Original Article 3, Issue 6.3
Long Term Patient Centered Outcomes Following Treatment with Oral Appliance Therapy for Obstructive Sleep Apnea
http://dx.doi.org/10.15331/jdsm.7088
Carolyn Cronin, DMD, MS1; Greg Essick, DDS, PhD2; Hunter Boone, BA3; Ceib Phillips, PhD, MPH1
1Department of Orthodontics, University of North Carolina School of Dentistry, Chapel Hill, NC; 2Department of Restorative Sciences / Division of Prosthodontics, University of North Carolina School of Dentistry, Chapel Hill, NC; 3Predoctoral DDS Program, University of North Carolina School of Dentistry, Chapel Hill, NC
ABSTRACT
Study Objectives:
This study assessed the long-term general and condition-specific quality of life (QOL) and perceived occlusal and functional changes of individuals with obstructive sleep apnea (OSA) who had oral appliance therapy (OAT) delivery 2 years ago or longer.
Methods:
Three validated (Calgary Sleep Apnea Quality of Life Index for OSA symptoms, Medical Outcomes Study 36-Item Short Form for general QOL, Problems with Occlusion and Function for functional and occlusal changes) and one custom questionnaire were mailed to 139 identified patients from the UNC Adams School of Dentistry Dental Sleep Clinic who met the inclusion criteria of a polysomnography diagnosis of OSA, age 18-60 years at time of OAT delivery and previous delivery of OAT 2 years ago or longer for management of OSA.
Results:
Twenty-six percent of the 139 eligible patients (n=36) returned questionnaires. Of these, 31 patients, 58% male, returned completed questionnaires. Fifty-eight percent continued to use OAT for an average of 4.9 years (standard deviation=1.78). There were no statistically significant average differences between individuals who did or did not wear oral appliances in regard to Problems With Occlusion and Function or Medical Outcomes Study 36-Item Short Form subscores (p >0.15). For the Calgary Sleep Apnea Quality of Life Index, those who wore an oral appliance reported a better perception of general health than those who discontinued OAT (p=0.02) Those who did not wear an oral appliance reported significantly greater problems with side effects from current treatment for OSA than did those who continued to use OAT (p= 0.01).
Conclusions:
Those who continued to use OAT reported QOL benefits associated with this type of therapy for managing OSA. Long-term OAT adherence is a function of patients’ perceptions of both the conferred benefits of treatment and the unfavorable treatment-induced side effects.
Keywords:
mandibular advancement device; obstructive sleep apnea; oral appliance therapy; quality of life
Citation:
Cronin C, Essick G, Boone H, Phillips C. Long Term Patient Centered Outcomes Following Treatment with Oral Appliance Therapy for Obstructive Sleep Apnea. J Dent Sleep Med. 2019;6(3)
INTRODUCTION
Obstructive sleep apnea (OSA) is a type of sleep-disordered breathing (SDB) that has gained attention in recent years because of its prevalence and associated health concerns. Obstructive sleep apnea syndrome (OSAS) is defined as having both SDB and an apnea-hypopnea index (AHI) ≥5 per hour, coupled with self-reported daytime hyper-somnolence.1 Using polysomnographic data from the Wisconsin Sleep Cohort of 602 middle-aged, working men and women, Young et al. reported that 24% of men and 9% of women had an AHI ≥ 5 per hour and that 4% and 2% respectively had OSAS, i.e., AHI >5 per hour and daytime sleepiness symptoms.1 In 2013, Peppard et al. reported an increased prevalence of SDB and OSAS in recent decades using the Wisconsin Sleep Cohort 1990s and 2007-2010 data of 1,520 middle-aged men and women who underwent sleep studies and completed the Epworth Sleepiness Scale.2 Peppard et al. reported an overall prevalence of 26% adults who had an AHI ≥ 5 per hour, and 10% with AHI ≥ 15 per hour.2 These estimates are more than double the estimates from 1993.2
OSA is a chronic disorder that requires long-term multidisciplinary management. The American Academy of Sleep Medicine (AASM) recommends the following therapies to manage the disease: behavioral therapy, continuous positive airway pressure (CPAP), oral appliance therapy (OAT), and maxillomandibular advancement surgery.3 Oral appliances, or mandibular advancement devices (MADs), advance the mandible to a protrusive position, in which the attached tongue and soft tissues follow, increasing the volume and patency of the upper airway.4 The gold standard, CPAP, has been shown to be more efficacious at reducing AHI than OAT.5–7 However, compliance has been reported to be higher with oral appliances than CPAP.5,7 The discrepancy in compliance seems to offset the increased efficacy of the CPAP, and thus OAT and CPAP show similar overall effectiveness at reducing symptoms of OSA, including improvement in quality of life (QOL) outcomes and decreasing daytime sleepiness for patients with mild, moderate, and severe OSA.8,9 However, the long-term compliance with OAT is not well documented in the literature.
