Original Article 2, Issue 9.4
Dental Sleep Medicine Among Dental Practitioners: Preliminary Findings From the National Dental Practice-Based Research Network
http://dx.doi.org/10.15331/jdsm.7264Maria Therese Galang-Boquiren, DMD, MS, MBA1; Rahma Mungia, BDS, MSc, DDPHRCS2; Veerasathpurush Allareddy, BDS, MBA, MHA, PhD, MMSc1; Yasmarie Santana-Rivera, BS3,4; Gregg H. Gilbert, DDS, MBA5
1University of Illinois Chicago, Chicago, Illinois, USA, 2University of Texas Health Science Center, San Antonio, Texas, USA, 3University of Puerto Rico Medical Sciences Campus, San Juan, Puerto Rico, USA, 4The National Practice-Based Research Network Collaborator Group, 5University of Alabama at Birmingham, Birmingham, Alabama, USA
ABSTRACT
Objectives/Introduction:
Dental sleep medicine (DSM) focuses on oral appliance therapy (OAT) to manage sleep-disordered breathing (SDB), including obstructive sleep apnea (OSA). This brief poll aimed to assess the interest and practices of dental practitioners in DSM. Currently, data are lacking regarding how DSM practices function in the clinical setting. Therefore, identifying knowledge gaps in DSM among dental practitioners may improve patient outcomes.
Methods:
A preliminary brief questionnaire (“Quick Poll”) on DSM was conducted through the National Dental Practice-Based Research Network (Network) members (n=311). The poll contained five questions about DSM.
Results:
Results showed that 66% of practitioners have involvement in DSM patient care. A total of 44% of practitioners who answered the Quick Poll do not screen for snoring or SDBs. Approximately 40% of respondents are either interested in continuing education courses on the topic or had already taken multiple courses on DSM. The top three topics of DSM research of interest to practitioners were various DSM practice models, response to OAT, and compliance with OAT.
Conclusions:
Network dental practitioner respondents face challenges regarding the treatment of SDBs. Despite these challenges, most practitioners are interested in engaging in DSM. Based on these preliminary findings, there are informational needs regarding the current state of clinical care, side effects of OAT, choice of OAT, titration protocols, and patient outcomes.
Clinical Implications:
MAD should be selected on an individual basis, according to patient preference and trained dentist recommendation, as the design did not affect the effectiveness in terms of AHI improvement.
Keywords:
dental sleep medicine (DSM), sleep-disordered breathing (SDB), obstructive sleep apnea (OSA)
Citation:
Galang-Boquiren MT, Mungia R, Allareddy V, Santana-Rivera Y, Gilbert GH. Dental sleep medicine among dental practitioners: Preliminary findings from the National Dental Practice-Based Research Network. J Dent Sleep Med. 2021;9(4)
INTRODUCTION
As the profession of dentistry has gradually expanded its scope of practice, growth in the interest in dental sleep medicine (DSM) has emerged. DSM was defined in 2008 by the American Academy of Dental Sleep Medicine (AADSM) as “an area of dental practice that focuses on the use of oral appliance therapy (OAT) to treat sleep-disordered breathing (SDB), including snoring and obstructive sleep apnea (OSA)”.1 Eight years later an alternate definition was proposed by Lobbezoo et al. defining DSM as “the discipline concerned with the study of the oral and maxillofacial causes and consequences of sleep-related problems”.2 Some of these sleep-related problems include, and are not limited to, orofacial pain, gastroesophageal reflux disorder, bruxism, insomnia, narcolepsy, xerostomia, and manifestations including sleep disturbance or excessive sleepiness.3
Men have a higher prevalence (49.7%) of moderate to severe SDB, according to a 2015 study by Heinzer et al.4 One of the most prevalent sleep-related breathing disorders is OSA5,6 which is commonly described as a cessation of breathing during sleep as a result of airway collapse7
consisting of a repetitive obstruction of the upper airway that causes apneas.8 Over the past few years, the prevalence of OSA has been exponentially increasing, with estimates ranging from 9% to 38% of the global population.9 An estimated 54 million Americans are affected10 by OSA, with 80% of the cases remaining undiagnosed.11 This can lead to severe economic costs, including motor vehicle accidents, comorbidities, substance, tobacco, and alcohol abuse, decreased productivity at work, reduced quality of life, and stress on interpersonal relationships.12,13 These undiagnosed cases cost the United States approximately $149.6 billion in 2015.11 Thus, there is a need for treatment to reduce the health burden associated with untreated OSA.5
The most significant gaps in the diagnosis and treatment of SDB are signs and symptoms recognition. Bian, in a 2004 survey (n=192), observed that 58% of general dentists did not know the signs and symptoms associated with OSA, and approximately half did not know about the use of OAT to manage OSA.14 Moreover, almost all respondents agreed that OSA is a life-threatening illness in that same study.14 A survey conducted in 1997 by Loube and Strauss (n=124) concluded that the lack of standardization in the use of oral appliances for OSA treatment was problematic.15 These results suggest a deficiency in the education received about DSM, including during predoctoral and postdoctoral studies.
