Original Article 2, Issue 8.1
Acceptance and Efficacy of Mandibular Advancement Device Treatment in Military Veterans With Obstructive Sleep Apnea: Effect on Posttraumatic Stress Disorder
http://dx.doi.org/10.15331/jdsm.7172Moh’d Al-Halawani, MD1,3; Sreelatha Naik, MD 1,2; Michael Chan, MD1, Iouri Kreinin, CCRP1,3; Jonathan Meiers, DMD4; Meir Kryger, MD1,3
1Department of Pulmonary, Critical Care and Sleep Medicine, Yale School of Medicine, New Haven, Connecticut; 2Department of Pulmonary, Critical Care and Sleep Medicine, Geisinger Health System, Wilkes-Barre, Pennsylvania; 3Department of Pulmonary, Critical Care and Sleep Medicine, Veterans Affairs Connecticut Healthcare System, West Haven, Connecticut; 4Dental Division, Veterans Affairs Connecticut Healthcare System, West Haven, Connecticut
ABSTRACT
Study Objectives:
Obstructive sleep apnea (OSA) and posttraumatic stress disorder (PTSD) often coexist in military veterans. Adherence to continuous positive airway pressure (CPAP) is poor among military veterans. The goal of the study was to evaluate whether veterans who were nonadherent to CPAP would accept treatment with mandibular advancement (MAD) devices, and whether those with PTSD experienced improvement in symptoms.
Methods:
The subjects were 75 military veterans in whom OSA was diagnosed (with an apnea-hypopnea index (AHI) >5 events per hour, central AHI <5 events per hour and <50% of total AHI) and who could not tolerate treatment with CPAP; 43% of subjects had concomitant PTSD. They were evaluated and treated by the Veterans Administration dental service and a MAD device was fabricated and provided to them. Treatment acceptance, efficacy and compliance were evaluated, as well as the effect of OSA treatment with MAD on PTSD symptoms.
Results:
Of 75 subjects who met initial inclusion criteria, 49 completed the study protocol and 47% of those were using MAD with good reported compliance. In approximately 45% of subjects, AHI was reduced by 50% from pretreatment baseline or AHI was less than 10 events per hour. A diagnosis of PTSD was documented in 43%, and 35.5% of patients with PTSD reported improvement in PTSD symptoms at the end of the study.
Conclusions:
Treatment of OSA with a MAD is a good alternative for patients who cannot tolerate CPAP, and may be associated with symptomatic improvement in those patients with concomitant PTSD.
Keywords:
continuous positive airway pressure; mandibular advancement device; obstructive sleep apnea; post-traumatic stress disorder
Citation:
Al-Halawani M, Naik S, Chan M, Kreinin I, Meiers J, Kryger M. Acceptance and efficacy of mandibular advancement device treatment in military veterans with obstructive sleep apnea: Effect on posttraumatic stress disorder. J Dent Sleep Med. 2021;8(1)
INTRODUCTION
Obstructive sleep apnea (OSA) and posttraumatic stress disorder (PTSD) are common in military veterans and frequently coexist in this patient population. Both disorders share an array of similar symptoms that are thought to be more severe in patients with comorbid OSA and PTSD.1, 2
Continuous positive airway pressure (CPAP) is the treatment of choice for OSA.3 Another treatment option is the use of a mandibular advancement device (MAD), which is recommended for patients with OSA who cannot tolerate CPAP therapy or prefer alternate therapy.4 Adherence to CPAP is poor among military veterans.5, 6 Mask claustrophobia, anxiety, and PTSD are issues that make PAP tolerance difficult,1, 5 and therefore, treatment with an MAD may be beneficial in this patient population. Untreated OSA has been shown to conversely worsen control of these disorders, in addition to many other well-described health effects.7
To further explore the relationship between PTSD and OSA, a total of 49 veterans were studied who had an established diagnosis of PTSD and OSA, who were unable to tolerate CPAP treatment, and therefore were referred for treatment of OSA with an MAD. It was hypothesized that successful treatment with MADs of patients with OSA who were intolerant of CPAP will have a favorable clinical effect in those with concomitant PTSD.
