Original Article 2, Issue 13.1
Domain Classification and Content Validation of FAirEST-15 for Pediatric Sleep-Disordered Breathing: A Tool Structuring Study for Dental Screening
http://dx.doi.org/10.15331/jdsm.7418
Lekshmy SR Nair, MDS in Pediatric and Preventive Dentistry 1; Sageena George, MDS in Pediatric and Preventive Dentistry1; Anandaraj Soman, MDS in Pediatric and Preventive Dentistry1; Deepak Jose, MDS in Pediatric and Preventive Dentistry1
1Department of Pediatric and Preventive Dentistry, PMS College of Dental Science and Research, Trivandrum, Kerala, India
ABSTRACT
Background:
Sleep-Disordered Breathing (SDB) in children affects craniofacial growth, behavior, and general health but remains underdiagnosed. The FAirEST-15 (Functional Airway Evaluation Screening Tool) includes 15 observable features to help clinicians identify SDB risk. However, the tool lacks a domain-wise structure and risk stratification system, limiting its broader application. Aim: To develop a domain-level classification system for the FAirEST-15 tool through expert consensus and evaluate its content validity and inter-rater agreement.
Methods:
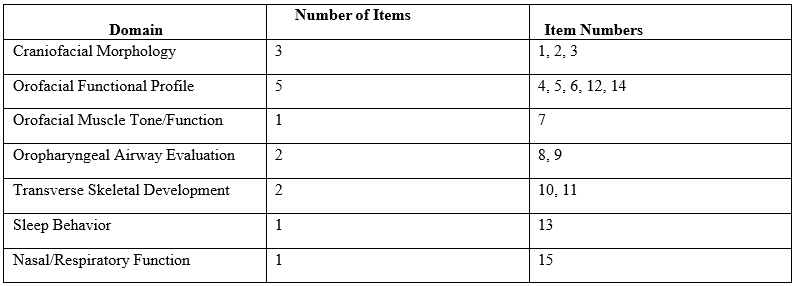
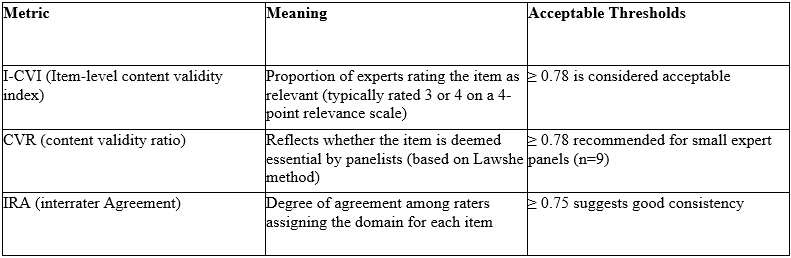
A cross-sectional methodological study was conducted involving nine subject-matter experts—three each from pediatric dentistry, orthodontics, and pediatric ENT. Experts independently reviewed and assigned each FAirEST-15 item to a relevant domain. A modified Delphi method was used to reach consensus, resulting in a seven-domain classification: Craniofacial Morphology, Orofacial Functional Profile, Orofacial Muscle Tone/Function, Oropharyngeal Airway Evaluation, Transverse Skeletal Development, Sleep Behavior, and Nasal/Respiratory Function. Validity was assessed using Item level Content Validity Index (I-CVI), Content Validity Ratio (CVR), and Inter-Rater Agreement (IRA).
Results:
Nine of the 15 items achieved perfect I-CVI (1.00), CVR (1.00), and IRA (≥0.89). Most other items showed acceptable agreement (I-CVI and CVR ≥0.78; IRA ≥0.75). Only one item—Maxillary Intercanine Distance—showed lower indices, suggesting the need for future re-evaluation.
Conclusion:
This study presents a validated domain-wise classification for FAirEST-15, enhancing its clinical interpretability and supporting its integration into structured pediatric SDB screening. The findings enable more targeted assessment and facilitate interdisciplinary collaboration in early identification and management.
