Original Article 3, Issue 8.1
Polysomnographic Pilot Study of a New Mandibular Oral Device for Mild to Moderate Obstructive Sleep Apnea
http://dx.doi.org/10.15331/jdsm.7174Giacomo Chiaro, MD1; Ninfa Amato, PhD1; Francesco Fanfulla, MD2; Massimo Ciocco, DMD3; Damiano Frigerio, DMT3; Alessia Sada, DMD4; Renato Piantanida, MD5; Marco Pons, MD6; Mauro Manconi, MD, PhD1,7,8
1Sleep Medicine Unit, Neurocenter of Southern Switzerland, Ospedale Regionale, Lugano, Switzerland; 2Respiratory Function and Sleep Medicine Unit, Istituti Clinici Scientifici Maugeri IRCCS, Pavia, Italy; 3Private Practice, Lugano, Switzerland; 4Private Practice, Verbania, Italy; 5Department of Otorhinolaryngology, Civic Hospital of Lugano, Lugano, Switzerland; 6Department of Pulmonology, Civic Hospital of Lugano, Lugano, Switzerland; 7Faculty of Biomedical Sciences, Università della Svizzera Italiana, Lugano; 8Bern University, Bern, Switzerland
ABSTRACT
Study Objectives:
The mandibular advancement device (MAD) in study, the velolingual bite (VLB), was a custom-made, monobloc device including a tongue retention and suction cavity and a direct anchorage onto the mandibular bone and not onto the teeth. The main objective of the study was to evaluate the efficacy of the MAD in reducing pathologic sleep-related breathing events and in improving overall sleep quality. The study also sought to evaluate tolerability of and compliance to the MAD therapy.
Methods:
This was a monocentric, prospective, open-label, interventional, polysomnographic pilot study. The main study outcome was the reduction in pathologic sleep-related breathing events. Treatment response was defined as a decrease of ≥50% in apnea-hypopnea index (AHI) and respiratory disturbance index (RDI). Treatment success was defined as the normalization of the AHI (< 5 events per hour). Secondary outcomes included improvement of video-polysomnographic parameters and subjective sleep quality and daytime somnolence. Side effects, tolerability, and compliance to treatment were adjunctive secondary outcomes, measured subjectively by means of a semi-structured self-administered questionnaire.
Results:
Twenty patients (3 females) were enrolled, of whom 19 completed the study. Complete treatment success (AHI <5 events per hour) was met in 11 cases. Treatment response (decrease of ≥50% in AHI and RDI) was reached in 13 and 14 patients, respectively. The MAD was well tolerated and no major side effects were reported.
Conclusions:
The VLB was effective in reducing pathologic sleep-related breathing events. Treatment response and treatment success were both met in a large proportion of subjects. The MAD was well tolerated, with mild side effects that were mostly confined to salivation issues and initial and transient toothache and temporomandibular joint discomfort.
Keywords:
mandibular advancement device; custom-made; velolingual bite; sleep apnea; polysomnography
Citation:
Chiaro G, Amato N, Fanfulla F, et al. Polysomnographic pilot study of a new mandibular oral device for mild to moderate obstructive sleep apnea. J Dent Sleep Med. 2021;8(1)
INTRODUCTION
Mandibular advancement devices (MAD) are a valid alternative to continuous positive airway pressure (CPAP) ventilation during sleep in the treatment of snoring and mild to moderate obstructive sleep apnea syndrome (SAS).1 MADs may also be considered in patients with severe SAS who do not tolerate CPAP treatment or in combination with it.2 Worn intraorally during sleep, they are usually anchored onto the dental arches and induce mandibular advancement (i.e., protrusion), resulting in several beneficial anatomic changes, including anteroposterior and lateral retrolingual and pharyngeal space enlargement, resulting in increased oropharyngeal cross-sectional areas and upper airway volume. The reduction in pathologic respiratory events during sleep seems to correlate with the previously mentioned modifications in upper airway dimensions induced by MADs.3
