Original Article 2, Issue 4.3
The Efficacy of a Titrated Tongue Stabilizing Device on Obstructive Sleep Apnea and the Quality of Life: A Clinical Trial Study Protocol
http://dx.doi.org/10.15331/jdsm.6680
Kentaro Okuno, PhD1 ; Mona M. Hamoda, BDS, MSc, MHSc1 ; Waled M. Alshhrani, BDS, MS1,2; John A. Fleetham, PhD3 ; Najib T. Ayas, PhD3 ; Robert Comey, MD4 ; Alan A. Lowe, DMD, PhD1 ; Benjamin T. Pliska, DDS, MS, FRCD(C)1 ; Fernanda R. Almeida, DDS, MSc, PhD1
1Department of Oral Health Sciences, Faculty of Dentistry, University of British Columbia, Vancouver, British Columbia, Canada; 2Department of Prosthetic Dental Sciences, College of Dentistry, King Saud University, Riyadh, Saudi Arabia; 3Division of Respiratory Medicine, Department of Medicine, University of British Columbia, Vancouver, British Columbia, Canada; 4Division of Psychiatric Medicine, Department of Medicine, University of British Columbia, Vancouver, British Columbia, Canada
ABSTRACT
Study Objectives:
A tongue stabilization device (TSD) is a preformed appliance that uses suction to maintain the tongue in a protruded position and improves upper airway size and function. TSDs are simple and less expensive than other treatment options currently available for obstructive sleep apnea (OSA), including continuous positive airway pressure (CPAP) and the mandibular advancement device (MAD). The following is a description of an ongoing clinical trial. The main objective of the clinical trial is to determine the efficacy of TSD treatment for sleep-disordered breathing, daytime sleepiness, and quality of life. The second objective is to identify the subjective compliance and side effects of TSD treatment. The third objective is to determine the efficacy of titration of TSDs to compare initial treatment with TSD, 4 mm titrated TSD, and 7 mm titrated TSD.
Methods:
Sixty patients with OSA will be recruited for this study. Each participant will complete a series of validated questionnaires and undergo level III sleep monitoring to evaluate their baseline OSA. The TSD appliances will be provided to each patient and will be titrated to hold the tongue forward in a stepwise fashion using a 4- or 7-mm titration accessory before repeating the questionnaires and sleep monitoring. Finally, we will perform a detailed split-night polysomnography (PSG), half of the night with the TSD and the other half without the device.
Conclusions:
The evidence provided by this trial will improve the management of patients with OSA, especially those who cannot receive or tolerate CPAP and/or a MAD. The results of this trial will reveal the potential of the TSD as a treatment option for OSA.
Clinical Trial Registration:
United States Clinical Trials Registry, ID: NCT02329925.
Keywords:
obstructive sleep apnea, oral appliance, quality of life, tongue stabilization device
Citation:
Okuno K, Hamoda MM, Alshhrani WM, Fleetham JA, Ayas NT, Comey R, Lowe AA, Pliska BT, Almeida FR. The efficacy of a titrated tongue stabilizing device on obstructive sleep apnea and the quality of life: a clinical trial study protocol. Journal of Dental Sleep Medicine. 2017;4(3):65–69.
INTRODUCTION
Obstructive sleep apnea (OSA) is characterized by recurrent episodes of partial or complete upper airway collapse during sleep and is highly prevalent in the general population.1,2 Daytime consequences of OSA include a range of symptoms including excessive sleepiness, neurocognitive impairment, and mood disturbance, which significantly impair quality of life (QOL).3 In addition, there is an increased incidence of cardiovascular mortality, stroke, and heart attack.4–6 Hence, OSA is a major public health problem, imposing a financial burden on health care systems.7,8
There are a variety of treatment options currently available for OSA, ranging from lifestyle modifications such as weight loss, to invasive soft tissue and/or orthognathic surgery. Continuous positive airway pressure (CPAP) is the most efficient treatment for OSA and has been demonstrated to improve many health outcomes, including sleepiness and QOL, and to reduce the incidence of cardiovascular events.9,10 Despite these changes, adherence is often poor, with many patients either rejecting treatment or only partially tolerating it, which can result in untreated OSA.11
Use of a mandibular advancement device (MAD) is a widely used treatment for OSA. Although the overall effect of these devices on sleep-disordered breathing may be inferior to CPAP, adherence is generally higher.12 Sleepiness, blood pressure, and disease-specific QOL improve as a result of treatment by MAD and CPAP by similar amounts.13,14 CPAP and MAD are associated with significant costs.
