Original Article 2, Issue 2.4
Class III Bimaxillary Orthognathic Surgery and Sleep Disordered Breathing Outcomes
http://dx.doi.org/10.15331/jdsm.5116
Jason M. Scherer, DDS, MS1 ; Rose D. Sheats, DMD, MPH2 ; Ceib Phillips, PhD, MPH3
1Private Practice, Canton, OH; 2Oral Facial Pain Group, Dental Sleep Medicine Unit, School of Dentistry, University of North Carolina, Chapel Hill, NC; 3Department of Orthodontics, School of Dentistry, University of North Carolina, Chapel Hill, NC
ABSTRACT
Study Objectives:
To assess whether patients with class III malocclusions who underwent bimaxillary orthognathic surgery (BOS) are at an increased risk for obstructive sleep apnea (OSA) and/or a reduction in sleep-related quality of life compared to class III patients treated with orthodontics alone.
Methods:
Questionnaires were mailed to class III patients who had BOS and a matched control group of class III patients previously treated with orthodontics alone. Subjects were asked to complete the Berlin Questionnaire to assess OSA risk and the Functional Outcomes of Sleep-10 (FOSQ-10) and Epworth Sleepiness Scale (ESS) to assess sleep-related quality of life.
Results:
Seventy-eight subjects in the BOS group responded (29.8% response rate) and 24 subjects in the control group responded (13.7% response rate). Compared to the control group, the surgery group was significantly older, had longer follow-up times, and had more Caucasians. There was no significant difference between the surgery and orthodontic-only groups in their responses to the Berlin Questionnaire or the FOSQ-10. According to the Berlin Questionnaire, 9.0% of the surgery group were at high risk for OSA, while 16.7% of the orthodontic-only group were at high risk. The median total FOSQ-10 score for the surgery group and the orthodontic-only group was 18.3 and 18.1, respectively. The surgery group had a significantly lower ESS score of 6.3 compared to the orthodontic-only group score of 6.9. These findings compared favorably with scores for healthy individuals.
Conclusions:
Patients receiving BOS for the correction of class III malocclusions are at no greater risk for OSA and/or reduction in sleep-related quality of life compared to Class III patients treated with orthodontics alone.
Keywords:
sleep disordered breathing, obstructive sleep apnea, quality of life, bimaxillary orthognathic surgery, 2 jaw surgery, Berlin Questionnaire, Functional Outcomes of Sleep Questionnaire-10, Epworth Sleepiness Scale
Citation:
Scherer JM, Sheats RD, Phillips C. Class III bimaxillary orthognathic surgery and sleep disordered breathing outcomes. Journal of Dental Sleep Medicine 2015;2(4):157–162.
Sleep disordered breathing (SDB) is regarded as a spectrum of diseases involving increased upper airway resistance during sleep and includes snoring, upper airway resistance syndrome, and obstructive sleep apnea (OSA).1 Individuals with SDB can progress in severity from snoring to OSA, with increased airway collapse over time. OSA is characterized by the recurrent narrowing and obstruction of the pharyngeal airway during sleep. OSA and other forms of SDB have been reported to increase the risk of morbidity and mortality through the association with diabetes, hypertension, cardiovascular disease, and cerebrovascular disease.2–4 With the prevalence of SDB among adults in the United States estimated at 26%,5 jaw surgeries that could alter the risk for SDB should be carefully evaluated.
Mandibular setback surgery, either alone or in conjunction with maxillary advancement, is a surgical treatment option for patients with skeletal class III malocclusions. This type of malocclusion is characterized by either mandibular prognathism, maxillary deficiency, or a combination of both. Several studies have suggested that patients may develop OSA after mandibular setback surgery due to a narrowing of the posterior airway space (PAS).6–8 In a recent systematic review of cephalometric and cone-beam computed tomography (CBCT) studies on setback surgery and airway, the authors concluded that there is moderate evidence that isolated mandibular setback surgery leads to a decrease in oropharyngeal airway volume after surgery.9 Follow-up studies of a year or greater have also shown a continued decrease in upper and middle airway dimension over time.10,11
Due to concerns about airway reduction and unfavorable facial profile esthetics, many surgeons in the United States are doing fewer isolated mandibular setbacks. Less than 10% of class III surgery patients are receiving isolated setbacks, while approximately 40% undergo bimaxillary orthognathic surgery (combination of mandibular setback and maxillary advancement); the other half receive maxillary advancement surgery alone.12 With the growing preference for bimaxillary orthognathic surgery (BOS), many recent studies have looked at its effect on the airway. In recent CBCT studies on changes in airway volume after BOS, the effect on the airway is still not clear. Some CBCT studies found an overall decrease in airway volume after BOS,13–15 but others found an increase,16 or even no change.17,18
Although studies have reported an association between reduced airway volume and the risk for sleep disordered breathing,19 threshold limits for airway size have not been established for the development of SDB. Even if BOS leads to a decrease in airway volume, the risk for developing SDB after surgery has not been sufficiently explored. Studies are limited, and conclusions vary, regarding the extent to which BOS leads to SDB confirmed by polysomnography (PSG).16,20,21 Moreover, no study was identified that assessed patients’ perception of sleep-related quality of life after BOS.
