Original Article 2, Issue 3.4
Predicting Therapeutic Outcome of Mandibular Advancement Device Treatment in Obstructive Sleep Apnoea (PROMAD): Study Design and Baseline Characteristics
http://dx.doi.org/10.15331/jdsm.6250
Annelies E.R. Verbruggen, MD1,6; Anneclaire V.M.T. Vroegop, MD, PhD1,6; Marijke Dieltjens, MBS, PHD1,2,6; Kristien Wouters, PhD5 ; Chloé Kastoer, MD1,6; Wilfried A. De Backer, MD, PhD3,4,6; Johan A. Verbraecken, MD, PhD3,4,6; Marc Willemen, Eng3 ; Paul H. Van de Heyning, MD, PhD1,3,6; Marc J. Braem, DDS, PhD2,6; Olivier M. Vanderveken, MD, PhD1,3,6
1Antwerp University Hospital, ENT Department and Head and Neck Surgery, Edegem, Antwerp, Belgium; 2Antwerp University Hospital, Department of Special Dentistry Care, Edegem, Antwerp, Belgium; 3Antwerp University Hospital, Multidisciplinary Sleep Disorders Centre, Edegem, Antwerp, Belgium; 4Antwerp University Hospital, Department of Pulmonary Medicine, Edegem, Antwerp, Belgium; 5Antwerp University Hospital, Department of Scientific Coordination and Biostatistics, Edegem, Antwerp, Belgium; 6University of Antwerp, Faculty of Medicine and Health Sciences, Edegem, Antwerp, Belgium
ABSTRACT
Study Objectives:
Oral appliances have gained their place in the treatment of obstructive sleep apnea (OSA) where custom-made titratable mandibular advancement devices (OAm) have become the oral appliance of choice. Retrospective studies assessing possible predictors of treatment outcome with OAm have been published but are lacking uniformity in their conclusions. The “PRedicting therapeutic Outcome of Mandibular Advancement Device treatment in OSA” (PROMAD) study aims at identifying predictive screening methods for treatment success with OAm, assessing the following upper airway (UA) evaluation methods: awake nasendoscopy including Müller manoeuvre, and drug-induced sedation endoscopy (DISE) will identify the level, degree, and pattern of UA collapse; while computed tomography (CT)-scan based computational fluid dynamics (CFD) will evaluate changes in UA volume and resistance.
Methods:
PROMAD is a prospective, single-center cohort study that enrolled 100 consecutive patients with diagnosed OSA (5 events/h < apnea-hypopnea index (AHI) < 50 events/h) to be treated with a custom-made titratable OAm. Primary endpoints are the positive and negative predictive values of awake nasendoscopy including Müller manoeuvre, DISE, and CFD with and without the OAm, toward reduction in AHI. Univariate and multivariate analyses will be performed to determine which of the investigations and/ or combinations thereof predict success.
Conclusions:
PROMAD is a prospective trial to investigate the predictive potential of awake nasendoscopy including Müller manoeuvre, DISE, and CFD, and any combination thereof in the prediction of reduction of AHI with OAm in OSA patients. The results will allow translating the assessments into optimal OSA patient selection, leading to evidence-based decision making and targeted OAm treatment.
Clinical Trial Registration:
Clinicaltrial.gov identifier: NCT01532050
Keywords:
oral appliance, awake nasendoscopy, sleep endoscopy, computed tomography, computational fluid dynamics
Citation:
Verbruggen AE, Vroegop AV, Dieltjens M, Wouters K, Kastoer C, De Backer WA, Verbraecken JA, Willemen M, Van de Heyning PH, Braem MJ, Vanderveken OM. Predicting therapeutic outcome of mandibular advancement device treatment in obstructive sleep apnoea (PROMAD): study design and baseline characteristics. Journal of Dental Sleep Medicine 2016;3(4):119–138.
INTRODUCTION
Obstructive sleep apnea (OSA) is a highly prevalent disease and public health issue, affecting approximately 34% of middleaged men and 17% of middle-aged women in the United States.1 The condition is characterized by periodic partial or complete obstruction of the upper airway (UA) during sleep, causing sleep fragmentation and hypoxemia.2 The severity of OSA is expressed in terms of the number of apneas and hypopneas per hour of sleep, the apnea-hypopnea index (AHI). OSA poses a strong and independent risk factor for cerebro- and cardiovascular morbidity, associated with high rates of morbidity and mortality.3–7
Continuous positive airway pressure (CPAP) is the advised standard of treatment for patients diagnosed with AHI > 15 events/h.8 However, its clinical effectiveness is limited by moderate patient acceptance and tolerance, leading to unsatisfactory compliance.9–11 The most commonly used class of oral appliances, the mandibular advancement device (OAm), is recommended as a first-line therapy for patients with sleep-disordered breathing, having an AHI of up to 15 events/h, and in patients who fail or refuse treatment with CPAP.12 The OAm is worn intra-orally during sleep and maintains the mandible in a protruded position, commonly with a design to additionally protrude the mandible in search for the most effective protrusion.13–15 The aim is to prevent UA collapse during sleep by increasing the cross-sectional pharyngeal area, thereby reducing snoring and OSA.16–19 However, there is a high interindividual variability in success rate with OAm as reported in the literature.20 Optimal prediction of individual treatment outcome, improving the selection of OSA patients for OAm therapy, is therefore desirable from both therapeutic as well as financial perspectives, although it remains an unresolved key issue.
Awake nasendoscopy including Müller manoeuvre as well as drug-induced sedation endoscopy (DISE) can be used to assess the anatomical level at which snoring and pharyngeal collapse with and without mandibular protrusion21 will occur as well as the pattern of collapse and anatomical abnormalities. These techniques have been suggested as valuable prognostic indicators of successful OAm treatment in the individual patient.22–24
In the past, UA imaging techniques using a three-dimensional and dynamic approach have been applied to study the pathophysiological aspects of OSA.18,25–29 Computer models have been developed according to the principles of computational fluid dynamics (CFD) using transformed data from three-dimensional computer tomography (CT) images of OSA patients. CFD models allow for evaluation of the airflow and the resistance within the pharynx of the individual OSA patient.30,31 In previous studies, CFD is suggested as a potential adequate predictive tool for treatment outcome with OAm in OSA patients.32–34
The “PRedicting therapeutic Outcome of Mandibular Advancement Device treatment in obstructive sleep apnea” (PROMAD) trial aims at identifying the predictive power of awake nasendoscopy including Muller manoeuvre, DISE, and CT-scan based CFD in treatment outcome with OAm. Additionally, the effect of the combination of these techniques and their relative weight, in terms of predicting the treatment outcome with OAm therapy, is explored.
