Original Article 4, Issue 4.2
Obstructive Sleep Apnea and Tooth Wear: Association and Confounding Factors
http://dx.doi.org/10.15331/jdsm.6528
Eduardo Anitua, PhD1,2,3; Joaquin Durán-Cantolla, PhD3,4,5,6,7; Juan Saracho, DDS1 ; Mohammad Hamdan Alkhraisat, PhD2,3?
1Clínica Eduardo Anitua, Vitoria, Spain; 2BTI Biotechnology Institute, Vitoria, Spain; 3Eduardo 11Anitua Foundation, Victoria, Spain; 4Sleep Disorders Unit, Clínica Eduardo Anitua, Vitoria, Spain; 5Sleep Disorders Unit, Hospital Universitario Araba, Vitoria, Spain; 6BioAraba Project, Hospital Universitario Araba, Vitoria, Spain; 7Cyber of Respiratory Diseases (CibeRes), ISCIII, Madrid, Spain
ABSTRACT
Study Objectives:
Obstructive sleep apnea (OSA) is a common health problem that is not adequately managed because of the low percentage of patients that receive the appropriate diagnosis. The multidisciplinary nature of sleep disorders mean that those other than physicians (including dentists) could aid in the identification of patients at risk for OSA. This study aimed at investigating the frequency and the association of tooth wear in patients with OSA.
Methods:
Patients were selected if they had undergone a sleep study for suspected OSA. Tooth wear was assessed in these patients and was classified as mild, moderate, or severe. Anthropometric data were also obtained. Descriptive statistics and correlation analysis were performed to assess the association between tooth wear and OSA. Multiple regression analysis was also performed.
Results:
Ninety-nine patients met the inclusion criteria. Using the apnea-hypopnea index to classify OSA, 31 patients had no OSA (control group). Thirty-four patients had mild OSA, 21 had moderate OSA, and 13 had severe OSA. The frequency of severe tooth wear increased as the severity of OSA increased. The frequency was zero, 5.9%, 28.6%, and 61.5% for patients without OSA, and those with mild, moderate, and severe OSA, respectively. Spearman correlation indicated the presence of a statistically significant association between the severity of tooth wear and the severity of OSA. Multiple regression analysis indicated that the severity of OSA and age affected significantly the severity of tooth wear.
Conclusions:
More studies are needed on the association of tooth wear and OSA.
Keywords:
age, apnea-hypopnea index, obstructive sleep apnea, OSA, tooth wear
Citation:
Anitua E, Durán-Cantolla J, Saracho J, Alkhraisat MH. Obstructive sleep apnea and tooth wear: association and confounding factors. Journal of Dental Sleep Medicine. 2017;4(2):45–50.
INTRODUCTION
Obstructive sleep apnea (OSA) is characterized by episodes of complete and/or partial collapse of the upper airway accompanied by a decrease in oxygen saturation. These events provoke temporal arousal and sleep fragmentation that lead to nonreparative sleep.1,2 The repeated oxygen desaturation and saturation provokes endocrine and metabolic disturbances that increase the risk of systemic complications.3,4 Many studies have established OSA as a risk factor for arterial hypertension and cardiovascular and cerebrovascular complications.3,5–8 OSA has also been related to traffic accidents, and a higher mortality has been reported among patients with OSA.9,10
Despite these consequences, OSA is still not adequately managed. It has been estimated that only 10% of the population with OSA receive a diagnosis and undergo treatment.11 Furthermore, it is estimated that more than 20% of patients have an apnea-hypopnea index (AHI) higher than 5, and 2% to 8% have severe OSA.2,5 The prevalence of OSA has been reported to be 3.1% to 7.5% in men and 1.2% to 3.2% in women.12 These statistics make the establishment of clinical markers to detect OSA, and the need to perform a sleep study on those found likely to be diagnosed with OSA necessary.
