Original Article, Issue 3.1
Continuous Positive Airway Pressure and Oral Appliance Hybrid Therapy in Obstructive Sleep Apnea: Patient Comfort, Compliance, and Preference: A Pilot Study
http://dx.doi.org/10.15331/jdsm.5362
Grietje E. de Vries, MSc1,2; Michiel H.J. Doff, DMD, PhD3 ; Aarnoud Hoekema, MD, PhD3 ; Huib A.M. Kerstjens, MD, PhD1,2; Peter J. Wijkstra, MD, PhD1,2,4
1 University of Groningen, University Medical Center Groningen, Department of Pulmonary Medicine and Tuberculosis, Groningen, the Netherlands; 2University of Groningen, University Medical Center Groningen, GRIAC Research Institute, Groningen, the Netherlands; 3University of Groningen, University Medical Center Groningen, Department of Oral and Maxillofacial Surgery, Groningen, the Netherlands; 4University of Groningen, University Medical Center Groningen, Center for Home Mechanical Ventilation, Groningen, the Netherlands
ABSTRACT
Study Objectives:
Patients with obstructive sleep apnea syndrome (OSAS) using continuous positive airway pressure (CPAP) often report pressure-related discomfort. Both lower pressure and increased comfort may improve patients’ compliance with CPAPtherapy, thereby improving therapeutic effectiveness. Combining CPAP with an oral appliance (hybrid therapy) could be an adequate alternative therapy.
Methods:
Seven patients with moderate to severe OSAS who tolerated their CPAP despite high pressures (≥ 10 cm H2O) were fitted with hybrid therapy. The mandible was set at 70% of patient’s maximum protrusion, and CPAP pressure was set at 6 cm H2O. When OSAS complaints persisted, pressure was increased. After 3 months, a polysomnographic study was performed. At baseline (conventional CPAP) and after 3 months (hybrid therapy) patients filled in questionnaires assessing comfort, compliance, and satisfaction with treatment, excessive daytime sleepiness, and quality of life.
Results:
Four of seven patients reported hybrid therapy to be more comfortable and effective and preferred it over conventional CPAP. There were no differences between baseline (conventional CPAP) and follow-up (hybrid therapy) scores in compliance, satisfaction, daytime sleepiness, and quality of life. Effectiveness of hybrid therapy was good as apnea-hypopnea index (AHI) significantly decreased from median AHI 64.6/h (interquartile range [IQR] 31.0–81.0) at diagnosis to median AHI 1.5/h (IQR 1.0–33.4) with hybrid therapy. There was no statistical difference in effectiveness between conventional CPAP and hybrid therapy (median AHI with conventional CPAP was 2.4/h [IQR 0.0–5.0]).
Conclusions:
Although pressure could be lowered and hybrid therapy seems a comfortable alternative to conventional CPAP, there were no differences between both therapies regarding compliance, satisfaction, and both objective and experienced effectiveness. Combined therapy is feasible in OSAS and should now be investigated in a RCT including assessment of comfort and long-term compliance.
Keywords:
obstructive sleep apnea syndrome; continuous positive airway pressure; oral appliance; treatment
Citation:
de Vries GE, Doff MH, Hoekema A, Kerstjens HA, Wijkstra PJ. Continuous positive airway pressure and oral appliance hybrid therapy in obstructive sleep apnea: patient comfort, compliance, and preference: a pilot study. Journal of Dental Sleep Medicine 2016;3(1):5–10.
INTRODUCTION
Treatment with continuous positive airway pressure (CPAP) prevents upper airway collapse by pneumatically “splinting” the upper airway during sleep1 and is the most frequently prescribed treatment for OSAS.2 In severe OSAS (apneahypopnea index [AHI] > 30/h), it is the current standard of treatment and improves symptoms and quality of life as well as cardiovascular outcomes.2–4 Oral appliance therapy, however, has become an attractive alternative, especially in mild and moderate OSAS.5 Oral appliance therapy aims at relieving upper airway collapse during sleep by modifying the position of the mandible, tongue, and pharyngeal structures. Side effects have been reported to be mild, improve with time, and are mostly reversible.6–9
Patients with moderate to severe OSAS using CPAP often report pressure-related discomfort or intolerance. Other frequently mentioned complaints with the device are claustrophobia, comfort problems due to the mask or straps on the head, leakage, and dry eyes and nose. Discomfort can ultimately result in reduced therapeutic compliance.