The tongue stabilization device (TSD) is a preformed appliance that uses suction to hold the tongue in a protruded position, aiming at increasing upper airway size, and is more simple and less expensive than CPAP and MAD. TSD treatment has been reported to improve OSA, with demonstrated reductions in apnea-hypopnea index (AHI) and arousal frequency similar to MAD.15 However, TSD is associated with poorer adherence when compared to MAD treatment.15 Unlike CPAP, where the optimal pressure can be titrated, and MAD, which has the ability to titrate the amount of mandibular protrusion, TSD is limited by the inability to standardize the degree of tongue protrusion, which may be important to maximize the treatment effects.
In our ongoing clinical trial, we will use a newly designed TSD, which has thinner material, to improve patient comfort and the ability to provide some level of titration with the use of 4- and 7-mm titration accessories that act to further protrude the tongue. The main objective of the study is to determine the efficacy of titrated TSD treatment for sleep-disordered breathing (as measured by the AHI), daytime sleepiness (as measure by the Epworth Sleepiness Scale [ESS]), and QOL (as measured by the Chalder Fatigue Scale, The Functional Outcomes of Sleep Questionnaire-10 [FOSQ-10], and Medical Outcomes Study 36-Item Short Form [SF-36]). A second objective is to identify the subjective compliance and side effects of TSD treatment. A third objective is to determine the efficacy of titration of TSDs when compared between initial TSD, 4- and 7-mm titrated TSD positions.
METHODS
Ethical Aspects
The study protocol and participant information documents have been approved by the Clinical Research Ethics Board of the University of British Columbia (H14-01333). The trial is registered in the United States Clinical Trials Registry (NCT02329925). Informed consent will be obtained from each eligible participant before proceeding with the trial.
Inclusion and Exclusion Criteria
A total of 60 patients with OSA will be recruited for the study. To be considered for inclusion in the study, the patients must be older than 18 years, have received a diagnosis of OSA (AHI score or oxygen desaturation index of 5 events/h to 50 events/h), have a body mass index of less than 35 kg/m2 . For the purpose of this study, we have accepted all diagnostic tools used in the community, portable monitor levels III and IV, and full PSG. The participants are excluded if they have had previous soft palate surgery, exhibit a neuromuscular disease, and/or are taking medications that disturb sleep.
Tongue Stabilizing Device
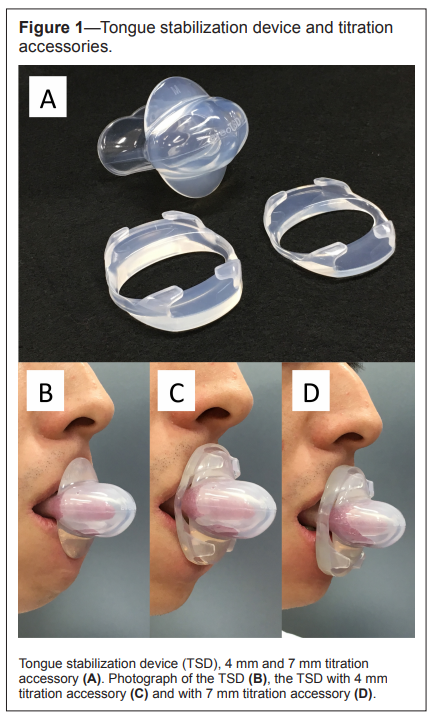
The tongue stabilizing device used in this trial is a preformed silicon appliance that uses suction to hold the tongue in a protruded position and improve the size of the upper airway during sleep (Aveo-TSD, Innovative Health Technologies, New Zealand). Patients are instructed to place the flanges of the TSD on the outside of the upper and lower lips, insert the tongue into the bulb as far as is comfortable, then squeeze and release the bulb to generate suction. Patients are advised to increase the suction by protruding the tongue further and squeezing the bulb more should the device loosen or be insufficiently retentive, or conversely decrease the suction should there be excessive discomfort. A titration accessory for the device will also be used, which attaches to the TSD and results in a greater amount of protrusion of 4 and 7 mm (Figure 1).