METHODS
Design
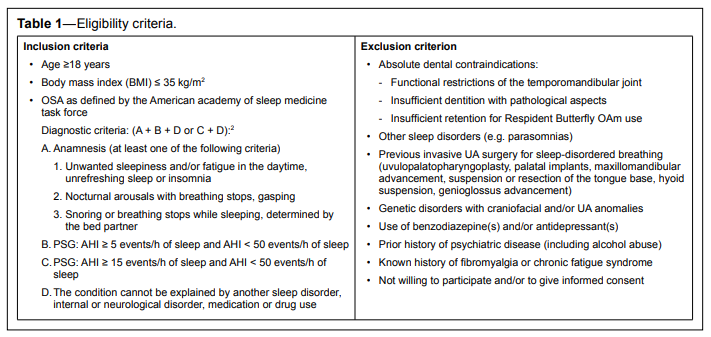
The PROMAD-study is a prospective, single-center, cohort study that evaluates 100 eligible OSA patients. The eligibility criteria are summarized in Table 1.
Table 1Eligibility criteria. |
{kind=link}
A comprehensive characterization of the patients comprises anthropometric data, polysomnography (PSG), awake nasendoscopy including Muller manoeuvre, DISE, and awake UA CT-scan with CFD.
Objective baseline evaluation is performed by PSG, and in particular by assessing the AHI. Then treatment is initiated with a titratable custom-made duobloc OAm (Respident Butterfly, Respident, Orthodontic Clinics NV, Antwerp, Belgium). Re-evaluation by PSG with the OAm in situ is performed after 3 months and 1 year after treatment initiation.
Data analysis of the predictive value of awake nasendoscopy including Müller manoeuvre, DISE, and CT-scan based CFD consists of correlating baseline findings without the OAm in situ with changes in AHI following OAm treatment. Moreover the findings of these same investigations with the OAm in situ in 75% of the individual maximal protrusion will be correlated with the therapeutic outcome. Patients as well as investigators assessing the clinical, polysomnographic, and radiological response remain blinded to the data.
The institutional ethics committee has approved the study protocol and written informed consent is obtained from all participants.
The Mandibular Advancement Device
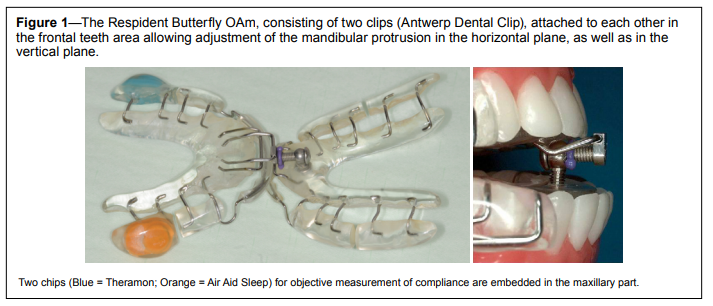
A custom-made, titratable, commercially available duobloc OAm with an interconnecting mechanism located in the frontal teeth area allowing for precise adjustment of mandibular protrusion was selected (Respident Butterfly, RespiDent, Orthodontic Clinics NV, Antwerp, Belgium).35 The appliance consists of two clips (Antwerp DentalClip) (see Figure 1), attached to each other via a small screw system located in the frontal teeth area (Nelissen Titrator) allowing for additional gradual titration. The device is set at 75% of the individual maximal protrusion of each patient. The vertical opening, being the distance between the incisal edges of the upper and lower incisors, is kept constant during the treatment on a minimal distance.36
Figure 1The Respident Butterfly OAm, consisting of two clips (Antwerp Dental Clip), attached to each other in the frontal teeth area allowing adjustment of the mandibular protrusion in the horizontal plane, as well as in the vertical plane. |
{kind=link}
Two temperature-sensitive microsensors with on-chip integrated readout electronics were embedded in the OAm on opposites sides of the maxillary part, to objectively measure the therapy compliance (TheraMon, Handelsagentur Gschladt, Hargelsberg, Austria37–39; and Air Aid Sleep, Air Aid GmbH & Co. KG, Frankfurt am Main, Germany39) (Figure 1).
Polysomnography
A standard full-night PSG is performed (Brain RT software, OSG, Belgium) at baseline to verify the inclusion PSG criteria and to fix the starting point of the study, followed by evaluation after 3 months and after 1 year of OAm therapy. The PSG provides information on respiration, oxygen saturation, and sleep state, as well as on body position, heart rhythm, limb movements and snoring. It comprises recording of respiratory data, including nasal airflow by using an external thermistor, nasal pressure by means of a nasal pressure cannula and respiratory effort through respiratory induction plethysmography. Oxygen saturation is monitored using a pulse oximeter with a finger probe. A microphone qualitatively records snoring, and body position is assessed with a piezoelectric sensor. The PSG includes electroencephalography (EEG), right and left electrooculography, electromyography of the genioglossus muscle and tibialis anterior muscle, and electrocardiography. All sleep records are scored manually according to the American Academy of Sleep Medicine criteria,40 by the same qualified sleep technician. The sleep technician is blinded to the results of the other examinations.
Assessment of Subjective Complaints and Quality of Life
Subjective information is collected by digital versions of different relevant questionnaires. The Epworth Sleepiness Scale (ESS) is used to assess excessive daytime sleepiness.41 The visual analogue scale (VAS) for snoring scores the snoring on a scale of 0 (no snoring) to 10 (partner leaves the bedroom). The Functional Outcomes of Sleep Questionnaire (FOSQ)42 determines the functional status in adults with OSA. The Sleep Apnea Quality of Life Index (SAQLI)43 questions the OSA-related quality of life. The Pittsburgh Sleep Quality Index (PSQI)44 assesses sleep quality and disturbances. The Type D Scale-14 (DS14)45 measures negative affectivity and social inhibition. The NEO-Five Factor Inventory (NEO-FFI46) explores the five domains of the adult personality. The Short Form Health Survey (SF-36)47 investigates the patients’ health status. The Beck Depression Inventory (BDI)48 evaluates mood disturbances.
