although the number of total subjects was limited.
By contrast, to authors’ surprise, only 16 of 76 TSD users (21%) managed to complete the follow-up PSG with a TSD. Furthermore, based on the total number of 76 patients, only 7% (5 responders) had a successful outcome. We were greatly disappointed that 34% (26/76) of TSD users were gradually lost to follow-up and 29% (22/76) did not tolerate the appliance, although all of the patients were encouraged to regularly visit the outpatient clinic after appliance prescription. Since an additional logistic regression analysis demonstrated that continuation of TSD treatment was not associated with gender, age, JESS, BMI, and the severity of OSA at baseline, we speculate that the lower adherence may be due to the side effects, which included excess salivation, dryness of the mouth, and irritation of the tongue and soft tissues. These side effects have been previously reported by Deane et al.8,9 Dort and Brant reported that 45% of users indicated that they would continue treatment with a tongue-retaining device because their snoring was reduced.6 While a TSD was likely to benefit OSA patients based on a balanced positive predictive value and negative predict value in this study (Table 3), an unexpectedly higher percentage of intolerance and lost to follow-up within 2 months could be related to an attenuated risk-benefit profile. Therefore, modification of the appliance design to decrease subjective symptoms and discomfort of the tongue may be needed, while retaining the simplicity of the design. A TSD should still be considered in the treatment of OSA for individuals who cannot use either nCPAP or MADs.
Table 3Use of a cut off baseline apnea-hypopnea index for predicting the outcome of treatment with the tongue-stabilizing device. |
{kind=link}
Pathophysiologically, the velopharynx is the major site of occlusion in patients with OSA.16 A previous report demonstrated that a TSD improved velopharyngeal airway patency by a ventral displacement of the tongue.10 Since simple tongue stabilization at a protruded position appears to produce ventral traction of the soft palate, even without mandibular advancement,17 the connection between the tongue and the soft palate via the palatoglossus muscle could contribute to the favorable response. To increase the retention of the tongue in a protruded position, Dort and Brant attempted to narrow the base of the tongue bulb and succeeded in improving the respiratory disturbance index in OSA patients.5 Dort and Remmers17 further suggested that the efficacy of treatment improved when an anterior bulb was incorporated into a mandibular advancing splint. Tsuiki et al.19 recently reported that holding the tongue in position would likely alleviate dorsal displacement of the tongue while sleeping in a severe OSA patient without protruding the tongue. Thus, an approach that focuses on controlling the tongue in position, rather than tongue protrusion, could be meritorious in oral appliance therapy while avoiding (1) the common dental/ temporomandibular joint side effects frequently seen with the use of MADs and (2) the irritation/soreness of the tongue in TSD therapy, leading to improving patients’ adherence.
In conclusion, we have documented the outcome of TSD use in a single multidisciplinary sleep center. A TSD can be as efficacious as mandibular advancing splints, especially in patients with mild OSA, if they can tolerate the device. The high percentage of dropouts and/or loss to follow-up suggests that redesign or modification of the TSD design may be necessary to improve patients’ adherence to therapy.
REFERENCES
2. Kirby T. Colin Sullivan: inventive pioneer of sleep medicine. Lancet 2011;377:485.
3. Kushida CA, Littner MR, Hirshkowitz M, et al.; American Academy of Sleep Medicine. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances: an update for 2005. Sleep 2006;29:240–3
4. Ferguson KA, Cartwright R, Rogers R, Schmidt-Nowara W. Oral appliances for snoring and obstructive sleep apnea: a review. Sleep 2006;29:244–62.
5. Cartwright RD, Samelson CF. The effects of a nonsurgical treatment for obstructive sleep apnea. The tongue-retaining device. JAMA 1982;13;248:705–9.
6. Dort L, Brant R. A randomized, controlled, crossover study of a noncustomized tongue retaining device for sleep disordered breathing. Sleep Breath 2008;12:369–73.