Optimal compliance is essential for a therapy such as CPAP to be successful and effective. It is important to search for alternative treatment options that are equally effective to CPAP in the treatment of moderate to severe OSAS. Combining CPAP with an oral appliance could be such an alternative therapy (hybrid therapy). By combining both therapies, CPAP pressure may be lowered substantially as an oral appliance increases upper airway patency. Second, the CPAP nose mask can be fixed onto the oral appliance, which could improve the comfort of the treatment (no headstrap required, no shifting of the hose/tube). Both lower pressure and increased comfort may improve patients’ compliance with therapy, thereby improving therapeutic effectiveness.
To date, only two case reports10,11 and one pilot study,12 reporting on the simultaneous use of CPAP and oral appliance therapy in OSAS, have been published. These studies included only patients intolerant to CPAP, and in two studies10,12 patients were ineffectively treated with an oral appliance. Furthermore, the studies provide insufficient information about comfort and compliance. In one other case report, the use of an oral appliance in combination with noninvasive ventilation in a patient with amyotrophic lateral sclerosis was described.13
The aim of this study was to evaluate whether hybrid therapy is an adequate alternative to conventional CPAP in moderate to severe OSAS. For this study, patients being effectively treated with conventional CPAP and who did tolerate their CPAP and were satisfied with it, despite relative high therapeutic pressures (i.e., > 10 cm H2O) were selected. Primary outcomes were comfort and compliance with hybrid therapy. Secondary outcomes were effectiveness of hybrid therapy and the effect of this treatment on quality of life.
METHODS
Subjects
Patients were eligible for the study when they: (1) were diagnosed with moderate to severe OSAS (apnea-hypopnea index (AHI) ≥ 15/h) during overnight poly(somno)graphy, (2) used conventional CPAP with pressure ≥ 10 cm H2O and could tolerate this pressure, (3) were aged > 18 years.
Exclusion criteria were (1) previously treated with an oral appliance, (2) dental contra-indications for oral appliance therapy (i.e., extensive periodontal disease or tooth decay, active temporomandibular joint disease [including severe bruxism], restrictions in mouth opening [< 25 mm] or advancement of the mandible [< 5 mm], partial or complete edentulism [< 8 teeth in upper or lower jaw]),5 (3) morphologic abnormalities of the upper airway, (4) current untreated endocrine dysfunction, (5) reported or documented severe cardiac or pulmonary comorbidity, and (6) patients being treated for psychiatric disorders at the moment of inclusion for the study.
Patients were considered effectively treated with conventional CPAP when AHI reduced to < 5/h or reduced ≥ 50% from the diagnostic value to an absolute value < 20/h5 (confirmed by poly(somno)graphic evaluation), or when subjective obstructive sleep apnea symptoms were absent and CPAP machine software readout showed sufficient suppression of AHI (therefore in the latter category of patients no poly(somno)graphic evaluation had been performed).
Study Design
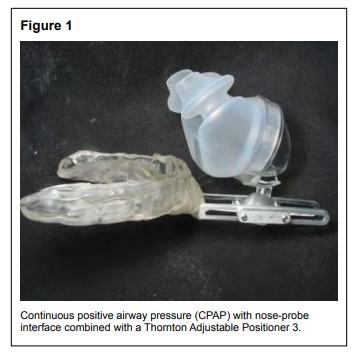
This study is a longitudinal quantitative as well as a qualitative study without a control group. The oral appliance (Thornton Adjustable Positioner [TAP3, Airway Management Inc., Dallas, TX, USA]) was custom-made for each patient. The Thornton Adjustable Positioner is an oral appliance that consist of 2 separate parts for both the maxilla and the mandible. The mandibular protrusion can be adjusted with 0.2-mm increments with a propulsion screw, which was incorporated anteriorly in the oral appliance. The maximum range of mandibular protrusion was first determined with a George-Gauge (H-Orthodontics, Michigan City, IN, USA). When initiating oral appliance therapy, the mandible was set at 70% of the patient’s maximum protrusion or at 60% when 70% was uncomfortable to the patient.