Several studies have investigated the association between sleep bruxism and OSA13–16; however, conclusive evidence is still lacking.17,18 The definitive diagnosis of bruxism is made by polysomnography.19 Polysomnography is expensive, time consuming, and has been associated with the risk of the misdiagnosis of the absence of bruxism.18 Moreover, patients who are suspected of having OSA may have had previous episodes of bruxism that they would not demonstrate in one night of polysomnography testing. In practice, the presence of clinical signs of occlusal wear patterns on natural teeth or restorative materials is frequently used by dentists to diagnose bruxism. All of these issues would justify the assessment of the association between tooth wear and OSA. The diagnosis of tooth wear is immediate, less expensive than polysomnography, and is made by the inspection of the tooth surface.20 Moreover, a significant correlation between the clench index and AHI has been established.21
Recently, an association between tooth wear and OSA has been reported.20 However, this study was limited by a small sample size and lack of a control group to evaluate the confounding factors that could affect the association between tooth wear and OSA. The main objectives of the current study were (1) investigate the frequency of tooth wear in patients with OSA, (2) test the association between them, and (3) identify possible confounding factors. Patients who had undergone a sleep study were recruited and their grade of tooth wear was assessed. The null hypothesis was that there is no association between tooth wear and OSA.
METHODS
This article was written following the STROBE (Strengthening the Reporting of Observational studies in Epidemiology) guidelines. The study was performed in accordance with the Declaration of Helsinki. Patient records were retrospectively reviewed to select those who were treated in the sleep disorders unit at the dental center. Patients of both sexes were eligible to participate in this study and were selected according to the following inclusion criteria:
• Older than 18 years
• Had undergone a sleep study
The exclusion criteria were:
• Complete edentulism
• Crossbite and/or tooth wear localized in one or two teeth
• Absence of posterior teeth contact in centric occlusion
• Presence of less than 8 teeth per arch
• Partial edentulism with free distal end
• Teeth with wear having as antagonists a rehabilitated tooth
To achieve a blinded evaluation, the dentist responsible for tooth wear assessment was a prosthodontist and had no opportunity to see the results of the sleep study. The sleep technician was not aware of the presence/absence of tooth wear when analyzing the sleep recordings.
Tooth Wear Assessment
The dentist evaluated the patient’s dentition for type and severity of tooth wear. Intraoral radiographs, clinical photographs, and cast models were examined. The severity of the tooth wear was then classified as22:
• Mild: the loss of tooth substance was limited to the enamel
• Moderate: the loss of tooth substance extended to the dentin and was not limited to the occlusal/incisal surface but limited to less than one-third of the tooth (shortening of the tooth height)
• Severe: extensive wear of the dentin was observed and it affected more than one-third of the tooth
Tooth wear was also classified into abrasion, attrition, and erosion. Abrasion means that the cause of tooth wear was exogenous objects and substances.23 Attrition occurs when the cause was tooth-tooth contact.23 Erosion occurs when the cause was chemical action not involving bacteria.24
Sleep Study
The weight and height of each patient were obtained. The body mass index (BMI) was calculated by dividing the body weight in kilograms by the body height in meters squared.
A validated respiratory polygraphy (BTI APNiA, BTI Biotechnology Institute, Vitoria, Spain) was employed to perform the sleep study at the patient’s home.25 This respiratory polygraphy is a type III home sleep monitoring device. The device measured the nasal air flow with a probe connected to a transducer and the oxygen saturation with cutaneous pulse oximetry via a finger probe (model 7000A and Modl XPOD 3012LP; Nonin Medical; Plymouth, Minnesota, United States). All sleep studies were analyzed automatically by BTI-APNiA according to the criteria of the American Academy of Sleep Medicine.26,27 The sleep analysis was controlled by a sleep technician and was supervised by a sleep medicine specialist. The minimum time of recording was 6 hours and the minimum time of sleep was 180 minutes. The following definition of the respiratory variables were used:
• Apnea: a drop in the respiratory signal of more than 90% during a minimum of 10 seconds
• Hypopnea: a drop in the respiratory signal between 30% and 90%, accompanied by a drop in oxygen saturation ≥ 3% and/or arousal
Statistical Analysis
Quantitative data were described by the calculation of the mean and standard deviation. Continuous variables were expressed by mean ± typical deviation and were compared with analysis of variance or Kruskal-Wallis test according to the results of the normality test (Shapiro-Wilk). The patients with AHI < 5 served as a control group. Qualitative variables were expressed in number of events and were compared with the χ2 test. The frequency of qualitative variables was also calculated. The association between severity of OSA, tooth wear, and confounders (age, sex, BMI) was evaluated using Spearman correlation test. Only factors with significant association with tooth wear and OSA were then introduced in a linear regression analysis to evaluate the collinearity of variables. Then a multiple regression analysis was performed to test the effect of OSA severity, sex, age, and BMI on the severity of tooth wear. Statistical analysis was performed using SPSS 15.0 (SPSS Inc.; IBM). Statistical significance was set at P < .05.
