Original Article 3, Issue 4.2
Prevalence of Malocclusion in Children With Sleep-Disordered Breathing
http://dx.doi.org/10.15331/jdsm.6526
Benjamin T. Pliska, DDS, MS, FRCD(C)1 ; Janson Lee2 ; Neil K. Chadha, MBChB(Hons), MPHe BSc(Hons), FRCS3
1Division of Orthodontics, Faculty of Dentistry, The University of British Columbia, Vancouver, British Columbia, Canada; 2Faculty of Dentistry, The University of British Columbia, Vancouver, British Columbia, Canada; 3Division of Pediatric Otolaryngology, British Columbia Children’s Hospital, Vancouver, British Columbia, Canada
ABSTRACT
Study Objectives:
Correction of retrognathia or maxillary constriction has previously been shown to ameliorate sleep-disordered breathing symptoms in some children. The purpose of this study was to examine the prevalence of dental features that indicate a need for early orthodontic treatment in a cohort of children referred to a tertiary care center for the management of sleep-disordered breathing.
Methods:
A prospective observational cross-sectional study of 90 consecutive children aged 5 to 10 years, assessed at the otolaryngology clinic of a tertiary care hospital over a 14-month period, was performed. All subjects underwent a full clinical assessment by the attending otolaryngologist and orthodontist. Indications of orthodontic intervention and airway features were recorded.
Results:
The average patient age was 6.8 years. In terms of maxillary constriction, 15.5% of patients had a posterior crossbite, whereas 5.5% of patients had an anterior crossbite. Significant retrognathia (overjet > 7 mm) was reported in 4.8% of patients, and 8.5% of patients presented with an excessive deepbite (overbite > 90%).
Conclusions:
The prevalence of malocclusion in this cohort of children with suspected sleep-disordered breathing was not greater than what has been reported for the general population. Maxillary expansion and mandibular advancement were indicated in 15.5% and 4.8% of the sample, respectively.
Keywords:
children, obstructive sleep apnea, orthodontics, sleep apnea complications
Citation:
Pliska BT, Lee J, Chadha NK. Prevalence of malocclusion in children with sleep-disordered breathing. Journal of Dental Sleep Medicine. 2017;4(2):41–44
INTRODUCTION
Sleep-disordered breathing (SDB) is characterized by an abnormal respiratory pattern during sleep, and encompasses a spectrum of disorders that increase in severity from snoring to obstructive sleep apnea (OSA). OSA is the most significant presentation of SDB and is now recognized as a serious medical condition that affects an estimated 1.2% to 5.7% of children.1,2 Morbidity associated with OSA in children includes failure to thrive, attention deficit and hyperactivity disorder, excessive daytime sleepiness, and poor learning. There is also significant concern about long-term cardiopulmonary risks in these patients.3 The inadequate function and collapse of the upper airway during sleep is a dynamic and complex process. As such, OSA in children can result from a combination of factors including inflammation and altered neuromuscular tone of the upper airway, obesity, and hypertrophic adenoids and tonsils. As the pathophysiology of SDB in children has become better defined and understood, altered craniofacial morphology has been shown as a contributing risk factor for the disease in some children.4 The most commonly reported dentofacial characteristics in children with OSA are those associated with a long narrow face, including mandibular retrognathia, maxillary constriction, increased lower face height, and a convex profile.5–7
The correction of two specific dentofacial anomalies, maxillary constriction and mandibular retrognathia, have been previously shown to significantly improve or eliminate both objective and subjective measures of OSA in children.8–13 Villa et al.8 first described the use of a functional appliance, a monoblock-type intraoral device that positions the mandible forward, for the treatment of retrognathia associated with OSA in children. In children with transverse constriction of the maxilla, rapid maxillary expansion is indicated. This involves distraction of the midpalatal suture over a period of several weeks using an intraoral expansion appliance bonded to the upper molar teeth. Several studies have demonstrated the effectiveness of maxillary expansion in treating OSA in children both with12 and without11 tonsillar hypertrophy, and that results are persistent after a period of 24 months.13
Although orthodontics as an adjunctive form of treatment for OSA shows promise in carefully selected children with specific dentofacial abnormalities, it has not been widely adapted and the extent to which it may be applicable in everyday clinical settings has been questioned.14 A better understanding of the prevalence and severity of altered craniofacial morphology and malocclusion in this patient population will facilitate the design and implementation of interdisciplinary treatment of pediatric OSA. The aim of this study was to report on the prevalence of malocclusion and indication for specific forms of orthodontic treatment in a cohort of children referred to a tertiary care pediatric center for the management of SDB.
