Original Article 4, Issue 8.1
Adherence of Mandibular Advancement Device for Obstructive Sleep Apnea in a Veteran Population
http://dx.doi.org/10.15331/jdsm.7176Harmeet K. Chiang, BDS, DDS, MS, FAGD1; John L. Smith, MS2; Elsa V. Mathew, MD3,5; Leslee E. Hudgins, DO3,5; Al M. Best, PhD6; Antony Fernandez, MD4,5
1 Associate Professor, School of Dentistry, Virginia Commonwealth University, Richmond, Virginia, USA; 2 Student, School of Dentistry, Virginia Commonwealth University, Richmond, Virginia, USA; 3 Assistant Professor of Neurology, Virginia Commonwealth University, Richmond, Virginia, USA; 4Professor of Psychiatry & Neurology, Virginia Commonwealth University, Richmond, Virginia, USA; 5Physician, Integrated Sleep Disorders Center, McGuire Veterans Affairs Medical Center, Richmond, Virginia, USA; 6 Emeritus Professor, School of Dentistry, Virginia Commonwealth University, Richmond, Virginia, USA;
ABSTRACT
Study Objectives:
To determine the adherence rate of a custom-fit mandibular advancement device (MAD), and the factors that may affect this adherence within a veteran population with obstructive sleep apnea (OSA).
Methods:
This is a retrospective chart review on veteran patient adherence for the treatment for OSA. Adherence was defined as wearing the MAD for at least 4 hours per night and for at least 70% of that time. Patients ranged from having mild to severe OSA and many were not compliant with continuous positive airway pressure (CPAP) usage. A DentiTrac® microrecorder (Braebon, https://www.braebon.com/products/dentitrac/, Ontario, Canada) was embedded within each MAD to record patient compliance. Compliance data were recorded at days 14, 30, and 90. Patient demographic and clinical characteristics were reviewed to identify additional factors affecting adherence.
Results:
The 57 subjects had an average age of 54.6 years, body mass index 30.7 kg/m2, and average apnea-hypopnea index (AHI) before treatment of 15.3 events per hour. Adherence was at 72% after 14 days (95% confidence interval = 64% to 80%), 67% at 30 days (95% confidence interval = 59% to 77%) and 63% at 90 days (55% to 72%). A repeated-measures mixed model indicated that pretreatment AHI was negatively related to the 14-day, 30-day, and 90-day adherence percentages (P = 0.025).
Conclusions:
The MAD should be considered a valuable first-line treatment option for mild or moderate OSA in the veteran population, although maintaining adherence across time seems to be a challenge. It appears that MAD adherence may be superior to CPAP adherence in this population.
Keywords:
adherence; apnea-hypopnea index; compliance; mandibular advancement device; microrecorder; obstructive sleep apnea; veterans; oral appliance therapy
Citation:
Chiang HK, Smith JL, Matthew EV, Hudgins LE, Best AM, Fernandez A. Adherence of mandibular advancement device for obstructive sleep apnea in a veteran population. J Dent Sleep Med. 2021;8(1)
INTRODUCTION
Obstructive sleep apnea (OSA) is a repetitive collapse of the upper airway during sleep. This disorder is described as ranging from obstructive apneas, hypopneas, and/or respiratory effort-related arousals.1 OSA is the most common sleep-related breathing disorder.1 It is estimated that one billion people worldwide have OSA in some form. Of that total, treatment is needed for 454 million people who have moderate to severe OSA.2 If left untreated, OSA can result in increased risk of excessive daytime sleepiness, decrease in cognitive function, hypertension, cardiovascular disease, and in severe cases, death.3,4 Treatments range from behavioral, nonsurgical, surgical, and or a combination of these. The first-line nonsurgical treatment is fixed continuous positive airway pressure (CPAP) and its effectiveness is well established.5,6 However, adherence is believed to be on average less than 50%, with different studies reporting adherence ranging from 17% to 71%. Adherence has been established as the usage of the CPAP machine for a minimum of 4 hours in a 24-hour period for 70% of use.7,8 Adherence for a mandibular advancement device (MAD) is defined in the same way. In the veteran population, when good adherence was defined as use of CPAP on 3 or more nights per week, only 39% to 53% of patients with mild to severe OSA maintained good adherence.9 Randomized controlled trials have shown that oral appliances are a good alternative because of their low cost, relative comfort, and ease of use, which results in greater patient adherence.9-11 Traditionally, adherence for oral appliances is self-reported by the patient but more objective measurements can now be reported with radiofrequency identification, tooth microphones, or different microsensors.