RESULTS
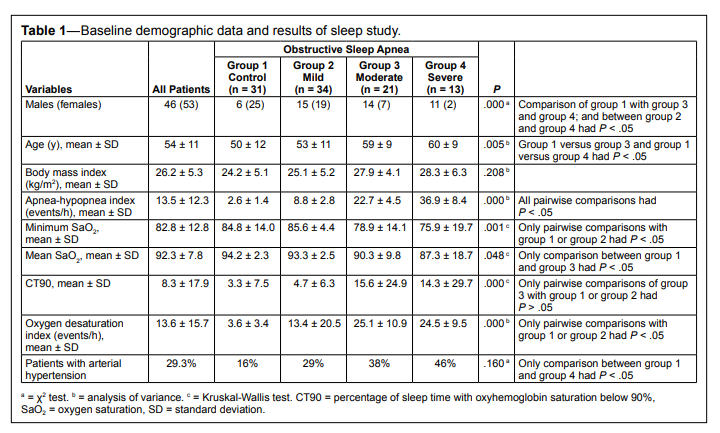
One hundred seventy-one records were retrospectively reviewed. A total of 99 patients were included in the analysis; 72 patients did not meet the inclusion criteria or had at least one of the exclusion criteria. Tooth wear could not be evaluated in 15 patients, teeth were restored in 23, partial edentulism with free distal end and absence of posterior tooth contact were observed in 7, presence of fewer than 8 teeth per arch in 10, complete edentulism was observed in 1, crossbite/deep overbite was observed in 4 patients, no tooth contact in 1 patient, and teeth with wear having as antagonists a rehabilitated tooth was observed in 11.The baseline demographic characteristics of the patients are shown in Table 1. There were 46.5% of the patients who were males, and the mean ± standard deviation age was 54 ± 11 years. The mean BMI indicated the presence of overweight subjects among the study group. Using AHI to classify OSA indicated that 31 patients had no OSA (AHI < 5) (control group), 34 had mild OSA (5 ≤ AHI < 15), 21 had moderate OSA (15 ≤ AHI < 30), and 13 had severe OSA (AHI ≥ 30). The parameters that described oxygen saturation worsened as the severity of OSA increased. The fraction of patients with arterial hypertension was significantly higher in patients with severe OSA than in the control group.
Table 1Baseline demographic data and results of sleep study. |
{kind=link}
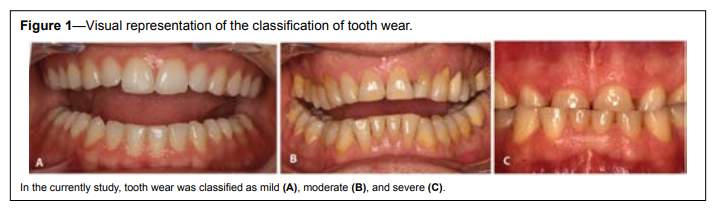
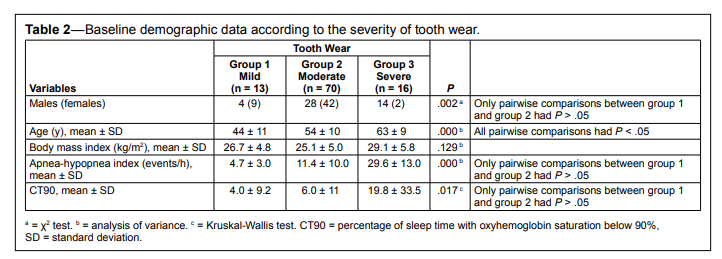
Figure 1 shows mild, moderate, and severe tooth wear. The tabulation of the data according to the severity of tooth wear is shown in Table 2. There was a proportional relationship between the severity of tooth wear and the value of the AHI. The AHI was 29.6 ± 13.0 for patients with severe tooth wear in comparison with 4.7 ± 3.0 for those with mild tooth wear. The analysis of variance indicated that these differences were statistically significant (P = .000). Patients were older as tooth wear increased. The percentage of males in the group was greater as tooth wear increased.
