Original Article 2, Issue 4.2
Utilization of a Mandibular Advancement Device for Obstructive Sleep Apnea in the Veteran Population
http://dx.doi.org/10.15331/jdsm.6524
Aaron J. Feinstein, MD, MHS1,2; Michael Zaki, BA1,2; Soroush Zaghi, MD1,2; Tracey Tajima, DDS3 ; Marilene B. Wang, MD1,2
1Department of Head and Neck Surgery, David Geffen School of Medicine at UCLA, Los Angeles, California; 2Department of Surgery, Veterans Affairs Greater Los Angeles Healthcare System, Los Angeles, California; 3Department of Dentistry, Veterans Affairs Greater Los Angeles Healthcare System, Los Angeles, California
ABSTRACT
Study Objectives:
Obstructive sleep apnea (OSA) is a common health problem with significant cardiovascular complications. Nonsurgical treatment options include continuous positive airway pressure as well as mandibular advancement devices (MAD). We sought to determine which factors explain the adherence rate of custom-fit MADs within the military veteran population with OSA.
Methods:
All patients receiving a custom-fit MAD from the Department of Dentistry at a regional veterans health center between December 2007 and August 2013 were retrospectively reviewed. Patient demographic and clinical characteristics were collected and reviewed. Binomial univariate logistic regression models were utilized to assess for the association of these characteristics with the primary outcome: adherence at 6 months after delivery of the MAD.
Results:
There were 48 patients meeting inclusion criteria, with a mean age of 60 years. The mean (standard deviation) body mass index was 30.4 (4.76), and the mean (standard deviation) apnea-hypopnea index on the preintervention polysomnogram was 32.1 (26.5). Adherence among all patients was 66.8% at 2 weeks, and 58.3% at 6 months. Among the subgroup of patients identified as having limiting social circumstances, the adherence was 100% at 2 weeks and 100% at 6 months.
Conclusions:
The MAD is a valuable first-line treatment option for mild or moderate OSA, particularly in patients anticipated to have difficulty complying with continuous positive airway pressure.
Keywords:
continuous positive airway pressure, mandibular advancement device, obstructive sleep apnea, sleep-disordered breathing, veterans
Citation:
Feinstein AJ, Zaki M, Zaghi S, Tajima T, Wang MB. Utilization of a mandibular advancement device for obstructive sleep apnea in the veteran population. Journal of Dental Sleep Medicine. 2017;4(2):37–40.
INTRODUCTION
Obstructive sleep apnea (OSA) is a common health problem in the United States, with an estimated prevalence of 4% in men and 2% in women.1,2 OSA is associated with hypertension, cardiovascular disease, insulin resistance, and asthma, as well as reduced quality of life and increased likelihood of motor vehicle accidents; its treatment is therefore of great importance.3–5 Treatment options include weight loss in overweight patients, continuous positive airway pressure (CPAP), mandibular advancement device (MAD), and surgery focused on the appropriate level of obstruction.6–8
OSA may be suspected after a thorough history and physical examination, but the diagnosis requires confirmation with a polysomnogram (PSG). The initial PSG may include titration for a CPAP machine, which is the most common intervention for OSA.9 CPAP is highly effective; however, many patients find it to be intolerable, and long-term adherence rates in some series are less than 50%.10 Some typically cited reasons for discontinuation of CPAP are bothersome noise, discomfort from the mask, xerostomia, aesthetic appearance, and difficulty transporting the device to different sleep sites. CPAP is meant to be used throughout sleep; however, even the typical metric of 4 h/night is accomplished in only 46% to 83% of patients.10 In the veteran population, when good adherence was defined as use of CPAP on 3 or more nights per week, only 39% to 53% of patients with mild to severe OSA maintained good adherence.11
Oral appliances such as the MAD are frequently recommended for patients with mild or moderate OSA because they are simple to use, noninvasive, and may be tolerated better than CPAP.12 They may be considered first-line treatment in these patients. Randomized controlled trials have shown that they are a good alternative for snoring and OSA because of their low cost, relative comfort, and ease of use, which may result in greater patient adherence.13
With the increasing understanding of the need for adequate treatment of OSA, investigations into the populations most likely to benefit from particular interventions is of great importance. Patients in the veteran population have a high rate of OSA, as well as increased rates of comorbid medical and psychiatric problems.11,14,15 As many as 34% to 47% of veterans are considered to be at high risk for OSA. In addition, there is a greater frequency of socioeconomic challenges and lack of support systems, which can make adherence with medical treatment more difficult.16 Adherence to CPAP in the veteran population has been found to be 50% or less,10,11 and thus an alternative treatment with high ease of use, low cost, and improved tolerability might result in improved adherence. We therefore examined patients within the military veterans population with OSA receiving treatment with a custom-made MAD to understand adherence to the device in this unique patient population.