Citation:
Nair LS, George S, Anandaraj S, Jose D. Domain Classification and Content Validation of FAirEST-15 for Pediatric Sleep-Disordered Breathing: A Tool Structuring Study for Dental Screening. J Dent Sleep Med. 2026;13(1)
INTRODUCTION
Sleep-disordered breathing (SDB) in children is a prevalent yet underdiagnosed condition, with potential effects on craniofacial growth, behavior, learning, and systemic health.1-3 It encompasses a spectrum ranging from primary snoring to obstructive sleep apnea (OSA).4 Early identification and intervention are essential, particularly in pediatric populations where symptoms may be subtle and misattributed.5
Dental professionals and ear, nose, and throat (ENT) specialists are increasingly recognized as frontline screeners for pediatric SDB because of their routine contact with children and the visibility of associated clinical features during examinations.6-8 In this context, tools such as the FAirEST-15 (Functional Airway Evaluation Screening Tool) have been developed to guide structured clinical assessment. This tool consists of 15 observable features spanning ENT, dental, myofunctional, and skeletal domains that may signal a risk of SDB.9
Despite its comprehensiveness, the FAirEST-15 currently lacks an organized domain-level classification of its 15 items. Unlike its condensed counterpart, FAirEST-6, which selects six key indicators and provides risk categorization based on a simple count of positive signs, the FAirEST- 15 does not group features into validated domains, limiting its interpretability and potential for advanced data analysis.9 Furthermore, no standard risk stratification model exists for the FAirEST-15, creating a barrier for its broader application in clinical research and community screening.
Domain-level classification offers several advantages: it enables thematic grouping of symptoms, enhances clinical utility, and supports integration with other validated tools. Grouping clinical features into logically and clinically coherent domains also facilitates future development of simplified versions, composite scoring systems, and targeted interventions.10-11 However, such classification must be grounded in expert consensus and validated for content relevance and inter- rater agreement.12
This study was undertaken to create a domain-level classification system for the FAirEST-15 items through expert consensus from three specialties—pediatric dentistry, orthodontics, and pediatric ENT—and to evaluate the content validity of these domain assignments using standard indices such as the content validity index (CVI), content validity ratio (CVR), and interrater agreement (IRA).
The results of this study will enhance the interpretability of the FAirEST-15, facilitate its integration with other pediatric sleep screening tools, and provide a foundation for developing a domainwise scoring and risk classification system. Ultimately, this work aims to support more structured, evidence-based community screening and interdisciplinary collaboration in managing pediatric sleep-disordered breathing.
METHODS
Study Settings and Design
This study was a cross-sectional methodological research project conducted in a multidisciplinary academic environment, involving experts from the departments of Pediatric Dentistry, Orthodontics, and Pediatric Otorhinolaryngology. The primary objective was to establish an expert-derived domain classification for the FAirEST-15 clinical screening tool and assess the content validity and interrater reliability of the domain assignments. The study spanned 3 months and followed a structured, phased approach incorporating expert consensus and statistical validation techniques.Participants
A total of nine subject matter experts were purposively selected to participate in the study. These individuals were selected in line with published guidance that panels of 6 to 10 experts are sufficient to facilitate both diversity of judgment and methodological rigor in tool validation.13-14 Panel size 9 was also a realistic compromise, providing enough breadth of qualification while being reasonable considering the numbers of qualified specialists in pediatric dentistry and associated disciplines who were willing and available to serve.The nine experts were chosen based on prespecified inclusion criteria to provide clinical and academic relevance. Experts needed a minimum of 5 years of professional experience and documented expertise in pediatric SDB or closely related fields such as pediatric dentistry, orthodontics, otorhinolaryngology, and pediatric medicine. Further criteria for selection were active participation in clinical management of children with suspected or confirmed SDB and experience with screening and assessment frameworks such as FAirEST-15. The last panel was a well-balanced group consisting of experts with academic, clinical, and research background to provide a holistic assessment of the tool.