METHODS
Eligible subjects were 5 to 10 years of age, and referred to the otolaryngology clinic at British Columbia Children’s Hospital over a 14-month period for evaluation of SDB following an initial clinical assessment by their primary care physicians. Under an integrated multidisciplinary approach to SDB assessment in this department, referrals with a primary concern of SDB are consolidated to clinics attended by both an otolaryngologist and orthodontist. As such, during their initial visit all patients underwent a baseline interview and comprehensive clinical examination by both specialists during the same initial visit. Otolaryngologic and orthodontic clinical data were collected prospectively. The orthodontic assessment included a standardized extraoral and intraoral examination evaluating facial balance, tooth eruption, jaw morphology, and occlusion. Characteristics related to specific indications for early orthodontic intervention were recorded, including anterior crossbite (of at least one tooth), posterior crossbite (of at least one tooth), severe excess overjet (horizontal overlap of the anterior teeth > 7 mm), and severe excess overbite (vertical overlap of the anterior teeth ≥ 90%). The otolaryngology evaluation included assessment of tonsil15 and adenoid16 size as part of an assessment of nasal, nasopharyngeal, and oropharyngeal anatomy and function. For this study patients with cleft lip and/or palate, craniofacial syndromes, significant medical comorbidities, or those outside the age range of 5 to 10 years were excluded on the basis of potentially being unsuitable for any proposed orthodontic treatment.
Descriptive statistics summarized baseline characteristics, as well as orthodontic and otolaryngologic examination findings. Variables were presented as percentages and analyzed using the Pearson chi-square test or the Fisher exact test for categorical data and the Mann–Whitney U test for continuous variables. Statistical significance was assessed at P < .05. Data were analyzed with SPSS software (version 15; SPSS, Chicago, Illinois, United States). The Clinical Research Ethics Board of the University of British Columbia approved this project (#H14-01596).
RESULTS
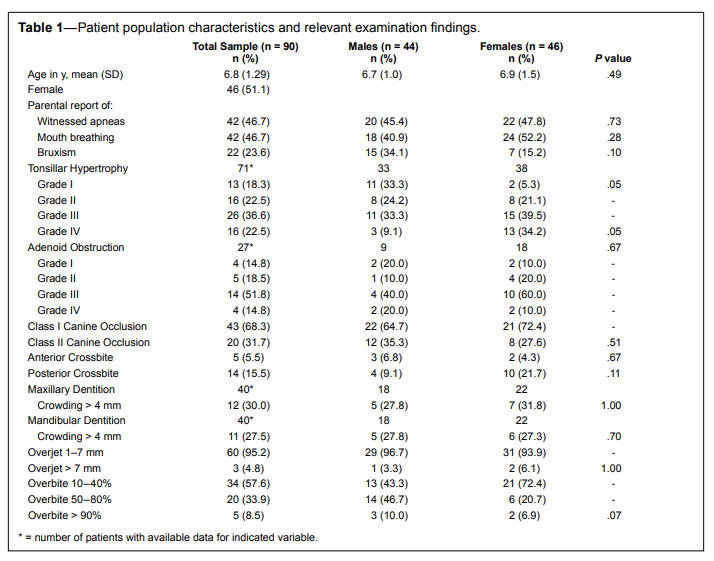
During the study period data were obtained on 90 consecutive subjects meeting the inclusion criteria. Initial patient characteristics and examination findings are shown in Table 1. The parents of 46.7% of the patients reported both a history of mouth breathing and witnessed apneas during sleep, whereas 59.1% of the patients presented with either grade 3/4 or 4/4 tonsillar hypertrophy on the Brodsky grading scale.Overall in terms of maxillary constriction, 15.5% of patients had a posterior crossbite, whereas 5.5% of patients had anterior crossbite. An increased overjet > 7 mm was reported in 4.8% of patients, and 8.5% of patients presented with an overbite of at least 90%. No statistically significant differences were observed between male and female patients for any of the variables reported, except for Brodsky grade of tonsillar hypertrophy (more boys had grade 1/4 tonsillar hypertrophy than girls [33.3% versus 5.3%], and more girls had grade 4/4 tonsillar hypertrophy than boys [34.2% versus 9.1%])
The outcome of the clinical consultation in terms of patient treatment was varied and based on severity of sleep-related symptoms, clinical findings, and parental concerns. A polysomnography study was scheduled for 7.3% of the patients and 25.5% of patients were scheduled for adenotonsillectomy. A course of intranasal steroid therapy was prescribed for 32.7% of patients, and 34.3% of the patients were asked to follow up with their family physicians, having no specific indication for medical treatment at the time of assessment mainly due to symptoms improving since the time of initial referral. Patients presenting with a malocclusion requiring early orthodontic intervention were referred for treatment to a hospital or community-based orthodontist.