A wide variety of MADs are available on the market, covering a range of sophistication and cost. They slightly differ from one another in the following aspects: configuration (i.e., one or two pieces); size; material; degree of attachment to patient's dentition; coupling mechanism (i.e., the method by which the two upper and lower pieces connect); occlusal coverage (i.e., coverage of the surfaces of the teeth that touch each other when the mouth is closed); ability to titrate the mandibular protrusion (so far, only two-piece devices are available for custom titration); propulsive mechanism, and oral respiration. Custom-fitted and titratable MADs are preferrable to self-administered and non-titratable, over-the-counter varieties (i.e., boil and bite), since they appear to be more effective, comfortable, and more likely to be retained by both dental arches, ensuring that the lower jaw does not fall out of the appliance during sleep.4-6 There has been a proliferation of various designs since the first commercially available oral appliances were introduced in the 1980s.7 In March 2013, the American Academy of Dental Sleep Medicine (AADSM) published a definition of an effective MAD, focusing on custom-titratable MADs.8
The MAD in the study, the velolingual bite (VLB), consists in a custom-made monobloc device including a tongue retention and suction cavity to push the tongue down and forward onto the mouth floor, thus preventing its lifting towards the hard palate. Its design requires the presence of only four occlusal points, allowing for a non-invasive frontal push onto the vestibular face of the mandibular bone, thus reducing the risk for occlusal changes, tooth loosening, and the development of an anterior crossbite, which represent the major long-term adverse effects of oral appliances. Currently, the VLB represents the first monobloc device that can be titrated. It holds a Swiss patent and trademark. European equivalents are underway. All VLB components are CE marked and have a 5-year warranty. The possibility of printing further duplicates with three-dimensional machinery is currently under development (Appendix A, supplemental materials).
STUDY OBJECTIVES
The main objective of this study consisted in exploring the efficacy of the VLB in reducing pathologic sleep-related breathing events and improving overall sleep quality. The study also sought to evaluate the tolerability of and compliance to MAD therapy.
METHODS
Trial Design
This was a monocentric, prospective, open-label, interventional, polysomnographic pilot study.
Inclusion and Exclusion Criteria
Eligible study subjects had to be consecutive female and male patients aged 18 to 65 years referred to the sleep center for suspected SAS, and who underwent video-polysomnography (VPSG) within the past 3 months from study beginning date. Patients had to have mild to moderate SAS (AHI ≥ 5 events per hour and < 30 events per hour). The presence of at least four teeth both in the posterior lower and upper arches and the ability to protrude the mandible for at least 6 mm were a requirement.
Any one of the following criteria led to the exclusion of the participant: other significant neurologic conditions; major ear, nose, and throat surgery modifying the anatomy of the upper airways (i.e., uvulopalatopharyngoplasty; palatoschisis; neoplastic lesions); limited mental capacity; treatment with drugs affecting sleep (i.e.: hypnotics, antidepressants, neuroleptics, antiepileptics); trigeminal neuralgia and/or myofacial pain dysfunction; sleep-related central breathing disorders; obesity with a body mass index (BMI) ≥ 30 kg/m2. Prior to inclusion, significant oropharyngeal disease (especially adenotonsillar and/or tonsillar hypertrophy) had to be ruled out by means of fibro- endoscopic evaluation, performed by a trained ear, nose, and throat (ENT) specialist (RP). Patients who concomitantly used CPAP or positional therapy were excluded from the study. All patients gave their written consent for the study, which was approved by the local ethics committee.
