Original Article 2, Issue 6.2
Assessment of Potential Tooth Movement and Bite Changes With a Hard-Acrylic Sleep Appliance: A 2-Year Clinical Study
http://dx.doi.org/10.15331/jdsm.7070
Nikola Vranjes, DDS1, Gene Santucci, DDS, MA2, Karen A. Schulze, PhD, DDS2, David Kuhns, PhD3, Allen Khai2
1The Snore Centre, Calgary, Alberta, Canada; 2 University of Pacific, San Francisco, California; 3ProSomnus Sleep Technologies, Pleasanton, California
ABSTRACT
Study Objectives:
The objective of this study was to test a proprietary hard-acrylic computer-aided design/computer-aided manufacturing (CAD/CAM) oral appliance with “retainer-like fit” and determine whether it resulted in tooth movement upon regular wear over a minimum 2-year period. Additionally, this study focused on determining patient acceptance of said device considering any reported side effects.
Methods:
The 2-year clinical study reports on selected patients in whom sleep apnea has been diagnosed (n=18) recruited from The Snore Center in Calgary. Patients were fitted with a ProSomnus® Sleep Appliance. Impressions were taken at baseline, after approximately 1 year, and after 2 years of use with the oral appliance. Models were marked, scanned, and scored; upper and lower anterior teeth crowding was assessed; and overjet and overbite were measured independently at the University of Pacific. Patients were surveyed on compliance, satisfaction with the appliance, and quality of life using the Sleep Apnea Quality of Life Index (SAQLI-10).
Results:
This study shows a rigid OA made with proprietary CAD/CAM technology demonstrated no significant change in tooth position during the 2.3-year test period, or in bite changes per maximum intercuspation (MIP), as measured by overjet and overbite. At 2 years, the mean change in Little Irregularity Index for the lower anterior teeth was 0.007 mm (95% confidence interval = [-0.03, 0.05]), which was not statistically different from zero (P>0.05). Patients were highly satisfied with the device and considered it beneficial.
Conclusions:
A key component to any treatment is patient's acceptance of the appliance and the willingness to wear the OA long term. When patient compliance is observed, hard-acrylic sleep appliances have little effect on tooth movement and MIP bite changes as shown by overjet/overbite.
Clinical Trial Registration:
Health Research Ethics Board of Alberta: CTC-16-0108
Keywords:
CAD/CAM technology, obstructive sleep apnea, oral appliance, tooth movement
Citation:
Vranjes N, Santucci G, Schulze K, Kuhns D, Khai A. Assessment of potential tooth movement and bite changes with a hard-acrylic sleep appliance: A 2-year clinical study. J Dent Sleep Med. 2019;6(2)
INTRODUCTION