Figure 1Tongue stabilization device and titration accessories. |
{kind=link}
Titration Protocol
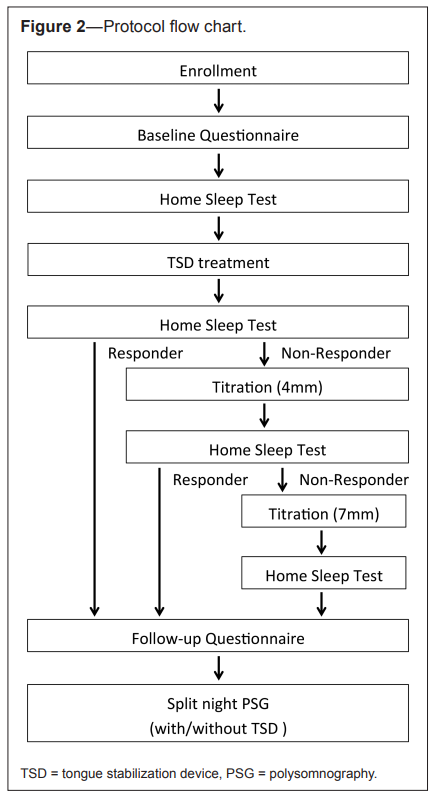
Figure 2 provides a flow chart for the baseline assessment, interventions, and follow-up assessment. Before TSD treatment begins, each participant will complete a series of questionnaires and we will perform a limited sleep study with a level III monitor to evaluate the baseline level of OSA. The TSD appliances will then be provided to each patient along with standardized instructions on use and care. After an acclimatization period of at least 2 months, the subjects will undergo a second limited sleep study to determine treatment effectiveness.
Figure 2Protocol flow chart. |
{kind=link}
A titration protocol will be initiated only for those patients inadequately treated by the initial TSD. The TSD will first be titrated to hold the patient’s tongue forward an additional 4 mm, followed by a 1-month acclimatization period and a follow-up limited sleep study. In a similar fashion, an additional 3 mm of advancement with the 7 mm titration accessory will be added as required, followed again by a limited sleep study. All subjects will undergo a split-night laboratory-based PSG and complete the follow-up questionnaires after a satisfactory response to treatment (a reduction in AHI < 10 events/h and > 50% reduction in AHI) or the maximum amount of comfortable titration has been achieved. Finally, we will compare the results of split-night PSG with TSD and without TSD. We will also analyze and compare the level III portable monitor measurements before and afterward.
Limited Sleep Study
The level III portable monitoring device (MediByte; Braebon Medical Corporation, Ontario, Canada) will be utilized for the titration of the TSD treatment. The portable device consists of two inductance bands for thoracic and abdomen measurement, a nasal cannula pressure transducer airflow signal, finger pulse oximetry, an acoustic microphone for recording snoring sound, and a body position sensor. The description and validation of this portable monitor in 128 valid comparisons of the in-laboratory PSG and portable monitoring device has been previously published.16 With a preset diagnostic AHI cutoff of < 10, the portable monitoring device derived respiratory disturbance index had a sensitivity and specificity of 79% and 86%, respectively.
Participants will be instructed on how to use a portable monitoring device by a dentist and will be given a portable monitoring device to take home and wear for 1 night, with a preaddressed mailer to return the device to the sleep laboratory. Data from the device are autoscored and then manually reviewed by a trained sleep technologist. Apneas are scored when there is a 95% or more reduction in airflow for at least 10 seconds. Hypopneas are scored based on airflow reduction measured by nasal pressure of 30% to 95% from baseline with an accompanying 3% oxygen desaturation.
Polysomnography
At the end of the trial, patients will have an in-laboratory PSG according to standard criteria.17,18 PSG recordings will be conducted in a split-night study, half of the night recording the patient not wearing the TSD and the other half of the night with the TSD in place. Each split-night recording will be continued until the detection of at least one rapid eye movement (REM) sleep period. The order of with/without TSD will be randomized.
Standard measurements will include electroencephalography, electrooculography, submental electromyography, electrocardiography, chest and abdominal respiratory impedance plethysmography, arterial oxygen saturation (pulse oximeter), and nasal airflow (nasal cannulae connected to a pressure transducer).
Respiratory events will be scored according to the criteria published by the American Academy of Sleep Medicine.18 Apnea will be defined as cessation of both nasal and oral airflow with its duration more than 10 seconds. Hypopnea will be defined as a reduction in nasal airflow greater than 30%, with a duration of more than 10 seconds associated with either a decrease in oxygen saturation by at least 3% or an electroencephalography arousal. The AHI will be the mean number of apneas and hypopneas per hour of sleep.