Design of the Study
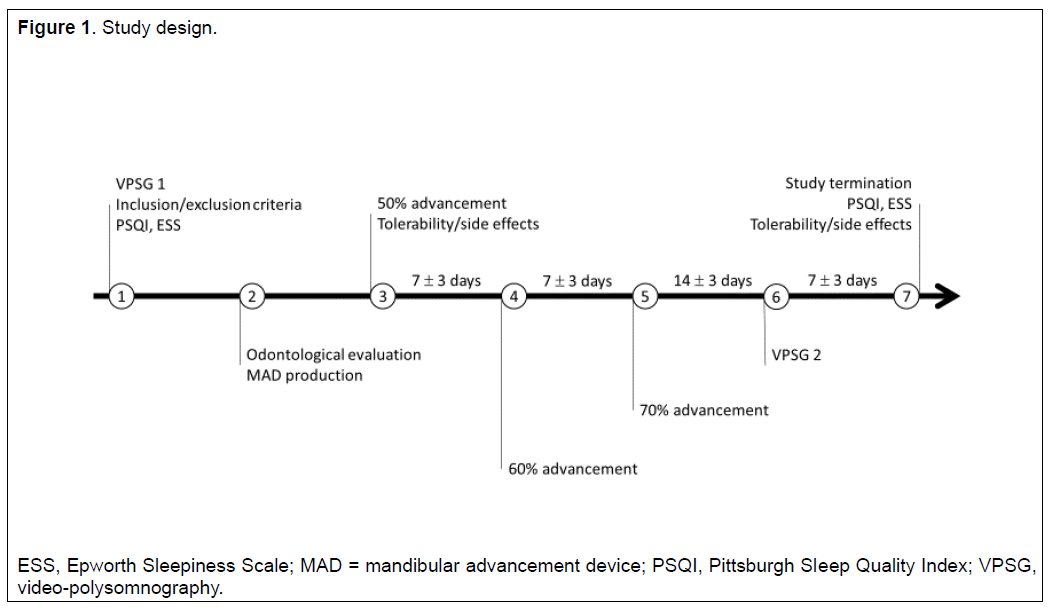
The study consisted of seven visits (Figure 1). At visit 1, inclusion and exclusion criteria were checked and eligible subjects were included in the study. The Pittsburgh Sleep Quality Index (PSQI) and Epworth Sleepiness Scale (ESS) were administered.
At visit 2, subjects underwent an odontologic evaluation. Thereafter, the MAD was produced and, at visit 3, it was administered at 50% of each subject’s mandibular advancement, as previously assessed on calculations of the subject’s maximal mandibular protrusion. Immediate tolerability and side effects (myofacial pain, temporomandibular tension) were checked at study visits 3 and 7 by means of a semi-structured self-administered questionnaire (Appendix B, supplemental materials). If the subject experienced important side effects at this stage, the study would be discontinued.
At visits 4 and 5, further mandibular advancements – to 60% and 70% respectively – of the calculated maximal mandibular protrusion were performed by the dentist.
At visit 6, the subject underwent a second VPSG while wearing the MAD. If, at any point from MAD administration (visit 3) to the achievement of a 70% mandibular protrusion (visit 5), any serious side effect occurred, the dentist would stop the mandibular advancement process and return to the previous level of mandibular protrusion, at which no side effects were experienced. The subject would then proceed directly to VPSG and leave the study thereafter.
At the final evaluation (visit 7), the subject met with the investigators again. PSQI and ESS were administered. The custom-made MAD was left with the subject free of charge.
VPSG Methods
Each subject underwent two full-night VPSG recordings, carried out following standard American Academy of Sleep Medicine procedures,9 described in detail in a previous study.10 All recordings were scored by a single physician expert in sleep medicine (GC) and the final diagnosis of SAS was confirmed by the senior author (MM). Those patients who had a supine AHI at least double the nonsupine AHI during basal PSG were defined as positional.
Outcome Measures and Assessments
The main study outcome was the reduction in pathologic sleep-related breathing events. Related primary outcome measures were the AHI, RDI, and supine AHI. Treatment success per each patient was defined as the normalization of the AHI (< 5 events per hour). Positive treatment response was defined as a decrease of ≥50% in AHI and RDI.
Secondary outcomes included improvement of sleep efficiency, sleep quality, and daytime somnolence. The improvement of sleep quality and daytime somnolence were measured subjectively with the PSQI and ESS. Related secondary outcome measures were polysomnographic parameters such as sleep efficiency, sleep latency, and wake after sleep onset, a measure of infrasleep awakenings.
Side effects, tolerability, and compliance to treatment were monitored and measured subjectively by means of a semi-structured self-administered questionnaire (Appendix B, supplemental materials) covering the following aspects: usage (nights/week; hours/night); side effects, reasons for interrupting usage; Visual Analog Scale for Pain (VAS Pain)11; Visual Analog Scale for Satisfaction (VAS Satisfaction). The number of dropouts and the percentage of incomplete mandibular advancements were other outcome measures.