Oral appliance therapy (OAT) has been shown to successfully treat patients with obstructive sleep apnea/hypopnea syndrome (OSAHS).1-3 However, OAT is often associated with the occurrence of side effects such as unwanted tooth movement. Positive airway pressure therapy is more commonly used to treat OSAHS, because of the reluctance to prescribe OAT as a result of these side effects.4 Even so, Pliska5 does report on tooth movement due to tongue thrusting as a result of the use of positive airway pressure. Although OAT is an effective treatment for OSAHS along with its greater compliance, long-term use of some oral appliances has been shown to result in several side effects, including tooth movement. Past studies have shown this to result in significant effects, such as craniofacial changes,6-8 anteroposterior positioning of the molars, inclination of the upper and lower incisors,9 and irregularity of the lower incisors.10 According to the American Academy of Dental Sleep Medicine’s published article on management of side effects, tooth movement (specifically occlusal changes represented by incisor changes, position of canines, decreased overjet/overbite, and altered occlusal contacts/bite changes) is one of the five significant concerns during the treatment of obstructive sleep apnea using an oral appliance.11 It was reported that there is a significant difference in anterior crowding using a flexible oral appliance without incisor coverage versus a rigid OA. 10 The rigid OA demonstrated less tooth movement. Recently, new devices with proprietary computer-aided design/computer-aided manufacturing (CAD/CAM) technology have been introduced and made available to clinicians. This study aims to investigate the changes in tooth movement with a hard-acrylic rigid oral appliance, the ProSomnus® Sleep Appliance, over a 2-year period. This research project was based on an approved Internal Review Board (IRB) protocol.12
METHODS
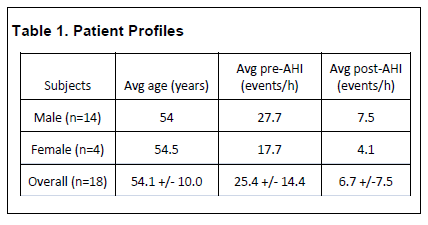
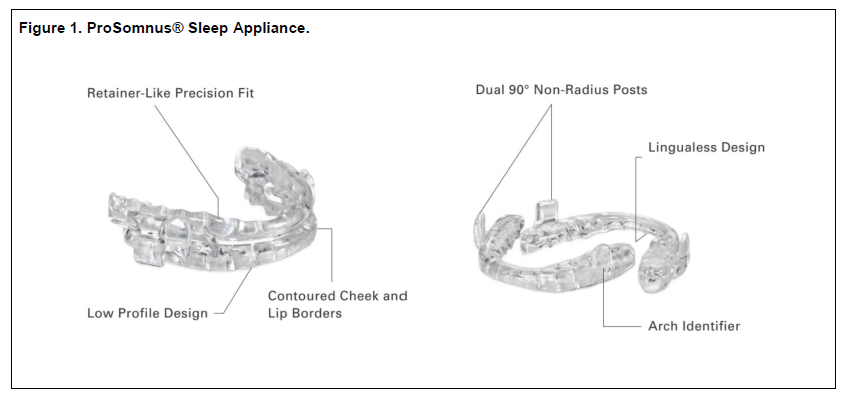
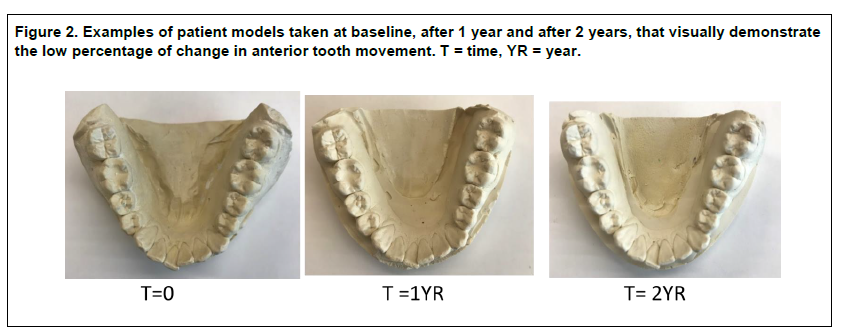
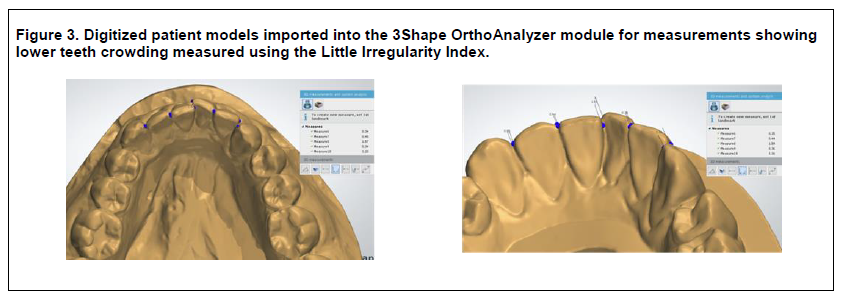
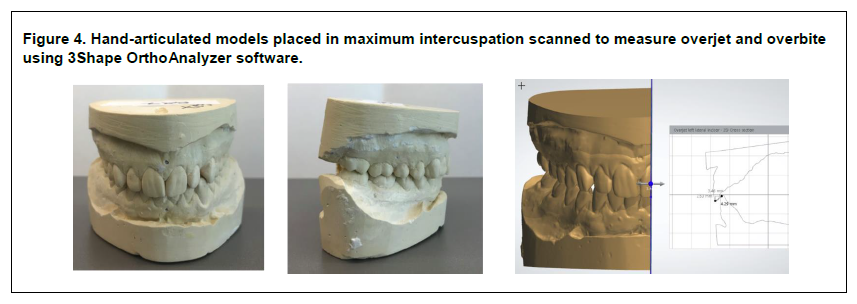
Patients were accepted into the study who were willing to return for follow-up impressions to be taken at the respective time points of 1 and 2 years. Patients were recruited from a pool of randomly selected patients (n=53) from an earlier study3 with an acceptance criterion of body mass index less than 35 kg/m2 and AHI greater than 10 events per hour. Eighteen of the 53 patients (14 male/4 female) with sleep apnea were recruited for this study. Average patient age was 54 years, with an overall pretreatment AHI of 25.4 events per hour and posttreatment AHI of 6.7 events per hour (Table 1). Patients’ pretreatment impressions were taken and the bite position captured using the George Gauge, and patients were fitted with a ProSomnus® Sleep Appliance (Figure 1) at The Snore Centre in Calgary. Patients were not fitted with a morning aligner. The patient’s bite was determined by the MATRx (Zephyr Sleep