Study Protocol
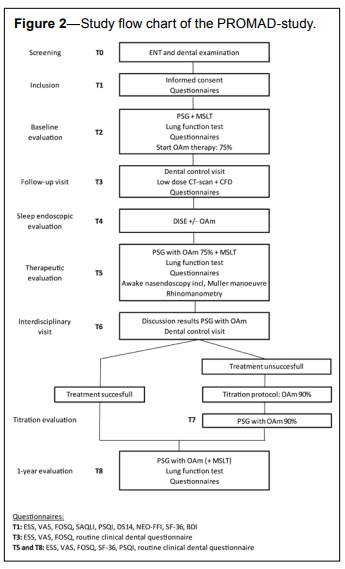
As illustrated in Figure 2, at T0, patients are screened and complete assessment of the patient status is performed, including medical history, standard ear-nose-throat clinical examination with awake upright nasendoscopy including the Muller manoeuvre and rhinomanometry. The patient is then referred to the dental sleep professional for a general dental examination including an orthopantomography. If the patient meets the eligibility criteria and wants to participate in the PROMAD-study, informed consent is obtained and dental impressions are taken (T1). Different questionnaires, as specified in the previous section, were digitally filled out using touch screen technology.
Figure 2Study flow chart of the PROMAD-study. |
{kind=link}
At T2, a baseline full-night PSG in the sleep laboratory is performed, including lung function testing, arterial blood gas analysis, and a clinical questionnaire as routinely used in the sleep laboratory (see Appendix 1 for the English translated version). In the 19 days prior to the baseline PSG, the patients fill out each day an ESS questionnaire on paper, a sleep diary with the sleeping and waking times, and the PSQI. The day after T2, PSG is followed by a multiple sleep latency test (MSLT) and the start of the OAm therapy upon fitting of the OAm in the 75% protrusive position of the individual patient.
A first follow-up visit is planned 1 month after the start of OAm therapy (T3) and includes a dental checkup with control of the protrusive position at 75%. Subsequently, a low-dose CT scan of the head and neck region is made with and without the OAm in the 75% protrusive position, for CFD analysis including level diagnosis. At this time, subjective information is again collected through digital versions of the following questionnaires: ESS, VAS for snoring, FOSQ, and a clinical dental questionnaire (see Appendix 2) as routinely used in our multidisciplinary clinic. Between 1 and 3 months after T2, a DISE (T4) is performed with and without the OAm in the 75% protrusive position.
Three months after initiating OAm therapy (T5), a full-night PSG is performed with the OAm in the 75% protrusive position, including lung function testing, arterial blood gas analysis, and the routine clinical sleep questionnaire, as described before. Prior to T5, the patient fills out again the sleep diary and the ESS each day for 19 days, as well as the PSQI. Other subjective information is again collected through digital versions of the following questionnaires: ESS, VAS for snoring, FOSQ, SF-36, PSQI, and the routine clinical dental questionnaire. Prior to the PSG, a dental examination is conducted with control of the 75% protrusive position of the OAm. The next day, MSLT, rhinomanometry, and awake nasendoscopy including Muller manoeuvre are performed.
Four weeks after T5, an interdisciplinary visit at the dental and medical outpatient clinic is scheduled (T6) and the results of the PSG evaluation with the OAm are discussed with the patient. From this point on, patients and investigators are not blinded anymore to the results of the investigations. In case the remaining AHI with the OAm in situ is higher than 5 events/ hour, the study protocol requires further adjustment of protrusion in order to lower the AHI: the patient is invited to participate in a titration protocol with advancement of the mandible to 90% of the baseline maximal protrusion. The OAm is then fixed in this 90% protrusive position. After a habituation and adaptation period of 2 months, an additional PSG is performed to assess the effect of the 90% protrusive position on AHI (T7).
One year after initiation of treatment a PSG is scheduled in all study patients, with the OAm in either 75% or 90% protrusive position, depending on the patient (T8). Also lung function testing and arterial blood gas analysis are performed. In case of previously pathological MSLT results, the PSG is followed by MSLT the next day. At this time, the patient is also examined by the dental sleep professional to check the condition of the OAm as well as its protrusive position. The questionnaires as on T5 are completed again.
Data collection occurs at screening (T0), at baseline assessment (T2), 1-month follow-up (T3), during DISE (T4), at 3-month follow-up (T5), after titration if needed (T7), and 1 year (T8) after starting therapy. Objective and subjective compliance are verified at T3, T5, and T8.
Study Population and Enrolment
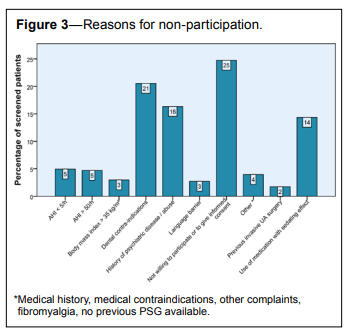
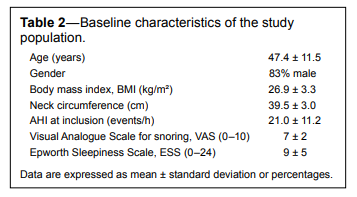
The PROMAD investigators screened consecutively 402 OSA patients diagnosed with recent PSG, from January 2012 until March 2014 at the Antwerp university hospital (UZA, Belgium). Patients were referred to the special care dentistry unit for treatment with an OAm. A group of 202 of these patients did not fulfil the eligibility criteria as defined by the PROMAD study protocol, and 58 (29%) of these patients had more than one reason for non-participation. One hundred invited patients declined to participate because of personal considerations or the inability to comply with the time demands of the protocol (Figure 3). One hundred eligible patients were enrolled, of whom 38 patients had mild OSA (5 events/h < AHI < 15 events/h), 41 patients had moderate OSA (15 events/h < AHI < 30 events/h), and 21 patients had severe OSA (30 events/h < AHI < 50 events/h). The baseline characteristics of the patients are summarized in Table 2. The last baseline PSG was performed in June 2014.