Figure 1Visual representation of the classification of tooth wear. |
{kind=link}
Table 2Baseline demographic data according to the severity of tooth wear. |
{kind=link}
Tooth attrition was the main cause of tooth wear in most of the patients. Three patients with moderate tooth wear had tooth abrasion, in another two both attrition and abrasion coexisted, and in one patient both attrition and erosion were identified. Tooth attrition was observed in all patients with severe tooth wear and tooth erosion was additionally observed in two patients.
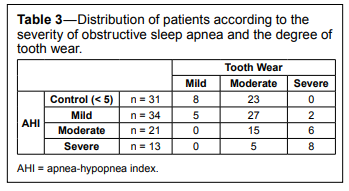
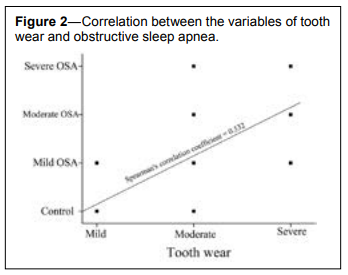
The tabulation of patients according to the severity of tooth wear and the severity of OSA is shown in Table 3. Of the control group, 74.2% had moderate tooth wear, but no individuals in the control group had severe tooth wear. As the severity of OSA increased the number of patients with severe tooth wear increased. More than 28% and 61% of patients with moderate and severe OSA, respectively, had severe tooth wear. Spearman correlation indicated the presence of a statistically significant association between the two variables (coefficient = .532; P = .000) (Figure 2). To test the influence of age, sex, and BMI in this association a linear regression analysis was first performed to evaluate the collinearity between variables. The values of variance inflation factor were all less than 3 and a multiple regression analysis was performed. The results indicated that only age (P = .007) and severity of OSA (P = .021) had a significant effect on the severity of tooth wear (Cox and Snell pseudo R2 = .513).
Table 3Distribution of patients according to the severity of obstructive sleep apnea and the degree of tooth wear. |
{kind=link}
Figure 2Correlation between the variables of tooth wear and obstructive sleep apnea. |
{kind=link}
DISCUSSION
The results of this study support the rejection of the null hypothesis. The severity of tooth wear is significantly correlated with the severity of OSA. This is in accordance with the previously published data by Duran-Cantolla and coworkers.20 All patients in the control group had mild to moderate tooth wear, whereas patients with more severe OSA had more severe tooth wear. All patients with severe tooth wear had OSA.
The results of the multiple regression analysis identify age as a variable that significantly affected the association between tooth wear and OSA. This has a few possible explanations. It has been found that sleep fragmentation also results in altered sympathetic activity and psychological alterations (mood changes).28 Altered sympathetic activity can increase the chance of masticatory muscle contraction and the risk of occlusal overloading.28 Given that arousals precipitate sleep fragmentation, and that arousals are increasingly frequent in older people, a line could be drawn connecting sleep fragmentation and tooth wear. Tooth contact occurring in association with arousals has been more frequently observed in patients with tooth grinding than those without tooth grinding,29 and in patients with occlusal wear, a prolongation of occlusion time has also been observed.30
A second explanation may be that tonic masticatory muscle activity was frequently found at the conclusion of apneic events.31–33 Interestingly, a significant correlation between the clench index and AHI was found.21 Phillips et al. concluded that the sleep arousal or disturbances caused by sleep apnea was related to parafunctional activities.21
Third, it is known that the prevalence of both tooth wear and OSA increase with age.5,34
Pigno et al. have reported that tooth wear has been greater in patients reporting teeth grinding/clenching.35 Several studies have investigated the association between sleep bruxism and OSA14–16; however, conclusive evidence is still lacking.17,18,32 Bruxism is a factor that could be associated with tooth wear,36 although in a 2011 study it was concluded that the overall significance of bruxism as a causative factor of tooth wear is not fully known.37
Tooth wear could lead to changes in the height of the lower face that could affect the patency of the upper airway. In a recent study, Sanders et al. reported that tooth loss could be an independent risk factor for OSA.38 The loss of teeth would provoke changes that could compromise the patency of the upper airway. These changes include the horizontal and vertical atrophy of the alveolar process, the reduction in the vertical dimension of the occlusion, the upward rotation of the mandible, and the posterior positioning of the tongue at rest.39–42