Statistical Analysis
Values are presented as mean ± standard deviation. Data were first checked for normality and homogeneity of variance using the Shapiro-Wilk test and the Levene test, respectively. Within subjects, comparisons were then performed using the Wilcoxon rank-sum test. The Holm correction was applied to deal with multiple testing, and differences were considered significant at a value of P < 0.05 after correction. All statistical analyses were performed using SPSS® Version 25 (IBM, Armonk, NY).
The power calculation estimated at least 15 subjects, evaluated with two polysomnograms (PSGs) each (one basal and one on-treatment), as the number of subjects to allow the rejection of the null hypothesis with a power of 0.8 and type I error probability of 0.01.
Figure 1Study design. |
{kind=link}
RESULTS
Demographics
A total of 20 subjects (3 females) were enrolled, with an age range between 25 and 59 years (49.3 ± 9.2). Baseline BMI was 25.3 ± 2.4 and 25.2 ± 2.2 at the time of the second VPSG recording. One subject decided to discontinue the study before the MAD was produced. The remaining 19 patients completed the study, with 18 of them having proceeded to a mandibular advancement equal to 70% and one to 60% of their calculated total jaw excursion.
Polysomnographic Results
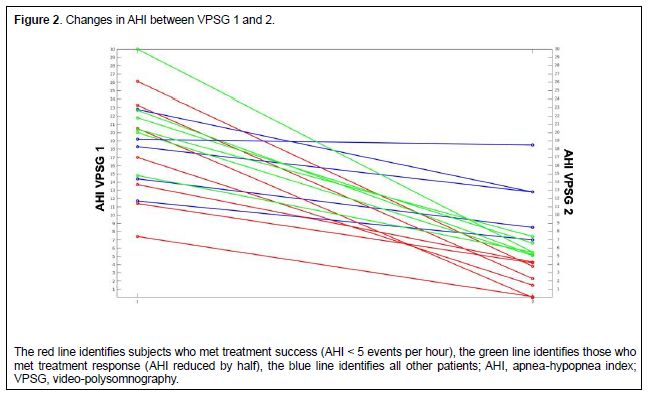
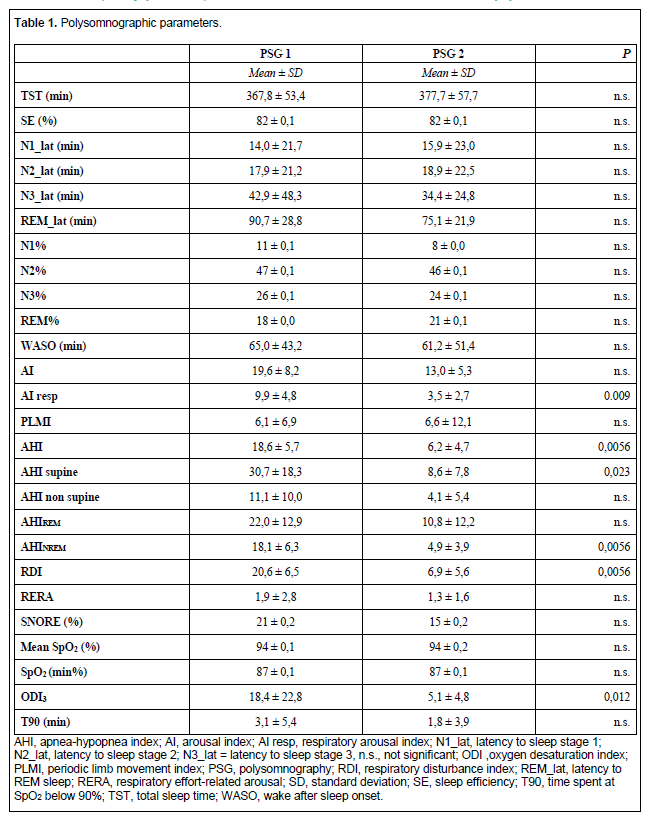
Polysomnographic data are summarized in Table 1. Overall, statistically significant reductions in AHI, supine AHI, RDI, and oxygen desaturation index 3% were found between PSGs before and during treatment. Complete treatment success (AHI <5 events per hour), which represented the main study outcome, was met in 11 cases. Treatment response (decrease of ≥50% in AHI or RDI) was reached in 13 and 14 cases, respectively (Figure 2). The arousal respiratory index significantly decreased (9.9 ± 4.8 vs. 3.5 ± 2.7, P = 0.009). Supine AHI as well non-rapid eye movement AHI were strongly suppressed by treatment, whereas the effect on rapid eye movement (REM) AHI was less evident. Twelve of 19 patients were affected by positional obstructive sleep apnea, as defined in the Methods section.