Systemic objective measurements such as AHI and oxygen saturation are important for diagnosis and evaluation of the severity of OSA, but these values correlate poorly with subjective symptomology of the disease.10 Patient-centered outcomes of QOL, daytime sleepiness, cognitive status, and performance in daily activities including work can be more important to individuals with OSA.11,12 Individuals with OSA often seek initial treatment because of their subjective symptoms and the disruption that their daytime sleepiness has on daily functioning.10
Overall, there exists limited long-term data for patient-centered outcomes of QOL and perceived functional and occlusal changes for patients being treated for OSA with OAT.6,13 Understanding the long-term patient perceptions of OAT will help guide clinicians to more effective treatment of patients with OSAS. The objective of this study was to determine the patient-centered outcomes of QOL and of functional and occlusal changes following long-term use of OAT (greater than 2 years) for OSAS.
METHODS
This study was approved by the Institutional Review Board at the University of North Carolina at Chapel Hill (IRB 16-1659). Eligible participants who underwent treatment at least 2 years prior to March 2017 at the University of North Carolina at Chapel Hill Adams School of Dentistry Dental Sleep Clinic for management of OSA with a titratable MAD were identified by a systematic search of the clinic’s database. All patients were treated by a single clinician (author G.E.), who was responsible for delivering and adjusting the custom MADs. The appliance type was chosen by the clinician after consideration of the patient’s dentition, periodontal status, tongue space, history of bruxism, and third-party-payer requirements. Patients were eligible to participate if OSA had been diagnosed by a sleep physician and with polysomnography and referred to the clinic for treatment; were age 18 to 60 years at the time of oral appliance delivery; and had complete chart entries, with demographic and contact information, available. Patients with a diagnosis of central or complex sleep apnea or a congenital syndrome with or without severe retrognathia were excluded. Of the 828 potentially eligible patients from the sleep medicine database, 139 participants met the inclusion and exclusion criteria.
Demographics
Demographic data collected from the Dental Sleep Clinic database for eligible participants included: sex, age, and body mass index (BMI) at the time of delivery of the oral appliance, date of delivery of the oral appliance, OSA diagnosis, and pretreatment polysomnography results.
Description of Questionnaires
The Medical Outcomes Study 36-Item Short Form (SF-36) is a validated general health QOL questionnaire that includes 36 questions scored on a Likert scale.14,15 Health is measured on a multiitem scale in the following eight dimensions: (1) physical functioning, (2) role limitations because of physical health problems, (3) bodily pain, (4) social functioning, (5) general mental health, (6) role limitations because of emotional problems, (7) vitality, and (8) general health perceptions. The scores from the items making up each dimension were summed and then transformed to a scale of 0 to 100. Two summary scores were calculated with special algorithms and represent the Physical Component Summary and Mental Component Summary. Higher dimension and summary scores are associated with better QOL.
The Calgary Sleep Apnea Quality of Life Index (SAQLI) is a validated condition-specific questionnaire that measures QOL outcomes for patients with sleep apnea.12 The Short Form SAQLI, as used in this study, functions as an abbreviated, self-administered questionnaire in clinical settings.16 Questions 1 through 14 assessed daily functioning, social interactions, and emotional functioning and were rated on a 7-point Likert-scale from “a very large amount” to “not at all.” The average score of the 14 items was calculated and higher scores indicated better QOL. For questions 15 to 17, respondents listed up to three treatment symptoms and rated them based on degree of problem on a 7-point Likert-scale with higher scores indicating a greater problem. The final question asked respondents to rate how much of a problem (1 = no problem; 7 = a very large problem) the treatment symptoms were compared to the treatment benefits. A weighted score was then calculated by multiplying the total sum for the symptoms by a weight ranging from 0.25 (no problem compared to the benefits) to 1.0 (side effects about equal or larger than the benefits). Higher scores indicated less benefit to therapy relative to side effects.