Table 1Patient population characteristics and relevant examination findings. |
{kind=link}
DISCUSSION
The current study reports the prevalence of malocclusion in a cohort of children referred to a tertiary care center for evaluation of suspected SDB. Altered craniofacial morphology is now established as an etiological factor in pediatric OSA, and the need to investigate this population and the efficacy of orthodontic treatment has been recently emphasized.17 Although adenotonsillectomy has and will likely remain the gold-standard treatment for pediatric OSA, as a recent large multicenter study has shown,18 a significant subset of children will not be adequately treated by surgery alone, making it desirable to find appropriate adjunctive or alternative treatments.
The correction of two specific dentofacial malocclusions, retrognathia and maxillary constriction, has been described to improve measures of OSA in children. In order to facilitate the design and implementation of future studies on orthodontic treatment of pediatric OSA, with the current study we report how often this treatment may be applicable to patients who are also most likely to benefit. No differences were found between the sexes with respect to the prevalence of any dentofacial characteristics, consistent with previous reports. The excess horizontal overlap, or overjet of the anterior teeth, results from a sagittal deficiency of the mandible and is an indication for orthodontic mandibular functional advancement. We defined the need to advance the mandible by the presence of an overjet of at least 7 mm, and 4.8% of our population fit this rigid criterion. In the general population in a similar age group, the prevalence of this excess of overjet ranges from 3.7% to 13.2%.19–21
A transverse deficiency of the maxilla often manifests as a crossbite of the posterior dentition, and can include primary or permanent molars, as well as canines and premolars if severe. The posterior crossbite can present either unilaterally or bilaterally and is an indication for orthodontic maxillary expansion. In the current study a posterior crossbite was found in 15.5% of patients, with no differences in prevalence between the sexes. Within the general population of a similar age group, this type of malocclusion has a reported prevalence ranging from 7.7% to 23.3%.19–22 The prevalence of other specific forms of malocclusion that indicate a need for early orthodontic treatment included anterior crossbite (5.5%) and severe anterior deepbite (8.5%). These orthodontic findings have been reported to occur in 9.5% to 22.8%20–22 and 5.2% to 18.1%20,22 of the general pediatric population, respectively.
It should be clear from the data presented that the majority of children presenting for management of suspected obstructive sleep issues will not have any obvious signs of altered craniofacial morphology, at least not in terms of readily identifiable indications for early orthodontic treatment. Although statistically significant differences in cephalometric variables have been reported among children with and without OSA,23,24 these differences are not large (often < 2°) and may therefore be of limited clinical significance. Similarly, any subtle differences in dentofacial morphology and occlusion due to differences in SDB severity may have been missed by the rigid criteria (> 7 mm overjet, posterior crossbite) orthodontists use as an indication for early treatment. The challenges of clearly identifying children with OSA based on clinical assessments alone have also been reported in the medical literature.25 Recently, data from a large multicenter trial also demonstrated that evaluation of clinical parameters such as tonsillar size and palate position by physical examination provides very limited information on OSA severity in prepubertal children.26 Therefore, it would be prudent for clinicians to screen for symptoms of the disease in all patients and not just those who present with the classic associated features of adenoid facies. Should positive responses to a medical history form, interview, or questionnaire27 lead to suspicion of an obstructive sleep disorder, the patient can then be referred the appropriate pediatric sleep specialist for diagnosis and management.