METHODS
The study was conducted at the Sleep Disorders Center at the Connecticut VA Healthcare System and was approved by the Institutional Review Board. Patients were enrolled between the years 2014 and 2017. All patients provided written consent prior to enrollment in this study.
This is a prospective cohort of veterans in whom OSA was diagnosed (with an apnea-hypopnea index (AHI) >5 events per hour, central AHI <5 events per hour, and <50% of total AHI) who could not tolerate CPAP treatment. A significant number of veterans carried a diagnosis of PTSD, which was diagnosed by the psychiatry department at the same facility.
Demographic information including age, sex, ethnicity, body mass index, and comorbid conditions were gathered for all patients. An in-laboratory polysomnography, Epworth Sleepiness Scale (ESS) score, Sleep Apnea Quality of Life Index (SAQLI), tolerability of oral appliance, and single-question assessment of PTSD symptoms were obtained for each patient at the beginning and end of the study. In-laboratory sleep studies were attended by a sleep technologist. Electroencephalogram, electrooculogram, electromyogram, electrocardiogram, nasal pressure transducer and thermistor for airflow measurement, and respiratory effort (by chest and abdominal plethysmography) and oxygen saturation all were acquired using a Compumedics system (Compumedics Corp, Charlotte, NC) and analyzed using Profusion 3 software. Studies were scored using the 2012 American Academy of Sleep Medicine scoring criteria (currently in use at the time the study was conducted).8 Apneas were defined as 90% decrease in the thermistor signal or more for at least 10 seconds. Hypopneas were defined as a 30% or more reduction flow (measured through nasal pressure transducer) for at least 10 seconds, associated with oxygen desaturation or arousal. Polysomnography was analyzed and interpreted by a board-certified sleep specialist. A diagnosis of OSA was made if the patient’s respiratory events reach an AHI of >5 events per hour.
Nocturnal oximetry parameters including nadir oxygen saturation, percent time with SpO2<90%, and oxygen desaturation index (3% and 4% oxygen desaturation index [ODI]) were obtained. ODI was defined as the number of desaturations (3% and 4%) per hour of total sleep time.
Patients were referred to an in-house dental sleep medicine-certified dentist for custom fitting, fabrication, and titration of the oral appliances. The oral appliances used were dual-block adjustable designs consisting of a vertical fin design, the SomnoDent® Flex (SomnoMed, Inc, Sydney, Australia), and a horizontal traction design, Narval ™ CC (ResMed, San Diego, CA). The choice of appliance design for a specific patient was determined by the number, position, location, and shape of the teeth, the cheek and lip tension, and the space between the dental arches and the buccal vestibules. Records were obtained by taking full arch impressions of the maxilla and mandible using stock trays and VPS (Panasil® Kettenbach LP). A protrusive record was obtained using a George Gauge™ with a 5-mm vertical bite fork. The initial protrusive starting position was set at 60% the maximum protrusion for the patient. The appliances were tried in and any needed adjustments for fit or to achieve balanced occlusion were performed. Bite repositioners (Good Morning Positioner, SML Global) were provided to all patients. Instructions for wearing and how to adjust and maintain the appliance and a titration schedule were provided to all patients. Patients were re-appointed in 3 weeks for a follow-up visit to evaluate any fit, comfort issues, and the progression with the titration process. The titration schedule was the same for each patient and changed if problems arose during the progression. Patients were advanced from their initial starting position in 0.5-mm increments until snoring was eliminated and the patient stated a change in their energy levels and wakefulness. Once that position was reached a decision was made, based on the remaining distance to reach maximum protrusion, whether the patient’s mandible would be further advanced. Each patient was individually titrated to their treatment position and this occurred over varying periods of time. Once this position was reached the patient was scheduled for a follow-up PSG with the appliance in 3 months. Compliance with the MAD therapy was via patient report.