Along with the evaluation of the degree of tooth wear, the type of tooth substance loss (attrition, abrasion, erosion, or abfraction) was also evaluated. We found only three patients with signs of tooth erosion. Tooth wear and erosion can become more severe when sleep-related gastroesophageal reflux is comorbid with sleep bruxism.43 This prompted the analysis of the effect of gastroesophageal reflux disease (GERD) on the association between the severity of tooth wear and the severity of OSA. GERD is considered one of the most common chronic diseases in adults and its relation to OSA has received attention.44,45 In one cohort study, the prevalence of GERD was significantly increased in patients with primary snoring and OSA, but the severity of OSA did not influence GERD prevalence.44 The authors concluded that OSA was not likely a causative factor for GERD. In another study, the complicating hiatal hernia was suggested to link reflux esophagitis to OSA.46 Yang and coworkers concluded that in patients with coexisting GERD and OSA, both awakening and arousal preceded gastroesophageal reflux events, but gastroesophageal reflux does not appear to precipitate sleep-related events.47 The role of consumption of soft drinks on tooth wear could not be assessed due to the retrospective nature of the study.
The diagnosis of tooth wear is immediate, inexpensive, and can be made based on the clinical examination of tooth surfaces. These characteristics make tooth wear a good potential identifier of patients at risk of having OSA. The involvement of more medical professionals in identifying patients who are likely to have OSA would aid in the early diagnosis of the disease and minimize the effect of its consequences. However, scientific evidence solidifying the association between tooth wear and OSA is still needed. We encourage research groups to further investigate this association and to help establish definitive conclusions.
This study is affected by the limitation of retrospective design, in which the dependency on the availability and accuracy of medical/dental records could not be excluded. It is difficult to control bias and confounders, although the dentist who evaluated tooth wear was not aware of the results of the sleep study. Another limitation is that the method of assessing tooth wear severity is subjective. However, it is a simple assessment that all dentists can adequately provide. In the current study, the combination of study models and clinical photographs permitted the evaluation of tooth wear. In future prospective studies, intraoral inspection should be included. The 32 patients with AHI < 5 served as controls to compare the results of patients with OSA. A selection bias could not be ruled out as patients were selected from those who underwent a sleep study. This means that there was a need for a sleep study from the point of view of a specialist in sleep medicine.
We think these outcomes justify the performance of prospective and controlled clinical studies to evaluate the association between tooth wear and OSA and to identify confounders that may influence this association. The results of the current study would be helpful in calculating the sample size of prospective and controlled clinical studies.
CONCLUSIONS
Tooth wear is significantly affected by the severity of OSA. Tooth wear severity may be an indicator of the presence of OSA. There is a need for more scientific evidence to further explore this relationship.REFERENCES
2. Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328(17):1230–1235.
3. Bradley TD, Floras JS. Obstructive sleep apnoea and its cardiovascular consequences. Lancet. 2009;373(9657):82–93.
4. Xu T, Feng Y, Peng H, Guo D, Li T. Obstructive sleep apnea and the risk of perinatal outcomes: a meta-analysis of cohort studies. Sci Rep. 2014;4:6982.
5. Duran J, Esnaola S, Rubio R, Iztueta A. Obstructive sleep apneahypopnea and related clinical features in a population-based sample of subjects aged 30 to 70 yr. Am J Respir Crit Care Med. 2001;163(3 Pt 1):685–689.
6. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046–1053.
7. Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342(19):1378–1384.
8. Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353(19):2034–2041.
9. Rich J, Raviv A, Raviv N, Brietzke SE. All-cause mortality and obstructive sleep apnea severity revisited. Otolaryngol Head Neck Surg. 2012;147(3):583–587.