7. Lazard DS, Blumen M, Lévy P, et al. The tongue-retaining device: efficacy and side effects in obstructive sleep apnea syndrome. J Clin Sleep Med 2009;5:431–8.
8. Randerath WJ, Verbraecken J, Andreas S, et al.; European Respiratory Society task force on non-CPAP therapies in sleep apnoea. Non-CPAP therapies in obstructive sleep apnoea. Eur Respir J 2011;37:1000–28.
9. Deane SA, Cistulli PA, Ng AT, Zeng B, Petocz P, Darendeliler MA. Comparison of mandibular advancement splint and tongue stabilizing device in obstructive sleep apnea: a randomized controlled trial. Sleep 2009;32:648–53.
10. Sutherland K, Deane SA, Chan AS, et al. Comparative effects of two oral appliances on upper airway structure in obstructive sleep apnea. Sleep 2011;34:469–77.
11. Tsuiki S, Shiga T, Maeda K, Matsuzaki-Stromberger R, Inoue Y. A dentist’s role: prevention of snoring at temporary refuges for victims of the East Japan earthquake and the Fukushima Daiichi Nuclear Power Plant accident on March 11, 2011. Sleep Breath 2012;16:587–9.
12. Tsuiki S, Kobayashi M, Namba K, et al. Optimal positive airway pressure predicts oral appliance treatment response to sleep apnoea. Eur Respir J 2010;35:1098–105.
13. Fukuda T, Tsuiki S, Kobayashi M, Nakayama H, Inoue Y. Selection of response criteria affects the success rate of oral appliance treatment for obstructive sleep apnea. Sleep Med 2014;15:367–70.
14. Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. The report of an American Academy of Sleep Medicine Task Force. Sleep 1999;22:667–89.
15. Takegami M, Suzukamo Y, Wakita T, et al. Development of a Japanese version of the Epworth Sleepiness Scale (JESS) based on Item Response Theory. Sleep Med 2009;10:556–65.
16. Isono S, Remmers JE, Tanaka A, Sho Y, Sato J, Nishino T. Anatomy of pharynx in patients with obstructive sleep apnea and in normal subjects. J Appl Physiol 1997;82:1319–26.
17. Isono S, Tanaka A, Tagaito Y, Sho Y, Nishino T. Pharyngeal patency in response to advancement of the mandible in obese anesthetized persons. Anesthesiology 1997;87:1055–62.
18. Dort L, Remmers JE. A combination appliance for obstructive sleep apnea: the effectiveness of mandibular advancement and tongue retention. J Clin Sleep Med 2012;8:265–9.
19. Tsuiki S, Isono S, Minamino O, et al. Tongue position controller as an alternative treatment for obstructive sleep apnea. Sleep Breath 2012;16:957–60.
ACKNOWLEDGMENTS
The present study was supported in part by a Grant-in-Aid for Scientific Research (grant number 25515010, 15H05301) from the Japan Society for the Promotion of Science. The authors greatly thank Mr. Kazuyoshi Namba and Ms. Yuka Suzuki for their data analyses and telephone follow-up. We also thank Dr. Keiko Maeda for her sampling of patients.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication March, 2015
Submitted in final revised form January, 2016
Accepted for publication February, 2016
Address correspondence to: Satoru Tsuiki, DDS, PhD, Division of Dental Sleep Medicine, Japan Somnology Center, Institute of Neuropsychiatry, 1-24-10, Yoyogi, Shibuya-ku, Tokyo, Japan 151-0053; Tel: +81-3-3374- 9112; Fax: +81-3374-9125; Email: tsuiki@somnology.com
DISCLOSURE STATEMENT
This was not an industry supported study. This work was performed at the Institute of Neuropsychiatry and supported in part by a Grant-inAid for Scientific Research [grant number 25515010,15H05301] from the Japan Society for the Promotion of Science. The authors have indicated no financial conflicts of interest.
PDF