A study in 2003 by Ivanhoe et al. reported that approximately 42% of the US dental schools that responded to their survey teach about upper airway disorders but only dedicate approximately 2.5 hours to the topic.16 The remaining 58% of responding schools in this study stated that they had no available curriculum time to teach about sleep disorders.16 A study by Karimi et al. utilized a survey questionnaire sent out to North American dental schools, 37% (28 of 76) of which responded. Of these 28 schools, 12 reported having a dental sleep medicine clinic, and among those, 7 schools faced challenges in implementing a dental sleep medicine clinic due to issues with administration, space, funds, and understaffing.17
The “Quick Poll” informal survey discussed in this paper aimed to collect descriptive data about DSM among members of the National Dental Practice-Based Research Network (Network). Specific topics included the assessment, diagnosis, and treatment of DSM. The mission of the Network is to improve oral health by conducting dental practice-based research and serving dental professionals and their patients through education and collegiality.18 One of the ways that the network uses to engage its members is through Quick Polls. The Network, through its newsletter, sends out these Quick Polls to address different topics and interests among its members. The Network can establish a baseline to gauge its members’ interest in various topics from the data collected to expand further research and better understand the challenges its members face.
METHODS
In February 2021, a Quick Poll on DSM was conducted by the Network. “Quick Polls” are a simple, low-cost means to engage network members in clinical topics of interest. We expect the findings from these preliminary polls will inform the design of a subsequent, rigorously designed, full-scale clinical study that the network might conduct later. Network members are sent a single invitation to complete the poll. No follow-up of nonrespondents is done because all data are captured in anonymous fashion, making