The data presented in this study have some limitations, most notably that the patient population was suspected of SDB following clinical evaluation by a primary care physician and history described by a parent or caregiver. It is possible that the referring primary care physicians have varying experiences and sensitivities to SDB problems in children, thus adding to the variability of the sample. This is in contrast to an objective diagnosis of OSA that requires polysomnography and would clearly strengthen the current findings. Because more than onethird of patients were referred back to their family physicians because of no specific treatment being required or inconclusive clinical history, it is clear that this population represents a very wide range of SDB symptoms. However, we think this population is reflective of a typical clinical setting for a regional sleep center, and should orthodontic treatment be applied to pediatric patients with OSA it would be best discussed in conjunction with the other planned interventions. Patient ethnicity is not routinely recorded at our institution and is missing from the current data. Because the incidence of some forms of malocclusion is known to vary among ethnicities, our results may differ from those of other centers. Observationally we can report that this sample largely reflects the greater Vancouver population as a whole, which is very ethnically diverse, with large percentages of Asian and Southeast Asian in addition to Caucasian patients. An additional limitation of the data is the lack of information on patient weight or body mass index. Obesity is a known confounder in OSA in both children and adults; therefore, the potential influence of body weight or obesity on the current findings is unclear.
CONCLUSIONS
A significant prevalence of skeletal malocclusion was not found in this pediatric population with sleep-disordered breathing.REFERENCES
2. Bixler EO, Vgontzas AN, Lin H-M, et al. Sleep disordered breathing in children in a general population sample: prevalence and risk factors. Sleep. 2009;32(6):731–736.
3. Kheirandish-Gozal L, Etzioni T, Bhattacharjee R, et al. Obstructive sleep apnea in children is associated with severity-dependent deterioration in overnight endothelial function. Sleep Med. 2013;14(6):526–531.
4. Ikävalko T, Tuomilehto H, Pahkala R, et al. Craniofacial morphology but not excess body fat is associated with risk of having sleepdisordered breathing—the PANIC Study (a questionnaire-based inquiry in 6–8-year-olds). Eur J Pediatr. 2012;171(12):1747–1752.
5. Zucconi M, Caprioglio A, Calori G, et al. Craniofacial modifications in children with habitual snoring and obstructive sleep apnoea: a casecontrol study. Eur Respir J. 1999;13(2):411–417.
6. Huynh NT, Morton PD, Rompré PH, Papadakis A, Remise C. Associations between sleep-disordered breathing symptoms and facial and dental morphometry, assessed with screening examinations. Am J Orthod Dentofacial Orthop. 2011;140(6):762–770.
7. Pirilä-Parkkinen K, Pirttiniemi P, Nieminen P, Tolonen U, Pelttari U, Löppönen H. Dental arch morphology in children with sleepdisordered breathing. Eur J Orthod. 2009;31(2):160–167.
8. Villa MP, Bernkopf E, Pagani J, Broia V, Montesano M, Ronchetti R. Randomized controlled study of an oral jaw-positioning appliance for the treatment of obstructive sleep apnea in children with malocclusion. Am J Respir Crit Care Med. 2002;165(1):123–127.
9. Schütz TCB, Dominguez GC, Hallinan MP, Cunha TCA, Tufik S. Class II correction improves nocturnal breathing in adolescents. Angle Orthod. 2011;81(2):222–228.
10. Zhang C, He H, Ngan P. Effects of twin block appliance on obstructive sleep apnea in children: a preliminary study. Sleep Breath. 2013;17(4):1309–1314.
11. Pirelli P, Saponara M, Guilleminault C. Rapid maxillary expansion in children with obstructive sleep apnea syndrome. Sleep. 2004;27(4):761–766.
12. Villa MP, Malagola C, Pagani J, et al. Rapid maxillary expansion in children with obstructive sleep apnea syndrome: 12-month follow-up. Sleep Med. 2007;8(2):128–134.