Figure 3Reasons for non-participation. |
{kind=link}
Table 2Baseline characteristics of the study population. |
{kind=link}
Multiple Sleep Latency Test (MSLT)
The MSLT is an objective assessment of the tendency to fall asleep, and requires EEG evaluation of the participants. The day after the PSG, the patient is lying on a bed in a quiet, darkened room and is instructed to fall asleep. The test is conducted according to the standard practice of the American Academy of Sleep Medicine.49 The time required to reach the first epoch of any sleep stage is determined in a 20-minute period every 2 hours during the day for a total of 4 test sessions. The mean sleep latency is then calculated and is considered pathological if it is less than 8 minutes and normal if it is longer than 10 minutes. Nineteen days prior to the testing, the patient is asked to keep a sleep diary reporting the patient’s sleeping and waking times.Imaging with Computational Fluid Dynamics Analysis
All patients undergo a low-radiation dose CT scan with and without the OAm in 75% of the protrusive position, to evaluate the UA geometry. This scan is performed while awake and in supine position during one breath hold at the end of a normal inspiration. The scanned area starts at the nasopharynx and extends down to the larynx. Based on these images, three-dimensional computer-aided design models of the segments of interest can be reconstructed using a commercial software package (Mimics, Materialise, Leuven, Belgium), based on Hounsfield units. These models are then exported and used for detailed analysis of the anatomical parameters, volume meshing, and CFD simulation, as previously described.30,32,33 CFD outcome parameters describe changes in volume of the UA as well as changes in resistance of the simulated amount of air passing through this airway.Drug-Induced Sedation Endoscopy
Drug-induced sedation endoscopy (DISE) is performed by an experienced ENT surgeon in a semi-dark and silent operating theatre with the patient lying in supine position in a hospital bed.50 The OAm in 75% protrusive position is placed intraorally and verified by the dental sleep professional, prior to the intravenous administration of sedative drugs. Artificial sleep is induced by an intravenous bolus administration of 1.5 mg midazolam and a target-controlled infusion of Propofol (2.0–3.0 µg/mL).50 During the procedure, standard cardiovascular monitoring is carried out. The level of sedation is continuously assessed by a bispectral index (BIS) monitoring system (BIS VISTA monitor; Aspect Medical Systems Inc., Norwood, USA) which involves a leaf of four sensor electrodes (BIS Quatro; Aspect Medical Systems Inc., Norwood, USA) attached to the forehead. It records values between 0, when there is no brain activity, and 100, representing the patient is fully awake.51 DISE assessment in the PROMAD study protocol is conducted at BIS values between 50 and 70.A flexible fiberoptic nasopharyngoscope (Olympus END-GP, diameter 3.7 mm, Olympus Europe GmbH, Hamburg, Germany) is inserted transnasally, and the different levels of the UA are observed. The presence of UA collapse is reported using a standard scoring system (Figure 4),23 assessing the level, the degree, and the direction of the collapse pattern.23 First, the UA dimensions are assessed with the OAm positioned intraorally during at least 5 minutes with BIS values between 50 and 70. Next, the OAm is removed by the dental sleep professional, allowing assessment of the UA in a baseline setting without any mandibular repositioning, and with a minimal duration of 5 minutes. Thereafter, the dental sleep professional brings the mandible in the maximal protrusive position by pulling it gently forward, also referred to as the chin-lift manoeuvre. This phase lasts for 2 minutes and allows for the observation of the effects of maximal protrusive positioning on the UA collapse patterns.
Figure 4A standard scoring system for DISE, classified per UA level. |
{kind=link}
Awake Nasendoscopy Including Müller Manoeuvre
At screening (T0) and the day after the PSG with the OAm in situ (T5), a nasopharyngoscopy is performed with a flexible fiberoptic nasopharyngoscope (Olympus END-GP, diameter 3.7 mm, Olympus Europe GmbH, Hamburg, Germany) by a single ENT surgeon and while the patient is awake. At T5, the endoscopy is performed with and without the OAm in situ, both in supine and upright position. In each of the 4 phases of this examination, the patient is asked to simulate snoring and to perform a Müller manoeuvre. For this manoeuvre, both nose and mouth are occluded and the patient is asked to inhale maximally. During the awake endoscopy, the degree, the level, and the pattern of UA collapse are observed and scored using the same scoring system as during DISE.23?Treatment Outcome Measures
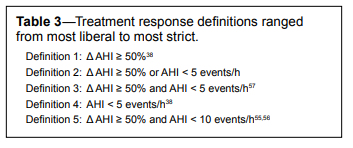
The PROMAD study will explore the predictive value of awake nasendoscopy including Müller manoeuvre, DISE and CFD with and without the OAm in the 75% protrusive position on treatment outcome, determined on T5. For those patients who are unsuccessfully treated at T5, the predictive value of the baseline findings during the investigations will be further analyzed on treatment outcome at T7 with the OAm in 90% protrusion.Regarding the AHI, several definitions of success can be found in the literature,38,52–58 with or without requirement for symptomatic improvement. In the PROMAD study, we will analyze the data according to five various definitions of success, shown in Table 3. Since patients are included based on an AHI ≥ 5 events/h, the main definition of treatment response is that “Δ AHI ≥ 50% or AHI < 5 events/h”.
Table 3Treatment response definitions ranged from most liberal to most strict. |
{kind=link}
Data Collection and Statistical Analysis
Data are stored in Open Clinica (Open Clinica LLC, Waltham, USA, Version: 3.1.4.1), an open source clinical trial software for electronic data capture and clinical data management. Data will be statistically analyzed using R statistical software (R version 3.0.1, R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics for clinical characteristics of patients will be presented as mean ± standard deviation for continuous, normally distributed variables and median, Q1-Q3 for non-normally distributed variables. Unpaired t-tests will be used to compare baseline measurements between responders and non-responders when data are normally distributed. Nonparametric tests will be used in case the variables are not normally distributed. Categorical variables will be analysed using χ2 tests. Multiple logistic regression models will be used to predict response versus non-response based on baseline measurements of the screening procedures correcting for confounding factors. Sensitivity, specificity, and positive (PPV) and negative predictive value (NPV) will be calculated for each of the screening measurements together with their 95% confidence interval. A p value of < 0.05 will be considered statistically significant.Sample Size Justification
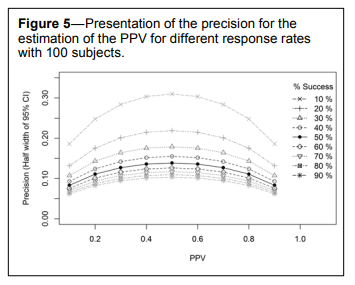
To accurately estimate the positive predictive value (PPV), we included 100 subjects in the study. In Figure 5, the precision for the PPV is presented for different response rates with 100 subjects: with a response rate of 50%, we are able to estimate a PPV of 0.5 with a precision (i.e., half width of 95% confidence interval, CI) of 0.125. For a lower or a higher PPV, the precision is improved. Since we expect the response rate to be lower than in studies with a preselected group of patients,35 a response rate of 50% seems realistic. In case the response rate turns out to be higher, the precision reduces, if the response rate is lower, the precision improves.