it impossible to identify who responded. The Network has conducted more than 50 Quick Polls based on topics in which practitioners have expressed interest. Although responses to Quick Polls are not linked to members’ identifiers, they offer an easy way for members to give input about ideas for Network studies. Practice-based research network (PBRN) study ideas often come from the practitioners in a bottom-up approach to study selection.19 Based on current knowledge, the National Dental PBRN is the only Network that successfully uses Quick Polls to gauge interest in future study topics.
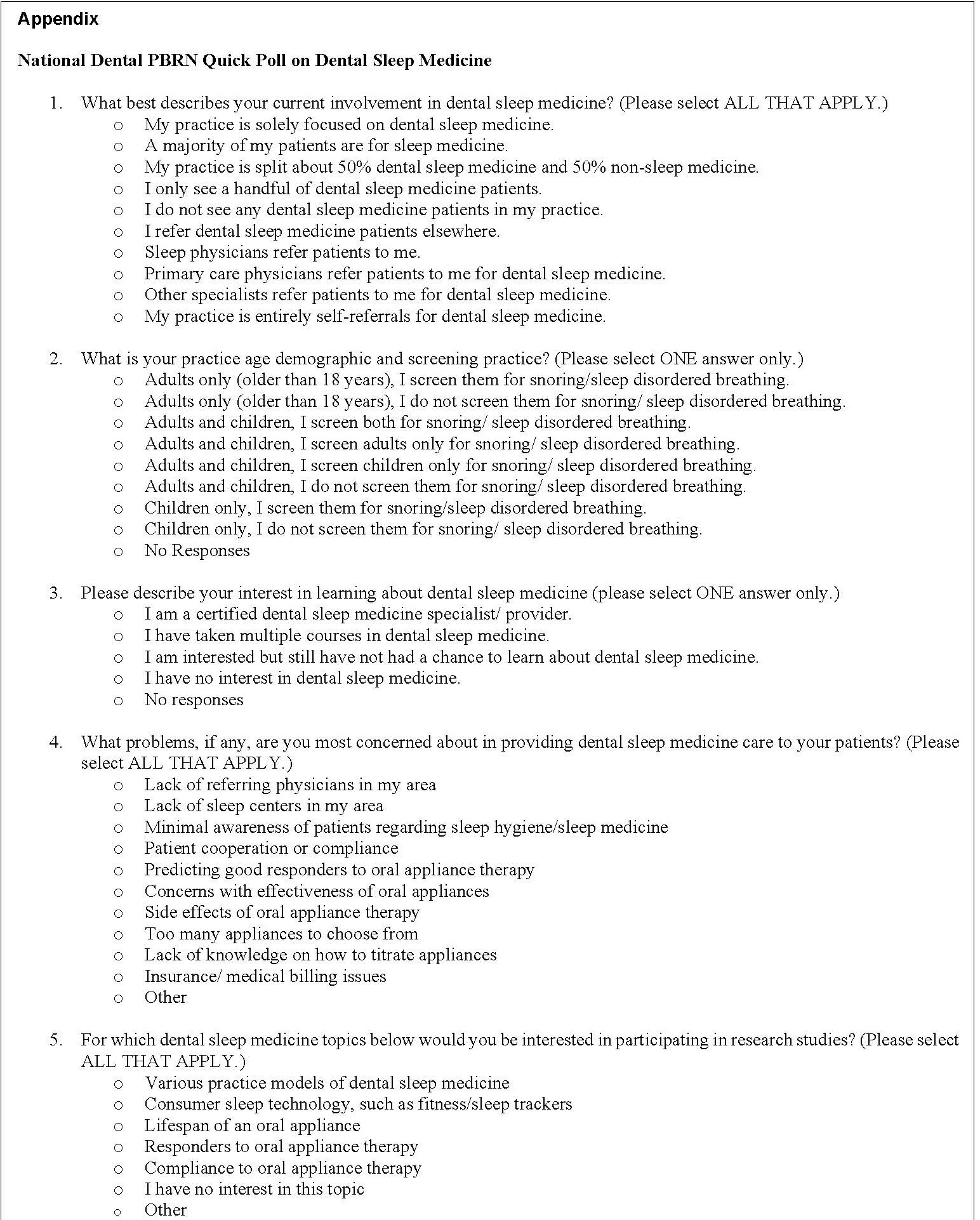
The PBRN “Quick Poll” goal was to compile a sense of members’ involvement in DSM, using a five-question questionnaire (see Appendix) sent through the Network’s newsletter, using the following criteria:
- Current involvement in DSM
- Practice demographics and screening practice
- Interest in DSM
This Quick Poll was sent to the Network’s active members (5,104 at the time of the Poll), of whom approximately 20% are not clinically active dentists or dental hygienists (this includes office staff, students, residents, retired or no longer practicing practitioners, and others).
The study conforms to recognized standards of the US Federal Policy for the Protection of Human Subjects. The Institutional Review Board approval was obtained from the University of Alabama at Birmingham (IRB-040903006, The National Dental PBRN Administrative & Resource Center).
RESULTS
From all the Network’s members who received the newsletter, a total of 311 responded to the Quick Poll (6%).
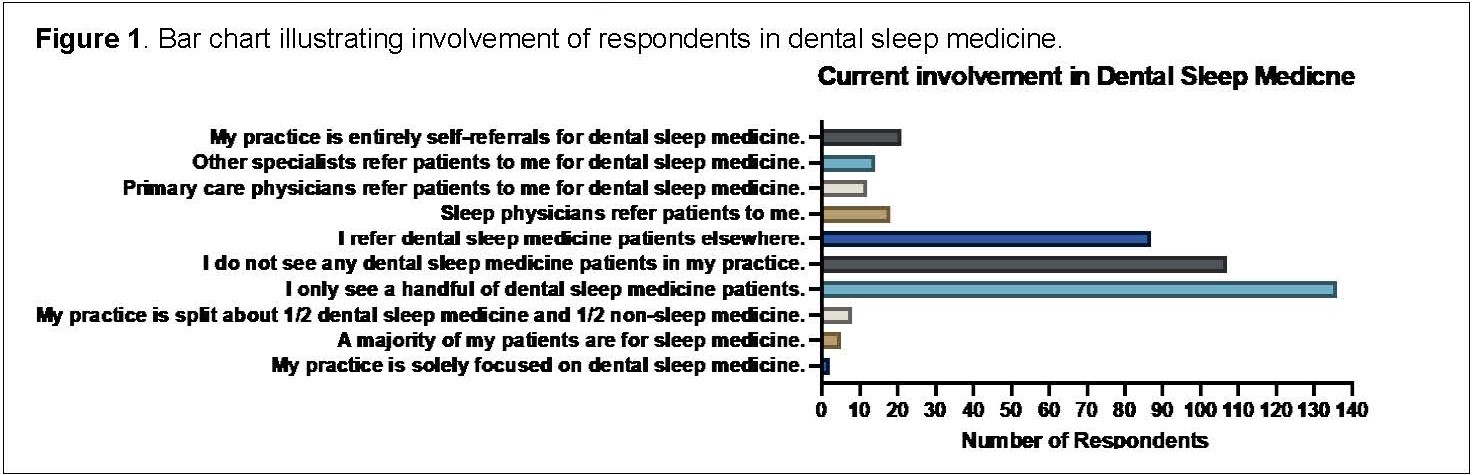
Results from the Quick Poll suggest that 66% of the respondents have some type of involvement in DSM, from which only 2 respondents' practice is solely focused on DSM. Moreover, approximately one-third of the respondents do not provide any DSM service. Interestingly, 4% of respondents state that they receive patients referred from primary care physicians for DSM, whereas 6% receive patients referred by sleep physicians (Figure 1).