Questionnaires
Specific questionnaires will be used at baseline and after TSD acclimatization and titration according to the protocol. Daytime sleepiness will be assessed by the ESS19 which is an eight-item, four-point scale (0 to 3). Participants will be asked to rate their likelihood of dozing in eight different sedentary situations. The ESS has demonstrated high validity and reliability.20
We will use the Chalder Fatigue Scale to measure fatigue. The questionnaire includes questions about symptoms of mental and physical fatigue. The 11 items assess fatigue and are scored on a Likert scale (0, 1, 2, and 3).21
FOSQ-10 will be used to assess the effect of excessive sleepiness on daily activities. These 10 items are distributed among 5 subscales as follows: general productivity (2 items), activity level (3 items), vigilance (3 items), social outcomes (1 item), and sexual relationship (1 item).22 Items are rated on a scale of 1 to 4 (1 = extreme difficulty, 2 = moderate difficulty, 3 = a little difficulty, 4 = no difficulty). The total score ranges from 5 to 20 and higher scores indicate better functional status.
The QOL measurement will be evaluated by SF-36. It is a standard questionnaire assessing QOL, both in the general healthy population as well as groups of sick patients.23 It consists of 36 questions grouped into 8 domains measuring different aspects of QOL (Physical Functioning, Role Physical, Bodily Pain, General Health, Vitality, Social Functioning, Role Emotional, and Mental Health). The results are converted into a scale from 0 to 100, where 0 indicates the lowest and 100 indicates the highest QOL. The SF-36 also allows summarization of the results into two summary measures: a physical component summary and a mental component summary.
Patients will be asked to keep a sleep diary with the hours of sleep and hours of TSD usage per night for 30 days. Subjective compliance will be evaluated by measuring hours per night and the number of days per week from a sleep diary. Side effects will be described by participants in terms of subjective side effects, device related side effects and sleep related side effects.
Statistical Analysis
All data will be analyzed by SPSS 15.0 statistical software (SPSS Inc., Chicago, IL, United States). The normality of the data distribution will be assessed using the Kolmogorov-Smirnov test. Descriptive statistics for clinical characteristics will presented as a mean ± standard deviation. Continuous variables will be evaluated with a paired t test or Mann-Whitney U test to compare between baseline and follow-up, as appropriate. The categorical variables will be compared using Pearson chisquare or Fisher exact test depending on the number of events. The Kruskal-Wallis analysis of variance will assess the differences in the variables of level III monitor recordings between the degrees of titration of TSD (initial, 4 mm, 7 mm). When the analysis of variance shows a value of P < 0.05, comparisons between the degrees of titration of TSD (initial, 4 mm, 7 mm) will be performed using a Mann-Whitney U test with a Bonferroni correction. A value of P < .05 will be used to indicate statistical significance.
DISCUSSION
This trial will advance the understanding of the effectiveness of titrated TSD treatment for OSA. Because of the high costs associated with the main forms of OSA treatment such as CPAP and MAD, from a public health perspective there is a strong desire to investigate more economic forms of therapy including the TSD.
This trial has a limitation about a split-night PSG. The method of a split-night PSGs has the potential to include low sleep efficiency and short duration or lack of REM sleep. Therefore, each split night recording of half will be continued until the detection of at least one REM sleep period to close to the same sleep stages pattern among split-night PSG ideally. To add to the efficacy assessment, we will also assess before and after TSD with a level 3 portable monitor.
Furthermore, patient populations unsuitable for MAD treatment such as edentulous patients or those with advanced periodontal disease who lack the dental support to tolerate the mandibular protrusion are also likely to benefit from TSD therapy. The evidence provided by this trial will help patients with OSA—especially those who cannot tolerate or afford CPAP and/or MAD—and reveal the potential of the TSD as a treatment option for OSA.
REFERENCES
2. Young T, Evans L, Finn L, Palta M. Estimation of the clinically diagnosed proportion of sleep apnea syndrome in middle-aged men and women. Sleep. 1997;20(9):705–706.
3. Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002;165(9):1217–1239.
4. Young T, Finn L, Peppard P, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep. 2008;31(8):1071–1078.
5. Gottlieb DJ, Yenokyan G, Newman AB, et al. Prospective study of obstructive sleep apnea and incident coronary heart disease and heart failure: the Sleep Heart Health Study. Circulation. 2010;122(4):352–360.