Figure 5Presentation of the precision for the estimation of the PPV for different response rates with 100 subjects. |
{kind=link}
This study is not powered to reveal differences in odds for each individual measurement in the screening procedure. Instead our goal is to find a combination of screening measurements that can predict treatment success. Results need to be confirmed in a second trial, which will be powered based on the odds ratios and prevalence rates found in the current study.
DISCUSSION
OAm therapy is increasingly used in clinical practice to treat snoring and OSA and has emerged as a valuable alternative for CPAP treatment. The OAm therapy is proven to be efficient in reducing snoring and obstructive breathing events, and it has shown beneficial effects on associated health outcomes such as daytime sleepiness. However, a major issue confronting OAm therapy is that one-third of the patients undergoing such a therapy do not show a beneficial response in terms of reduction in AHI. The inability to adequately and consistently predict treatment outcome potentially results in suboptimal patient selection. Predicting the effectiveness of OAm therapy in the individual patient is a clinical challenge and is important from both treatment and cost-benefit point of view. Ideally the selection procedure has to be accurate, feasible, easily accessible and cost-effective.
However, the search for a predictive model is complicated. First, there are the variety of mechanisms that underlie OSA, such as UA dilator muscle response, ventilator control instability, and anatomic compromise.59 The interaction between those mechanisms is complex and not yet completely understood. Second, there is the mode of action of the OAm, with both anatomical and functional aspects determining treatment efficacy. The relative contributions of these factors will differ among patients, impeding straightforward prediction of treatment outcome. A single structural or functional assessment may prove to be inadequate to accurately predict treatment outcome in all patients. The combination of patient characteristics, structural, and functional assessments may therefore increase the predictive value of the individual techniques. Third, a complicating factor is the use of a variety of definitions of treatment success in literature (see Table 3). Treatment success is variously expressed as a reduction in AHI below a specific value or by a percentage reduction in AHI from baseline, with or without requirement for symptomatic improvement. In the PROMAD study, data will be evaluated using different definitions of success (see Table 3). A commonly used surgical criterion of success that is not mentioned in Table 3 is “Δ AHI ≥ 50% and postoperative AHI < 20 events/h”: the original criterion, however, as published by Sher,58 was stated as a change in apnea index (AI) or respiratory disturbance index (RDI) of at least 50% and a post-surgery AI below 10 events/h or a post-surgery RDI below 20 events/h. As those parameters currently have become obsolete in describing success, this criterion is not listed in the table. Other commonly used criterions of success not mentioned in our listing are “AHI < 10 events/h.” 54 and “Δ AHI ≥ 50% or AHI < 10 events/h.” 53 These definitions are not used because they are not suitable to the sample as the inclusion criterion for participation to the study is baseline AHI > 5 events/h. The main definition of treatment response used in the PROMAD study, being “Δ AHI ≥ 50% or AHI < 5 events/h,” is rather unusual but dictated by one of the main inclusion criteria, namely baseline AHI ≥ 5 events/h.
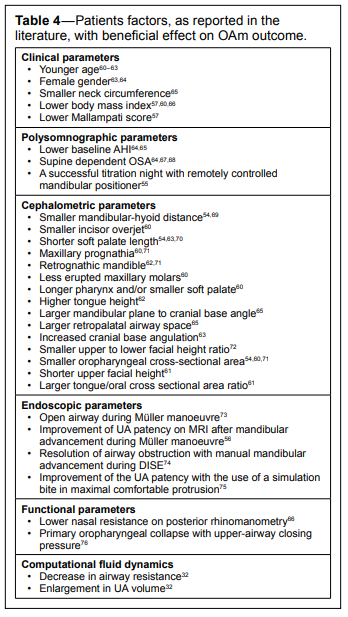
Previous research, mostly relying on retrospective analysis, showed several anthropometric, polysomnographic, physiologic, and anatomical factors to be associated with OAm success (see Table 4). However, those studies lack uniformity, are mostly underpowered, and the results are not always consistent. Furthermore, the indicators of success have often not been tested prospectively, prior to appliance construction. Therefore, the proof on predictability is still rather limited and research is ongoing. In this study, each distinct investigation gives rise to several variables that are prospectively collected and of which the predictive value will be analyzed. For example, for the findings during DISE we will perform an extensive analysis based on the level, the degree, the direction, and specific collapse patterns. A strength of the present study is that data of the investigations are collected in baseline circumstances as well as with the OAm in situ in 75% of the maximal individual protrusion. Thus predictability can be investigated in a prospective way, based on baseline findings as well as based on the findings with the OAm in situ. In addition, collection of the data from awake nasendoscopy, DISE, and CFD was performed in a blind fashion, meaning that the treating dentist and sleep physician were blinded to the results of the other investigations. As such, included patients were treated with the OAm in a fixed degree of protrusion regardless of the results of the investigations.