Technologies, Calgary, AB, Canada) target position3 in which the bite position was at a percentage of maximum protrusion ranging from 40% to 100%. Polyvinylsiloxane impressions were taken at baseline, after approximately 1 year (mean = 1.2 years) and after 2 years (mean = 2.3 years) of use with the oral appliance. Patients were surveyed on compliance and quality of life using the Sleep Apnea Quality of Life Index (SAQLI). The compliance survey asked patients to subjectively report on their compliance; patients were asked if they wore their appliance more than 4 hours per night, more than 5 days per week. The SAQLI survey was given to patients at the 1- and 2-year time points. The initial time point was unavailable as recruited patients had already been wearing their appliances upon study initiation. Models were marked, per the IRB, to scrub the patient data and to obscure the time points of each patient, from the measurement technician, to reduce measurement bias. Statistical analysis was completed by a separate party not involved in the measurement procedure. The mixed-effects model for analysis was chosen to provide the best estimates of the mean and confidence intervals. This model deals more adequately with the variable number of measurement replicates at each time point for each subject. Patient models (Figure 2) were scanned on a TRIOS lab scanner (3Shape, Copenhagen, Denmark) and scored using 3Shape OrthoAnalyzer software (3Shape, Copenhagen, Denmark).13 The upper and lower anterior teeth crowding was calculated using the Little Irregularity Index method14 (Figure 3). The models were placed in maximum intercuspation (MIP) and scanned, and overjet and overbite were measured using 3Shape OrthoAnalyzer software (Figure 4). Scanning and measurements were completed by the University of Pacific School of Dentistry.
Table 1Patient Profiles |
{kind=link}
Figure 1ProSomnus® Sleep Appliance. |
{kind=link}
Figure 2Examples of patient models taken at baseline, after 1 year and after 2 years, that visually demonstrate the low percentage of change in anterior tooth movement. T = time, YR = year. |
{kind=link}
Figure 3Digitized patient models imported into the 3Shape OrthoAnalyzer module for measurements showing lower teeth crowding measured using the Little Irregularity Index. |
{kind=link}
Figure 4Hand-articulated models placed in maximum intercuspation scanned to measure overjet and overbite using 3Shape OrthoAnalyzer software. |
{kind=link}
Patients were given two surveys, the SAQLI-10 short version and one to measure compliance and satisfaction with the rigid oral appliance. The purpose of the surveys was to determine whether patients would wear the appliance, their satisfaction level, and whether the appliance was considered beneficial. The compliance metric will demonstrate that the tooth movement results are under the condition that patients wore the device.