6. Redline S, Yenokyan G, Gottlieb DJ, et al. Obstructive sleep apnea hypopnea and incident stroke: the Sleep Heart Health Study. Am J Respir Crit Care Med. 2010;182(2):269–277.
7. Hillman DR, Murphy AS, Pezzullo L. The economic cost of sleep disorders. Sleep. 2006;29(3):299–305.
8. Jennum P, Kjellberg J. Health, social and economical consequences of sleep-disordered breathing: a controlled national study. Thorax. 2011;66(7):560–566.
9. McDaid C, Durée KH, Griffin SC, et al. A systematic review of continuous positive airway pressure for obstructive sleep apnoeahypopnoea syndrome. Sleep Med Rev. 2009;13(6):427–436.
10. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046–1053.
11. Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc. 2008;5(2):173–178.
12. Lim J, Lasserson TJ, Fleetham J, Wright J. Oral appliances for obstructive sleep apnoea. Cochrane Database Syst Rev. 2004;(4):CD004435.
13. Phillips CL, Grunstein RR, Darendeliler MA, et al. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea: a randomized controlled trial. Am J Respir Crit Care Med. 2013;187(8):879–887.
14. Bratton DJ, Gaisl T, Wons AM, Kohler M. CPAP vs mandibular advancement devices and blood pressure in patients with obstructive sleep apnea: a systematic review and meta-analysis. JAMA. 2015;314(21):2280–2293.
15. Deane SA, Cistulli PA, Ng AT, Zeng B, Petocz P, Darendeliler MA. Comparison of mandibular advancement splint and tongue stabilizing device in obstructive sleep apnea: a randomized controlled trial. Sleep. 2009;32(5):648–653.
16. Pereira EJ, Driver HS, Stewart SC, Fitzpatrick MF. Comparing a combination of validated questionnaires and level III portable monitor with polysomnography to diagnose and exclude sleep apnea. J Clin Sleep Med. 2013;9(12):1259–1266.
17. Rechtschaffen A, Kales A. A Manual of Standardized Terminology, Techniques and Scoring System for Sleep Stages of Human Subjects. Brain Information Service/Brain Research Institute, University of California; 1968.
18. Iber C, Ancoli-Israel S, Chesson AL, Quan SF; for the American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep Associated Events: Rules, Terminology and Technical Specifications. 1st ed. Westchester, IL: American Academy of Sleep Medicine; 2007.
19. Johns MW. A new method for measuring daytime sleepiness: the Epworth Sleepiness Scale. Sleep. 1991;14(6):540–545.
20. Johns MW. Reliability and factor analysis of the Epworth Sleepiness Scale. Sleep. 1992;15(4):376–381.
21. Chalder T, Berelowitz G, Pawlikowska T, et al. Development of a fatigue scale. J Psychosom Res. 1993;37(2):147–153.
22. Chasens ER, Ratcliffe SJ, Weaver TE. Development of the FOSQ-10: a short version of the functional outcomes of sleep questionnaire. Sleep. 2009;32(7):915–919.
23. Ware JE, Kosinski M, Keller SD. SF-36 Physical and Mental Health Summary Scales: A User’s Manual. Boston, MA: The Health Institute, New England Medical Center; 1994.
ACKNOWLEDGMENTS
The trial is funded by the Frontier Clinical Research Centre (grant number: 1403). The treatment device (tongue stabilizing devices) used in this study was provided at no cost by Innovative Health Technologies Ltd., New Zealand. The sleep monitor was provided at no cost by Braebon Medical Corporation MediByte, Canada (MediByte®). The authors would also like to acknowledge the study collaborators: Peter Hamilton, Chris Hilliam, Sandra Harrison, Mary Wong, Samantha Song, Sundus Hussain, and Adam Ludlow.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication May 24, 2016
Submitted in final revised form February 23, 2017
Accepted for publication March 31, 2017
Address correspondence to: Kentaro Okuno, DDS, PhD, Department of Oral Health Sciences, Faculty of Dentistry, The University of British Columbia, 2199 Wesbrook Mall, Vancouver, BC, Canada V6T 1Z3; Email: okuno-kentaro-ig@alumni.osaka-u.ac.jp
DISCLOSURE STATEMENT
The authors declare that they have no competing interests. Funding for this study was provided by Frontier Clinical Research Centre in Faculty of Dentistry, the University of British Columbia (grant number: 1403).