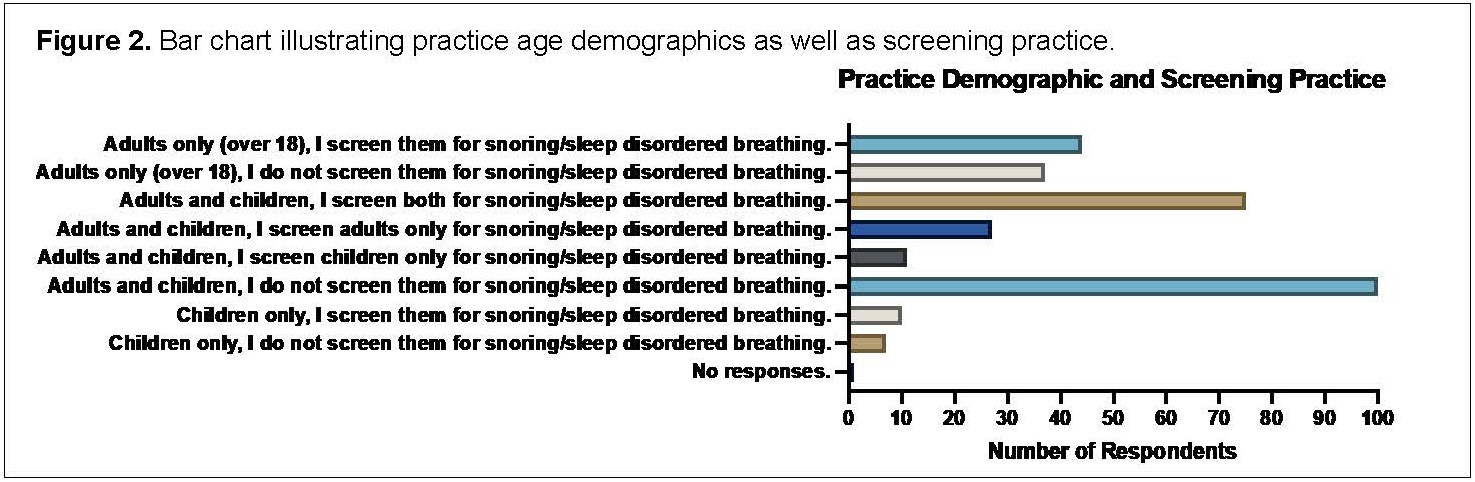
Most respondents (68%) see both adults and children in their practice but only one-fourth (24%) screen for SBD, leaving approximately one-third (32%) who do not do any form of screening for SBD. Of the practices that saw only adults, 54% screen for SDB. For practices that only see children (17 respondents), approximately 60% screen for SDB (Figure 2).
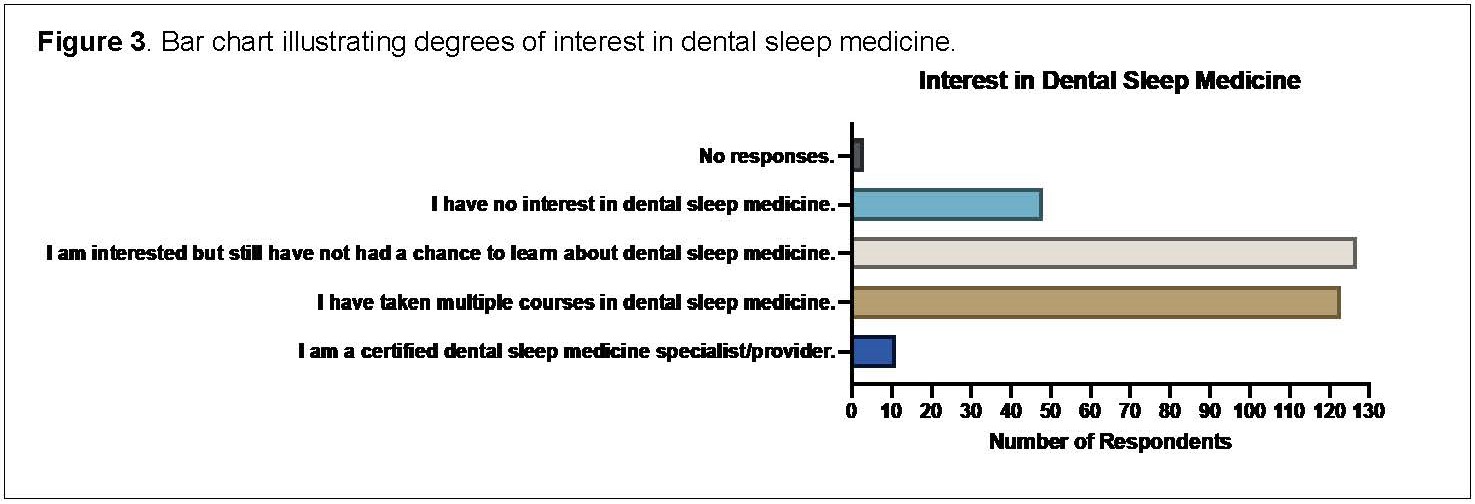
In gauging interest in the topic of DSM, the Quick Poll found that 41% of respondents were quite interested but had not taken continuing education courses on the topic. Another 39% have already taken multiple courses on DSM. A few (15%) were not interested in DSM, and only 11 respondents were already certified DSM specialists. DSM is not a recognized specialty by the American Dental Association; however, AADSM continuing education courses are recognized by the American Dental Association Continuing Education Recognition Program20 (Figure 3).
