Original Article 2, Issue 12.4
ApnoDent®: A New Hybrid Mandibular Advancement Device for the Treatment of Temporomandibular Joint and Sleep-Related Breathing Disorders
http://dx.doi.org/10.15331/jdsm.7410
Joseph Yousefian, DMD, MS, MA1; Sunil Aggarwal, MD, PhD2; Colette Cozean, PhD3; Jay Levy, DDS4
1ApnoMed. Inc. Cofounder and Chief Scientific Officer, Bellevue, WA, USA, Private Practice, Bellevue, WA, USA; 2Advanced Integrative Medical Science Institute, Seattle, WA, USA, College of Arts and Sciences, University of Washington, Seattle, WA, USA; 3The EyeDeas Company, Lake Forest, CA. USA, Fuller Foundation: Board Member, Executive Committee Member, Co-Chair of Strategic Planning Committee. Lake Forest, CA. USA, East Africa Partnership: President and Chair of the Board of Directors. Lake Forest, CA, USA; 4Private Practice, Portland, OR, USA
ABSTRACT
Objectives:
To evaluate ApnoDent® as a new hybrid mandibular advancement device for treating patients with temporomandibular joint and sleep-related breathing disorders.
Methods:
Retrospective baseline and titration polysomnogram comparisons of 91 patients with obstructive sleep apnea and temporomandibular joint disorder after wearing a hybrid mandibular advancement device (ApnoDent®) for 6 to 12 months were reported.
Results:
The clinical data showed the resolution of symptoms of temporomandibular joint disorder in 95.5% of patients (P<0.00001).
The optimum resolution with an apnea-hypopnea index less than 5 events/h was achieved for 91% of mild-moderate cases and 77% of severe-very severe cases (P=0.0001). No adverse events or harms were reported.
Conclusion:
Patients with temporomandibular joint disorder and mild to very severe obstructive sleep apnea may benefit from a hybrid mandibular advancement device as an alternative treatment option.
Keywords:
temporomandibular joint disorders, obstructive sleep apnea, bruxism, sleep-related breathing disorders, mandibular advancement device
Citation:
Yousefian J, Aggarwal S, Cozean C, Levy J. ApnoDent®: A New Hybrid Mandibular Advancement Device for the Treatment of Temporomandibular Joint and Sleep-Related Breathing Disorders. J Dent Sleep Med. 2025;12(4)
INTRODUCTION
Sleep-related breathing disorders (SRBD) and their severe form, obstructive sleep apnea (OSA), are characterized by episodes of partial or total obstruction in the upper airway during sleep, combined with snoring and often daytime sleepiness and tiredness. The airway obstruction causes an arousal reaction, with consequent sleep disturbance and impairment of sleep quality. The short-term effects of OSA are often job-related and also include traffic accidents due to excessive daytime sleepiness.1 The long-term medical consequences of untreated OSA are an increased risk of the development of high blood pressure, stroke, and heart failure.2
OSA currently is often diagnosed by a sleep physician but comprehensive management is by an interdisciplinary team.3 The first treatment choice for OSA, the most severe form of SRBD, is continuous positive airway pressure (CPAP). However, oral appliances are the most accepted and clinically proven alternatives to CPAP. These appliances classically cover the upper and lower dental arches and are designed to keep the lower jaw protruding during sleep. Oral appliance therapy utilizes mandibular advancement, increases the pharyngeal airway space, and reduces upper airway collapsibility. Results with the mandibular advancement device (MAD) can be comparable to CPAP in some patients.4 A recent 2-year follow-up study involving oral appliance therapy suggested that mild-to-moderate cases could be effectively managed with an adjustable oral appliance, whereas severe OSA should be initially managed with CPAP.5 A MAD that advances the mandible in a protruded position is an alternative treatment that opens the airway and thus avoids the collapse of the pharynx during sleep.6 Compliance is higher with a MAD than with CPAP. Although CPAP reduces the apnea-hypopnea index (AHI) more than the MAD, Anandam et al7 found that both CPAP and MAD are equally effective therapies in reducing the risk of fatal cardiovascular events in patients with severe OSA. White et al4 compared CPAP and MAD after 1 month of use and found that most patients preferred using a MAD (51%) rather than CPAP (21%); this finding is in agreement with earlier reports.7 Several different MAD designs are available commercially, and all seem associated with short- and long-term adverse experiences. The short-term adverse effects are complaints about the temporomandibular joint (TMJ), jaw muscles, and teeth.8,9,10
In a 10-year follow-up study with MAD treatment, Fransson et al2 found a significant change in the proclination of the mandibular incisors, retroclination of the maxillary incisors, increased anterior face height, and posterior rotation of the mandible. Other studies with follow-up of 7 years confirmed the same observations. In this study, as a result of the orthodontic adverse effects of the MAD appliances, retroclination of the maxillary incisors and proclination of the mandibular incisors with associated reductions in overbite and overjet were observed.11