Table 4Patients factors, as reported in the literature, with beneficial effect on OAm outcome. |
{kind=link}
The screening of possible candidates for the study took a long time as a result of the strict eligibility criteria that caused the exclusion of many patients. However, a rigorous screening is necessary to obtain a homogeneous group of patients to achieve accurate predictive factors, without interaction of confounding factors biasing the study outcome. We had to screen 402 patients during 27 months to include 100 patients in the study who fulfilled all criteria for inclusion and exclusion in the PROMAD trial. The most common reason for exclusion is dental-related pathology as found in 83 patients (20%), including an insufficient number of teeth, periodontal disease, fragile crown and bridge restorations, limited protrusive capacity, and dentition with pathological aspects. It is important to mention that we evaluated this contraindication as a function of the particular type of OAm used in this study for which an optimal dentition is required to guarantee adequate retention. Therefore, the absolute rate of dental contraindications for OAm in general will be lower than in the present study. Compared to the literature, the present rate of exclusion on dental aspects is clearly lower than the 34% reported earlier in 200277. A history of psychiatric disease or alcohol or substance abuse was found in 17% of the patients (n = 66). A study performed in 6 European countries including Belgium, reported a prevalence of 25% for a lifetime presence of any mental disorder, including anxiety disorders, mood disorders, and alcohol dependence.78
In a previous study, we found a prevalence of 18% to 32% of residual excessive sleepiness based on ESS-scores despite successful OAm treatment (AHI < 5 events/h).79 In the PROMAD-study, MSLTs are additionally performed to obtain the prevalence of residual excessive sleepiness in a prospective way and based on objective tests as well. This is performed in a homogenous group of patients without confounding factors such as medical or psychiatric comorbidities and vigilance-influencing medication.
CONCLUSIONS
The PROMAD study prospectively identifies which of the several previously published predictive factors of success with OAm therapy would adequately forecast success of OAm. It is a prospective nonrandomized observational study that evaluates pre-defined baseline parameters for their ability to predict clinical and polysomnographic response to OAm treatment in OSA patients. Given the prospective nature of data in the PROMAD study, we will be able to fully characterize these patients and identify important and potentially new predictive factors for treatment outcome with OAm. The advantages of each of the individual pre-treatment investigations will be combined with the aim of translating it into an optimal selection procedure, leading to an evidence based decision making and targeted treatment of patients with OSA.ABBREVIATIONS
AHI, apnea-hypopnea indexBDI, Beck depression index
BIS, bispectral index
BMI, body mass index
CFD, computational fluid dynamics
CI, confidence interval
CPAP, continuous positive airway pressure
CT, computer tomography
DISE, drug-induced sedation endoscopy
DS14, type D scale-14
EEG, electroencephalography
ESS, Epworth Sleepiness Scale
FOSQ, functional outcomes of sleep questionnaire
MSLT, Multiple Sleep Latency Test
NEO-FFI, NEO-Five factor inventory
NPV, negative predictive value
OAm, mandibular advancement device
OSA, obstructive sleep apnea
PPV, positive predictive value
PROMAD, predicting therapeutic outcome of mandibular advancement treatment in obstructive sleep apnea
PSG, polysomnography
PSQI, Pittsburgh Sleep Quality Index
SAQLI, sleep apnea quality of life index
SF-36, short form health survey
UA, upper airway
VAS, visual analogue score
REFERENCES
2. Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. Sleep 1999;22:667–89.
3. Vanderveken OM, Boudewyns A, Ni Q, et al. Cardiovascular implications in the treatment of obstructive sleep apnea. J Cardiovasc Transl Res 2011;4:53–60.
4. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 2005;365:1046–53.
5. Bradley TD, Floras JS. Obstructive sleep apnoea and its cardiovascular consequences. Lancet 2009;373:82–93.
6. Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med 2005;353:2034–41.
7. Somers VK, White DP, Amin R, et al. Sleep apnea and cardiovascular disease: an American Heart Association/American College of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council on Cardiovascular Nursing. J Am Coll Cardiol 2008;52:686–717.
8. Sullivan CE, Issa FG, Berthon-Jones M, Eves L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet 1981;1:862–5.
9. Grote L, Hedner J, Grunstein R, Kraiczi H. Therapy with nCPAP: incomplete elimination of sleep related breathing disorder. Eur Respir J 2000;16:921–7.
10. Lindberg E, Berne C, Elmasry A, Hedner J, Janson C. CPAP treatment of a population-based sample--what are the benefits and the treatment compliance? Sleep Med 2006;7:553–60.
11. Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc 2008;5:173–8.
12. Kushida CA, Morgenthaler TI, Littner MR, et al. Practice parameters for the treatment of snoring and Obstructive Sleep Apnea with oral appliances: an update for 2005. Sleep 2006;29:240–3.
13. Dieltjens M, Vanderveken OM, Heyning PH, Braem MJ. Current opinions and clinical practice in the titration of oral appliances in the treatment of sleep-disordered breathing. Sleep Med Rev 2012;16:177–85.
14. Gagnadoux F, Fleury B, Vielle B, et al. Titrated mandibular advancement versus positive airway pressure for sleep apnoea. Eur Respir J 2009;34:914–20.
15. Fleury B, Rakotonanahary D, Petelle B, et al. Mandibular advancement titration for obstructive sleep apnea: optimization of the procedure by combining clinical and oximetric parameters. Chest 2004;125:1761–7.
16. Randerath WJ, Verbraecken J, Andreas S, et al. Non-CPAP therapies in obstructive sleep apnoea. Eur Respir J 2011;37:1000–28.
17. Tsuiki S, Lowe AA, Almeida FR, Kawahata N, Fleetham JA. Effects of mandibular advancement on airway curvature and obstructive sleep apnoea severity. Eur Respir J 2004;23:263–8.
18. Chan AS, Sutherland K, Schwab RJ, et al. The effect of mandibular advancement on upper airway structure in obstructive sleep apnoea. Thorax 2010;65:726–32.
19. Kato J, Isono S, Tanaka A, et al. Dose-dependent effects of mandibular advancement on pharyngeal mechanics and nocturnal oxygenation in patients with sleep-disordered breathing. Chest 2000;117:1065–72.
20. Ferguson KA, Cartwright R, Rogers R, Schmidt-Nowara W. Oral appliances for snoring and obstructive sleep apnea: a review. Sleep 2006;29:244–62.
21. Vanderveken OM, Vroegop AV, van de Heyning PH, Braem MJ. Druginduced sleep endoscopy completed with a simulation bite approach for the prediction of the outcome of treatment of obstructive sleep apnea with mandibular repositioning appliances. Operative Techniques in Otolaryngology-Head and Neck Surgery 2011;22:175–82.
22. Battagel JM, Johal A, Kotecha BT. Sleep nasendoscopy as a predictor of treatment success in snorers using mandibular advancement splints. J Laryngol Otol 2005;119:106–12.
23. Vroegop AV, Vanderveken OM, Dieltjens M, et al. Sleep endoscopy with simulation bite for prediction of oral appliance treatment outcome. J Sleep Res 2013;22:348–55.