The Problems with Occlusion and Function (PSPOF) is a custom questionnaire designed to assess patient perception of occlusal, functional, and temporomandibular joint (TMJ)-related problems.17 This questionnaire was validated as part of a National Institutes of Health grant. The questionnaire consists of 14 items rated on a 5-point Likert scale from strongly disagree to strongly agree. Six items are reverse keyed. Two domain scores were calculated to reflect a patient’s perception of occlusal problems and TMJ-related problems respectively. Domain scores were calculated as the average of the items in each domain. Higher scores indicate greater negative perception.
A questionnaire about custom oral appliances was developed to address outcomes not included in the aforementioned questionnaires. Questions related to compliance of OAT, an explanation for discontinuation of the oral appliance if applicable, and whether other sleep apnea management therapies were being used. A section of five questions adapted from the Pittsburgh Sleep Quality Index18 were included to address sleep habits and quality from the month prior to answering the questionnaires.
Distribution of Questionnaires
Eligible participants were sent an envelope containing an information sheet explaining the study, a Health Insurance Portability and Accountability Act authorization form, the four questionnaires, and an addressed, stamped envelope for return of questionnaires to the lead investigator. Informed consent was affirmed upon return of the completed questionnaires. Return of uncompleted questionnaires indicated the patient declined to participate. Three rounds of questionnaires were sent to eligible participants, the second and third rounds were only sent to nonrespondents from previous rounds. There was a 1-month grace period between rounds. Google and Yellow Page searches were used to identify current addresses for potential respondents for whom envelopes were returned undelivered. Questionnaires were completed between October 2017 and February 2018.
Statistical Analysis
Statistical analysis was performed using SAS/STAT® software version 9.4 (SAS Institute, Inc., Cary, North Carolina, United States).19 Exact unpaired t tests and Fisher exact tests were used to analyze differences in demographics and clinical characteristics between responders and nonresponders and between individuals who did or did not wear an oral appliance. Two-sided exact Wilcoxon rank-sum tests were used to analyze average differences in the subscales for SF-36, SAQLI, and PSPOF between responders who continued wearing oral appliances and those who discontinued use. Level of significance was set at 0.05.
RESULTS
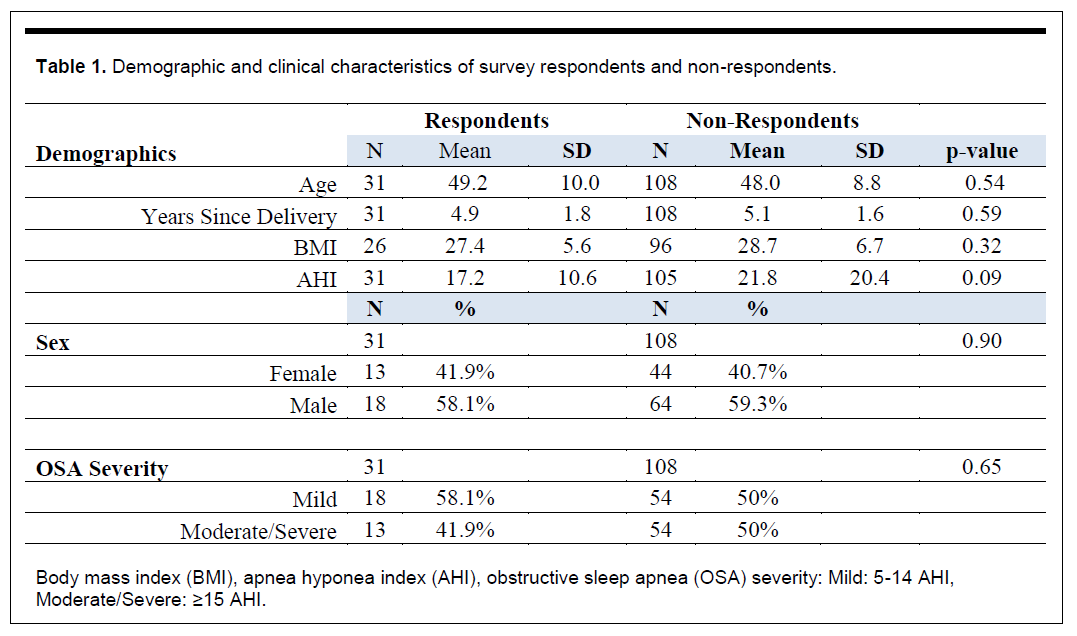
Twenty-six percent of the 139 patients (n=36) identified under the inclusion and exclusion criteria returned questionnaires: 31 consented to participate and 5 declined. An additional 25 envelopes were returned as addressee unknown. There were no statistically significant differences (p>0.09) between respondents (those who completed questionnaires n=31) and nonrespondents (n=108) when comparing age, sex, BMI, AHI at time of OAT delivery, and time since oral appliance delivery (Table 1).