After adjusting the oral appliance, nose-probes from a CPAP interface were attached to the oral appliance by means of a connection-unit (Figure 1). No headstraps were used for hybrid therapy.
Figure 1Continuous positive airway pressure (CPAP) with nose-probe interface combined with a Thornton Adjustable Positioner 3. |
{kind=link}
When starting with hybrid therapy CPAP pressure was set at 6 cm H2O for all patients. After an adjustment period of about 2–4 weeks, the degree of mandibular protrusion or CPAP pressure was adjusted if necessary, based on patients’ reported symptoms, until the desired effectiveness had been reached or until the adjustments became uncomfortable to the patient. Whether the degree of mandibular protrusion or CPAP-pressure had to be adjusted was decided in accordance with the patient. There was, however, not a strict adjustment protocol.
After 3 months of hybrid therapy, current CPAP pressure was assessed and effectiveness of the therapy was measured with home-based polysomnography. Furthermore, patients were asked about their treatment preference regarding comfort, efficacy, and satisfaction when comparing hybrid therapy with conventional CPAP therapy.
At baseline (conventional CPAP) and after 3 months (hybrid therapy) patients filled in questionnaires assessing comfort of, and compliance and satisfaction with their current treatment, excessive daytime sleepiness (Epworth Sleepiness Scale (ESS),14 quality of life (Short-Form 36-item Health Survey (SF-36),15 and Functional Outcomes of Sleep Questionnaire (FOSQ),16 and anxiety and depressive feelings (Hospital Anxiety and Depression Scale (HADS).17
The study was approved by the local Ethical Committee (METc University Medical Center Groningen; METc2010/051). All patients gave written informed consent for using their data for this study and publication before inclusion.
Measurements
Polysomnography
Polysomnographic overnight home-based evaluations (Vitaport-4 PSG, Temec Instruments BV, Kerkrade, the Netherlands) were used to diagnose OSAS and to assess the effect of the hybrid therapy at follow-up. Sleep stages were measured with surface electroencephalography, left and right electrooculography, and submental electromyography. Oxygen saturation was recorded with pulse oximetry. Oronasal airflow was recorded with a pressure cannula. Respiratory effort was monitored with thoracic and abdominal strain bands. Apnea was defined as a complete obstruction resulting in a cessation in airflow (i.e., reduction of airflow ≥ 90%) ≥ 10 seconds. Hypopnea was defined as a substantial (i.e., ≥ 30%) reduction in airflow ≥ 10 seconds when associated with oxygen desaturation (≥ 4%).18
Compliance, Satisfaction, and Preference
The number of nights per week and hours per night using therapy were assessed through a self-report questionnaire. Satisfaction with the current therapy was assessed with a visual analog scale of 0–100 mm without anchors. Patients were asked to draw a vertical line crossing the horizontal scale. After 3 months, patients were asked to indicate whether they preferred conventional CPAP or hybrid therapy based on satisfaction with therapy, long-term use, comfort, and effectiveness, (i.e., the experience that the device is effective in reducing sleep apnea symptoms).
Comfort
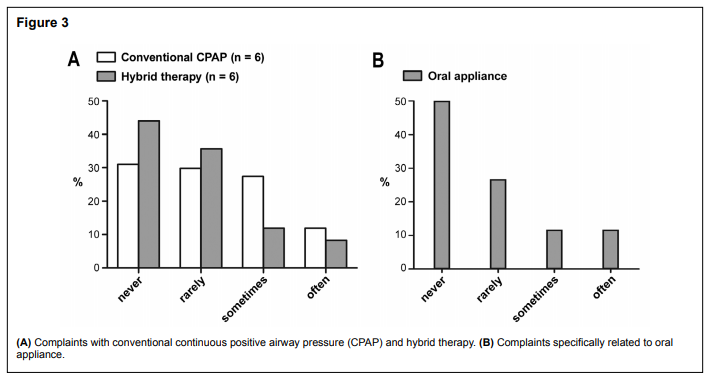
Complaints with conventional CPAP (e.g., irritation of CPAP mask; leakage; dry eyes; claustrophobia), oral appliance (e.g., tooth or molar pain; painful jaws, joint, muscles), and the combination of both therapies (hybrid therapy) (e.g., hindered by therapy when falling asleep; awakened by poorly fitted or lose equipment) were assessed through a self-report questionnaire. Patients scored how frequently they experienced a specific complaint on a 4-point scale, ranging from never to often (0–3).