Patients were followed up in clinic/by telephone and were asked about changes in posttraumatic stress symptoms (Better, Worse or No change), and daytime sleepiness measured by ESS.
Patients included in the study were aged 18 years and older, with a diagnosis of OSA who could not tolerate CPAP therapy. Reasons for CPAP intolerance included a comorbid diagnosis of anxiety disorder, PTSD, and claustrophobia related to military service.
Patients with morbid obesity (body mass index greater than 40 kg/m2), history of respiratory failure, heart failure, or stroke were excluded from the study, as well as patients with cognitive impairment and inability perform the activities required for this research.
Patients were also excluded if their dentition has signs of untreated caries, fractured teeth, or periodontal disease or if they did not have enough teeth to properly anchor an oral appliance.
Statistical Analysis
Statistics were analyzed using GraphPad Prism 7 software. For normally distributed and non-normally distributed data, Student t-test and Mann-Whitney U test, respectively, were used to assess the differences in parameters before and after treatment. A value of P ≤ 0.05 was considered statistically significant.
RESULTS
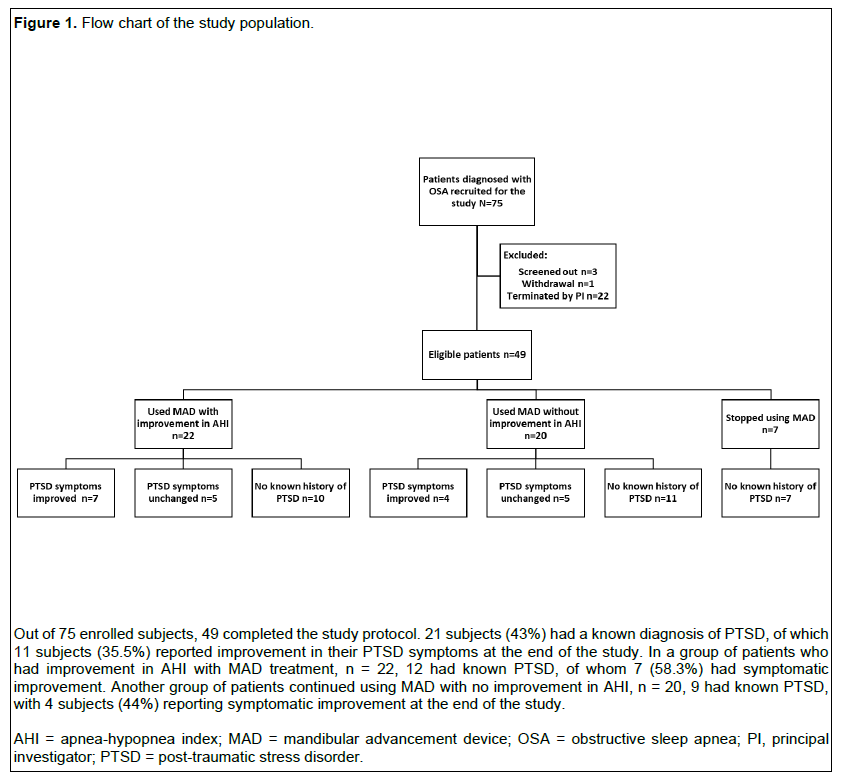
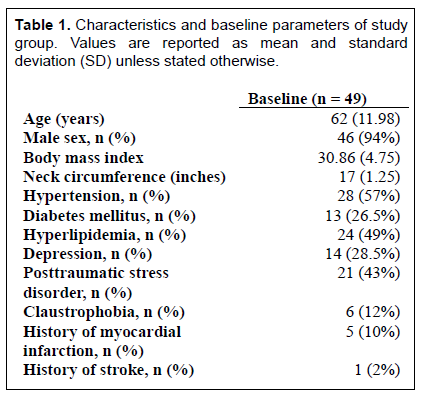
Of 75 subjects who met initial inclusion criteria, 49 completed the study protocol (65% MAD use), (12 patients were lost to follow up, 3 switched back to CPAP, 1 used a MAD and CPAP combined therapy, 6 stopped using MAD because of side effects, 1 withdrew, 3 were screened out because of malignancy, cognitive impairment and AHI<4 events per hour on repeat PSG) (Figure 1). Reported side effects included temporomandibular joint pain, dental pain, excessive gagging, and mouth dryness. The patient population was predominantly male, middle-aged, obese, CPAP-intolerant military veterans with OSA and a high prevalence of PTSD, n = 21 (45%). The most common causes for CPAP intolerance were attributed to claustrophobia, high CPAP pressures, dislike of wearing CPAP, lack of symptomatic benefit, and insomnia. Baseline characteristics and comorbidities are summarized in Table 1. Table 2 describes parameters that changed with therapy.