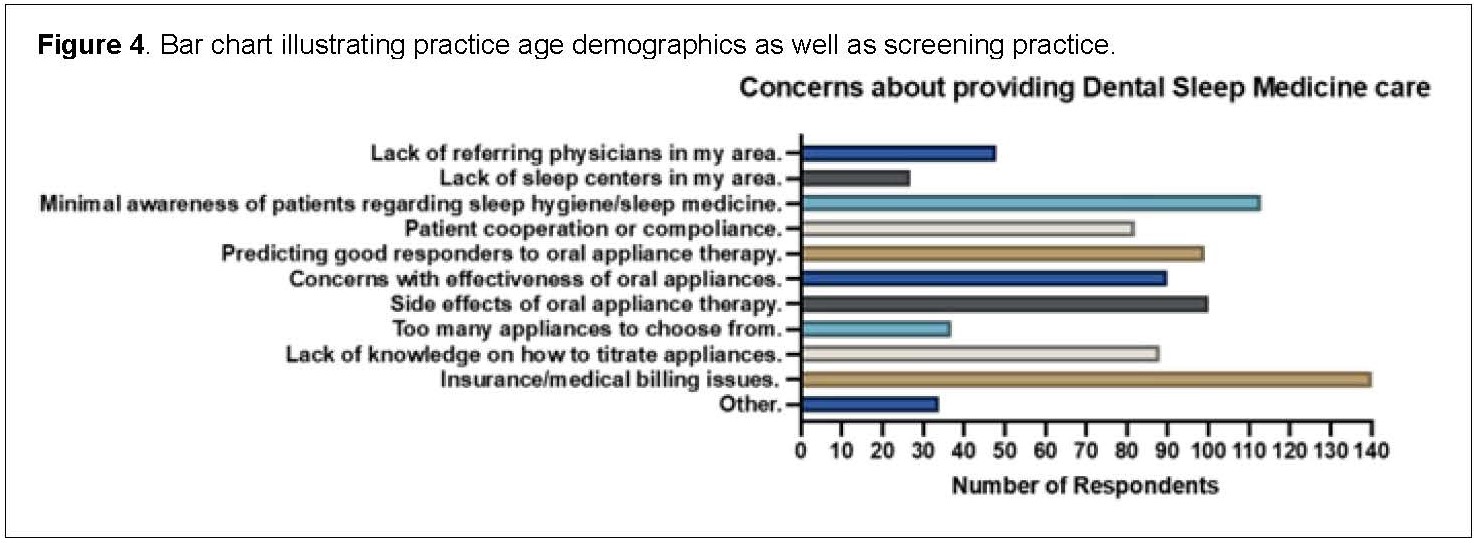
The Quick Poll attempted to identify the concerns of practitioners regarding providing DSM services. Responders could choose multiple concerns they found applicable in their practice setting. The top five most common issues identified were: insurance/ medical billing issues (47%), lack of patients’ knowledge on sleep hygiene/ sleep medicine (38%), side effects of OAT (33%), predicting good responders to OAT (33%), and concerns with the effectiveness of oral appliance (30%) (Figure 4).