With the prevalence of sleep disordered breathing known to increase with age and evidence suggesting continual decreases in airway space after setback surgery, long-term follow up studies on BOS and SDB risk are needed.10,11,22 The purpose of this study was to assess whether patients with skeletal class III malocclusions who underwent bimaxillary orthognathic surgery are at an increased risk for OSA and/or a reduction in perceived sleep-related quality of life compared to a group of non-surgical class III patients treated with orthodontics alone.
METHODS
This study was approved by the Biomedical Institutional Review Board of the University of North Carolina.
Subjects
Bimaxillary Surgery
Two hundred sixty-two subjects with class III malocclusions who had undergone bimaxillary orthognathic surgery at the University of North Carolina (UNC) Memorial Hospital between 2003 and 2012 were identified from the UNC orthognathic surgery database after accounting for inclusion and exclusion criteria. Subjects were included if they were at least 1 year post-surgery, had current contact information, and were able to understand and read English. The presence of a congenital syndrome led to exclusion from the study.
Orthodontic-Only Control
One hundred seventy-five patients with class III malocclusions who were treated nonsurgically in the UNC graduate orthodontic clinic and who met the same inclusion and exclusion criteria as the surgery group were frequency matched to the surgery group based on gender, age, and time since deband.Each subject was mailed a packet which included a cover letter for informed consent, a HIPAA authorization, an opt-out form, a set of questionnaires, and a business reply envelope. Demographic data, information on OSA diagnosis or management since their class III treatment, and responses to items on three questionnaires to assess OSA risk and quality of life were requested. The questionnaires were created in Teleform so that returned questionnaires could be easily scanned, verified, and input into a SAS dataset for analysis. Non-responders were mailed a second and, if necessary, a third packet at monthly intervals.
Questionnaires
Subjects were asked to report age in years and months, gender (male/female), height in feet and inches, weight in pounds, race/ethnicity, and information on previous OSA diagnosis or treatment. Three sleep questionnaires (Berlin, Functional Outcomes of Sleep-10, and Epworth Sleepiness Scale) were completed by participants in this study to assess OSA risk and sleep- related quality of life. Although the diagnostic gold standard for assessing OSA is overnight polysomnography (PSG), validated disease-specific questionnaires are frequently used as convenient and cost-effective screening tools for OSA.23The Berlin Questionnaire is a validated survey that scores subjects as “high risk” or “low risk” for OSA.24 In a recent systematic review of validated OSA screening questionnaires, the Berlin had a pooled sensitivity and specificity of, 77% and 74%, respectively.25 The Berlin Questionnaire is composed of 10 questions divided among 3 symptom categories: snoring, daytime sleepiness, and obesity/hypertension. Patients with frequent and persistent symptoms in any 2 of the 3 categories are considered at high risk for OSA. At least 2 affirmative answers in either the snoring or daytime sleepiness categories is confirmation of the presence of that symptom. For the obesity/hypertension category, an answer of “yes” to having hypertension or a body mass index (BMI) > 30 kg/m2 is considered a positive score. BMI was calculated from the self-reported height and weight.
The Functional Outcomes of Sleep Questionnaire (FOSQ-30) is a valid and reliable 30-item questionnaire that is considered to be the gold standard in assessing the impact of sleepiness on quality of life.26 The FOSQ-10 is a shorter version of the original FOSQ-30 and has been shown to be easier to use and to reach the same statistical conclusions as the longer version regarding comparisons in sleep-related quality of life between normal controls and patients with OSA.27 The FOSQ-10 assesses quality of life via 10 questions measuring 5 subscales: general productivity, activity level, vigilance, social outcome, and intimacy and sexual relationships.26 Total scores range from 5–20 with lower values suggesting poorer sleeprelated quality of life.