Of the 31 who completed the questionnaires, 58% were male and the mean age was 49.2 years (standard deviation [SD]=10.02) (Table 1). The mean time since delivery of the oral appliance was 4.9 years (SD=1.77), the mean BMI at oral appliance delivery was 27.38 kg/m2 (SD=5.61) and the mean AHI was 17.15 per hour (SD=10.59) (Table 1). In terms of OSA severity, 58.06% had received a diagnosis of mild OSA and 41.94% as moderate to severe OSA (Table 1).
Table 1Demographic and clinical characteristics of survey respondents and non-respondents. |
{kind=link}
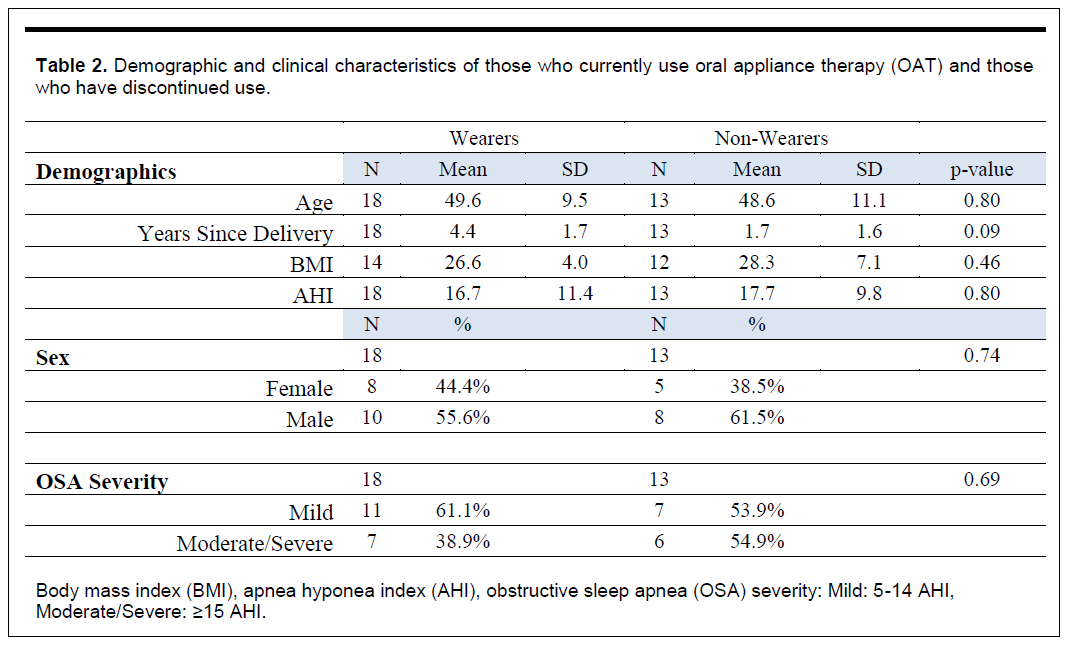
Fifty-eight percent of the respondents currently managed their OSA with OAT whereas 42% (N=13) had discontinued use of OAT. The use or nonuse of OAT was based on the response to the question “are you currently wearing your oral appliance for sleep apnea?”. The two groups did not differ significantly (p>0.09) in demographic characteristics or OSA severity (Table 2). The reasons for discontinuation of OAT included the perception that it did not appear to be working, TMJ aggravation and pain, dental and gingival discomfort, and resolution of OSA through surgery or weight loss. Of the individuals who had discontinued OAT, seven switched to CPAP, two used weight loss to control OSA, one had a bilateral sagittal split osteotomy advancement, and three currently used nothing to manage their OSA.