The primary aim of the study was to determine the adherence rate of a custom-fit MAD within a veteran population with OSA and, secondarily, to describe factors that may affect adherence.
METHODS
This is a retrospective chart review on patients of the McGuire Veterans Affairs Medical Center: Integrated Sleep Disorders Center receiving a custom-fit MAD for the treatment for OSA from November 2016 to September 2017. Patients were eligible for use of the MAD according to the Veteran Affairs criteria: mild to moderate OSA, or moderate to severe OSA after failed CPAP, or in conjunction with other modalities. Each MAD appliance had a DentiTrac® microrecorder embedded within the device. Compliance data were uploaded from the DentiTrac® base station. Daily adherence was defined as the percentage of days wearing the MAD for at least 4 hours. Patient adherence was defined as daily adherence of at least 70% (yes or no). Adherence was calculated at day 14, day 30, and day 90 of wearing the MAD. The fit of the MAD was assessed after 14 days as well as adherence data from the microrecorder. Patient demographic and clinical characteristics were reviewed to determine factors affecting adherence. Fifty-seven patients received a custom-made MAD and were thus eligible for the study. Statistical analysis used a modified intent-to-treat protocol. The modification was that all patients with data at each of the follow-up occasions were analyzed. That is, 54 patients had data at 14 days, 48 at 30 days, and 35 at 90 days.
RESULTS
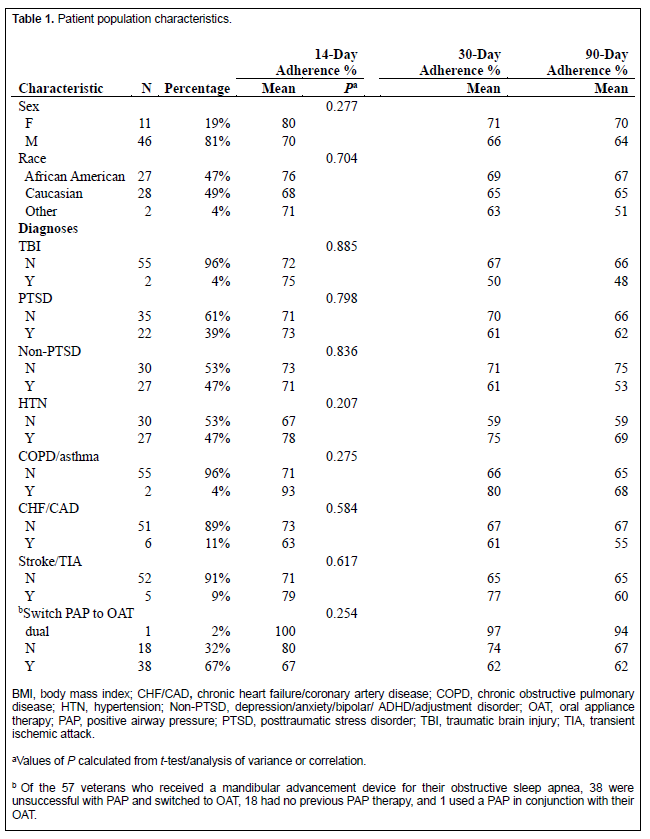
The 57 subjects (Table 1) had an average age of 54.6 years, body mass index 30.7 kg/m2, and an average before-treatment apnea-hypopnea index (AHI) of 15.3 events per hour. After 14 days 65% of the patients were adherent, and at 30 days 56% were adherent, and at 90 days 50% were adherent.