The Epworth Sleepiness Scale (ESS) assesses daytime sleepiness and is one of the most widely used sleep assessment questionnaires in clinical settings. Although the ESS has been found to have a low predictive value when used as a screening method for OSA,28–30 a study using participants from the Sleep Heart Heath Study found excessive daytime sleepiness to be strongly associated with reduced quality of life.31 The subject rates from 0–3 (0-never, 3-high) his/her chances of dozing off in 8 situations that are often encountered in daily life. ESS scores range from 0–24, and a score > 10 (i.e., 11+) is considered indicative of excessive daytime sleepiness.32
Statistical Analysis
All statistical analyses were conducted using SAS (SAS Institute Inc. Version 9.3 2011. Cary, NC: SAS Institute Inc.).The orthognathic surgery and orthodontic-only groups were compared to assess characteristic differences (age, sex, time since surgery/deband, race, BMI, diagnosis of OSA, prescription for OSA treatment) and to assess whether the groups differed with respect to perception of quality of life and risk for OSA. Descriptive and inferential statistics were used to analyze the data. A χ2 or Fisher exact test was used to compare categorical variables, and a Cochran-Mantel-Haenszel row mean score test was used to compare continuous variables between groups. The level of significance was set at 0.05.
RESULTS
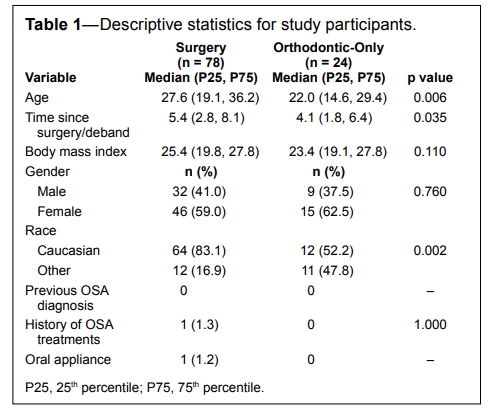
Of the 262 surgery subjects sent questionnaires, 78 patients responded (response rate of 29.8%). Surgery participants included 46 females and 32 males with a median age of 27.6 (19.1, 36.2). They were all at least 2 years post-surgery with a median time since surgery of 5.4 (2.8, 8.1) years. Twenty-four of the 175 subjects in the control group responded (response rate of 13.7%). The control group consisted of 15 females and 9 males with a median age of 22.0 (14.6, 29.4) years. They were all at least 1 year post deband with a median time since deband of 4.1 (1.8, 6.4) years. The 2 groups were significantly different in median age (p < 0.01), time since surgery/deband (p < 0.05), and race (p < 0.01). Compared to the control group, the surgery group was older, had a longer follow-up time, and was composed of a higher percentage of Caucasians. No statistical difference between gender and BMI was detected (Table 1). One participant in the surgery group acknowledged being treated with an oral appliance, but denied having a previous OSA diagnosis. Either the patient failed to recall a diagnosis or was provided the oral appliance in absence of an official diagnosis. The patient also stated that it had been 2 years since the appliance was used.
Table 1Descriptive statistics for study participants. |
{kind=link}
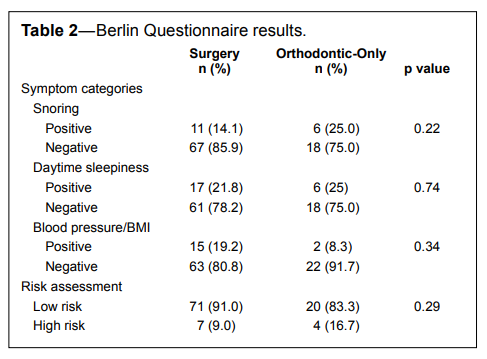
The Berlin Questionnaire did not reveal any statistically significant difference in the OSA risk assessment between the surgery and orthodontic-only groups nor were there any statistically significant differences between groups in any of the symptom categories (Table 2). Overall, 9.0% of the surgery group and 16.7% of the orthodontic-only group were found to be at high risk for OSA.