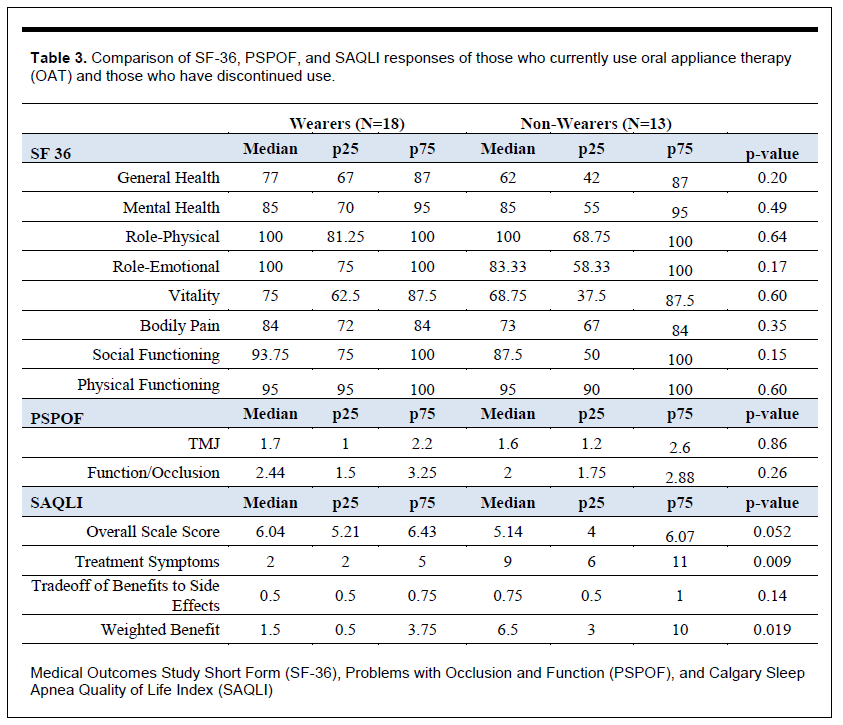
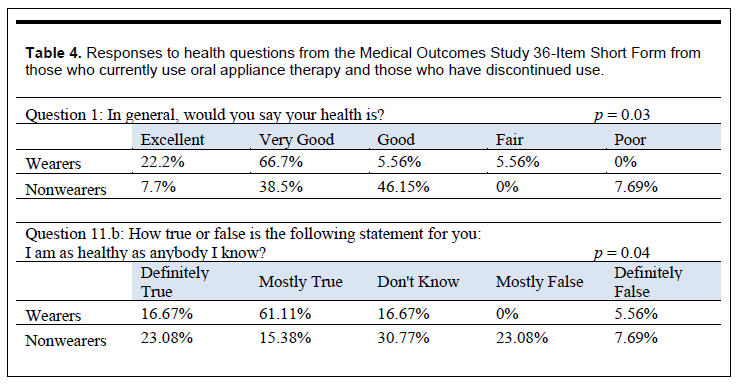
There were no statistically significant average differences between those who discontinued OAT and those who continued OAT for the subscales of SF-36: physical functioning, role limitations because of physical health problems, bodily pain, social functioning, general mental health, role limitations because of emotional problems, vitality, and general health perceptions (p>0.15) (Table 3). Although no significant differences were found in the subscales, responses to “In general, how is your health?” and “How true or false is the following statement for you: I am as healthy as anybody I know” were informative. Of those who had discontinued use of OAT, only 46.2% reported their general health as excellent or very good whereas of those who continued to use OAT, 88.9% reported their general health as excellent or very good. (Table 4). In addition, 38.45% of those who had discontinued use of OAT and 77.8% of those who continued to use OAT found the statement “I am as healthy as anybody I know” as “definitely to mostly true” (Table 4).