Study Phases
The study proceeded in three key phases. In Phase 1, the 15 items of the FAirEST-15 tool were independently reviewed by the experts. Each item was accompanied by a brief clinical description to ensure consistent understanding. Experts were asked to classify each item under a suitable domain based on anatomical and functional relevance. In Phase 2, a modified Delphi method was used to achieve consensus. Feedback from the first round was anonymized and redistributed to the experts for a second round of review. Through this iterative process, a seven-domain classification emerged: Craniofacial Morphology, Orofacial Functional Profile, Orofacial Muscle Tone/Function, Oropharyngeal Airway Evaluation, Transverse Skeletal Development, Sleep Behavior, and Nasal/Respiratory Function. In Phase 3, the domain assignments were statistically validated. Item-level content validity index (I-CVI) was calculated to assess the proportion of agreement among experts rating each item as either "relevant" or "highly relevant" to the assigned domain. A threshold of ≥0.78 for I-CVI was considered acceptable, corresponding to agreement by at least 7 out of the 9 experts on the panel. The CVR was then computed using the Lawshes method, based on experts' judgments about the essentiality of each item. A CVR of 0.78 or higher was deemed acceptable given the panel size.IRA was determined using Fleiss kappa, with values ≥0.75 interpreted as substantial agreement and values ≥0.80 as excellent.
Data Collection and Ethical Approval
Data collection was facilitated through secure online forms, with each expert providing individual responses in two rounds. This study was conducted as part of the secondary objective of a PhD research proposal aimed at developing and validating a comprehensive screening tool for pediatric sleep disturbances and approved by the Institutional Ethics Committee of the study center (IEC Number:PMS/IEC/2024/Add/dhr/June/45/Rev-1).
RESULTS
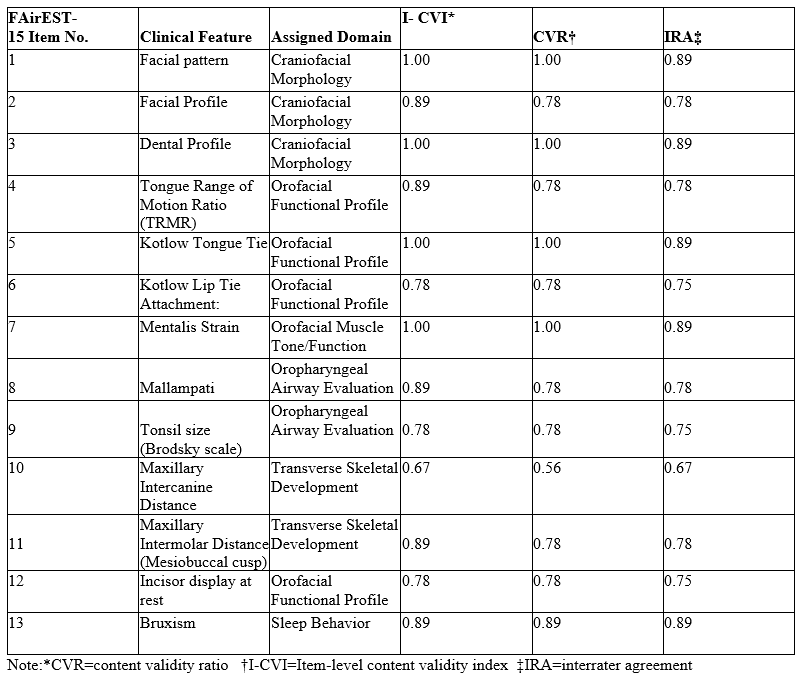
Nine of the 15 features received an I-CVI of 1.00, indicating complete agreement among experts regarding their relevance to the assigned domains. These items included Facial Pattern, Dental Profile, Kotlow Tongue Tie, Mentalis Strain, Swallowing Tongue Thrust Compensation Test, and Bruxism. These features also achieved perfect CVR scores (1.00) and high IRA values (≥0.89), underscoring their consensus on both essentiality and interrater consistency.