Table 2Berlin Questionnaire results. |
{kind=link}
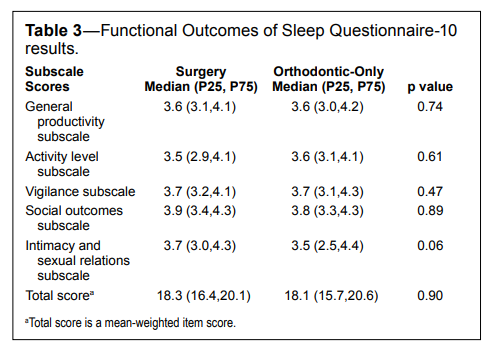
Analysis of the FOSQ-10 indicated no statistically significant difference between the total FOSQ-10 score for the surgery and orthodontic-only groups with median total scores of 18.3 (16.4, 20.1) and 18.1 (15.7, 20.6), respectively. The two groups did not differ significantly in any of the subscales: productivity, activity, vigilance, social outcomes, or intimacy and sexual relations (Table 3).
Table 3Functional Outcomes of Sleep Questionnaire-10 results. |
{kind=link}
The difference in the Epworth Sleepiness Scale scores was significantly different between the surgery and orthodontic-only groups (p < 0.05). After excluding those with missing data, the median ESS score for the surgery group was 6.3 (3.3, 9.3) compared to 6.9 (2.4, 11.4) for the orthodontic-only group. Both median scores, however, fell within the normal range for daytime sleepiness. When assessed for the proportion of subjects who demonstrated excessive daytime sleepiness, 10.5% of the surgery group and 20.8% of the orthodontic-only group had an ESS total score > 10 (p = 0.29; Table 4)
Table 4Epworth Sleepiness Scale (ESS) results. |
{kind=link}
DISCUSSION
Sleep disordered breathing, including OSA, is a serious condition associated with increased morbidity and mortality.3,4 Isolated mandibular setbacks are becoming rare in the United States due to both esthetic reasons and concerns over the risk of airway reduction possibly leading to SDB. Studies on the effects of bimaxillary orthognathic surgery with mandibular setback (BOS) on sleep function are limited. Objective measures, primarily from polysomnograms, have traditionally been reported in the literature and have led to varying conclusions. In the PSG study of Foltán et al,20 BOS was found to worsen respiratory parameters with significant decreases in oxygen saturation (SpO2 ) and nasal airflow measured before and after (mean 8.5 months) surgery. However, in a different PSG study, Hasebe et al.21 was unable to detect significant differences in SDB or changes in SpO2 or apnea-hypopnea index (AHI) in patients 6 months after BOS. The investigators did note that 2 patients with very large mandibular setbacks were diagnosed with mild OSA after surgery. Turnbull and Battagel33 compared overnight pulse oximetry and respiratory noises before and after BOS and found no significant changes despite identifying a reduction in the retrolingual airway diameter in all patients. In a recent PSG study by Gokce et al.,16 sleep quality and efficiency improved significantly after BOS (mean 1.4 years) with significant increases in SpO2 and decreases in AHI.
While objective measures of SDB have traditionally been reported in the literature, quality of life assessments are increasingly being recognized as an important outcome variable as well.31,35 A number of studies have examined quality of life subsequent to jaw surgery for dentofacial deformities,36 however, no studies were identified that explored the impact of Class III jaw surgeries on sleep-related quality of life. Our finding of no significant difference in Berlin Questionnaire scores between the BOS group and the orthodontic-only group is consistent with the objective measure studies that were unable to demonstrate an increased risk of SDB after BOS. The BOS group scores were also found to be similar to a recent population study on OSA risk. For example, the Berlin Questionnaire was used in a national sleep poll of 1,506 people, and 19% of participating adults were found to meet the criteria for high risk of OSA.34 In our study, 9.0% of the surgery group and 16.7% of the orthodontic-only group were found to be at high risk for OSA.
In our study, we used 2 validated sleep questionnaires, the FOSQ-10 and ESS, to focus on how BOS may affect patients’ perception of sleep-related quality of life. To our knowledge, this is the first study to assess patients’ perception of daytime sleepiness after BOS. With a median post-surgery time of 5.4 (2.8, 8.1) years, our study offered information on subjects with a longer follow-up than any previous study that measured sleep outcomes after BOS.