10. Teran-Santos J, Jimenez-Gomez A, Cordero-Guevara J. The association between sleep apnea and the risk of traffic accidents. Cooperative Group Burgos-Santander. N Engl J Med. 1999;340(11):847–851.
11. Young T, Evans L, Finn L, Palta M. Estimation of the clinically diagnosed proportion of sleep apnea syndrome in middle-aged men and women. Sleep. 1997;20(9):705–706.
12. Lee W, Nagubadi S, Kryger MH, Mokhlesi B. Epidemiology of obstructive sleep apnea: a population-based perspective. Expert Rev Respir Med. 2008;2(3):349–364.
13. Kato T. Sleep bruxism and its relation to obstructive sleep apneahypopnea syndrome. Sleep Biol Rhythms. 2004;2(1):1–15.
14. Kato T, Thie NM, Huynh N, Miyawaki S, Lavigne GJ. Topical review: sleep bruxism and the role of peripheral sensory influences. J Orofac Pain. 2003;17(3):191–213.
15. Lavigne GJ, Kato T, Kolta A, Sessle BJ. Neurobiological mechanisms involved in sleep bruxism. Crit Rev Oral Biol Med. 2003;14(1):30–46.
16. Ohayon MM, Li KK, Guilleminault C. Risk factors for sleep bruxism in the general population. Chest. 2001;119(1):53–61.
17. Hosoya H, Kitaura H, Hashimoto T, et al. Relationship between sleep bruxism and sleep respiratory events in patients with obstructive sleep apnea syndrome. Sleep Breath. 2014;18(4):837–844.
18. Maluly M, Andersen ML, Dal-Fabbro C, et al. Polysomnographic study of the prevalence of sleep bruxism in a population sample. J Dent Res. 2013;92(7 Suppl):97S–103S.
19. Lobbezoo F, Ahlberg J, Glaros AG, et al. Bruxism defined and graded: an international consensus. J Oral Rehabil. 2013;40(1):2–4.
20. Duran-Cantolla J, Alkhraisat MH, Martinez-Null C, Aguirre JJ, Guinea ER, Anitua E. Frequency of obstructive sleep apnea syndrome in dental patients with tooth wear. J Clin Sleep Med. 2015;11(4):445–450.
21. Phillips BA, Okeson J, Paesani D, Gilmore R. Effect of sleep position on sleep apnea and parafunctional activity. Chest. 1986;90(3):424–429.
22. Paesani DA. Dental Erosion. In: Paesani DA, ed. Bruxism: Theory and Practice. Hanover Park, IL: Quintessence Publishing; 2010:149–183.
23. Mair LH. Wear in dentistry--current terminology. J Dent. 1992;20(3):140–144.
24. Eccles JD. Tooth surface loss from abrasion, attrition and erosion. Dent Update. 1982;9(7):373–374, 376–378, 380–381.
25. Duran-Cantolla J, Zamora Almeida G, Vegas Diaz de Guerenu O, et al. Validation of a new domiciliary diagnosis device for automatic diagnosis of patients with clinical suspicion of OSA. Respirology 2017;22(2):378–385.
26. Collop NA, Tracy SL, Kapur V, et al. Obstructive sleep apnea devices for out-of-center (OOC) testing: technology evaluation. J Clin Sleep Med. 2011;7(5):531–548.
27. Ferber R, Millman R, Coppola M, et al. Portable recording in the assessment of obstructive sleep apnea. ASDA standards of practice. Sleep. 1994;17(4):378–392.
28. Kato T, Yamaguchi T, Okura K, Abe S, Lavigne GJ. Sleep less and bite more: sleep disorders associated with occlusal loads during sleep. J Prosthodont Res. 2013;57(2):69–81.
29. Baba K, Clark GT, Watanabe T, Ohyama T. Bruxism force detection by a piezoelectric film-based recording device in sleeping humans. J Orofac Pain. 2003;17(1):58–64.
30. Sierpinska T, Kuc J, Golebiewska M. Assessment of masticatory muscle activity and occlusion time in patients with advanced tooth wear. Arch Oral Biol. 2015;60(9):1346–1355.