Statistical Analysis
The mean change from baseline was estimated in a repeated-measures (mixed-effects) linear model. This model allows for missing values at certain time points and efficiently uses all the data to estimate effects. Time was treated as a categorical variable. The model also yields an estimate of the measurement error for an impression at a single time point.RESULTS
At the beginning of the study, the anterior upper and lower arches were measured in each patient. The same measurements were done after an average of 1.2 years. Variation from time zero to year 1 for individual pairs of teeth, for example, between 27-26 on the lower arch and 8-9 on the upper arch, had an overall average shift of -.022 mm for the upper arch and -.014 mm for the lower arch. The average difference for the total Little Irregularity Index for the same 18 patients at an average of 2.3 years for the upper arch was -0.007 mm. The average difference for the lower arch was 0.003 mm total. Within this study sample size, these differences were not shown to be statistically significant. The average change in the patients’ overbite after 2.3 years was 0.0045 mm and for overjet -.015 mm.
Lower Arch
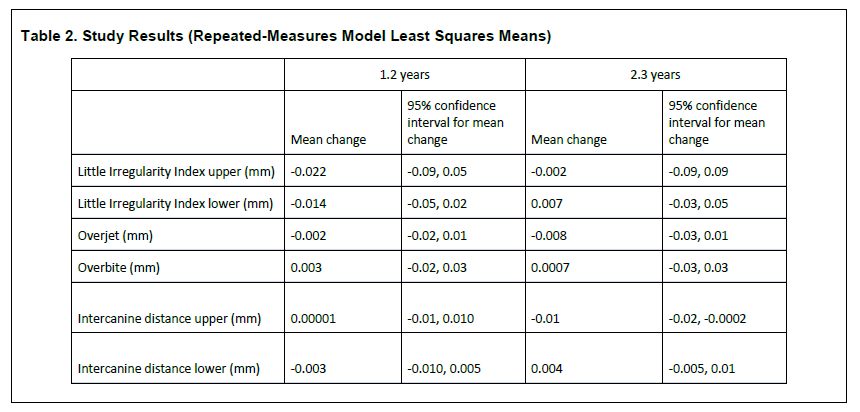
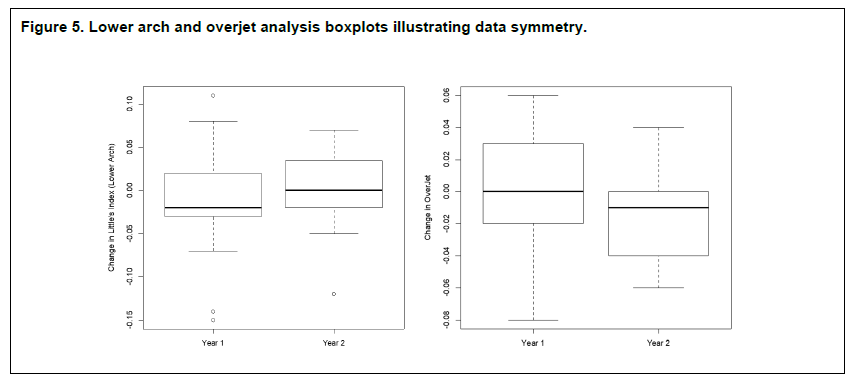
The mean change in Little Irregularity Index at 1 year was -0.014 mm (95% confidence interval [CI]= -0.05, 0.02), which was not statistically different from zero (P>0.05). The estimated measurement error was 0.05 mm; the mean change is thus less than the measurement error. At 2 years, the mean change in Little Irregularity Index was 0.007 mm (95% CI = -0.03, 0.05), which was not statistically different from zero (P>0.05). The mixed-effects model estimates of the mean change in Little Irregularity Index are presented in Table 2 and the change in measures are presented graphically in Figure 5. The boxplot shows acceptable symmetry in the spread of the data for a sample set of this size.