In a recent study evaluating ESS scores between OSA patients and non-OSA patients, the average values found were 10.9 and 7.7, respectively.30 Although we found a statistically significant difference in ESS scores between our 2 groups (p < 0.05), with the surgery group having a lower median daytime sleepiness score, ESS scores in both groups fell within the normal range. Both groups in our study were less than the reported non-OSA score of 7.7, with the surgery group having a median ESS score of 6.3 (3.3, 9.3) and the orthodontic-only group a score of 6.9 (2.4, 11.4). It has been estimated that 10% to 20% of the general population has ESS scores > 10.37 Our results were in that range with 10.5% of the BOS group and 20.8% of the orthodonticonly group having ESS scores > 10. The significantly lower ESS score and lower proportion of scores > 10 in the surgery group suggest that BOS does not adversely impact daytime sleepiness.
The FOSQ was developed to measure the impact of sleep on quality of life. Higher FOSQ scores reflect better quality of life. In a previous FOSQ-10 study, patients with OSA had an average score of 12.5, while non-OSA participants had an average score of 17.2.27 In our BOS group, the FOSQ-10 score of 18.3 (16.4, 20.1) compared favorably to the reported value in the non-OSA patients. Thus, results from both the ESS and FOSQ-10 in our study suggest that Class III bimaxillary surgery did not significantly affect the patients’ sleep-related quality of life post-surgery.
Study Limitations
The median age of both of our study groups was relatively young. Due to the conversion in 2003 from paper charts to the electronic patient record (EPR) at our institution, we were limited in the time frame for which we had current contact information for patients in the UNC surgery database. As such, the median age of both groups was < 28 years and may not reflect OSA outcome differences that may occur with increasing age.38 A well-known risk assessment questionnaire, the STOP-Bang, uses age 50 as a threshold for increased OSA risk.39 If or how our groups differ after age 50 would be valuable information on clarifying whether BOS is associated with an increased risk of OSA over time. Although we attempted to frequency match the age of the orthodontic-only group to the age of the surgery group respondents, the median age of the surgery group was approximately 5 years older, which one might have speculated would have magnified a difference in OSA risk if it existed.
The increased follow-up time of approximately 1 year for the BOS group compared to the orthodontic-only group is understandable because up to a year of orthodontic finishing remains after surgery. We were not able to compare deband dates between groups because we did not have access to the deband dates of the surgery group. The majority of the orthognathic surgery patients seen at UNC have their orthodontic treatment carried out by local orthodontists.
The BMI used in this study was calculated from self-reported height and weight values. Although the BMI was not significantly different between groups, any inaccuracies in BMI could also have altered the scoring of the Berlin Questionnaire which uses BMI as one of its variables. Given that the study design did not evaluate patients clinically, obtaining accurate height and weight data from participants was not possible. The significantly more Caucasians in the surgery group is consistent with the demographics of the surgery patients at UNC.
There was a significant difference in response rate between the BOS group and orthodontic-only group with response rates of 29.8% and 13.7%, respectively. The BOS subjects may have been more likely to participate in our study because many had previously agreed to participate in an ongoing surgery stability study at UNC. In addition, the BOS subjects may have felt more of an obligation to participate because of the intense emotional and psychological impact that comes from the profound positive changes in function and facial esthetics after surgery. The low response rate in both groups is likely related to the transient nature of individuals who have treatment in their teens and early twenties and then relocate for college and jobs. No institutional effort is made to periodically update the contact information of patients who have completed treatment, which possibly negatively impacts retrospective study response rates, thereby limiting the generalizability of the findings.
To our knowledge, this study provides the longest followup information to date on the effects of Class III bimaxillary orthognathic surgery (BOS) on sleep disordered breathing (SDB). Moreover, this is the first study to assess sleep-related quality of life after BOS. The results of this study suggest that young adults receiving this double jaw surgical procedure for the correction of class III malocclusions are at no greater risk for OSA and/or reduction in sleep- related quality of life than patients treated with orthodontics alone. Patients have been shown to be at most risk for SDB if the mandible is set back significantly, preventing adaption to their new respiratory position during sleep.21 Bimaxillary orthognathic surgery for Class III malocclusions may be able to limit the risk of SDB by minimizing the amount of mandibular setback required and through compensating increases in the nasopharyngeal and velopharyngeal airways from the maxillary advancement.16,40 Prospective research is needed to evaluate sleep-related quality of life before and after BOS and to examine correlations between PSG data, sleep questionnaires, and 3D airway parameters. The ability to more clearly identify an orthognathic surgery patient’s presurgical risk of developing SDB is a goal that would guide surgeons and benefit patients in the future.