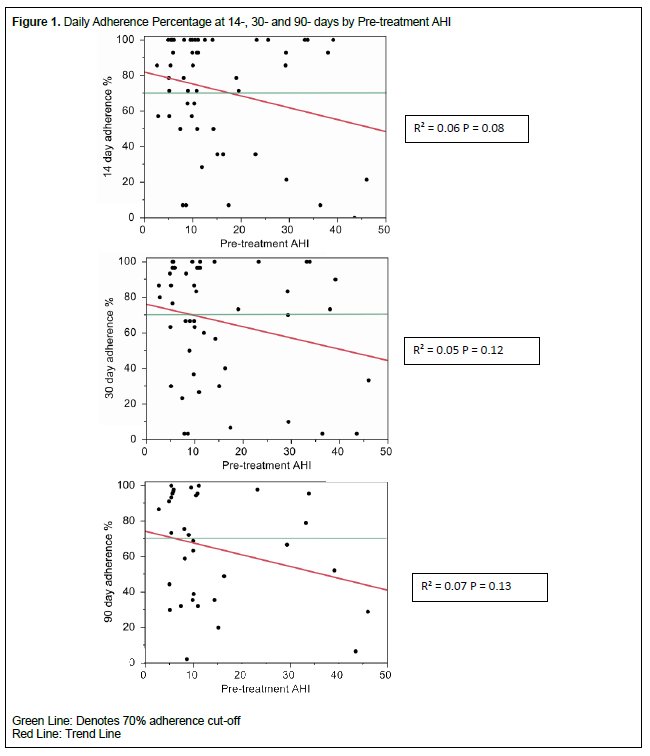
Each of the predictors in Table 1 were screened along with age, body mass index, and pretreatment AHI to determine which may be related to the 14-day adherence percentage. None passed a screening significance level of alpha= 0.20 except pretreatment AHI. Figure 1 shows scatterplots for the trend at each time point.
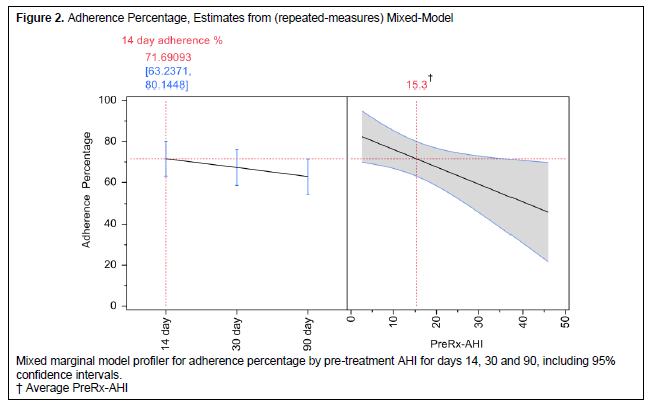
A repeated-measures mixed model indicated two things: (1) Pre-treatment AHI was negatively related to the 14-day, 30-day, and 90-day adherence percentages (P = 0.025). That is, the higher the AHI the lower the adherence. (2) Adherence percentage showed a nominal decline across the three time periods (P = 0.17). At the 14-day recall, the adherence percentage was 72% (95% confidence interval 63% to 80%), and by the 90-day recall adherence was 63% (95% confidence interval = 54% to 72%) Figure 2 and Table 2.
Figure 1Daily Adherence Percentage at 14-, 30- and 90- days by Pre-treatment AHI |
{kind=link}
Figure 2Adherence Percentage, Estimates from (repeated-measures) Mixed-Model |
{kind=link}
Table 1Patient population characteristics. |
{kind=link}
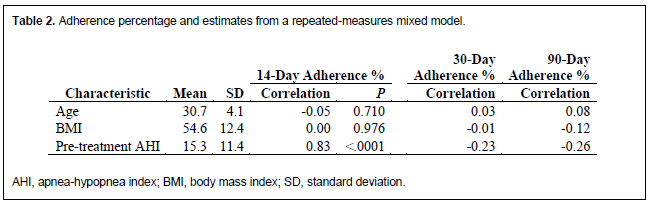
Table 2Adherence percentage and estimates from a repeated-measures mixed model. |
{kind=link}
DISCUSSION
Self-reporting was the main way that patient adherence was recorded for oral appliances. Technology has allowed for the placement of adherence tracking devices into an oral device. The inclusion of objective tracking of these devices can now provide a true adherence percentage. Oral appliance therapy with the MAD should be considered a valuable first-line treatment option for mild to moderate OSA in the veteran population, and with objective adherence reporting, OSA care for veterans can be better understood for providers. The efficacy of CPAP has been endorsed across many studies, when used properly and with good adherence.1-6, 12-23 Unfortunately, the adherence rates of CPAP are generally considered to be at approximately 50%.19 Because of the increased adherence, decreased cost, ease of use, and portability custom fit MADs should be considered a first-line treatment for OSA. Even with the ultimate need for a CPAP, a custom MAD would allow the patient to have an additional treatment option for OSA when CPAP adherence is not possible. A similar study with a veteran population reported adherence with custom MADs at 66.8% and 58.3% for the 2-week and 6-month recalls, respectively.24 These results were on par with the findings of this study. Socioeconomic challenges and lack of a support system increase the lack of adherence within the veteran population.24 These challenges could be a reason for the slight decrease in adherence between veteran and general population studies.