Data Analysis
Descriptive statistics are presented as means ± standard deviations or medians and interquartile ranges (IQR) for continuous variables. Categorical variables are presented in terms of proportions. Wilcoxon signed-rank tests were performed to assess the difference between measurements at baseline and after 3 months. Data were analyzed with SPSS 20.0 statistical software. A value of p < 0.05 was considered statistically significant.
RESULTS
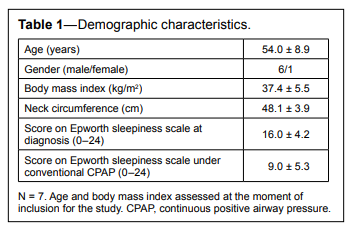
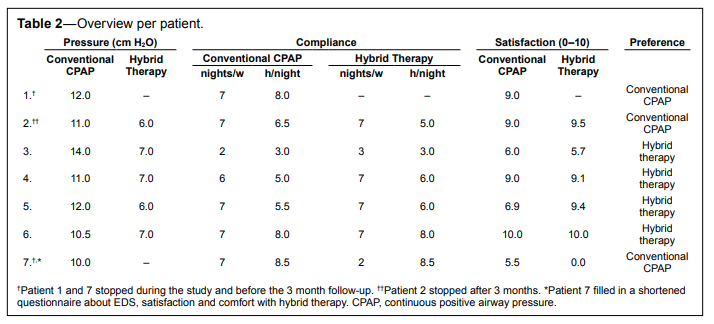
Seven patients (6 men) participated (mean ± SD age 54 ± 8.9 years). Table 1 contains the demographic characteristics of the patients at baseline. Pressure could be lowered from 11.5 ± 1.3 cm H2O with CPAP to 6.4 ± 0.5 cm H2O with hybrid therapy. Three patients had their pressure increased from 6 cm H2O to 7 cm H2O during the follow-up period on hybrid therapy. In 4 patients, the degree of mandibular protrusion was increased from 60% to 70% of the patient’s maximum protrusion (of whom 2 patients also had their pressure increased from 6 cm H2O to 7 cm H2O).
Table 1Demographic characteristics. |
{kind=link}
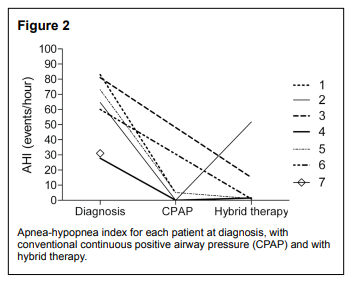
Five patients used hybrid therapy for the full 3 months, of whom one stopped after the study period. Two patients could not cope with the hybrid therapy and stopped before the 3-month endpoint. Four patients preferred hybrid therapy on the long term over conventional CPAP and also reported hybrid therapy as more comfortable and effective, (i.e., the experience that the device is effective in reducing sleep apnea symptoms) than conventional CPAP. The reasons to stop were feelings of dyspnea and anxiety, and being very restless during sleep due to the therapy and having specific oral appliance related complaints which were indicated as frequently occurring (tooth or molar pain, feeling that teeth are “out of place” in the morning, painful jaws, joints and chewing muscles). The patient who stopped after the study could not get used to hybrid therapy (claustrophobia), and hybrid therapy was not effective in this patient (AHI at follow-up of 51.8/h, Figure 2).
Figure 2Apnea-hypopnea index for each patient at diagnosis, with conventional continuous positive airway pressure (CPAP) and with hybrid therapy. |
{kind=link}
There were no differences in compliance between conventional CPAP (median 7.0 nights/week [IQR 6.0–7.0]); 6.5 h/ night [IQR 5.0–8.0]) and hybrid therapy (median 7.0 nights/ week [IQR 2.8–7.0]); 6.0 h/night [IQR 4.5–8.1]), both p = 1.0. Satisfaction rates on the visual analog scale did not differ between conventional CPAP (median 90.0 [IQR 60.0–90.0]) and hybrid therapy (median 92.5 [IQR 42.8–96.3]), p = 0.89. Nevertheless, when explicitly asked to make a choice between both treatment modalities, 4 of 7 patients reported to be more satisfied with hybrid therapy (Table 2).