METHODS
We selected patients receiving treatment for OSA at the Greater Los Angeles Veterans Affairs Healthcare System from December 2007 to August 2013. All patients older than 18 years receiving the MAD fitted by the Department of Dentistry during the period of the study were included for analysis. Patients were eligible for use of the MAD according to Veterans Affairs criteria: mild to moderate OSA, or moderate to severe OSA after failing CPAP, or in conjunction with other modalities; with sufficient periodontally sound teeth, and without significant temporomandibular joint (TMJ) disorders. All patients underwent a detailed discussion about treatment options, including MAD as well as CPAP, prior to electing MAD therapy. The custom-fit Silencer device (Silencer Products International Ltd., Vancouver, BC, Canada )was used in all cases.17 Institutional Review Board A granted approval for this study (# 2014-080869).
Demographic data were collected, including age, sex, and race, as well as clinical data including smoking status, and body mass index (BMI). Reports of overnight PSG performed prior to the delivery of the MAD were reviewed to determine the baseline apnea-hypopnea index (AHI). Patient records were reviewed to search for surgical interventions to treat OSA occurring either before or after delivery of the MAD. Patient-reported adherence was assessed at 2 weeks following delivery of the MAD, when patients had scheduled follow-up with the Department of Dentistry to check the appropriate fit of the device, and also at 6 months, when patients had appointments with the sleep medicine clinic or their primary care physicians. Evaluation of dental disease, occlusion, and TMJ issues were recorded at the initial visit and during subsequent visits. Adverse effects of the device were routinely assessed at these intervals, and patients verbally responded to questions on consistent device use in a dichotomous manner. Patient records were reviewed to identify those patients with limiting social circumstances, such as absent or unstable housing, or those with a need for frequent travel. Patient documentation was systematically entered into a single centralized electronic medical record encompassing the primary hospital-based clinic site as well as affiliate hospitals and outpatient clinics.
Patients with and without limiting social circumstances were analyzed using a χ2 test for categorical variables. Binomial univariate logistic regression models were utilized to assess the association between the demographic and clinical variables and the primary outcome, adherence at 6 months after delivery of the MAD. For all statistical testing, we used a two-sided significance level of .05. Statistical analyses were performed using SPSS software, version 22.
RESULTS
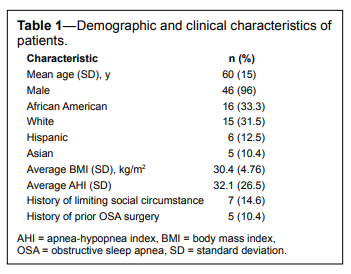
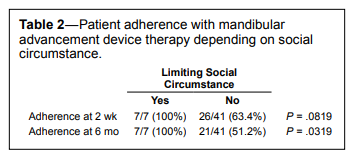
There were 48 patients meeting study inclusion criteria, of whom 96% were male (Table 1). The mean age was 60 years (range, 30–85). The racial distribution was diverse, with 33.3% African American, 31.6% white, 12.5% Hispanic, and 10.4% Asian. Among all patients the mean (standard deviation [SD]) BMI prior to the use of the MAD was 30.4 (4.76). The mean (SD) AHI on the preintervention PSG was 32.1 (26.5), indicating that this cohort consisted of patients with both moderate and severe OSA. There were four patients with unstable living situations, and three patients with very frequent travel, and they were considered to have limiting social circumstances.Overall adherence with the MAD device at 2 weeks after device delivery was 66.8% (n = 33), and overall adherence at 6 months was 58.3% (n = 28). Adherence was defined as patient report of continued use of the device, as we could not reliably measure hours per night or similar definite indicators of use. Among the patients with limiting social circumstances, adherence at 2 weeks was 100% (n = 7) and adherence at 6 months was also 100% (n = 7). Limiting social circumstances was the only factor that was positively associated with MAD adherence at 6 months (Table 2, P = .0319), and among other patients without limiting social circumstances the adherence at the 6-month time point was only 51.2% (n = 21). This indicates that no patients withdrew from treatment in the group with limiting social circumstances, whereas in the group without limiting social circumstances there were 20 patients who withdrew from treatment. Other factors, including age, BMI, AHI, sex, and smoking status, were not statistically significantly associated with adherence at either 2 weeks or 6 months.
Patients reported that reasons for discontinuing use of MAD included xerostomia, drooling, broken device, and dental or mandibular discomfort. Only three patients described intermittent tooth pain, although the relation between pain and use of the MAD or coexistent dental caries was uncertain. There were no cases of incident TMJ pain. No occlusal changes were evident at 6-month follow-up. Notably, five patients had undergone uvulopalatopharyngoplasty prior to attempting use of MAD, and two others proceeded to surgery following unsuccessful trial of MAD. Uvulopalatopharyngoplasty was the only surgical intervention performed in this cohort, although mandibular advancement surgery was recommended but not undertaken for one patient.