Several other items (for example, facial profile, tongue range of motion ratio, Mallampati, maxillary intermolar distance) demonstrated acceptable validity and agreement, with I-CVI and CVR values ranging from 0.78 to 0.89 and IRA values above 0.75. This indicates that although complete consensus was not reached, there was sufficient expert agreement to support inclusion.
Notably, maxillary intercanine distance (Item 10) showed relatively lower indices (I-CVI = 0.67, CVR = 0.56, IRA = 0.67). This suggests moderate disagreement among experts, warranting further clarification or reevaluation of this item in future studies.
| Table 1: Domain Summary of FAirEST-15 Clinical Features (more ...) |
{kind=link}
Table 2: Interpretation of I-CVI, CVR, and IRA for Each ItemTable 3: Domain Classification and Content Validation Metrics for FAirEST-15
{kind=link}
(more ...)
{kind=link}
DISCUSSION
Domain Classification in FAirEST-15
Craniofacial Morphology:
This domain includes features such as facial pattern, facial profile, and dental profile. Multiple studies have demonstrated that abnormal craniofacial growth patterns—such as a retrognathic mandible, long face syndrome, or a convex profile—are significantly associated with an increased risk for pediatric sleep-disordered breathing (SDB). For instance, Villa et al observed that children with skeletal discrepancies, particularly in vertical growth dimensions, were more likely to exhibit symptoms of OSA.15 These features provide a structural basis for compromised airway patency during sleep, making this domain clinically relevant in screening for SDB.
Orofacial Functional Profile:
This domain encompasses tongue mobility, tongue tie, lip tie, tongue thrust swallowing, and incisor display at rest. Studies by Zaghi et al highlight how restrictions in lingual and labial frenula affect oral rest posture and contribute to dysfunctional orofacial myofunctional patterns.16 Such patterns, including tongue thrust and low tongue posture, are implicated in upper airway collapse and reduced airway tone during sleep. The inclusion of incisor display is justified as it indirectly reflects lip incompetence and orofacial muscle imbalance, supporting its grouping within this domain.
Oropharyngeal Airway Evaluation:
Items such as the Mallampati score and tonsil size (via Brodsky scale) are widely used indicators of oropharyngeal crowding and obstruction. High Mallampati scores and hypertrophic tonsils correlate with an elevated risk of OSA in children, as established by Mitchell et al.17 These indicators directly visualize airway patency and are often part of preoperative evaluation for adenotonsillectomy in pediatric OSA management.
Orofacial Muscle Tone/Function:
Mentalis strain is a marker of compensatory perioral muscle activity in response to mouth breathing or tongue dysfunction. According to recent studies, the presence of such strain during lip closure is a reliable indicator of altered muscle tone, often associated with compromised oral function and breathing patterns.18 Its inclusion as a separate domain emphasizes the neuromuscular component of airway stability.
Transverse Skeletal Development:
This domain covers maxillary intercanine and intermolar distances. A constricted maxilla has been strongly associated with SDB due to decreased nasal cavity volume and increased nasal resistance Palatal expansion has shown improvements in nocturnal breathing in children, supporting the relevance of transverse skeletal metrics in screening and diagnosis of pediatric OSA.
Sleep Behavior:
Bruxism was placed under this domain because of its recognized link with microarousals and sympathetic nervous system activation during sleep. Studies have explored bruxism as both a symptom and a potential consequence of disturbed sleep architecture.19 It provides behavioral insight into sleep quality, justifying its distinct domain placement.
Nasal/Respiratory Function:
The nasal breathing test assesses nasal airflow and potential obstruction, which are foundational to upper airway patency. Chronic mouth breathing—often a compensatory mechanism for nasal blockage—is a well-documented risk factor for SDB.20 This item aligns with the domain of respiratory function, reinforcing the importance of nasal airflow evaluation in screening tools such as FAirEST.