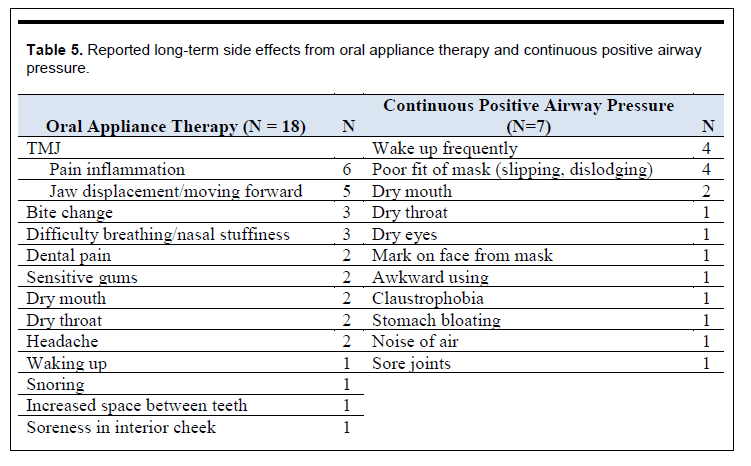
The averages for the TMJ and functional/occlusal summary scores on PSPOF between those who discontinued OAT and those who continued OAT were not statistically significantly different (p=0.86, p=0.26 respectively) (Table 3). In the Short Form SAQLI, the average difference between those who discontinued OAT and those who continued OAT for the overall scale score was marginally statistically significant (p=0.052). Those who wore an oral appliance had higher median scores than those who did not, corresponding to fewer problems with daily and emotional functioning and social interactions (Table 3). There were statistically significant average differences between those who discontinued OAT and those who continued OAT for the treatment symptom problem score (p=0.01) and for the weighted benefit-to-side-effect score (p=0.02) (Table 3). Those who discontinued OAT reported having a greater problem with side effects in the past 4 weeks from their current OSA management than those who currently used OAT to manage OSA. Considering the side effects and comparing those to the benefits of current treatment, those who discontinued OAT reported less benefit from therapy relative to side effects than those who continued OAT (Table 3) Reported side effects for OAT and CPAP treatment modalities are listed in Table 5. Forty-two percent of those who did not wear an oral appliance reported sleep quality as “fairly bad” and 58% as “fairly good” whereas 88.9% of those who did wear an oral appliance rated sleep as “fairly good” and 11% as “very good” (p <0.01). The proportion of those who did and those who did not wear an oral appliance was not significantly different in use of prescribed or over-the-counter medication as a sleep aid (p = 0.09). Approximately three fourths of those who did not and those who did wear an oral appliance (69% and 72%, respectively) reported taking medication three or more times a week.
Table 2Demographic and clinical characteristics of those who currently use oral appliance therapy (OAT) and those who have discontinued use. |
{kind=link}
Table 3Comparison of SF-36, PSPOF, and SAQLI responses of those who currently use oral appliance therapy (OAT) and those who have discontinued use. |
{kind=link}
Table 4Responses to health questions from the Medical Outcomes Study 36-Item Short Form from those who currently use oral appliance therapy and those who have discontinued use. |
{kind=link}
Table 5Reported long-term side effects from oral appliance therapy and continuous positive airway pressure. |
{kind=link}
DISCUSSION
Individuals with sleep apnea often seek initial treatment because of their subjective symptoms, which include daytime sleepiness and impaired QOL. Health-related QOL has become an important and recognized outcome measure of OSA treatment as well as an influence on the type of management strategy chosen by the patient.16,20 Furthermore, patient perception of the corresponding side effects of treatment plays an important role in patient adherence to therapy.
Understanding the QOL outcomes and perceived side effects from treatment are paramount to successful management of OSA. Unfortunately, there is not a single questionnaire that encompasses all aspects of subjective outcome measures for OSA management. For this reason, our study used three validated questionnaires to assess general (SF-36) and condition-specific (SAQLI) QOL and potential functional and occlusal side effects of OAT for patients with OSA.
After a mean 4.4 years, 58% of our respondents continued to use OAT to manage OSA. This adherence rate is similar to that in other long-term studies that showed 76% adherence after 1 year21 and 62% adherence after 4 years of OAT.22 The reasons reported for discontinuation of OAT were also consistent with other studies: perceived lack of effect, TMJ discomfort, dental and gingival discomfort, and no longer needing OAT because of resolution of OSA by weight loss or orthognathic surgery.8,21
General QOL was compared between those who wore an oral appliance and those who did not through the SF-36, and no statistically significant differences were observed between the two groups. The mean scores in the eight individual domains of the SF-36 for the group that wore an oral appliance ranged from 75 to 100, indicating positive QOL for those who wore an oral appliance in regard to their physical and social functioning, role limitations because of physical health and emotional problems, bodily pain, vitality, and general and mental health perceptions. The literature supports these results by reporting OAT is effective at improving QOL for patients with OSA, and that both OAT and CPAP show comparable improvements in QOL as measured by the SF-36.6–8,13
The Short Form SAQLI compared the condition-specific QOL between individuals who wore an oral appliance and those who did not. Those who wore an oral appliance reported less of a problem with side effects from OAT than those who did not with non-OAT therapy. Those who wore an oral appliance also perceived better QOL benefits from OAT relative to the experienced side effects than did those who did not wear an oral appliance. Literature is sparse in regard to the self-administered Short Form SAQLI and therefore this study provides novel evidence on the risk-weighted QOL benefits of OAT.