Table 2Overview per patient. |
{kind=link}
AHI decreased significantly with hybrid therapy (median AHI 1.5/h [IQR 1.0–33.4]) compared to AHI at diagnosis (median AHI 64.6/h [IQR 31.0–81.0]), p < 0.05. There was no statistical difference in effectiveness between conventional CPAP and hybrid therapy (median AHI with conventional CPAP was 2.4/h [IQR 0.0–5.0]).
Scores on the Epworth sleepiness scale dropped from 10.3 ± 4.4 (n = 6) at baseline with conventional CPAP to 9.2 ± 6.2 with hybrid therapy (p = 0.68). Quality of life, measured with the FOSQ, increased from 15.9 ± 3.2 (n = 5) with conventional CPAP to 16.3 ± 3.6 with hybrid therapy (p = 0.79). The physical subscale of the SF-36 increased from 50.9 ± 8.7 (n = 5) with conventional CPAP to 51.4 ± 6.2 with hybrid therapy (p = 0.73) and the mental subscale of the SF-36 increased from 42.7 ± 17.2 with conventional CPAP to 47.5 ± 16.3 with hybrid therapy (p = 0.41). Anxiety and depressive feelings, measured with the HADS, dropped from 12.4 ± 12.6 (n = 5) with conventional CPAP to 8.0 ± 9.0 with hybrid therapy (p = 0.16). All results were in the desired direction, but none of the differences were statistically significant.
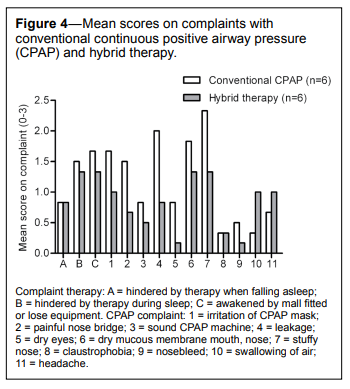
Six patients filled in the self-report questionnaire on complaints both at baseline (conventional CPAP) and at follow-up (hybrid therapy). Figure 3 displays the percentages of reported complaints for both therapies per category (calculated as the actual number of reported side effects or complaints for that category divided by the maximum expected number of reported complaints, i.e., the situation when all patients would have scored the same category). Mean scores per (specific) complaint were calculated in order to compare complaints for conventional CPAP with hybrid therapy (Figure 4).
Figure 3 |
{kind=link}
Figure 4Mean scores on complaints with conventional continuous positive airway pressure (CPAP) and hybrid therapy. |
{kind=link}
Patients had fewer CPAP complaints in combination with the oral appliance (hybrid therapy) than with conventional CPAP alone (Figure 3A). Specific oral appliance related complaints were reported as not frequently occurring (Figure 3B). Most complaints with conventional CPAP, such as stuffy nose, irritation of the mask, painful nose bridge, leakage, dry eyes, dry mucous membrane mouth and nose became less of a problem when using hybrid therapy, while the swallowing of air, and the presence of a headache appeared to increase slightly with hybrid therapy (Figure 4). When patients had to indicate the severity of their complaints on a scale of mild to severe, most complaints with conventional CPAP were indicated as mild (once absent, 5 times mild, and once moderate). Complaints with hybrid therapy were also indicated as mild most of the times (once absent, 3 times mild, once moderate, and once severe).
DISCUSSION
This study showed that CPAP – oral appliance hybrid therapy could be a comfortable and effective alternative to conventional CPAP in many but not all patients with moderate to severe OSAS. Patients were equally compliant with hybrid therapy and conventional CPAP.
Pressure could be lowered from 11.5 ± 1.3 cm H2O with conventional CPAP to 6.4 ± 0.5 cm H2O with hybrid therapy. In addition complaints were less frequently mentioned with hybrid therapy when compared with conventional CPAP.