Content Validation
In the current study, the domain classification of the FAirEST-15 clinical screening tool was systematically derived through a structured content validation process, incorporating expert consensus from three pediatric dentists, three orthodontists, and three pediatric ENT specialists. This method aligns with established frameworks for content validation where the relevance and clarity of each item in relation to the proposed domains were assessed using metrics such as the I-CVI, CVR, and IRA.
The use of a multidisciplinary panel enriched the process by ensuring that the clinical perspectives across specialties were represented, thereby increasing the robustness and applicability of the domain classification. This approach is consistent with prior validation efforts in tools such as the Sleep Disturbance Scale for Children, Pediatric Sleep Questionnaire, and Pediatric Sleep Clinical Global Impressions Scale, which have relied on expert panels to refine and validate questionnaire items or clinical features.21-23
The strength of the current validation process lies in its quantitative rigor (using I-CVI, CVR, and IRA), combined with qualitative consensus, which enhances the content credibility of the proposed domains. The high agreement scores observed (most I-CVI, CVR, and IRA values ≥ 0.78) indicate a strong consensus among experts about the categorization, suggesting high content validity.
However, certain limitations must be acknowledged. The content validation, though methodologically sound, does not substitute for construct or criterion validation, which would require psychometric modeling or outcome correlation (for example, with polysomnography or validated screening scores). In addition, the expert panel size, although acceptable for CVI analysis, may limit generalizability. Future studies with larger panels or involving Delphi consensus methods could further strengthen the findings.
Despite these limitations, this domain classification provides a structured framework for interpreting the FAirEST-15 tool, potentially enabling domain-specific risk scoring, subanalysis, and improved clinical utility—particularly in dental and ENT settings where SDB-related orofacial features are highly relevant.
CONCLUSIONS
The current study successfully established an expert-derived domain classification for the FAirEST-15 clinical tool, validated through strong content validity indices and interrater agreement. Organizing the 15 clinical features into 7 anatomically and functionally meaningful domains enhances the tool’s interpretability, diagnostic consistency, and potential for future risk stratification models.
The involvement of pediatric dentists in both the development and validation process reinforces the crucial role of dental professionals in the early identification of SDB in children. Because orofacial signs of airway dysfunction are often encountered during routine dental examinations, the use of structured screening frameworks such as the FAirEST-15—supported by validated domain classification—can empower pediatric dentists to make timely referrals and promote interdisciplinary care. This work adds value to pediatric dental practice by enabling evidence-based screening and aligning with broader preventive strategies in child health.
REFERENCES
1. Lumeng JC, Chervin RD. Epidemiology of pediatric obstructive sleep apnea. Proc Am Thorac Soc. 2008 Feb 15;5(2):242-52.
2. Gozal D. Sleep-disordered breathing and school performance in children. Pediatrics. 1998 Oct;102(3 Pt 1):616–20.
3. Kaditis AG, Alvarez MLA, Boudewyns A, et al. Obstructive sleep disordered breathing in 2- to 18-year-old children: Diagnosis and management. Eur Respir J. 2016;47(1):69–94.
4. Marcus CL, Brooks LJ, Ward SD, et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012 Sep;130(3):e714–55.
5. Bixler EO, Vgontzas AN, Lin HM, et al. Sleep disordered breathing in children in a general population sample: Prevalence and risk factors. Sleep. 2009 Jun;32(6):731–6.
6. Fagundes NCF, Flores-Mir C. Pediatric obstructive sleep apnea-Dental professionals can play a crucial role. Pediatr Pulmonol. 2022 Aug;57(8):1860-1868.
7. Pirelli P, Saponara M, Guilleminault C. Rapid maxillary expansion in children with obstructive sleep apnea syndrome. Sleep. 2004 Dec;27(4):761–6.
8. Guilleminault C, Huseni S, Lo L. A frequent phenotype for paediatric sleep apnoea: short lingual frenulum. ERJ Open Res. 2016 Feb;2(2):00043–2016.