OAT-related side effects on the SAQLI included TMJ-related discomfort and jaw displacement as well as changes in bite and dental and gingival sensitivity. Reports of similar adverse effects of OAT have been documented in the literature with varying frequency and duration of effects.7,9 Studies have indicated that OA wear causes objective dental and occlusal changes in individuals, most notably decrease in overbite, overjet, and number of posterior contacts,23–27 with duration correlating to dental changes of decreased overbite.26 Perez et al. determined that after 1 year of OAT, a posterior open bite developed in 17.9% of patients, but that only 28.6% of these patients were aware of a change in bite.27 Perception of and actual dental changes are discordant. Furthermore, despite evidence that OAT leads to development of TMJ-related signs or symptoms in a small percentage of patients, it is usually transient in nature.27
The main limitation of our study was the low response rate. The two factors that likely contributed to the response rate were (1) the lack of reliable contact information in the electronic patient record for patients and (2) the fact that this was a long-term follow-up. Some patients, particularly those who were no longing wearing the oral appliance, may have been reluctant to divulge that. Our comparison of individuals who wore an oral appliance to those who had discontinued OAT was suboptimal because the group that did not wear the oral appliance was using a blend of therapeutic interventions for management of OSA, which included CPAP, bilateral sagittal split osteotomy, and weight loss, as well as some who were using nothing to manage the disease. In addition, the subjective nature of survey research is limiting, as respondents may experience recall or social desirability bias. Finally, in regard to adherence, omission of inquiry to the date of discontinuation of OAT prohibited investigation of whether discontinuation was a reflection of either short- or long-term side effects of treatment. Another limitation of the generalizability of the results of this study may be limited because all participants were treated by the same clinician in the same clinic. However, the advantage of this protocol was that none of the results could be attributed to variation in treatment protocol among clinicians or clinics.
Because OAT is considered a viable treatment for individuals with OSA who cannot tolerate CPAP or who prefer an alternate therapy,8 more individuals are using OAT to manage their OSA. As a result, the recognition of treatment-related side effects is increasing through self-report in the literature. The relationship between these dental and functional side effects and long-term adherence is still unknown. Future prospective, systematic studies are needed to clarify the effects of ongoing OAT in efforts to improve adherence and manage or mitigate these untoward effects. Studies comparing objective dental and functional side effects to perception of dental problems would provide insight to the actual effect these changes have on the individual.
OAT is reported to be as effective as CPAP in improving health-related QOL,9 but long-term studies are needed to follow up on the perceived improvements in QOL. Future studies are needed to help understand the long-term subjective symptoms so that patients’ QOL is continually managed.
ACKNOWLEDGMENTS
The authors are grateful for the support of this project from the Southern Association of Orthodontics.
REFERENCES
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med 1993;328(17):1230-1235. doi:10.1056/NEJM199304293281704.
- Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol 2013;177(9):1006-1014. doi:10.1093/aje/kws342.
- Epstein LJ, Kristo D, Strollo PJ, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med 2009;5(3):263-276.
- Holley AB, Lettieri CJ, Shah AA. Efficacy of an adjustable oral appliance and comparison with continuous positive airway pressure for the treatment of obstructive sleep apnea syndrome. Chest 2011;140(6):1511-1516. doi:10.1378/chest.10-2851.
- Phillips CL, Grunstein RR, Darendeliler MA, et al. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea: a randomized controlled trial. Am J Respir Crit Care Med 2013;187(8):879-887. doi:10.1164/rccm.201212-2223OC.
- Lim J, Lasserson TJ, Fleetham J, Wright J. Oral appliances for obstructive sleep apnoea. Cochrane Database Syst Rev 2006;(1):CD004435. doi:10.1002/14651858.CD004435.pub3.
- Schwartz M, Acosta L, Hung Y-L, Padilla M, Enciso R. Effects of CPAP and mandibular advancement device treatment in obstructive sleep apnea patients: a systematic review and meta-analysis. Sleep Breath 2017. doi:10.1007/s11325-017-1590-6.
- Ramar K, Dort LC, Katz SG, et al. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: an update for 2015. J Clin Sleep Med 2015;11(7):773-827. doi:10.5664/jcsm.4858.
- Sutherland K, Phillips CL, Cistulli PA. Efficacy versus effectiveness in the treatment of obstructive sleep apnea: CPAP and oral appliances. JDSM 2015;02(04):175-181. doi:10.15331/jdsm.5120.