Table 2Study Results (Repeated-Measures Model Least Squares Means) |
{kind=link}
Figure 5Lower arch and overjet analysis boxplots illustrating data symmetry. |
{kind=link}
Upper Arch
The mean change in Little Irregularity Index at 1 year was -0.022 mm (95% CI = -0.09, 0.05), which was not statistically different from zero (P>0.05). The estimated measurement error was 0.11 mm; thus, the mean change was less than the measurement error. At 2 years, the mean change in Little Irregularity Index was -0.002 mm (95% CI = -0.09, 0.09), which was not statistically different from zero (P>0.05). The mixed-effects model estimates of the mean change in Little Irregularity Index are presented in Table 2.Overjet
The mean change in overjet at 1 year was -0.002 mm (95% CI = -0.02, 0.01), which was not statistically different from zero (P>0.05). The estimated measurement error was 0.026 mm; thus, the mean change was less than the measurement error. At 2 years, the mean change in overjet was -0.008 mm (95% CI = -0.03, 0.01), which was not statistically different from zero (P>0.05). The mixed-effects model estimates of the mean in overjet are presented in Table 2 and the change measurements are presented graphically in Figure 5.Overbite
The mean change in overbite at 1 year was 0.003 mm (95% CI = -0.02, 0.03), which was not statistically different from zero (P>0.05). The estimated measurement error was 0.036 mm; thus, the mean change was less than the measurement error. At 2 years, the mean change in overbite was 0.0007 mm (95% CI = -0.03, 0.03), which was not statistically different from zero (P>0.05). The mixed-effects model estimates of the mean change in overbite are presented in Table 2.Upper Intercanine Distance
The mean change in upper intercanine distance at 1 year was 0.00001 mm (95% CI = -0.001, 0.001), which was not statistically different from zero (P>0.05). The estimated measurement error was 0.014 mm; thus, the mean change was less than the measurement error. At 2 years, the mean change in upper intercanine distance was -0.01 mm (95% CI = -0.02, -0.0002), which was statistically different from zero (P<0.05). The mixed-effects model estimates of the mean change in upper intercanine distance are presented in Table 2.Lower Intercanine Distance
The mean change in lower intercanine distance at 1 year was -0.003 mm (95% CI= -0.010, 0.005), which was not statistically different from zero (P>0.05). The estimated measurement error was 0.011 mm; thus, the mean change was less than the measurement error. At 2 years, the mean change in lower intercanine distance was 0.004 mm (95% CI = -0.005, 0.01), which was not statistically different from zero (P>0.05). The mixed-effects model estimates change in lower intercanine distance are presented in Table 2.SURVEY RESULTS
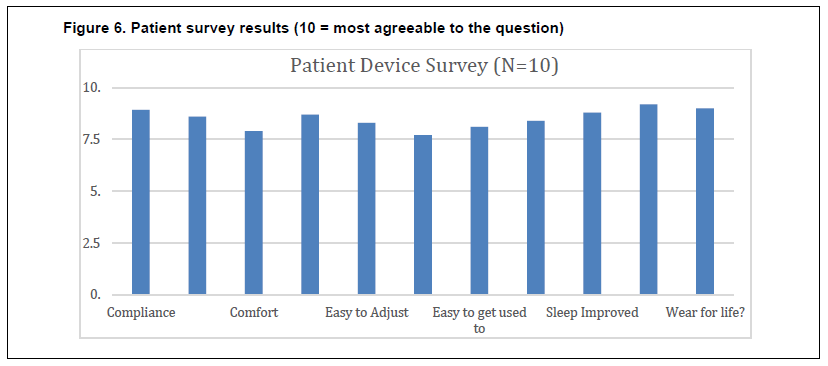
Two surveys were given to patients to assess their acceptance of the device and the OAT, and to test for quality of life improvements (SAQLI). A total of 56% of patients (n=10) responded to the device survey with an average duration of survey since appliance insertion of 2.3 +/- 0.4 years. A total of 28% of patients (n=5) completed two time points of the SAQLI survey. The device survey results are shown in Figure 6. Subjects were asked to rate their agreement on a 10-point scale, with 0 as "no agreement" and 10 as "full agreement." To determine patient compliance, patients were asked “Did you wear the device at least 5 days a week?” and “Did you wear the device at least 4 hours per night?”. Based on the two questions, patients were 89.3% compliant in wearing the hard-acrylic sleep device from ProSomnus; furthermore, 7 out of 10 surveyed were 100% compliant per Medicare guidelines. Survey results showed high levels of positive feedback for all questions, with patients scoring on average 8.5/10 points. While wearing the oral appliance, patients noted an improvement in sleep, the appliance was comfortable and easy to clean, they favored wearing the device for life, and will recommend the device to a friend.