A total of 23 subjects (47%) reported using MAD with good compliance (adherence at least 4 hours per night, at least 70% of the nights).
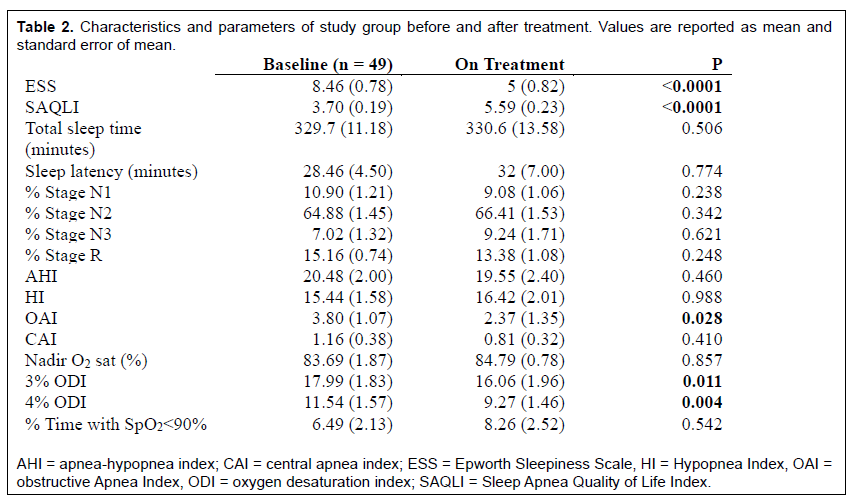
OSA treatment with MAD significantly improved excessive daytime sleepiness measured by ESS, SAQLI, obstructive apnea index, and ODI at 3% and 4% desaturation [Table 2]. There were no significant changes observed in other polysomnographic parameters.
One group of patients, n = 22 (44.9%), demonstrated improvement in AHI by >50% from pre-treatment baseline or to an AHI <10 events per hour with MAD on follow-up PSG. In this group, 12 subjects (54.5%) had a known diagnosis of PTSD, and 10 (45.5%) had no known history of PTSD.
A second group of patients, n = 20 (40.8%), did not show improvement in the AHI with MAD on follow-up PSG. In this group, 9 subjects (45%) had a known diagnosis of PTSD, and 11 subjects (55%) did not.
Seven of 49 patients (14.2%) eventually discontinued using their MADs because of side effects.
Among all patients with PTSD (n = 21), 11 (52.4%) reported improvement in their PTSD symptoms while being treated for OSA with MADs. A better response was observed in patients who demonstrated improvement in their AHI, n = 7 of 12 (58.3%), compared to those who did not, n = 4 of 9 (44.4%). Each of the two groups had 5 patients (41.7% and 55.6% respectively) that reported no change in their PTSD symptoms, and no patients reported worsening symptoms.