9. Oh JS, Zaghi S, Peterson C, Law CS, Silva D, Yoon AJ. Determinants of sleep-disordered breathing during the mixed dentition: Development of a functional airway evaluation screening tool (FAIREST-6). Pediatr Dent. 2021 Jul 15;43(4):262-272.
10. Goldstein NA, Pugazhendhi V, Rao SM, et al. Clinical assessment of pediatric obstructive sleep apnea. Pediatrics. 2004 Jul;114(1):33- 43.
11. McNamara JA Jr. Influence of respiratory pattern on craniofacial growth. Angle Orthod. 1981;51(4):269–300.
12. Rubio DM, Berg-Weger M, Tebb SS, Lee ES, Rauch S. Objectifying content validity: Conducting a content validity study in social work research. Soc Work Res. 2003;27(2):94–104.
13. Polit DF, Beck CT. The content validity index: Are you sure you know what's being reported? Critique and recommendations. Res Nurs Health. 2006;29(5):489–97.
14. Lynn MR. Determination and quantification of content validity. Nurs Res. 1986;35(6):382– 5.
15. Villa MP, Rizzoli A, Miano S, Malagola C. Efficacy of rapid maxillary expansion in children with obstructive sleep apnea syndrome: 36 months of follow-up. Sleep Breath. 2011;15(2):179– 84.
16. Zaghi S, Valcu-Pinkerton S, Gonzalez M, et al. Lingual frenuloplasty with myofunctional therapy: Exploring safety and efficacy in 348 cases. Laryngoscope Investig Otolaryngol. 2019 Feb;4(5):489–96.
17. Mitchell RB, Archer SM, Ishman SL, et al. Clinical practice guideline: tonsillectomy in children (update). Otolaryngol Head Neck Surg. 2019 Feb;160(1_suppl):S1–S42.
18. Zide BM, McCarthy J. The mentalis muscle: an essential component of chin and lower lip position. Plast Reconstr Surg. 1989 Mar;83(3):413-20. PMID: 2645595.
19. Carra MC, Huynh N, Lavigne GJ. Sleep bruxism: a comprehensive overview for the dental clinician interested in sleep medicine. Dent Clin North Am. 2012 Apr;56(2):387–413.
20. Abreu RR, Rocha RL, Lamounier JA, Guerra ÂF. Etiology, clinical manifestations and concurrent findings in mouth-breathing children. J Pediatr (Rio J). 2008;84(6):529–35.
21. Bruni O, Ottaviano S, Guidetti V, et al. The Sleep Disturbance Scale for Children (SDSC): construction and validation of an instrument to evaluate sleep disturbances in childhood and adolescence. J Sleep Res. 1996;5(4):251–261.
22. Chervin RD, Hedger K, Dillon JE, Pituch KJ. Pediatric Sleep Questionnaire (PSQ): Validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problems. Sleep Med. 2000;1(1):21–32.
23. Malow BA, Connolly HV, Weiss SK, et al. The Pediatric Sleep Clinical Global Impressions Scale-A new tool to measure pediatric insomnia in autism spectrum disorders. J Dev Behav Pediatr. 2016 Jun;37(5):370-6.
24. Zaghi S, Peterson C, Oh J, et al. Fairest-15. Tools. FAirEST.org; 2018. Available at: http://www.fairest.org/tools/
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted July 1, 2025
Submitted in final revised form September 1, 2025
Accepted for publication October 10, 2025
Address correspondence to: Dr. Lekshmy SR Nair, MDS. Email: lekshmysrnair@gmail.com
DISCLOSURE STATEMENT
Supplementary Appendix
Supplementary Appendix 1 – Part A: Original Items of FAirEST-15(more...)
{kind=link}
Supplementary Appendix 1 – Part B: Validated Domain Groupings of FAirEST-15
(more...)
{kind=link}