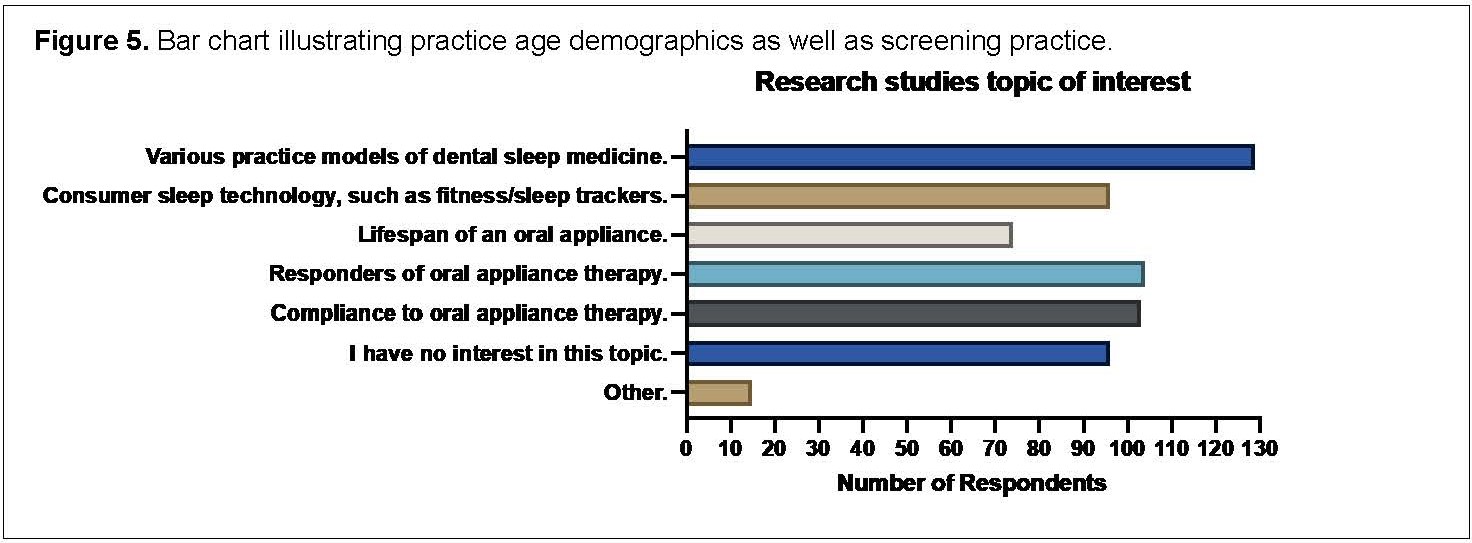
Finally, the practitioners were asked about topics of interest for PBRN studies related to DSM. Most were interested in DSM research, and the top three topics were: various practice models of dental sleep medicine (42%), responders to OAT (34%), and compliance with OAT (33%) (Figure 5).
Figure 1Bar chart illustrating involvement of respondents in dental sleep medicine.. |
{kind=link}
Figure 2Bar chart illustrating practice age demographics as well as screening practice. |
{kind=link}
Figure 3Bar chart illustrating degrees of interest in dental sleep medicine. |
{kind=link}
Figure 4Bar chart illustrating practice age demographics as well as screening practice. |
{kind=link}
Figure 5Bar chart illustrating practice age demographics as well as screening practice. |
{kind=link}
Appendix(more...) |
{kind=link}
DISCUSSION
The Quick Poll results suggest that dental practitioners face challenges regarding screening and treatment of patients with OSA. Despite these challenges, most respondents are interested in engaging in DSM. Currently, there is only one AADSM-recognized fellowship program in the United States that focuses on DSM offered to postdoctoral dental students.21 Despite the lack of formal academic-based training, organizations such as the AADSM provide many programs to develop DSM expertise, and there are many opportunities in the field, including collaboration with sleep physicians by helping to identify referring patients at risk for SDB, especially OSA. Another untapped opportunity is training dental students who are receiving little to no education on the know-how and how-to of screening for sleep-related breathing disorders.17
The dental office is an ideal setting for identifying such patients and potentially providing treatment once a sleep physician accurately diagnoses the patient. Providing education for dentists to screen for OSA is a first step in allowing more dentists to become part of the treatment process. Given that insurance/medical billing issues were the number one cited concern, some research focusing on reducing insurance/medical billing barriers would be recommended. Based on the findings of this PBRN survey, there are informational needs that may be met with further research regarding the current state of clinical care, including factors that affect OAT, specifically appliance choice, titration protocols, and patient outcomes. In addition, there are no published guidelines that clinicians and dentists can refer to for the management of side effects associated with OAT.22 Individual lectures are the primary source of information available to clinicians, which may lead to bias; as such, these knowledge gaps truly need to be addressed. 22
This study’s findings are in line with previous related research. Although Loube and Strauss15 and Bian14 both conducted formal surveys on OAT for OSA in contrast to the more informal Quick Poll, the results obtained in the current study were very similar, reflecting the gaps in knowledge that then translate to practice. This is especially important to consider when dentists have much to offer in terms of potentially successful alternative treatment to OSA's public health concern. Some common findings that emerged from Bian’s results were lack of familiarity with the upper airway, lack of knowledge of signs and symptoms of OSA, and mandibular advancement treatment or OAT.14 In addition, Bian’s survey respondents were more similar to this current study because surveys were sent to general dentists, in contrast to the study by Loube and Strauss, which targeted members of the Sleep Disorders Dental Society.15
A few similar studies were identified upon expanding the search to European counterparts. Vuorjoke-Ranta and colleagues surveyed general dentists and dental specialists in Helsinki, Finland (n=134) regarding their knowledge of OSA and their willingness to screen for and treat the condition.23 They found that the level of knowledge is crucial for successful treatment of OSA and highlight the importance of a collaboration between the dentist and sleep physician.23
In 2021, Leigh and colleagues also set out to understand the knowledge in sleep-related breathing disorders among general dental practitioners in the United Kingdom.24 A total of 152 general dentists responded to their survey, which revealed findings that slightly differed from those of the current study in that more than half of the respondents actually screen for SDB in their dental practices. Leigh et al. found that UK general practitioners have a theoretical knowledge of SBDs, but this may be due to their interest in the topic.24 Agreeing with the findings in the current study, their respondents believed that more information is needed regarding dental sleep medicine for general dentists.24 It was also recognized that there was a deficiency in predoctoral education about upper airway disorders.24
Moreover, Berggren et al. focused on patient care for patients with risk of oral health problems linked to OSA.25 This study was a qualitative focus group interview of dentists and hygienists with experience in the Swedish Dental Public Service. Once again, the experts they interviewed agreed that coincide with other studies, that more education about OSA should be imparted to dental professionals.25
Although none of the European studies revealed barriers in terms of medical insurance etc., the recurring theme was clear. Together, they demonstrate that there is a gap to be filled regarding education, predoctoral, and postdoctoral, when it comes to upper airway disorders, specifically OSA, as it relates to DSM.