13. Villa MP, Rizzoli A, Miano S, Malagola C. Efficacy of rapid maxillary expansion in children with obstructive sleep apnea syndrome: 36 months of follow-up. Sleep Breath. 2011;15(2):179–184.
14. Tsuiki S, Maeda K, Inoue Y. Rapid maxillary expansion for obstructive sleep apnea: a lemon for lemonade? J Clin Sleep Med. 2014;10(2):233.
15. Brodsky L. Modern assessment of tonsils and adenoids. Pediatr Clin North Am. 1989;36(6):1551–1569.
16. Parikh SR, Coronel M, Lee JJ, Brown SM. Validation of a new grading system for endoscopic examination of adenoid hypertrophy. Otolaryngol Head Neck Surg. 2006;135(5):684–687.
17. Marcus CL, Brooks LJ, Draper KA, et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012;130(3):e714–e755.
18. Marcus CL, Moore RH, Rosen CL, et al. A randomized trial of adenotonsillectomy for childhood sleep apnea. N Engl J Med. 2013;368(25):2366–2376.
19. Tausche E, Luck O, Harzer W. Prevalence of malocclusions in the early mixed dentition and orthodontic treatment need. Eur J Orthod. 2004;26(3):237–244.
20. Shalish M, Gal A, Brin I, Zini A, Ben-Bassat Y. Prevalence of dental features that indicate a need for early orthodontic treatment. Eur J Orthod. 2013;35(4):454–459.
21. Karaiskos N, Wiltshire WA, Odlum O, Brothwell D, Hassard TH. Preventive and interceptive orthodontic treatment needs of an innercity group of 6- and 9-year-old Canadian children. J Can Dent Assoc. 2005;71(9):649.
22. Bittencourt M, Machado AW. An overview of the prevalence of malocclusion in 6 to 10-year old children in Brazil. Dental Press J Orthod. 2010;15(6),113–122.
23. Katyal V, Pamula Y, Martin AJ, Daynes CN, Kennedy JD, Sampson WJ. Craniofacial and upper airway morphology in pediatric sleepdisordered breathing: systematic review and meta-analysis. Am J Orthod Dentofacial Orthop. 2013;143(1):20–23.
24. Flores-Mir C, Korayem M, Heo G, Witmans M, Major MP, Major PW. Craniofacial morphological characteristics in children with obstructive sleep apnea syndrome: a systematic review and metaanalysis. J Am Dent Assoc. 2013;144(3):269–277.
25. Brietzke SE, Katz ES, Roberson DW. Can history and physical examination reliably diagnose pediatric obstructive sleep apnea/ hypopnea syndrome? A systematic review of the literature. Otolaryngol Head Neck Surg. 2004;131(6):827–832.
26. Mitchell RB, Garetz S, Moore RH, et al. The use of clinical parameters to predict obstructive sleep apnea syndrome severity in children: the Childhood Adenotonsillectomy (CHAT) study randomized clinical trial. JAMA Otolaryngol Head Neck Surg. 2015;141(2):130–136.
27. De Luca Canto G, Singh V, Major MP, et al. Diagnostic capability of questionnaires and clinical examinations to assess sleep-disordered breathing in children: a systematic review and meta-analysis. J Am Dent Assoc. 2014;145(2):165–178.
ACKNOWLEDGMENTS
The authors acknowledge Julie Pauwels, for her work as Clinical Research Coordinator for this study.SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication August 4, 2016
Submitted in final revised form November 30, 2016
Accepted for publication January 28, 2017
Address correspondence to: Benjamin T. Pliska, DDS, MS, FRCD(C), UBC Faculty of Dentistry, 2199 Wesbrook Mall, Vancouver, BC, V6T 1Z3, Canada; Tel: 604-822-7237; Fax: 604-822-3562; Email: pliska@ dentistry.ubc.ca
DISCLOSURE STATEMENT
All work related to this study was performed at British Columbia Children’s Hospital, Vancouver, British Columbia, Canada. This work was supported with funding from a University of British Columbia Faculty of Dentistry Undergraduate Student Research Award, and an American Association of Orthodontists Foundation Biomedical Research Award. The authors have indicated no financial conflicts of interest.