Figure 1Flow chart of the study population. |
{kind=link}
Table 1Characteristics and baseline parameters of study group. Values are reported as mean and standard deviation (SD) unless stated otherwise. |
{kind=link}
Table 2Characteristics and parameters of study group before and after treatment. Values are reported as mean and standard error of mean. |
{kind=link}
DISCUSSION
Treatment of OSA with an MAD is a good alternative in patients unable to tolerate using CPAP; it also had an appropriate level of acceptance (65%) among this population as demonstrated in the study. MADs successfully decreased AHI by >50% from pretreatment baseline or to an AHI <10 events per hour in approximately 45% of our study population, significantly decreased the 3% and 4% ODI, symptoms of excessive daytime sleepiness measured by ESS and improved quality of life as measured by the SAQLI.
The study population had a high prevalence of PTSD; perhaps the most robust finding was the improvement of PTSD symptoms in more than half of the patients with this debilitating illness. The response was more evident in the group of patients who experienced a decrease in AHI by >50% or to an AHI <10 events per hour.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) defines PTSD as the development of a specific cluster of symptoms after exposure to a traumatic event that elicits a response of fear, helplessness, or horror; which is associated with four symptom clusters, including intrusion, avoidance, negative alterations in cognitions and mood, and alterations in arousal and reactivity.9
PTSD has a lifetime prevalence in US adults ranging between 7.8% to 12.3%.1 This prevalence increases to approximately 30% of Vietnam veterans and 11% to 17% of veterans who served in Afghanistan and Iraq.10-12
PTSD has been shown to alter sleep structure in affected patients. Although a consistent effect of PTSD on electroencephalography during sleep is not quite established, a meta-analysis by Kobayashi et al concluded that patients with PTSD had more stage N1 sleep, less slow wave sleep, and greater rapid eye movement density compared to subjects without PTSD.13
There are many comorbid overlapping sleep disorders in individuals with a diagnosis of PTSD, including insomnia, a fear of falling asleep, nightmares, sleep-disordered breathing (SDB), periodic limb movement disorders, parasomnias, and dream enactment behavior.1, 14 In addition, sleep terrors and nocturnal anxiety attacks are also more frequent in patients with PTSD.6
Studies have shown an increased prevalence of OSA in patients with PTSD and vice versa. OSA is associated with an increased prevalence of psychiatric conditions in veterans. In a large study conducted by Sharafkhaneh et al at the Veterans Health Administration assessing the relationship between OSA and psychiatric disorders, PTSD was present in 11.9% of patients with OSA and 4.7% in patients without OSA.15
SDB is also highly prevalent in patients with PTSD. Yesavage et al reported an SDB prevalence of 69% (AHI>10 events per hour) in Vietnam veterans with PTSD.16 A smaller study by Van Liempt et al did not show increased prevalence of OSA in patients with PTSD in comparison with control patients; however, it appeared that patients had increasing PTSD symptom severity in the presence of OSA.17 In one study screening for OSA in veterans seeking treatment for PTSD, there was a high rate of OSA in veterans with PTSD (72.7%) 2 Furthermore, Colvonen et al reported that 69.2% of veterans with PTSD screened as being high risk for OSA using the Berlin questionnaire; a rate much higher than those seen in community studies.12
Sleep disturbance is a common feature in OSA and PTSD. It is hypothesized that either disorder may exacerbate or perpetuate symptoms of the other, with sleep fragmentation being the culprit in this relationship. Obstructive events followed by arousals and sleep fragmentation have been shown to compromise fear extinction (which is beneficial in patients with PTSD) and cause interruption of memory consolidation, especially in rapid eye movement sleep, which might lead to the recurrence of maladaptive fear and anxiety and worsen PTSD symptoms.1
Sleep fragmentation may exacerbate SDB. In a study by Series et al, higher upper airway collapsibility was observed (as measured by critical pressure) after sleep fragmentation than after sleep deprivation.18 This suggests that sleep fragmentation induced by PTSD may increase the risk of the development of OSA. In a systematic review by Gupta et al,7the authors showed that there may be an increased prevalence of OSA in patients with PTSD, with a reported prevalence of 42.7% to 50% in military populations.