In November 2016, the Network did a Quick Poll on OSA, with 420 participants. In this Quick Poll, preliminary data found that one-third of dental professionals do not screen for OSA, and approximately 40% ask about sleep apneas in their questionnaires. From these preliminary data, fewer than half of the respondents screened for sleep apnea, with one-fifth of the respondents waiting for their patients to bring it up. Based on our latest poll, this problem still exists, as OSA is still the most prevalent sleep-related breathing disorder with a significant number of undiagnosed cases. Therefore, collaboration between dental professionals and physicians is key in diagnosing and treating OSA. Although currently the standard treatment of OSA is continuous positive airway pressure, OAT shows comparable outcomes and better compliance. If left untreated, OSA may result in poor long-term health outcomes.
This study has some limitations. The average response rate from previous Networks’ Quick Polls has been approximately 9%. In this study, a 6% response rate was obtained. The observed decrease in response rate may be partially attributed to the COVID-19 pandemic. Also, this poll is directed at a niche dental professional population interested in the practice of DSM, which could cause selection bias because perhaps persons were much more likely to have responded if they were interested in the topic. Furthermore, the results presented here are merely preliminary data highlighting the huge knowledge gap in DSM, as only one-third of the 311 participants in the current study reported exposure to DSM.
A low response rate is seen when comparing the current study limitations with previous studies. Although focused on a particular state, Bian's study was the first attempt to grasp the knowledge among general dentists regarding OSA. The lack of familiarity with the issue resulted in a low response rate.14 Upon considering the current study and its low response rate, the differences in methodology also should be considered, i.e., no follow-up contacts occurred, no patients were solicited formally, and how it tried to capture a national sample.
In conclusion, based on available literature and the results of this Quick Poll, much work needs to be put into DSM education and research. Important topics that need to be addressed include how DSM is practiced in the dental offices across the United States, identifying the phenotype of individuals who experience SDB, and creating more avenues for training and educating predoctoral and postdoctoral dental students.
ABBREVIATIONS
AADSM – American Academy of Dental Sleep Medicine
DSM – Dental Sleep Medicine
Network – National Dental Practice-Based Research Network
OAT – Oral Appliance Therapy
OSA – Obstructive Sleep Apnea
PBRN – Practice-Based Research Network
SDB – Sleep-disordered breathing
ACKNOWLEDGMENTS
The authors wish to thank the American Academy of Dental Sleep Medicine executive staff, Becky Roberts and Coreen Vick, for their feedback, and their Research and Policy Development Manager, Dr. Heather Montague, for her help reviewing and editing this manuscript. The authors are especially grateful for Dr. Greg Essick’s careful review and thoughtful input to improve the manuscript.
This work was supported by NIH grant U19-DE-28717. Opinions and assertions contained herein are those of the authors and are not to be construed as necessarily representing the views of the respective organizations or the National Institutes of Health. An Internet site devoted to details about the nation’s network is located at http://NationalDentalPBRN.org. The authors gratefully acknowledge all of the network practitioners who responded to this Quick Poll.
REFERENCES
American Academy of Dental Sleep Medicine. https://www.aadsm.org/. [homepage on the Internet]. About dental sleep medicine. Available from: https://www.aadsm.org/. Accessed January 4, 2021.
Lobbezoo F, Aarab G, Wetselaar P, Hoekema A, de Lange J, de Vries N. A new definition of dental sleep medicine. J Oral Rehabil. 2016;43(10):786–790.
Lavigne GJ, Goulet JP, Zuconni M, Morisson F, Lobbezoo F. Sleep disorders and the dental patient: a review of diagnosis, pathophysiol ogy and management. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:257–272.
Heinzer R, Vat, S., Marques-Vidal, P, et al. Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study. Lancet Respir Med. 2015;3(4):310–318.