REFERENCES
2. Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med 2000;342:1378–84.
3. Shahar E, Whitney CW, Redline S, et al. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the sleep heart health study. Am J Respir Crit Care Med 2001;163:19–25.
4. Young T, Finn L, Peppard PE, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep 2008;31:1071–8.
5. Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol 2013;177:1006–14.
6. Riley RW, Powell NB, Guilleminault C, Ware W. Obstructive sleep apnea syndrome following surgery for mandibular prognathism. J Oral Maxillofac Surg 1987;45:450–2.
7. Liukkonen M, Vahatalo K, Peltomaki T, Tiekso J, Happonen RP. Effect of mandibular setback surgery on the posterior airway size. Int J Adult Orthodon Orthognath Surg 2002;17:41–6.
8. Demetriades N, Chang DJ, Laskarides C, Papageorge M. Effects of mandibular retropositioning, with or without maxillary advancement, on the oro-naso-pharyngeal airway and development of sleep-related breathing disorders. J Oral Maxillofac Surg 2010;68:2431–6.
9. Mattos CT, Vilani GNL, Sant’Anna EF, Ruellas ACO, Maia LC. Effects of orthognathic surgery on oropharyngeal airway: a meta-analysis. Int J Oral Maxillofac Surg 2011;40:1347–56.
10. Kawakami M, Yamamoto K, Fujimoto M, Ohgi K, Inoue M, Kirita T. Changes in tongue and hyoid positions, and posterior airway space following mandibular setback surgery. J CranioMaxillofac Surg 2005;33:107–10.
11. Eggensperger N, Smolka W, Iizuka T. Long-term changes of hyoid bone position and pharyngeal airway size following mandibular setback by sagittal split ramus osteotomy. J CranioMaxillofac Surg 2005;33:111–7.
12. Busby BR, Bailey LJ, Proffit WR, Phillips C, White RP Jr. Long-term stability of surgical class III treatment: a study of 5-year postsurgical results. Int J Adult Orthodon Orthognath Surg 2002;17:159–70.
13. Kim MA, Kim BR, Choi JY, Youn JK, Kim YJ, Park YH. Three-dimensional changes of the hyoid bone and airway volumes related to its relationship with horizontal anatomic planes after bimaxillary surgery in skeletal class III patients. Angle Orthod 2013;83:623–9.
14. Park SB, Kim YI, Son WS, Hwang DS, Cho BH. Cone-beam computed tomography evaluation of short- and long-term airway change and stability after orthognathic surgery in patients with class III skeletal deformities: bimaxillary surgery and mandibular setback surgery. Int J Oral Maxillofac Surg 2012;41:87–93.
15. Degerliyurt K, Ueki K, Hashiba Y, Marukawa K, Nakagawa K, Yamamoto E. A comparative CT evaluation of pharyngeal airway changes in class III patients receiving bimaxillary surgery or mandibular setback surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:495–502.
16. Gokce SM, Gorgulu S, Gokce HS, Bengi AO, Karacayli U, Ors F. Evaluation of pharyngeal airway space changes after bimaxillary orthognathic surgery with a 3-dimensional simulation and modeling program. Am J Orthod Dentofacial Orthop 2014;146:477–92.
17. Lee Y, Chun YS, Kang N, Kim M. Volumetric changes in the upper airway after bimaxillary surgery for skeletal class III malocclusions: a case series study using 3-dimensional cone-beam computed tomography. J Oral Maxillofac Surg 2012;70:2867–75.
18. Jakobsone G, Neimane L, Krumina G. Two- and three-dimensional evaluation of the upper airway after bimaxillary correction of class III malocclusion. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110:234–42.
19. Enciso R, Nguyen M, Shigeta Y, Ogawa T, Clark GT. Comparison of cone-beam CT parameters and sleep questionnaires in sleep apnea patients and control subjects. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109:285–93.
20. Foltan R, Hoffmannova J, Donev F, et al. The impact of Le Fort I advancement and bilateral sagittal split osteotomy setback on ventilation during sleep. Int J Oral Maxillofac Surg 2009;38:1036–40.