OSA has a reported prevalence of 24% for men and 9% for women in the general population younger than 65 years, using a definition of AHI ≥ 5 events per hour without excessive daytime sleepiness. Moreover, the median prevalence of OSA in PTSD was 42.7% in seven clinic-based populations, ranging from 1.3% to 83%.7
Meanwhile, in an observational study by Mysliwiec et al that included 109 active-duty service members with recent combat exposure, the rate of OSA in military personnel with PTSD was 58.5%. PTSD symptoms and OSA severity in subjects with comorbid PTSD and OSA did not differ significantly compared to that of subjects with PTSD or OSA alone. However, there were significant differences in sleep quality between the comorbid PTSD/OSA and OSA groups when measured by the Pittsburgh Sleep Quality Index. Also, fatigue was increased significantly in the PTSD and PTSD/OSA groups compared to OSA alone.19
Treatment with CPAP has been demonstrated to resolve respiratory events and improve several OSA-related symptoms and disorders. Furthermore, satisfactory treatment of SDB may ameliorate anxiety, depression, and other cognitive disorders. It was also shown to cause a reduction in nightmare frequency and severity, and daytime flashbacks.1
Adequate treatment of SDB has been shown to mitigate PTSD-related symptoms in patients with comorbid OSA and PTSD. Nightmare recall is triggered through frequent nighttime awakenings and arousals caused by OSA; therefore, treatment with CPAP may reduce awareness of nightmares as well as daytime distress related to them by consolidating sleep.20, 21
CPAP compliance is reportedly lower in patients with PTSD in comparison with control patients, leading to increased nightmare severity; whereas a reduction in nightmare frequency is observed in patients who were adherent to CPAP.7 In a case-controlled study by Lettieri et al., active-duty service members with PTSD and OSA had worse sleepiness symptoms, quality of life, and lower compliance and response to CPAP compared to control groups. The low adherence to CPAP may have been related to comorbid insomnia in that study population. 22
Krakow et al found that treatment of OSA in patients with PTSD significantly improved sleep quality, frequency of nightmares, and daytime well-being. Nightmares were reported to be eliminated in five patients from the Treatment group and one from the No-Treatment group, and PTSD symptoms were eliminated in two from the Treatment group and one from the No-treatment group in that study. 21
In a larger retrospective study (n = 69), Tamanna et al. showed that CPAP therapy reduced PTSD-associated nightmares, with the mean number of nightmares decreased from 10.32 to 5.26 per week, (P < 0.001), and improved overall subjective PTSD symptoms in veterans with comorbid PTSD and OSA; these results were best predicted by CPAP compliance.23
Despite the reported improvement in PTSD symptoms with treatment of OSA, patients with PTSD continue to have lower CPAP compliance compared to other patients with OSA. Some reasons for nonadherence include mask discomfort, claustrophobia, and air hunger.5, 6 Other factors that may limit adherence to CPAP and are commonly seen in PTSD include insomnia, sleep fragmentation, and recurrent awakenings.24
In a study by El-Solh et al,5 multiple nighttime awakenings with anxiety attacks following nightmares may have been one of the factors infringing CPAP compliance in patients with PTSD. In the same retrospective study, where short-term CPAP compliance was evaluated, adherence to CPAP was significantly lower in the PTSD group (concomitant PTSD and OSA) compared to the control group (OSA without PTSD) (41% versus 70%, respectively; P < 0.001).