The case reports by Denbar10 and Upadhyay et al.11 and the pilot study by El-Solh et al.12 showed similar positive effects on therapeutic CPAP pressure and AHI reduction. Both studies, however, have some limitations. Patients in the study by El-Solh et al.12 used the combination therapy for only 3 days. Furthermore, the only patients selected were intolerant of CPAP and were ineffectively treated with an oral appliance. No overnight sleep study was performed at the end. The study of Denbar10 describes the treatment of one patient over a time period of 4.5 years, of which the last 1.5 years consisted of hybrid therapy. Both conventional CPAP and an oral appliance therapy were unsuccessful for this specific patient. Upadhyay et al.11 describe the treatment of one patient, who was intolerant of CPAP and was declared unfit for uvulopalatopharyngoplasty. The study describes a treatment period of 90 days during which the patient lost 9 kilograms in weight, which could have amplified the positive study results.
It is plausible that ineffectively treated patients or patients who regard their current treatment as uncomfortable are more eager to start, and are more satisfied with a new therapeutic modality. In order to avoid this bias we selected patients who did tolerate their CPAP and were satisfied with it, despite relative high therapeutic pressures (i.e., > 10 cm H2O). Including only patients who tolerate their CPAP therapy raises another possible bias, as those patients might tend to prefer the therapy they know. Our results show however that four patients preferred hybrid therapy over the long term over conventional CPAP.
Pressure could be lowered in all patients (mean 11.5 ± 1.3 cm H2O with conventional CPAP to mean 6.4 ± 0.5 cm H2O with hybrid therapy). Pressure was not again titrated before the start of this study. It is therefore possible that the conventional CPAP was not at the minimum efficient pressure as the CPAP pressure was the pressure patients were on before the period with hybrid therapy started. The conventional CPAP pressure was, however, increased until OSAS complaints were no longer present and the sleep study, or CPAP machine software readout showed sufficient suppression of the AHI. A lower efficient pressure is therefore not very likely.
Complaints were indicated as not frequently occurring for conventional CPAP as well as for hybrid therapy. Patients reported less specific CPAP complaints with hybrid therapy than with conventional CPAP, suggesting higher comfort with the hybrid therapy.
Our theory that lower pressure and better comfort could result in a better therapeutic compliance was not confirmed by our data. Moreover, satisfaction scores on the visual analog scale were similar. However, when forced to make a choice for one of the two treatments, four of seven patients preferred hybrid therapy over conventional CPAP. They reported hybrid therapy as more comfortable and effective. These patients continued using the hybrid therapy after completion of the study. Unfortunately, due to the small sample size, no statistics could be applied to assess whether complaints were significantly less with hybrid therapy than with conventional CPAP.
In our study, one patient had his AHI worsened using hybrid therapy. A possible explanation for this could be that this patient had gained weight compared to the time when the OSAS was diagnosed and also when compared to baseline (137 kg with hybrid therapy compared to 123 kg with conventional CPAP).
There are some other limitations to consider for this study. Unfortunately, we did not have polysomnographic data for all patients while using conventional CPAP, making a good comparison on objective effectiveness between conventional CPAP and hybrid therapy difficult. Four patients had polysomnography performed with both treatment modalities; the other three patients reported no subjective obstructive sleep apnea symptoms, and CPAP machine software readout showed sufficient suppression of AHI. Therefore, no follow-up poly(somno) graphic evaluation was indicated at that moment.
During the study period the degree of mandibular protrusion or CPAP pressure was adjusted when necessary. There was, however, not a strict protocol regarding which one to perform first. To date, there are no data to substantiate which approach is best in titrating hybrid therapy. This should be a point of attention in future studies assessing hybrid therapy.
The results of our study should be interpreted with caution, as this study consists only of a small patient sample and because there was no control group. Furthermore, a follow-up of 3 months may be too short to reveal effects on quality of life data.
CONCLUSIONS
In conclusion, although pressure could be lowered substantially, this pilot study did not show large differences between conventional CPAP and hybrid therapy regarding compliance, satisfaction, and both objective and experienced effectiveness. There are, however, some differences in scores on CPAP complaints, which could explain why hybrid therapy is preferred by four of the seven patients. Therefore, CPAP – oral appliance hybrid therapy could be a comfortable and effective alternative to conventional CPAP when high pressure is needed or in case of high pressure intolerance. Larger, longer term, and preferably randomized studies are needed to answer the question whether hybrid therapy can result in lower pressures leading to a more comfortable and effective treatment for patients with moderate to severe OSAS.