24. Ryan CF, Love LL, Peat D, Fleetham JA, Lowe AA. Mandibular advancement oral appliance therapy for obstructive sleep apnoea: effect on awake calibre of the velopharynx. Thorax 1999;54:972–7.
25. Stuck BA, Maurer JT. Airway evaluation in obstructive sleep apnea. Sleep Med Rev 2008;12:411–36.
26. Ikeda K, Ogura M, Oshima T, et al. Quantitative assessment of the pharyngeal airway by dynamic magnetic resonance imaging in obstructive sleep apnea syndrome. Ann Otol Rhinol Laryngol 2001;110:183–9.
27. Schwab RJ, Pasirstein M, Pierson R, et al. Identification of upper airway anatomic risk factors for obstructive sleep apnea with volumetric magnetic resonance imaging. Am J Respir Crit Care Med 2003;168:522–30.
28. Yucel A, Unlu M, Haktanir A, Acar M, Fidan F. Evaluation of the upper airway cross-sectional area changes in different degrees of severity of obstructive sleep apnea syndrome: cephalometric and dynamic CT study. AJNR Am J Neuroradiol 2005;26:2624–9.
29. Kyung SH, Park YC, Pae EK. Obstructive sleep apnea patients with the oral appliance experience pharyngeal size and shape changes in three dimensions. Angle Orthod 2005;75:15–22.
30. Vos W, De Backer J, Devolder A, et al. Correlation between severity of sleep apnea and upper airway morphology based on advanced anatomical and functional imaging. J Biomech 2007;40:2207–13.
31. Jeong SJ, Kim WS, Sung SJ. Numerical investigation on the flow characteristics and aerodynamic force of the upper airway of patient with obstructive sleep apnea using computational fluid dynamics. Med Eng Phys 2007;29:637–51.
32. De Backer JW, Vanderveken OM, Vos WG, et al. Functional imaging using computational fluid dynamics to predict treatment success of mandibular advancement devices in sleep-disordered breathing. J Biomech 2007;40:3708–14.
33. Van Holsbeke C, De Backer J, Vos W, et al. Anatomical and functional changes in the upper airways of sleep apnea patients due to mandibular repositioning: a large scale study. J Biomech 2011;44:442–9.
34. Zhao M, Barber T, Cistulli P, Sutherland K, Rosengarten G. Computational fluid dynamics for the assessment of upper airway response to oral appliance treatment in obstructive sleep apnea. J Biomech 2013;46:142–50.
35. Dieltjens M, Vanderveken OM, Hamans E et al. Treatment of obstructive sleep apnea using a custom-made titratable duobloc oral appliance: a prospective clinical study. Sleep Breath 2013;17:565–72.
36. Vroegop AV, Vanderveken OM, Van de Heyning PH, Braem MJ. Effects of vertical opening on pharyngeal dimensions in patients with obstructive sleep apnoea. Sleep Med 2012;13:314–6.
37. Dieltjens M, Braem MJ, Vroegop AV, et al. Objectively measured vs self-reported compliance during oral appliance therapy for sleepdisordered breathing. Chest 2013;144:1495–502.
38. Vanderveken OM, Dieltjens M, Wouters K, De Backer WA, Van de Heyning PH, Braem MJ. Objective measurement of compliance during oral appliance therapy for sleep-disordered breathing. Thorax 2013;68:91–6.
39. Kirshenblatt S, Chen H, Lowe A, Pliska B, Almeida F. Microsensor technology to monitor compliance with removable oral appliances. Sleep Breath 2013;17:879–94.
40. Iber C, Ancoli-Israel S, Chesson AL Jr., Quan SF, for the American Academy of Sleep Medicine. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications. Westchester, IL: American Academy of Sleep Medicine, 2007.
41. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep 1991;14:540–5.
42. Weaver TE, Laizner AM, Evans LK, et al. An instrument to measure functional status outcomes for disorders of excessive sleepiness. Sleep 1997;20:835–43.
43. Flemons WW, Reimer MA. Development of a disease-specific healthrelated quality of life questionnaire for sleep apnea. Am J Respir Crit Care Med 1998;158:494–503.
44. Buysse DJ, Reynolds CF, 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 1989;28:193–213.
45. Denollet J. DS14: standard assessment of negative affectivity, social inhibition, and Type D personality. Psychosom Med 2005;67:89–97.
46. Costa PT, McCrae RR. Revised NEO Personality Inventory and NEO Five Factor Inventory: Professional Manual. Odessa, FL: Psychological Assessment Resources, 1992.
47. Ware JE, Jr. SF-36 health survey update. Spine 2000;25:3130–9.
48. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry 1961;4:561–71.
49. Littner MR, Kushida C, Wise M, et al. Practice parameters for clinical use of the multiple sleep latency test and the maintenance of wakefulness test. Sleep 2005;28:113–21.
50. De Vito A, Carrasco Llatas M, Vanni A, et al. European position paper on drug-induced sedation endoscopy (DISE). Sleep Breath 2014;18:453–65.
51. Babar-Craig H, Rajani NK, Bailey P, Kotecha BT. Validation of sleep nasendoscopy for assessment of snoring with bispectral index monitoring. Eur Arch Otorhinolaryngol 2012;269:1277–9.
52. Vanderveken OM, Devolder A, Marklund M, et al. Comparison of a custom-made and a thermoplastic oral appliance for the treatment of mild sleep apnea. Am J Respir Crit Care Med 2008;178:197–202.
53. Schmidt-Nowara W, Lowe A, Wiegand L, Cartwright R, Perez-Guerra F, Menn S. Oral appliances for the treatment of snoring and obstructive sleep apnea: a review. Sleep 1995;18:501–10.
54. Eveloff SE, Rosenberg CL, Carlisle CC, Millman RP. Efficacy of a Herbst mandibular advancement device in obstructive sleep apnea. Am J Respir Crit Care Med 1994;149:905–9.
55. Remmers J, Charkhandeh S, Grosse J, et al. Remotely controlled mandibular protrusion during sleep predicts therapeutic success with oral appliances in patients with obstructive sleep apnea. Sleep 2013;36:1517–25.
56. Sanner BM, Heise M, Knoben B, et al. MRI of the pharynx and treatment efficacy of a mandibular advancement device in obstructive sleep apnoea syndrome. Eur Respir J 2002;20:143–50.