Previous studies have indicated that AHI was a strong predictor of long-term CPAP adherence.25-27 Patients with a higher AHI were more likely to adhere to long-term CPAP usage compared with patients with lower AHI. 25-27 Studies using oral appliances did not find a link between adherence and severity of OSA.28 However, a statistical association was seen between increased baseline AHI and lower adherence percentages. The higher the baseline AHI, the lower the adherence rates (P = 0.025). The current study did not find any significant association of adherence to PTSD or other comorbidities within the veteran population. This contradicts some theories linking the two.26
The use of CPAP is seen to be more effective than MADs in controlling OSA. However,10% to 50% of the patients who are prescribed a CPAP find it intolerable to use and therefore use an alternative treatment option. The remaining patients that do use CPAP have an adherence rate of approximately 50%.19,20 When patients were able to use both oral appliance therapy and CPAP, most patients preferred the oral device over the CPAP.11,21 The increase in adherence with MADs over CPAP allows for the overall effectiveness of MADs to be the same, if not better, in controlling OSA.23 Oral devices have been seen to decrease nighttime diastolic blood pressure. A significant decrease was observed when the oral device was compared to CPAP (P<0.05), placebo (P<0.05), and baseline (P<0.01).29 Patients with positional apnea would also benefit from a MAD because on average the supine position is more susceptible to OSA.22
There are limitations to the current study. Although every attempt was made to measure adherence at every time point, the missing patient follow-up data could result in overstating adherence.
Custom MADs should be considered a valuable first-line treatment option for mild or moderate OSA in the veteran population. Long-term maintenance of adherence is still a challenge that needs to be improved. However, adherence using MAD may be superior to that of CPAP in this population.
ACKNOWLEDGMENTS
A special thanks to Shekar Raman, MD and Edmund Cornman, MD.
ABBREVIATIONS
AHI: apnea-hypopnea index
CPAP: continuous positive airway pressure
MAD: mandibular advancement device
OSA: obstructive sleep apnea
REFERENCES
- Kline LR. Clinical presentation and diagnosis of obstructive sleep apnea in adults. UpToDate. Retrieved March 18, 2020, from https://www.uptodate.com/contents/clinical-presentation-and-diagnosis-of-obstructive-sleep-apnea-in-adults
- Benjafield AV, Ayas NT, Eastwood PR, Heinzer R, Ip MSM, Morrell MJ. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7:687–698.
- Morsy N, Farrag NS, Zaki NFW, et al. Obstructive sleep apnea: personal, societal, public health, and legal implications. Rev Environ Health. 2019;34(2):153-169.
- Knauert M, Naik S, Gillespie MB, Kryger M. Clinical consequences and economic costs of untreated obstructive sleep apnea syndrome. World J Otorhinolaryngol Head Neck Surg. 2015;1(1):17-27.
- Epstein LJ, Kristo D, Strollo PJ Jr, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(3):263–276.
- Brown LK, Lee W. Initiation of positive airway pressure therapy for obstructive sleep apnea in adults. UpToDate. Retrieved March 18, 2020, from https://www.uptodate.com/contents/initiation-of-positive-airway-pressure-therapy-for-obstructive-sleep-apnea-in-adults
- Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc. 2008;5(2):173–178.
- Weaver, T. Adherence with continuous positive airway pressure (CPAP). UpToDate. Retrieved March 18, 2020, from https://www.uptodate.com/contents/adherence-with-continuous-positive-airway-pressure-cpap
- Samson P, Casey KR, Knepler J, Panos RJ. Clinical characteristics, comorbidities, and response to treatment of veterans with obstructive sleep apnea, Cincinnati Veterans Affairs Medical Center, 2005-2007. Prev Chronic Dis. 2012;9:E46.
- Ahrens A, McGrath C, Hägg U. A systematic review of the efficacy of oral appliance design in the management of obstructive sleep apnoea. Eur J Orthod. 2011;33(3):318–324.
- Ferguson KA, Ono T, Lowe AA, Keenan SP, Fleetham JA. A randomized crossover study of an oral appliance vs nasal-continuous positive airway pressure in the treatment of mild-moderate obstructive sleep apnea. Chest. 1996;109(5):1269–1275.