The second survey given to patients during the study was the short version of the SAQLI. For this survey, five patients completed the surveys across two time points, year 1 and year 2, with an average duration of 10.4 months between surveys. For each survey question, the first data point was compared to the second data point, and if the answer was the same, the question scored a 0. If there was improvement of one level, the score was a 1. If the answer decreased in favorability, the question was scored negative to the increments of change, e.g. -1,-2 -3, etc. The most notable area of improvement in quality of life was the reduction in “irritation to snoring”. However, even though on average the scores showed a positive 0.5 step improvement, statistically it would be difficult to make a strong conclusion.
Figure 6Patient survey results (10 = most agreeable to the question) |
{kind=link}
DISCUSSION
Sleep physicians and general dentists often cite side effects as a leading reason to avoid OAT. Of the many possible side effects related to OAT, tooth movement is one that is discussed, and is relatively easy to measure, especially with the advent of digital scanners. When it comes to choosing an oral appliance, clinicians now have a wide variety of appliance designs and materials. Appliances that have areas of stronger pressure, such as ball clasps or open areas, are much more likely to result in tooth movement, rather than an appliance that covers every tooth.11 Similarly, a hard acrylic rigid appliance is likely to provide more tooth stability than a softer appliance.10 An appliance designed with a proprietary CAD/CAM process, made of hard acrylic with an even spacer around all areas in contact with the teeth, is therefore thought to provide enough stability to prevent tooth movement.
The study results show that when patients are compliant in wearing the appliance chosen in this study nightly (ProSomnus® Sleep Appliance) the data report minimal tooth movements, if any. Another significant finding discovered is that when models are hand-articulated into MIP, overjet and overbite did not change. The changes noted in this study appear to be less than in previous oral appliance studies.10 Additionally, a key component to any treatment is acceptance of the oral appliance and the willingness to wear the device long term. Treatment compliance is required to obtain useful efficacy. The survey results demonstrated that patients wore the device at a high rate and would recommend the device to friends and family. This clinical study demonstrates that the proprietary CAD/CAM oral appliance minimizes tooth movement, and patients found the appliance comfortable and favorable. From a clinician’s point of view, these study results can help alleviate concern from three audiences: the patient, a patient’s referring dentist, and a sleep physician. These key findings provide additional evidence and information for dental/orthodontic practitioners when prescribing OAT for OSAHS.
The challenge of understanding the significance of tooth movement by an appliance is understanding the natural amount of tooth movement that may occur without an appliance. Future studies should include a control to establish what is typical tooth movement for a comparative patient population. This can be tricky as a treated versus untreated population may have different degrees of tooth movement. Because the patient may have many factors15 that could affect tooth mobility and subsequent tooth movement due to natural and iatrogenic sources, the authors chose a relative comparison of the patient’s own data to specifically investigate the effect on the device to unwanted tooth movement. The study was limited by the ability to obtain surveys from all participants; many did not respond to further requests to create a complete dataset for the surveys. Understanding the change in the habitual bite was difficult in this case and the authors focused on the MIP of the patients’ models with the data available. A more in-depth look at the patients’ natural s bite via an intraoral scan, and cephalometric analysis and inspection of the temporal mandibular joint may provide a better understanding of bite changes. More studies are suggested to consider the many variables that contribute to occlusal changes and habitual bite changes and the tradeoffs to treating patients experiencing the effects of obstructive sleep apnea.
ACKNOWLEDGMENTS
An IRB protocol for the clinical trial in Canada was approved by the Health Research Ethics Board of Alberta, Canada.