- Weaver EM, Woodson BT, Steward DL. Polysomnography indexes are discordant with quality of life, symptoms, and reaction times in sleep apnea patients. Otolaryngol Head Neck Surg 2005;132(2):255-262. doi:10.1016/j.otohns.2004.11.001.
- Lau EYY, Eskes GA, Morrison DL, Rajda M, Spurr KF. The role of daytime sleepiness in psychosocial outcomes after treatment for obstructive sleep apnea. Sleep Disord 2013;2013:140725. doi:10.1155/2013/140725.
- Al-Shawwa BA, Badi AN, Goldberg AN, Woodson BT. Defining common outcome metrics used in obstructive sleep apnea. Sleep Med Rev 2008;12(6):449-461. doi:10.1016/j.smrv.2008.07.008.
- Kuhn E, Schwarz EI, Bratton DJ, Rossi VA, Kohler M. Effects of CPAP and mandibular advancement devices on health-related quality of life in OSA: a systematic review and meta-analysis. Chest 2017;151(4):786-794. doi:10.1016/j.chest.2017.01.020.
- Brazier JE, Harper R, Jones NM, et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. BMJ 1992;305(6846):160-164.
- Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992;30(6):473-483.
- Reimer MA, Flemons WW. Quality of life in sleep disorders. Sleep Med Rev 2003;7(4):335-349. doi:10.1053/smrv.2001.0220.
- Phillips C, Bennett ME. Psychological ramifications of orthognathic surgery. In: Betts NJ, Turvey TA, eds. Oral and Maxillofacial Surgery, vol 2. Philadelphia, Pennsylvania; 2000:527-530.
- Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 1989;28(2):193-213. doi:10.1016/0165-1781(89)90047-4.
- SAS Institute Inc. SAS/STAT 9.4 User’s Guide. Cary, NC: SAS Institute; 2013.
- Flemons WW. Clinical practice. Obstructive sleep apnea. N Engl J Med 2002;347(7):498-504. doi:10.1056/NEJMcp012849.
- Marklund M, Stenlund H, Franklin KA. Mandibular advancement devices in 630 men and women with obstructive sleep apnea and snoring. Chest 2004;125(4):1270-1278. doi:10.1378/chest.125.4.1270.
- Walker-Engström M-L, Tegelberg A, Wilhelmsson B, Ringqvist I. 4-year follow-up of treatment with dental appliance or uvulopalatopharyngoplasty in patients with obstructive sleep apnea: a randomized study. Chest 2002;121(3):739-746.
- Pliska BT, Nam H, Chen H, Lowe AA, Almeida FR. Obstructive sleep apnea and mandibular advancement splints: occlusal effects and progression of changes associated with a decade of treatment. J Clin Sleep Med 2014;10(12):1285-1291. doi:10.5664/jcsm.4278.
- Doff MHJ, Finnema KJ, Hoekema A, Wijkstra PJ, de Bont LGM, Stegenga B. Long-term oral appliance therapy in obstructive sleep apnea syndrome: a controlled study on dental side effects. Clin Oral Investig 2013;17(2):475-482. doi:10.1007/s00784-012-0737-x.
- Martínez-Gomis J, Willaert E, Nogues L, Pascual M, Somoza M, Monasterio C. Five years of sleep apnea treatment with a mandibular advancement device. Side effects and technical complications. Angle Orthod 2010;80(1):30-36. doi:10.2319/030309-122.1.
- Almeida FR de, Lowe AA, Sung JO, Tsuiki S, Otsuka R. Long-term sequellae of oral appliance therapy in obstructive sleep apnea patients: Part 1. Cephalometric analysis. Am J Orthod Dentofacial Orthop 2006;129(2):195-204. doi:10.1016/j.ajodo.2005.10.001.
- Perez CV, de Leeuw R, Okeson JP, et al. The incidence and prevalence of temporomandibular disorders and posterior open bite in patients receiving mandibular advancement device therapy for obstructive sleep apnea. Sleep Breath 2013;17(1):323-332. doi:10.1007/s11325-012-0695-1.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication September 20, 2018
Submitted in final revised form December 20, 2018
Accepted for publication February 5, 2019
Address correspondence to: Ceib Phillips, PhD, MPH; School of Dentistry, University of North Carolina, 3120 First Dental Bldg, CB 7450, Chapel Hill, NC 27599, Email: Ceib_phillips@unc.edu
DISCLOSURE STATEMENT
The authors have no conflicts of interest to disclose.
PDF