21. Hasebe D, Kobayashi T, Hasegawa M, et al. Changes in oropharyngeal airway and respiratory function during sleep after orthognathic surgery in patients with mandibular prognathism. Int J Oral Maxillofac Surg 2011;40:584–92.
22. Bixler EO, Vgontzas AN, Ten Have T, Tyson K, Kales A. Effects of age on sleep apnea in men: I. prevalence and severity. Am J Respir Crit Care Med 1998;157:144–8.
23. Pang KP, Terris DJ. Screening for obstructive sleep apnea: an evidencebased analysis. Am J Otolaryngol 2006;27:112–8.
24. Netzer NC, Stoohs RA, Netzer CM, Clark K, Strohl KP. Using the Berlin Questionnaire to identify patients at risk for the sleep apnea syndrome. Ann Intern Med 1999;131:485–91.
25. Abrishami A, Khajehdehi A, Chung F. A systematic review of screening questionnaires for obstructive sleep apnea. Can J Anaesth 2010;57:423–38.
26. Weaver TE, Laizner AM, Evans LK, et al. An instrument to measure functional status outcomes for disorders of excessive sleepiness. Sleep 1997;20:835–43.
27. Chasens ER, Ratcliffe SJ, Weaver TE. Development of the FOSQ-10: a short version of the Functional Outcomes of Sleep Questionnaire. Sleep 2009;32:915–9.
28. Chervin RD, Aldrich MS. The Epworth Sleepiness Scale may not reflect objective measures of sleepiness or sleep apnea. Neurology 1999;52:125–31.
29. Rosenthal LD, Dolan DC. The Epworth Sleepiness Scale in the identification of obstructive sleep apnea. J Nerv Ment Dis 2008;196:429–31.
30. Sil A, Barr G. Assessment of predictive ability of Epworth scoring in screening of patients with sleep apnoea. J Laryngol Otol 2012;126:372–9.
31. Baldwin CM, Griffith KA, Nieto FJ, O’Connor GT, Walsleben JA, Redline S. The association of sleep-disordered breathing and sleep symptoms with quality of life in the Sleep Heart Health Study. Sleep 2001;24:96–105.
32. Johns MW. A new method for measuring daytime sleepiness: the Epworth Sleepiness Scale. Sleep 1991;14:540–5.
33. Turnbull NR, Battagel JM. The effects of orthognathic surgery on pharyngeal airway dimensions and quality of sleep. J Orthod 2000;27:235–47.
34. Hiestand DM, Britz P, Goldman M, Phillips B. Prevalence of symptoms and risk of sleep apnea in the US population: results from the National Sleep Foundation Sleep in America 2005 Poll. Chest 2006;130:780–6.
35. Kushida CA, Littner MR, Hirshkowitz M, et al. Practice parameters for the use of continuous and bilevel positive airway pressure devices to treat adult patients with sleep-related breathing disorders. Sleep 2006;29:375–80.
36. Soh CL, Narayanan V. Quality of life assessment in patients with dentofacial deformity undergoing orthognathic surgery--a systematic review. Int J Oral Maxillofac Surg 2013;42:974–80.
37. Johns M, Hocking B. Daytime sleepiness and sleep habits of Australian workers. Sleep 1997;20:844–9.
38. Young T, Skatrud J, Peppard PE. Risk factors for obstructive sleep apnea in adults. JAMA 2004;291:2013–6.
39. Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology 2008;108:812–21.
40. Kobayashi T, Funayama A, Hasebe D, Kato Y, Yoshizawa M, Saito C. Changes in overnight arterial oxygen saturation after mandibular setback. Br J Oral Maxillofac Surg 2013;51:312–8.
ACKNOWLEDGMENTS
The authors are grateful for the generous support from the Dental Foundation of North Carolina for the MS Research Grant. We would like to thank Debbie Price, David Best, Kim Lorello, and Adane Wogu for their contributions to this study. Also, many thanks to all the participants that made this study possible.SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication April, 2015
Submitted in final revised form June, 2015
Accepted for publication July, 2015
Address correspondence to: Ceib Phillips, University of North Carolina, School of Dentistry, 3120 Old Dental, Chapel Hill, NC 27599; Email: Ceib_Phillips@unc.edu
DISCLOSURE STATEMENT
This was not an industry supported study. This research was supported by the MS Research Grant from the Dental Foundation of North Carolina. The authors have indicated no financial conflicts of interest