Table 1Demographic and clinical characteristics of patients. |
{kind=link}
Table 2Patient adherence with mandibular advancement device therapy depending on social circumstance. |
{kind=link}
DISCUSSION
In this cohort of veterans with OSA, we found that the MAD was a useful nonsurgical treatment option for OSA. Adherence was comparable to that observed in the general population for oral appliances or CPAP, with 58.3% utilizing the MAD at 6 months following device fabrication and delivery. The adherence was higher than that demonstrated in a recent cohort of 207 veteran patients, where only 29.5% were adherent to recommended CPAP therapy.18 Importantly, we identified a subgroup of patients with limiting social circumstances, such as homelessness and frequent travel, and found that among these patients the adherence with MAD was 100%. It is likely that these patients would have great difficulty utilizing a CPAP device, which is frequently bulky, heavy, and requires routine access to electricity. We also did not find significant adverse effects on occlusion or TMJ function.
The discontinuation rate among this group of veterans was greater than that observed in a cohort of 619 patients treated with a custom fabricated MAD, wherein 24% discontinued treatment.19 However, the percentage of women was greater in that group, and because female sex predicted treatment success this may account for the difference in adherence rates. One reason for discontinuation may be the development of dental side effects during treatment, which are known to occur with MAD use.20 However, dental side effects may also be seen with CPAP.21 The patients in our study did not experience significant dental or TMJ side effects. Thus, patients may have discontinued MAD use for other reasons such as perceived efficacy, comfort, or other factors.
Studies comparing MAD to CPAP have shown discordant results in assessing adherence. Doff et al. treated 103 patients with the Thornton Adjustable Positioner (Airway Management, Inc., Dallas, Texas, United States) or CPAP, and found that more patients were noncompliant with oral appliance therapy (47%) than with CPAP (33%), although this finding was not statistically significant.22 However, Phillips et al., utilizing the Somnodent device (SomnoMed Ltd., Sydney, Australia), found that adherence was higher with the MAD than with CPAP (6.5 h/night versus 5.2 h/night, P < .00001).23 Although these compliance rates are discordant, our series demonstrates that compliance with MAD at 6 months was greater than 50%, which is as good or better than reported compliance rates of veterans using CPAP, ranging from 39% to 53%.11 Our data confirm the hypothesis that compliance with MAD would be higher than with CPAP in the veteran population, because of its ease of use, low cost, and improved tolerability, especially for veterans with limiting social circumstances.
There were certain limitations in our study. Postintervention PSGs were not available for all patients, limiting our ability to assess the effectiveness of the treatment. Patient follow-up was inconsistent, with some patients seeking continued care in the sleep medicine clinic, dental clinic, or only with the primary care doctor. This sample was also 96% male, which may limit generalizability to the young veteran population, which includes a higher percentage of females.
In veterans with sleep-disordered breathing, a PSG should be obtained to confirm OSA and assess the severity of disease. These patients should then be counseled on their treatment options, with a discussion of both CPAP and MAD, as well as surgery in selected patients. Holley et al. utilized the Thornton Adjustable Positioner in a military population, and results of their analysis of 497 patients suggested that the appliance was comparable to CPAP for mild OSA, whereas CPAP was clearly better in moderate or severe disease.24 We therefore suggest that the device should be considered as an option for first-line therapy in patients with mild or moderate OSA, and should be preferentially selected for patients with limiting social circumstances or anticipation for extensive travel, where the use of CPAP may not be practical.
CONCLUSIONS
OSA is a chronic disease requiring long-term treatment with potentially uncomfortable devices such as CPAP or MAD. The veteran population has unique challenges, including limiting social circumstances and difficulty with long-term follow up; therefore, adherence to first-line therapy is of great importance. Patients with limiting social circumstances, including homelessness, lack of access to electricity, and frequent travel, demonstrate excellent adherence to MAD treatment.REFERENCES
2. Bixler EO, Vgontzas AN, Lin HM, et al. Prevalence of sleep-disordered breathing in women: effects of gender. Am J Resp Crit Care Med. 2001;163(3 Pt 1):608–613.
3. Nieto FJ, Young TB, Lind BK, et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study. Sleep Heart Health Study. JAMA. 2000;283(14):1829–1836.
4. De Torres-Alba F, Gemma D, Armada-Romero E, Rey-Blas JR, Lópezde-Sá E, López-Sendon JL. Obstructive sleep apnea and coronary artery disease: from pathophysiology to clinical implications. Pulm Med. 2013;2013:768064.