Age, BMI, RDI, AHI, supine AHI, and REM AHI were not predictors of either complete or partial response, when compared between responders (14 subjects, RDI cutoff value 50%) and non –responders (5 subjects). The same was true for those 11 subjects meeting treatment success (AHI >5 events per hour). These results should be taken into account carefully, given the low number of subjects.
Questionnaires
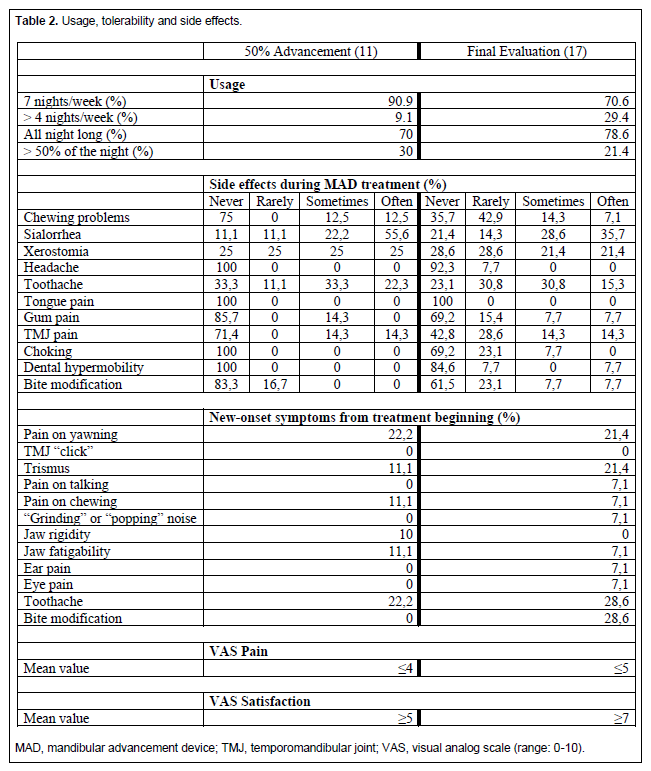
Eleven and 17 subjects out of 19 returned the semi-structured self-administered questionnaire regarding MAD tolerability and safety at study visit 3 and at the final evaluation, respectively. Results are summarized in Table 2. Overall, 70% of subjects reported using the device for 7 nights a week and 78% all night long. No subjects reported a score higher than 4 on the VAS Pain at 50% advancement and no subjects reported a score higher than 5 on the VAS Pain at final evaluation (only mean results are shown in the table). Regarding device satisfaction, all subjects reported a score higher than 5 on the VAS Satisfaction at 50% advancement, as well as a score higher than 7 at final evaluation.
All patients returned both sleep questionnaires (PSQI and ESS) at both study times. There was a significant reduction in the PSQI total score (6.6 ± 24 vs. 4.9 ± 2.6, P = 0.006), as well as in the ESS scores (7.0 ± 4.7 vs 5.0 ± 3.6, p = 0.02), although both scores (before and after treatment) were not pathologic.
Figure 2Changes in AHI between VPSG 1 and 2. |
{kind=link}
Table 1Polysomnographic parameters. |
{kind=link}
Table 2Usage, tolerability and side effects. |
{kind=link}
DISCUSSION
This study documented a significant efficacy of the new VLB device in reducing pathologic sleep-related breathing events, as measured by the reduction in AHI, in the supine position, as well as in non-REM sleep. A significant reduction was also detected for the RDI before and after intervention. Both treatment success and response were met in most of the subjects. Although RDI improved in all subjects, treatment response was not achieved in 4 of 19 subjects. A specific risk factor involved in such reduced efficacy for this minority of patients was not identified.
A significant improvement in sleep efficiency was not detected, nor was a reduction in both sleep latency and wake after sleep onset between the two PSGs, which is in line with previous findings and might depend on having normal values at baseline.4 Conversely, it was noted that the subjective perception of overall sleep quality, assessed through the PSQI, improved with treatment. Although the mean ESS score was normal at baseline, but close to the pathologic threshold, a significant improvement after treatment was observed.