31. Inoko Y, Shimizu K, Morita O, Kohno M. Relationship between masseter muscle activity and sleep-disordered breathing. Sleep Biol Rhythms. 2004;2(1):67–68.
32. Sjöholm TT, Lowe AA, Miyamoto K, Fleetham JA, Ryan CF. Sleep bruxism in patients with sleep-disordered breathing. Arch Oral Biol. 2000;45(10):889–896.
33. Yoshida K. A polysomnographic study on masticatory and tongue muscle activity during obstructive and central sleep apnea. J Oral Rehabil. 1998;25(8):603–609.
34. Van’t Spijker A, Rodriguez JM, Kreulen CM, Bronkhorst EM, Bartlett DW, Creugers NH. Prevalence of tooth wear in adults. Int J Prosthodont. 2009;22(1):35–42.
35. Pigno MA, Hatch JP, Rodrigues-Garcia RC, Sakai S, Rugh JD. Severity, distribution, and correlates of occlusal tooth wear in a sample of Mexican-American and European-American adults. Int J Prosthodont. 2001;14(1):65–70.
36. Paesani DA. Tooth Wear. In: Paesani DA, ed. Bruxism: Theory and Practice. Hanover Park, IL: Quintessence Publishing; 2010:123–147.
37. Johansson A, Omar R, Carlsson GE. Bruxism and prosthetic treatment: a critical review. J Prosthodont Res. 2011;55(3):127–136.
38. Sanders AE, Akinkugbe AA, Slade GD, Essick GK. Tooth loss and obstructive sleep apnea signs and symptoms in the US population. Sleep Breath. 2016;20(3):1095–1102.
39. Cawood JI, Howell RA. A classification of the edentulous jaws. Int J Oral Maxillofac Surg. 1988;17(4):232–236.
40. Douglass JB, Meader L, Kaplan A, Ellinger CW. Cephalometric evaluation of the changes in patients wearing complete dentures: a 20- year study. J Prosthet Dent. 1993;69(3):270–275.
41. Kotsiomiti E, Farmakis N, Kapari D. Factors related to the resting tongue position among partially and completely edentulous subjects. J Oral Rehabil. 2005;32(6):397–402.
42. Tallgren A, Lang BR, Walker GF, Ash MM Jr. Roentgen cephalometric analysis of ridge resorption and changes in jaw and occlusal relationships in immediate complete denture wearers. J Oral Rehabil. 1980;7(1):77–94.
43. Thie NM, Kato T, Bader G, Montplaisir JY, Lavigne GJ. The significance of saliva during sleep and the relevance of oromotor movements. Sleep Med Rev. 2002;6(3):213–227.
44. Basoglu OK, Vardar R, Tasbakan MS, et al. Obstructive sleep apnea syndrome and gastroesophageal reflux disease: the importance of obesity and gender. Sleep Breath. 2015;19(2):585–592.
45. Bor S, Mandiracioglu A, Kitapcioglu G, Caymaz-Bor C, Gilbert RJ. Gastroesophageal reflux disease in a low-income region in Turkey. Am J Gastroenterol. 2005;100(4):759–765.
46. Zenda T, Hamazaki K, Oka R, et al. Endoscopic assessment of reflux esophagitis concurrent with hiatal hernia in male Japanese patients with obstructive sleep apnea. Scand J Gastroenterol. 2014;49(9):1035–1043.
47. Yang YX, Spencer G, Schutte-Rodin S, Brensinger C, Metz DC. Gastroesophageal reflux and sleep events in obstructive sleep apnea. Eur J Gastroenterol Hepatol. 2013;25(9):1017–1023.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication September 9, 2016
Submitted in final revised form December 30, 2016
Accepted for publication January 30, 2017
Address correspondence to: Dr. Eduardo Anitua, Eduardo Anitua Foundation, C/ Jose Maria Cagigal 19, 01007 Vitoria, Spain; Email: eduardoanitua@eduardoanitua.com
DISCLOSURE STATEMENT
This was not an industry supported study. Dr. Anitua is the scientific director and Dr. Alkhraisat is an employee of BTI Biotechnology Institute, producer of the BTI APNiA respiratroy polygraphy. The other authors have indicated no financial conflicts of interest.