Lai V, Carberry JC, Eckert DJ. Sleep apnea phenotyping: Implications for dental sleep medicine. J Dent Sleep Med. 2019; 6(2). https://doi.org/10.15331/jdsm.7072.
Bonsignore MR., Baiamonte P, Mazzuca E, Castrogiovanni A, Marrone O. Obstructive sleep apnea and comorbidities: A dangerous liaison. Multidisciplinary Respiratory Medicine. 2019;14(1), 1–12.
Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353(19):2034-2041.
Sanders AE, Essick GK, Fillingim R, et al. Sleep apnea symptoms and risk of temporomandibular disorder: OPPERA cohort. J Dent Res. 2013;92(7 Suppl):70S-7S.
Senaratna CV, Perret JL, Lodge CJ, et al. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med Rev. 2017;34:70-81.
Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687-698.
Frost & Sullivan. Darien, IL: American Academy of Sleep Medicine; 2016. Hidden health crisis costing America billions. Underdiagnosing and undertreating obstructive sleep apnea draining healthcare system. Available from: https://aasm.org/advocacy/initiatives/economic-impact-obstructive-sleep-apnea/
Dudley KA, Patel SR. Disparities and genetic risk factors in obstructive sleep apnea. Sleep Med. 2016;18:96-102. https://doi.org/10.1016/j.sleep.2015.01.015.
Schwartz D, Levine M, Adame M, et al. American Academy of Dental Sleep Medicine Position on the Scope of Practice for Dentists Ordering or Administering Home Sleep Apnea Tests. J Dent Sleep Med. 2020;7(4).
Bian H. Knowledge, opinions, and clinical experience of general practice dentists toward obstructive sleep apnea and oral appliances. Sleep Breath. 2004;8(2):85-90.
Loube MD, Strauss AM. Survey of oral appliance practice among dentists treating obstructive sleep apnea patients. Chest. 1997;111(2):382-386.
Ivanhoe JR, Frazier KB, Parr GR, Haywood VB. The teaching and treatment of upper airway sleep disorders in North American dental schools. J Prosthet Dent. 2003;89(3):292–296.
Karimi N, Mehta NR, Pagni SE, Antonellou E, Doherty EH, Correa LP. The Current State of Dental Sleep Medicine Practice in Academic Institutions: A Questionnaire-Based Study. JDSM. 2019;6(4).
Gilbert GH, Williams OD, Korelitz JJ, et al; National Dental PBRN Collaborative Group. Purpose, structure, and function of the United States National Dental Practice-Based Research Network. J Dent. 2013;41(11):1051-1059. doi: 10.1016/j.jdent.2013.04.002.
Greene SM, Reid RJ, Larson EB. Implementing the learning health system: from concept to action. Ann Intern Med. 2012;157(3):207-210.
American Academy of Dental Sleep Medicine. https://www.aadsm.org/. [dental Sleep Medicine FAQs on the Internet]. Dental Sleep Medicine FAQs. Available from: https://www.aadsm.org/ dental_sleep_medicine_faqs_fo.php. Accessed January 20, 2022.
Tufts School of Dental Medicine. https://www.dental.tufts.edu/. [homepage on the Internet]. Dental Sleep Medicine Fellowship. Available from: https://dental.tufts.edu/academics/postgraduate-programs/dental-sleep-medicine-fellowship. Accessed January 4, 2021.
Sheats RD, Schell TG, Blanton AO, et al. Management of side effects of oral appliance therapy for sleep-disordered breathing. JDSM. 2017;4(4):111–125.
Vuorjoki-Ranta TR, Lobbezoo F, Vehkalahti M, Tuomilehto H, Ahlberg J. Treatment of obstructive sleep apnoea patients in community dental care: knowledge and attitudes among general dental practitioners and specialist dentists. J Oral Rehabil. 2016;43(12):937-942. doi: 10.1111/joor.12441. Epub 2016 Sep 28. PMID: 27627187
Leigh C, Faigenblum M, Fine P, Blizard R, Leung A. General dental practitioners' knowledge and opinions of snoring and sleep-related breathing disorders. Br Dent J. 2021;231(9):569-574. doi: 10.1038/s41415-021-3573-z. Epub 2021 Nov 12. PMID: 34773028
Berggren K, Broström A, Firestone A, Wright B, Josefsson E, Lindmark U. Oral health problems linked to obstructive sleep apnea are not always recognized within dental care-As described by dental professionals. Clin Exp Dent Res. 2022;8(1):84-95. doi: 10.1002/cre2.517. Epub 2021 Nov 17. PMID: 34791818
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted October 8, 2021
Submitted in final revised form May 15, 2022
Accepted for publication June 8, 2022
Address correspondence to: Maria Therese Galang-Boquiren, DMD, MS, MBA, 801 S. Paulina St., Rm 131 M/C 841, Chicago, IL 60612, Email: mgalang@uic.edu