Overall, the MAD was well tolerated, with mild side effects, mostly confined to salivation issues and initial and transient toothache and temporomandibular joint discomfort. New-onset symptoms provoked by VLB use were very mild and limited to transient muscle rigidity, pain during yawning, and temporary bite modifications. Compliance with the device was satisfactory, with more than 70% of the subjects using it every night of the week and 80% of them all night long. The short duration and the lack of comparison with another effective MAD are the two main limitations of the study.
The efficacy results of this study are in line with data existing in the previous literature, in particular, the latest meta-analysis by Sharples and colleagues,12 which recapitulated findings from three previous main meta-analyses.13-15 All these works stated, in summary, that MADs were effective in reducing AHI, ESS score, and other measures of sleep-disordered breathing compared with conservative management, but less than CPAP. Moreover, the VLB seemed to fulfill the characteristics proposed by Ramar et al. in their clinical practice guidelines for the treatment of SAS with MAD.4 Additionally, the VLB could sustain an effective protrusion level in all study subjects.16
Side effects causing patients to discontinue use of their oral appliance are less common than side effects causing adult patients with obstructive sleep apnea to discontinue the use of CPAP and include dry mouth, excessive salivation, tooth discomfort, muscle tenderness, and jaw stiffness.17 Problems such as pain and occlusal changes have been related to discontinuation of MAD use in 7.5% to 25% of cases. A much higher percentage of tooth movement and occlusal change have been documented in longer follow-up periods (1 to 4 years).18, 19
The new VLB is a custom-made, titratable oral device made out of biocompatible materials. In comparison with other MADs already available on the market, it features some novelties. Although it is one single piece, it allows the opening of the mouth and oral respiration through frontal holes. Its design requires the presence of only four occlusal points, allowing for a direct push onto the mandibular bone (no surgery required), thus reducing the risk for occlusal changes, tooth loosening, and the development of an anterior crossbite, which seem to represent the major long-term adverse effects of oral appliances.20 In addition, the VLB can be applied to patients with a reduced number of teeth. The presence of the winglet vault, which acts as a tongue retainer, might have a double benefit. On one side, it creates a suction cavity that pulls the tongue forward. On the other side, it acts as a tongue retainer, preventing pressure of the tongue on the hard palate, which is a defensive mechanism spontaneously occurring during obstructive sleep apneas. Such vertical pressure is accompanied by the lingual vertical muscle contraction against the hard palate, which, in turn, produces an increase of the tongue volume toward its posterior portion, favoring a retrolingual occlusion. Currently, the VLB represents the first monobloc device that can be titrated.
In conclusion, the new MAD was well tolerated and effective in mild-to-moderate obstructive sleep apnea on all sleep-related PSG breathing parameters. Longer and comparative studies are needed to test the long-term tolerability of this MAD and its superiority in comparison with other MADs.
ABBREVIATIONS
AHI = apnea/hypopnea index
BMI = body mass index
CPAP = continuous positive airway pressure
ESS = Epworth Sleepiness Scale
PSQI = Pittsburgh Sleep Quality Index
RDI = respiratory distress index
REM = rapid eye movement
SAS = sleep apnea syndrome
VAS = visual analog scale
VLB = velolingual bite
VPSG = video-polysomnography
ACKNOWLEDGMENTS
The authors thank Dr. Gennaro Lucera for his essential contribution in creating the prototype of the tested device (VLB). The patent of the VLB belongs to Lucera Investments AGL. The study was partially supported by an unrestricted grant provided by Lucera Investments Sagl (Via Curti 5, 6900 Lugano, Switzerland).
REFERENCES
- Ngiam J, Balasubramaniam R, Darendeliler MA, Cheng AT, Waters K, Sullivan CE. Clinical guidelines for oral appliance therapy in the treatment of snoring and obstructive sleep apnoea. Aust Dent J. 2013;58(4):408-419.
- Campbell T, Pengo MF, Steier J. Patients' preference of established and emerging treatment options for obstructive sleep apnoea. J Thorac Dis. 2015;7(5):938-942.