ABBREVIATIONS
AHI, apnea-hypopnea index
CPAP, continuous positive airway pressure
IQR, interquartile range
OSAS, obstructive sleep apnea syndrome
REFERENCES
2. Giles TL, Lasserson TJ, Smith BH, White J, Wright J, Cates CJ. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst Rev 2006;3:CD001106.
3. Diamanti C, Manali E, Ginieri-Coccossis M, et al. Depression, physical activity, energy consumption, and quality of life in OSA patients before and after CPAP treatment. Sleep Breath 2013;17:1159–68.
4. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 2005;365:1046–53.
5. Hoekema A, Stegenga B, Wijkstra PJ, van der Hoeven JH, Meinesz AF, de Bont LG. Obstructive sleep apnea therapy. J Dent Res 2008;87:882–7.
6. Ferguson KA, Ono T, Lowe AA, al Majed S, Love LL, Fleetham JA. A short-term controlled trial of an adjustable oral appliance for the treatment of mild to moderate obstructive sleep apnoea. Thorax 1997;52:362–8.
7. Doff MH, Veldhuis SK, Hoekema A, et al. Long-term oral appliance therapy in obstructive sleep apnea syndrome: a controlled study on temporomandibular side effects. Clin Oral Investig 2012;16:689–97.
8. Doff MH, Finnema KJ, Hoekema A, Wijkstra PJ, de Bont LG, Stegenga B. Long-term oral appliance therapy in obstructive sleep apnea syndrome: a controlled study on dental side effects. Clin Oral Investig 2013;17:475–82.
9. Fritsch KM, Iseli A, Russi EW, Bloch KE. Side effects of mandibular advancement devices for sleep apnea treatment. Am J Respir Crit Care Med 2001;164:813–8.
10. Denbar MA. A case study involving the combination treatment of an oral appliance and auto-titrating CPAP unit. Sleep Breath 2002;6:125–8.
11. Upadhyay R, Dubey A, Kant S, Singh BP. Management of severe obstructive sleep apnea using mandibular advancement devices with auto continuous positive airway pressures. Lung India 2015;32:158–61.
12. El-Solh AA, Moitheennazima B, Akinnusi ME, Churder PM, Lafornara AM. Combined oral appliance and positive airway pressure therapy for obstructive sleep apnea: a pilot study. Sleep Breath 2011;15:203–8.
13. Veldhuis SK, Doff MH, Stegenga B, Nieuwenhuis JA, Wijkstra PJ. Oral appliance to assist non-invasive ventilation in a patient with amyotrophic lateral sclerosis. Sleep Breath 2015;19:61–3.
14. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep 1991;14:540–5.
15. Ware JE Jr., Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992;30:473–83.
16. Weaver TE, Laizner AM, Evans LK, et al. An instrument to measure functional status outcomes for disorders of excessive sleepiness. Sleep 1997;20:835–43.
17. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983;67:361–70.
18. Iber C, Ancoli-Israel S, Chesson AL, Quan SF; for the American Academy of Sleep Medicine. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications, 1st ed. Westchester, IL: American Academy of Sleep Medicine, 2007.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication July, 2015
Submitted in final revised form September, 2015
Accepted for publication October, 2015 Address correspondence to: Grietje de Vries, MSc, University of Groningen, University Medical Center Groningen, Department of Pulmonary Medicine and Tuberculosis AA11, Hanzeplein 1, PO Box 30.001, 9700 RB Groningen, the Netherlands; Tel: +31 50 3619195; Email: g.e.de.vries@umcg.nl
DISCLOSURE STATEMENT
This was not an industry supported study. Dr. Hoekema has received research support from SomnoMed Goedegebuure. Dr. Wijkstra has received research support from Philips/Respironics, ResMed, Vivisol, and Air Liquide and has participated in speaking engagements for Philips/ Respironics, and Vivisol. The other authors have indicated no financial conflicts of interest.
PDF