The authors would like to thank and acknowledge support from University of Pacific, Arthur A. Dugoni School of Dentistry, Department of Preventive and Restorative Dentistry (San Francisco, CA). The authors also thank ProSomnus Sleep Technologies (Pleasanton, CA) for financial support, for technical support (3Shape OrthoAnalyzer Software) by Joshua Seefeldt at Argen (San Diego, CA), for statistical support from Colleen Kelly at Kelly Statistical Consulting (San Diego, CA), and the staff at Snore Centre Quarry Park (Calgary, AB, Canada).
REFERENCES
2. Chan AS, Cistulli PA. Oral appliance treatment of obstructive sleep apnea: an update. Curr Opin Pulm Med. 2009;15(6):591-596.
3. Remmers JE, Topor Z, Grosse J, et al. A feedback-controlled mandibular positioner identifies individuals with sleep apnea who will respond to oral appliance therapy. J Clin Sleep Med. 2017;13(7):871-880.
4. Ngiam J, Hons, Phil M, Cistulli PA. Think before sinking your teeth into oral appliance therapy. J Clin Sleep Med.2014;10(12):1293–1294.
5. Pliska BT, Almeida FR. Tooth movement associated with CPAP therapy. J Clin Sleep Med. 2018;14(4):701–702.
6. Uniken Venema J A.M., Stellingsma C, Doff MHJ, Hoekema A. Dental side effects of long-term obstructive sleep apnea therapy: A comparison of three therapeutic modalities. J Dent Sleep Med. 2018;5(2):39-46.
7. Doff MH, Hoekema A, Pruim GJ, Huddleston Slater JJ, Stegenga B. Long-term oral-appliance therapy in obstructive sleep apnea: a cephalometric study of craniofacial changes. J Dent. 2010;38(12):1010-1018.
8. Tsuda H, Almeida F, Tsuda T, Moritsuchi Y, Lowe A. Craniofacial changes after 2 years of nasal continuous positive airway pressure use in patients with obstructive sleep apnea. Chest. 2010;138(4):870–874.
9. Rose JE, Staats R, Virchow C Jr, Irmtrud E. Occlusal and skeletal effects of an oral appliance in the treatment of obstructive sleep apnea. Chest.2002;122(3):871-877.
10. Norrhem N, Nemeczek H, Marklund M. Changes in lower incisor irregularity during treatment with oral sleep apnea appliances; Sleep Breath. 2017;21(3):607-613.
11. Sheats RD, Schell TG, Blanton AO, et al. Management of side effects of oral appliance therapy for sleep-disordered breathing. J Dent Sleep Med. 2017;4(4):111–125.
12. IRB Approval: Health Research Ethics Board of Alberta (https://hreba.ca/) HREBA.CTC-16-0108
13. Bukhari SAAB, Kaladhar A, Reddy C, et al. Evaluation of virtual models (3Shape OrthoSystem) in assessing accuracy and duration of model analyses based on the severity of crowding. The Saudi J Dent Res. 2017; 8 (1-2):11–18.
14. Little RM. The irregularity index: A quantitative score of mandibular anterior alignment. Am J Orthod. 1975;68(5):554-563.
15. Karthik R. Tooth Mobility – Causes and Treatment, December 28, 2018. http://www.drkarthikreddy.com/2015/12/28/tooth-mobility/ Accessed April 2, 2019.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication February 15, 2019
Submitted in final revised form March 19, 2019
Accepted for publication March 29, 2019
Address correspondence to: David Kuhns, PhD, ProSomnus Sleep Technologies, 5860 West Las Positas Blvd., Suite 25, Pleasanton, CA, 94588, Email: dkuhns@prosomnus.com
DISCLOSURE STATEMENT
Drs. Santucci and Schulze received no compensation outside of University of Pacific salaries for this article; Dr. Vranjes and staff were compensated for office time by ProSomnus Sleep Technologies; Mr. Khai was compensated for lab time by ProSomnus Sleep Technologies; Dr. Kuhns is VP of Technology and ProSomnus Sleep Technologies.
The authors Drs. Santucci, Schulze, Vranjes and Allen Khai have no conflicts of interest; Dr. David Kuhns is Chief Science Officer of ProSomnus Sleep Technologies.
PDF