- Chan AS, Sutherland K, Schwab RJ, et al. The effect of mandibular advancement on upper airway structure in obstructive sleep apnoea. Thorax. 2010;65(8):726-732.
- Ramar K, Dort LC, Katz SG, et al. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015. J Clin Sleep Med. 2015;11(7):773-827.
- Vanderveken OM, Devolder A, Marklund M, et al. Comparison of a custom-made and a thermoplastic oral appliance for the treatment of mild sleep apnea. Am J Respir Crit Care Med. 2008;178(2):197-202.
- Quinnell TG, Bennett M, Jordan J, et al. A crossover randomised controlled trial of oral mandibular advancement devices for obstructive sleep apnoea-hypopnoea (TOMADO). Thorax. 2014;69(10):938-945.
- Epstein LJ, Kristo D, Strollo PJ, Jr, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(3):263-276.
- Scherr SC DL, Almeida FR, Bennett KM, et al. Definition of an effective oral appliance for the treatment of obstructive sleep apnea and snoring: a report of the American Academy of Dental Sleep Medicine. Journal of Dental Sleep Medicine. 2014;1(1):39-50.
- Iber C, American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology, and Technical Specifications. Westchester, IL: American Academy of Sleep Medicine; 2007.
- Chiaro G, Maestri M, Riccardi S, et al. Sleep-related rhythmic movement disorder and obstructive sleep apnea in five adult patients. J Clin Sleep Med. 2017;13(10):1213-1217.
- McCormack HM, Horne DJ, Sheather S. Clinical applications of visual analogue scales: a critical review. Psychol Med. 1988;18(4):1007-1019.
- Sharples LD, Clutterbuck-James AL, Glover MJ, et al. Meta-analysis of randomised controlled trials of oral mandibular advancement devices and continuous positive airway pressure for obstructive sleep apnoea-hypopnoea. Sleep Med Rev. 2016;27:108-124.
- McDaid C, Griffin S, Weatherly H, et al. Continuous positive airway pressure devices for the treatment of obstructive sleep apnoea-hypopnoea syndrome: a systematic review and economic analysis. Health Technol Assess. 2009;13(4):iii-iv, xi-xiv, 1-119, 43-274.
- Giles TL, Lasserson TJ, Smith BJ, White J, Wright J, Cates CJ. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst Rev. 2006(1):CD001106.
- Lim J, Lasserson TJ, Fleetham J, Wright J. Oral appliances for obstructive sleep apnoea. Cochrane Database Syst Rev. 2006(1):CD004435.
- Sakamoto Y, Furuhashi A, Komori E, et al. The most effective amount of forward movement for oral appliances for obstructive sleep apnea: a systematic review. Int J Environ Res Public Health. 2019;16(18).
- Ribeiro de Almeida F, Lowe AA, Tsuiki S, et al. Long-term compliance and side effects of oral appliances used for the treatment of snoring and obstructive sleep apnea syndrome. J Clin Sleep Med. 2005;1(2):143-152.
- Okuno K, Pliska BT, Hamoda M, Lowe AA, Almeida FR. Prediction of oral appliance treatment outcomes in obstructive sleep apnea: A systematic review. Sleep Med Rev. 2015;30:25-33.
- de Almeida FR, Lowe AA, Tsuiki S, et al. Long-term compliance and side effects of oral appliances used for the treatment of snoring and obstructive sleep apnea syndrome. J Clin Sleep Med. 2005;1(2):143-52.
- Martins OFM, Chaves Jr CM, Rossi RRP, Cunali PA, Dal-Fabbro C, Bittencourt L. Side effects of mandibular advancement splints for the treatment of snoring and obstructive sleep apnea: a systematic review. Dental Press J Orthod. 2018;23(4):45-54.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication March 24, 2020
Submitted in final revised form June 30, 2020
Accepted for publication August 1, 2020
Address correspondence to: Mauro Manconi, MD, PhD, Sleep and Epilepsy Center, Neurocenter of Southern Switzerland, Civic Hospital of Lugano, Via Tesserete, 48 CH-6900 Lugano, Switzerland
DISCLOSURE STATEMENT
The authors have no conflicts of interest to disclose.APPENDICES
Appendix A |
{kind=link}
Appendix B |