- Kryger, MH, Malhotra, A. Management of obstructive sleep apnea in adults. UpToDate. Retrieved March 18, 2020, from https://www.uptodate.com/contents/management-of-obstructive-sleep-apnea-in-adults
- Schwartz M, Acosta L, Hung Y-L, Padilla M, Enciso R. Effects of CPAP and mandibular advancement device treatment in obstructive sleep apnea patients: a systematic review and meta-analysis. Sleep Breath. 2017;22(3):555-568.
- Lee WH, Kwon SO, Kim J-W. Effectiveness of sleep surgery versus a mandibular advancement device for obstructive sleep apnea in terms of nocturnal cardiac autonomic activity. Sleep Breath. 2020; 24(4):1695-1703.
- Martins ODFM, Junior CMC, Rossi RRP, Cunali PA, Dal-Fabbro C, Bittencourt L. Side effects of mandibular advancement splints for the treatment of snoring and obstructive sleep apnea: a systematic review. Dent Press J Orthod. 2018;23(4):45-54. doi:10.1590/2177-6709.23.4.045-054.oar.
- Milano F, Billi M, Gobbi R, Gracco A, Sorrenti G. The impact of a multidisciplinary approach on response rate of mandibular advancing device therapy in patients with obstructive sleep apnoea syndrome. Acta Otorhinolaryngol Ital. 2013;33(5):337-342.
- Pitarch RM, García MS, Cuesta JP, Algarra JM, Julian EF, Font AF. Effectiveness of a mandibular advancement device in obstructive sleep apnea patients: a prospective clinical trial. Eur Arch Otorhinolaryngol. 2018;275(7):1903-1911.
- Aronson JK. Compliance, concordance, adherence. Br J Clin Pharmacol. 2007;63(4):383–384.
- Chan AS, Lee RW, Cistulli PA. Dental appliance treatment for obstructive sleep apnea. Chest. 2007;132(2):693-699.
- Clark GT, Blumenfeld I, Yoffe N, Peled E, Lavie P. A crossover study comparing the efficacy of continuous positive airway pressure with anterior mandibular positioning devices on patients with obstructive sleep apnea. Chest. 1996;109(6):1477-1483.
- Ferguson KA, Ono T, Lowe AA, Al-Majed S, Love LL, Fleetham JA. A short-term controlled trial of an adjustable oral appliance for the treatment of mild to moderate obstructive sleep apnoea. Thorax. 1997;52(4):362-368.
- Ruiter MHTD, Aarab G, Vries ND, Lobbezoo F, Lange JD. A stepwise titration protocol for oral appliance therapy in positional obstructive sleep apnea patients: proof of concept. Sleep Breath. 2020;24(3):1229-1236 .
- Basyuni S, Barabas M, Quinnell T. An update on mandibular advancement devices for the treatment of obstructive sleep apnoea hypopnoea syndrome. J Thorac Dis. 2018;10(S1).
- Feinstein AJ, Zaki M, Zaghi S, Tajima T, Wang MB. Utilization of a mandibular advancement device for obstructive sleep apnea in the veteran population. J Dent Sleep Med. 2017;4(2):37–40.
- Schoch OD, Baty F, Niedermann J, Rüdiger JJ, Brutsche MH. Baseline predictors of adherence to positive airway pressure therapy for sleep apnea: a 10-year single-center observational cohort study. Respiration. 2014;87(2):121-128.
- Gagnadoux F, Vaillant ML, Goupil F, et al. Influence of marital status and employment status on long-term adherence with continuous positive airway pressure in sleep apnea patients. PLoS One. 2011;6(8).
- Jacobsen AR, Eriksen F, Hansen RW, et al. Determinants for adherence to continuous positive airway pressure therapy in obstructive sleep apnea. PLoS One 2017;12(12): e0189614.
- Almeida F, Lowe A, Tsuiki S, et al. Long-term compliance and side effects of oral appliances used for the treatment of snoring and obstructive sleep apnea syndrome. J Clin Sleep Med. 2005;1(2):143-152.
- Barnes M, Mcevoy RD, Banks S, et al. Efficacy of positive airway pressure and oral appliance in mild to moderate obstructive sleep apnea. Am J Respir Crit Care Med. 2004;170(6):656-664.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication April 28, 2020
Submitted in final revised form September 27, 2020
Accepted for publication October 1, 2020
Address correspondence to: Harmeet K. Chiang, Virginia Commonwealth University School of Dentistry, Lyons Dental Building, 520 North 12th Street, Box 980566, Richmond, Virginia 23298-0566. Email: hkchiang@vcu.edu