Jaoude et al suggested that wearing a face mask with positive pressure may trigger PTSD symptoms by provoking old combat-related memories or experiences in veterans with PTSD, which may further have a negative effect on CPAP compliance.1
Furthermore, in a retrospective case-control study by Collen et al that included 90 young combat veterans with OSA (with and without PTSD), those with PTSD had a significantly lower use of CPAP compared with patients without PTSD (61.2% vs 76.8% of nights; P = 0.001). In the same study, the mean nightly use of CPAP was less in the PTSD group (3.4 ± 1.2 hour) compared with the control group (4.7 ± 2.2 h), P < 0.001. Regular use of CPAP, defined as > 4 hours per night for >70% of nights, was also lower in patients with comorbid PTSD and OSA compared to OSA alone (25.2% vs 58.3%, P = 0.01).6
MADs may be better accepted by some veterans than PAP. In a recent study by Feinstein et al, in veterans with OSA in whom treatment with CPAP failed, adherence to MADs was 58.3% at 6 months after device fabrication and delivery. The adherence was higher than that demonstrated in other studies including veteran populations treated with CPAP. 25
Finally, in a randomized crossover trial by El-Solh et al (n = 35) comparing the efficacy, adherence, and preference of CPAP versus MAD in veterans with concomitant PTSD and OSA; CPAP was more effective than MAD in reducing AHI and improving nocturnal oxygenation measured as percent of time spent with SpO2 >90% (P < 0.001 and P = 0.04, respectively). Both treatments reduced PTSD severity, measured by PTSD Checklist-Military version (PCL-M), with no significant difference in the extent of symptomatic improvement between the CPAP and MAD arms. Patients reported a significantly higher adherence to MAD than CPAP (P < 0.001) in this study with 58% of veterans preferring MAD, 29% preferring CPAP and 13% preferring neither for treatment of their sleep apnea.26
Therefore, MADs may be effective in improving sleep apnea, subjective sleepiness, and symptoms of PTSD. Although reported in patients treated with CPAP, to the authors’ knowledge there is not enough evidence showing clinical improvement in PTSD symptoms in patients with OSA treated with oral appliances. Furthermore, many patients are still unable to tolerate MAD, and efficacy remains variable.
Limitations
This study has some limitations. First, it is a single-center prospective observational study. Second, the study population is predominantly male veterans and therefore the results may not be generalizable. Third, compliance with MAD treatment was assessed by patient report and not objectively. Fourth, some of the respiratory events were scored using the 4% oxygen desaturation rule instead of 3% to define hypopneas on the diagnostic sleep studies, this may have led to underestimation of the baseline AHI of some patients and a statistically nonsignificant change in AHI after treatment. Fifth, a single question assessment was used to evaluate the improvement in PTSD symptoms.
CONCLUSION
Treatment of OSA with MADs is a well-tolerated, effective, and reliable alternative for patients who cannot tolerate treatment with CPAP and has been shown to improve symptoms and quality of life in patients with OSA. It may also be associated with improvement in PTSD symptoms in a group of patients with concomitant OSA and PTSD. More trials are needed to further study the relationship between OSA and PTSD and the effect of treatment of OSA on PTSD symptoms.
ACKNOWLEDGMENTS
This research was supported by ResMed, SomnoMed, and Kettenbach LP.
REFERENCES
- Jaoude P, Vermont LN, Porhomayon J, El-Solh AA. Sleep-disordered breathing in patients with post-traumatic stress disorder. Ann Am Thorac Soc. 2015;12:259-268.
- Forbus L, Kelly UA. Screening for obstructive sleep apnea in veterans seeking treatment of posttraumatic stress disorder. ANS Adv Nurs Sci. 2015;38:298-305.
- Epstein LJ, Kristo D, Strollo PJ Jr, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5:263-276.
- Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: an update for 2015. J Clin Sleep Med. 2015;11:773-827.
- El-Solh AA, Ayyar L, Akinnusi M, Relia S, Akinnusi O. Positive airway pressure adherence in veterans with posttraumatic stress disorder. Sleep. 2010;33:1495-1500.
- Collen JF, Lettieri CJ, Hoffman M. The impact of posttraumatic stress disorder on CPAP adherence in patients with obstructive sleep apnea. J Clin Sleep Med. 2012;8:667-672.
- Gupta MA, Simpson FC. Obstructive sleep apnea and psychiatric disorders: a systematic review. J Clin Sleep Med. 2015;11:165-175.
- Berry RB, Brooks R, Gamaldo CE, Harding SM, Marcus CL, Vaughn BV. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. Darien, Illinois: American Academy of Sleep Medicine, 2012;176.
- Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Washington, DC: American Psychiatric Association, 2013.
- Dohrenwend BP, Turner JB, Turse NA, Adams BG, Koenen KC, Marshall R. The psychological risks of Vietnam for U.S. veterans: a revisit with new data and methods. Science. 2006;313:979-982.
- Hoge CW, Castro CA, Messer SC, McGurk D, Cotting DI, Koffman RL. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N Engl J Med. 2004;351:13-22.
- Colvonen PJ, Masino T, Drummond SP, Myers US, Angkaw AC, Norman SB. Obstructive sleep apnea and posttraumatic stress disorder among OEF/OIF/OND Veterans. J Clin Sleep Med. 2015;11:513-518.
- Kobayashi I, Boarts JM, Delahanty DL. Polysomnographically measured sleep abnormalities in PTSD: a meta-analytic review. Psychophysiology. 2007;44:660-669.
- Mohsenin S, Mohsenin V. Diagnosis and management of sleep disorders in posttraumatic stress disorder:a review of the literature. Prim Care Companion CNS Disord. 2014;16.
- Sharafkhaneh A, Giray N, Richardson P, Young T, Hirshkowitz M. Association of psychiatric disorders and sleep apnea in a large cohort. Sleep. 2005;28:1405-1411.
- Yesavage JA, Kinoshita LM, Kimball T, et al. Sleep-disordered breathing in Vietnam veterans with posttraumatic stress disorder. Am J Geriatr Psychiatry. 2012;20:199-204.
- van Liempt S, Westenberg HG, Arends J, Vermetten E. Obstructive sleep apnea in combat-related posttraumatic stress disorder: a controlled polysomnography study. Eur J Psychotraumatol. 2011;2.
- Series F, Roy N, Marc I. Effects of sleep deprivation and sleep fragmentation on upper airway collapsibility in normal subjects. Am J Respir Crit Care Med. 1994;150:481-485.
- Mysliwiec V, Matsangas P, Gill J, et al. A comparative analysis of sleep disordered breathing in active duty service members with and without combat-related posttraumatic stress disorder. J Clin Sleep Med. 2015;11:1393-1401.
- Hicks RA, Bautista J. Snoring and nightmares. Percept Mot Skills.1993;77:433-434.
- Krakow B, Lowry C, Germain A, et al. A retrospective study on improvements in nightmares and post-traumatic stress disorder following treatment for co-morbid sleep-disordered breathing. J Psychosom Res. 2000;49:291-298.
- Lettieri CJ, Williams SG, Collen JF. OSA syndrome and posttraumatic stress disorder: clinical outcomes and impact of positive airway pressure therapy. Chest. 2016;149:483-490.
- Tamanna S, Parker JD, Lyons J, Ullah MI. The effect of continuous positive air pressure (CPAP) on nightmares in patients with posttraumatic stress disorder (PTSD) and obstructive sleep apnea (OSA). J Clin Sleep Med. 2014;10:631-636.
- Krakow B, Melendrez D, Pedersen B, et al. Complex insomnia: insomnia and sleep-disordered breathing in a consecutive series of crime victims with nightmares and PTSD. Biol Psychiatry. 2001;49:948-953.
- Feinstein AJ, Zaki M, Zaghi S, Tajima T,Wang MB. Utilization of a mandibular advancement device for obstructive sleep apnea in the veteran population. J Dent Sleep Med. 2017;4:37-40.
- El-Solh AA, Homish GG, Ditursi G, et al. A randomized crossover trial evaluating continuous positive airway pressure versus mandibular advancement device on health outcomes in veterans with posttraumatic stress disorder. J Clin Sleep Med. 2017;13:1327-1335.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted in final revised form April 10, 2020
Accepted for publication July 5, 2020
Address correspondence to: Moh’d Al-Halawani, MD, Yale School of Medicine, Department of Pulmonary, Critical Care and Sleep Medicine, 333 Cedar Street, New Haven, CT 06510; E-mail: mhalawanimd@gmail.com