5. Sassani A, Findley LJ, Kryger M, Goldlust E, George C, Davidson TM. Reducing motor-vehicle collisions, costs, and fatalities by treating obstructive sleep apnea syndrome. Sleep. 2004;27(3):453–458.
6. Piccirillo JF, Duntley S, Schotland H. Obstructive sleep apnea. JAMA. 2000;284(12):1492–1494.
7. Berry RB, Kryger MH, Massie CA. A novel nasal expiratory positive airway pressure (EPAP) device for the treatment of obstructive sleep apnea: a randomized controlled trial. Sleep. 2011;34(4):479–485.
8. Strollo PJ, Gillespie MB, Soose RJ, et al. Upper airway stimulation for obstructive sleep apnea: durability of the treatment effect at 18 months. Sleep. 2015;38(10):1593–1598.
9. Epstein LJ, Kristo D, Strollo PJ, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(3):263–276.
10. Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc. 2008;5(2):173–178.
11. Samson P, Casey KR, Knepler J, Panos RJ. Clinical characteristics, comorbidities, and response to treatment of veterans with obstructive sleep apnea, Cincinnati Veterans Affairs Medical Center, 2005-2007. Prev Chronic Dis. 2012;9:E46.
12. Ahrens A, McGrath C, Hägg U. A systematic review of the efficacy of oral appliance design in the management of obstructive sleep apnoea. Eur J Orthod. 2011;33(3):318–324.
13. Ferguson KA, Ono T, Lowe AA, Keenan SP, Fleetham JA. A randomized crossover study of an oral appliance vs nasal-continuous positive airway pressure in the treatment of mild-moderate obstructive sleep apnea. Chest. 1996;109(5):1269–1275.
14. Babson KA, Del Re AC, Bonn-Miller MO, Woodward SH. The comorbidity of sleep apnea and mood, anxiety, and substance use disorders among obese military veterans within the Veterans Health Administration. J Clin Sleep Med. 2013;9(12):1253–1258.
15. Goldstein G, Luther JF, Jacoby AM, Haas GL, Gordon AJ. A Taxonomy of medical comorbidity for veterans who are homeless. J Health Care Poor Underserved. 2008;19(3):991–1005.
16. Villa VM, Harada ND, Washington D, Damron-Rodriguez J. Health and functioning among four war eras of U.S. veterans: examining the impact of war cohort membership, socioeconomic status, mental health, and disease prevalence. Mil Med. 2002;167(9):783–789.
17. Wade PS. Oral appliance therapy for snoring and sleep apnea: preliminary report on 86 patients fitted with an anterior mandibular positioning device, the Silencer. J Otolaryngol. 2003;32(2):110–113.
18. Wohlgemuth WK, Chirinos DA, Domingo S, Wallace DM. Attempters, adherers, and non-adherers: latent profile analysis of CPAP use with correlates. Sleep Med. 2015;16(3):336–342.
19. Marklund M, Stenlund H, Franklin KA. Mandibular advancement devices in 630 men and women with obstructive sleep apnea and snoring: tolerability and predictors of treatment success. Chest. 2004;125(4):1270–1278.
20. Doff MHJ, Finnema KJ, Hoekema A, Wijkstra PJ, de Bont LGM, Stegenga B. Long-term oral appliance therapy in obstructive sleep apnea syndrome: a controlled study on dental side effects. Clin Oral Investig. 2013;17(2):475–482.
21. Tsuda H, Almeida FR, Tsuda T, Moritsuchi Y, Lowe AA. Craniofacial changes after 2 years of nasal continuous positive airway pressure use in patients with obstructive sleep apnea. Chest. 2010;138(4):870–874.
22. Doff MHJ, Hoekema A, Wijkstra PJ, et al. Oral appliance versus continuous positive airway pressure in obstructive sleep apnea syndrome: a 2-year follow-up. Sleep. 2013;36(9):1289–1296.
23. Phillips CL, Grunstein RR, Darendeliler MA, et al. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea: a randomized controlled trial. Am J Resp Crit Care Med. 2013;187(8):879–887.
24. Holley AB, Lettieri CJ, Shah AA. Efficacy of an adjustable oral appliance and comparison with continuous positive airway pressure for the treatment of obstructive sleep apnea syndrome. Chest. 2011;140(6):1511–1516.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication May 24, 2016
Submitted in final revised form February 2, 2017
Accepted for publication February 10, 2017
Address correspondence to: Marilene B. Wang, MD, 200 UCLA Medical Plaza Ste. 550, Los Angeles, CA 90095; Tel: (310) 206-6688; Fax: (310) 794-7083; Email: mbwang@ucla.edu
DISCLOSURE STATEMENT
This was not an industry supported study. The authors have indicated no financial conflicts of interest.