57. Tsuiki S, Ito E, Isono S, et al. Oropharyngeal crowding and obesity as predictors of oral appliance treatment response to moderate obstructive sleep apnea. Chest 2013;144:558–63.
58. Sher AE, Schechtman KB, Piccirillo JF. The efficacy of surgical modifications of the upper airway in adults with obstructive sleep apnea syndrome. Sleep 1996;19:156–77.
59. Verbraecken JA, De Backer WA. Upper airway mechanics. Respiration 2009;78:121–33.
60. Liu Y, Lowe AA, Fleetham JA, Park YC. Cephalometric and physiologic predictors of the efficacy of an adjustable oral appliance for treating obstructive sleep apnea. Am J Orthod Dentofacial Orthop 2001;120:639–47.
61. Mostafiz W, Dalci O, Sutherland K, et al. Influence of oral and craniofacial dimensions on mandibular advancement splint treatment outcome in patients with obstructive sleep apnea. Chest 2011;139:1331–9.
62. Liu Y, Park YC, Lowe AA, Fleetham JA. Supine cephalometric analyses of an adjustable oral appliance used in the treatment of obstructive sleep apnea. Sleep Breath 2000;4:59–66.
63. Ng AT, Darendeliler MA, Petocz P, Cistulli PA. Cephalometry and prediction of oral appliance treatment outcome. Sleep Breath 2012;16:47–58.
64. Marklund M, Stenlund H, Franklin KA. Mandibular advancement devices in 630 men and women with obstructive sleep apnea and snoring: tolerability and predictors of treatment success. Chest 2004;125:1270–8.
65. Mehta A, Qian J, Petocz P, Darendeliler MA, Cistulli PA. A randomized, controlled study of a mandibular advancement splint for obstructive sleep apnea. Am J Respir Crit Care Med 2001;163:1457–61.
66. Zeng B, Ng AT, Qian J, Petocz P, Darendeliler MA, Cistulli PA. Influence of nasal resistance on oral appliance treatment outcome in obstructive sleep apnea. Sleep 2008;31:543–7.
67. Marklund M, Persson M, Franklin KA. Treatment success with a mandibular advancement device is related to supine-dependent sleep apnea. Chest 1998;114:1630–5.
68. Yoshida K. Influence of sleep posture on response to oral appliance therapy for sleep apnea syndrome. Sleep 2001;24:538–44.
69. Yoshida K. Prosthetic therapy for sleep apnea syndrome. J Prosthet Dent 1994;72:296–302.
70. Lee CH, Kim JW, Lee HJ, et al. Determinants of treatment outcome after use of the mandibular advancement device in patients with obstructive sleep apnea. Arch Otolaryngol Head Neck Surg 2010;136:677–81.
71. Mayer G, Meier-Ewert K. Cephalometric predictors for orthopaedic mandibular advancement in obstructive sleep apnoea. Eur J Orthod 1995;17:35–43.
72. Liu Y, Zeng X, Fu M, Huang X, Lowe AA. Effects of a mandibular repositioner on obstructive sleep apnea. Am J Orthod Dentofacial Orthop 2000;118:248–56.
73. Chan AS, Lee RW, Srinivasan VK, Darendeliler MA, Grunstein RR, Cistulli PA. Nasopharyngoscopic evaluation of oral appliance therapy for obstructive sleep apnoea. Eur Respir J 2010;35:836–42.
74. Johal A, Hector MP, Battagel JM, Kotecha BT. Impact of sleep nasendoscopy on the outcome of mandibular advancement splint therapy in subjects with sleep-related breathing disorders. J Laryngol Otol 2007;121:668–75.
75. Vroegop AV, Vanderveken OM, Dieltjens M, et al. Sleep endoscopy with simulation bite for prediction of oral appliance treatment outcome. J Sleep Res 2013;22:348–55.
76. Ng AT, Qian J, Cistulli PA. Oropharyngeal collapse predicts treatment response with oral appliance therapy in obstructive sleep apnea. Sleep 2006;29:666–71.
77. Petit FX, Pepin JL, Bettega G, Sadek H, Raphael B, Levy P. Mandibular advancement devices: rate of contraindications in 100 consecutive obstructive sleep apnea patients. Am J Respir Crit Care Med 2002;166:274–8.
78. Alonso J, Angermeyer MC, Bernert S, et al. Prevalence of mental disorders in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr Scand Suppl 2004:21–7.
79. Verbruggen AE, Dieltjens M, Wouters, K et al. Prevalence of residual excessive sleepiness during effective oral appliance therapy for sleepdisordered breathing. Sleep Med 2014;15:269–72.
ACKNOWLEDGMENTS
The authors are grateful to the administrative and organizational support of Ms. Nadine De Kerpel. Furthermore, we thank the co-workers of the Sleep Laboratory of the Antwerp University Hospital for conducting the polysomnographic examinations.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication May, 2016
Submitted in final revised form September, 2016
Accepted for publication September, 2016
Address correspondence to: Annelies Verbruggen, Antwerp University Hospital (UZA), Wilrijkstraat 10, 2650 Edegem, Antwerp, Belgium; Tel: +32 3 821 52 21; Fax: +32 3 821 42 71; Email: annelies.verbruggen@uza.be
DISCLOSURE STATEMENT
This was not an industry supported study. This study was funded by a 3-year grant of the Flemish government agency for Innovation by Science and Technology (IWT-090864). Marc Braem and Olivier Vanderveken are promotors of the SomnoMed Research Grant at the University Hospital of Antwerp. Olivier Vanderveken is consultant for Inspire Medical Systems, Nyxoah and Philips Electronics. Paul Van de Heyning and Olivier Vanderveken received research support at the Antwerp University Hospital from Inspire Medical Systems. Olivier Vanderveken has got research support from ReVent and Nyxoah for clinical trials. He received research support in terms of free devices for an RCT with sleep position trainer in 20 patients from Nightbalance NV, Delft, the Netherlands; and he received lecture fees by Inspire Medical Systems, SomnoMed and Nightbalance. Johan Verbraecken received lecture fees from SomnoMed and AstraZeneca and is consultant for Jazz Pharmaceuticals. The other authors have indicated no financial conflicts of interest.
APPENDICES
|
Appendix 1 - Sleep questionnaire as routinely used in the sleep laboratory
|