There is evidence of the risk of the development of pain, change of bite, and functional impairment after long-term use of a MAD. It is also common for people to discontinue use of a MAD because of a reduced effect on OSA symptoms, especially if it is associated with adverse events.2,10,11
TMJ disorder, most often characterized by painful musculoskeletal signs and symptoms in the masticatory and pharyngorofacial system, is a pain syndrome estimated to affect approximately 5% to 15% of the population, predominantly women. Subjective sleep disturbance has been consistently reported in patients with TMJ disorder.12
The first line of treatment for TMJ disorder has been the nocturnal or diurnal use of masticatory stabilizing orthotics.13 Patients who present to the general dentist's office with complaints of TMJ pain may exhibit signs and symptoms such as muscle soreness, bruxism, joint soreness, limited range of movement, altered movement, facial pain, and tooth chipping or tooth movement. Dentists may be biased regarding whether these symptoms are oral or dental in origin. After a diagnosis of a TMJ disorder, bruxism, or muscular spasms due to occlusal instabilities is established, the treatment protocol often includes an oral appliance (such as a mouth guard worn at night), exercises, and pharmacologic agents. However, patients with SRBD can exhibit the same signs and symptoms as patients with TMJ disorders, and these symptoms can be misinterpreted as being dental in origin. Dental treatment can worsen these medical conditions, putting patients at further risk for untreated and aggravated SRBD along with its medical sequelae.14 A recent investigation using polysomnography (PSG) recordings and clinical sleep interviews in an uncontrolled sample of TMJ disorder cases showed that TMJ disorder is associated with primary sleep disorders, such as insomnia and OSA: almost 36% of cases of TMJ disorder met diagnostic criteria for insomnia, and more than 28% met criteria for OSA.12 In the same sample of TMJ disorder cases, sleep efficiency identified with PSG was directly related to a measure of pain threshold, suggesting an association between pain and sleep disturbance in TMJ disorder. Additionally, a high prevalence of TMJ disorder was reported in patients with mild to moderate OSA referred for a clinical dental evaluation, lending further support to the association between TMJ disorder and OSA. It was argued that a 28% rate of OSA diagnosis in a sample of patients with TMJ disorder composed mainly of young females with relatively low body mass index (BMI) lends support to the possibility of elevated risk of SRBD and OSA in TMJ disorder, requiring further evaluation in a large-scale study.12
Most patients consider that the positive treatment effect of a MAD on managing OSA outweighs the adverse effects.2 This may introduce a new opportunity for the clinician who treats this population of patients. A design of the appliance that can work for both purposes is an orthotic for TMJ disorder, which can also effectively manage OSA and sleep bruxism without the adverse effects of a MAD, a hybrid. The hybrid mandibular advancement device (HMAD) discussed in this article has six overlapping features: 1- TMJ disorder orthotic for stabilizing the masticatory system, 2- bruxism management, 3- anterior repositioning splint addressing intracapsular conditions including retrodiscitis, 4-a MAD for managing snoring, 5- a MAD for managing mild to moderate OSA, and 6- an orthodontic appliance helping to improve the malocclusion by itself or in combination with braces or aligners. The HMAD can also be used by patients who are getting orthodontic treatment with braces or aligners or simply wearing invisible retainers.
This retrospective study aims to achieve two objectives: to investigate the compliance, effectiveness, ease, and comfort of using HMAD for patients with mild to moderate experiencing TMJ disorder; and to test the effectiveness of HMAD for managing severe to very severe OSA and TMJ disorder cases using a novel in-laboratory titration method for patients who have not been able to tolerate CPAP and MAD therapy.
MATERIALS AND METHODS
- History of trauma or congenital abnormalities to the TMJ
- Odontogenic infections or any other pathologic swelling concerning the TMJ
- Metastatic tumors, cysts, or carcinomas of the oral cavity affecting the TMJ
- Regular intake of medicines such as analgesic agents or antianxiety drugs
{kind=link}
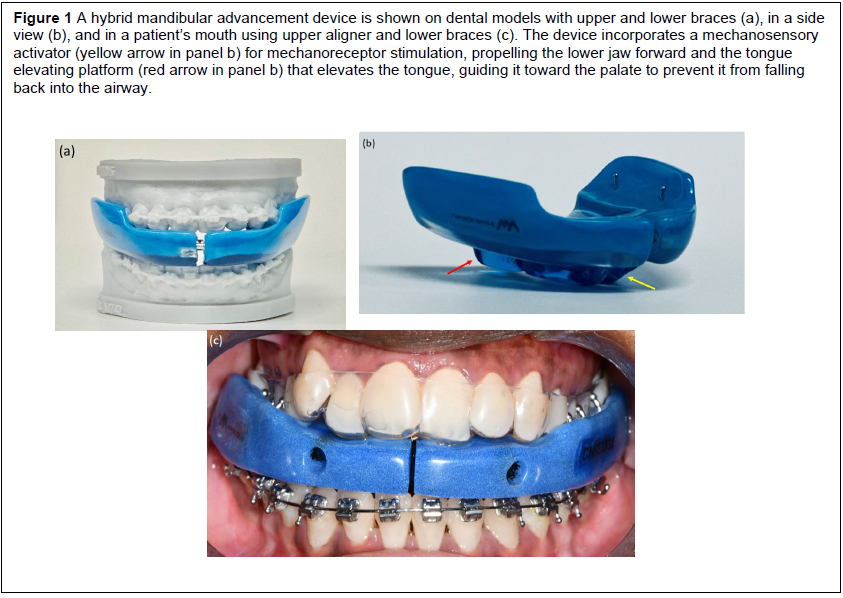
Some of these patients never had any diagnosis of OSA. Still, most had a previous diagnosis of mild to very severe levels of OSA and declined treatment or CPAP or other forms of MAD therapy were unsuccessful. The sample received treatment with Apnodent® as an HMAD, a masticatory orthotic and adjustable oral sleep appliance. The Apnodent® is approved by the US Food and Drug Administration (FDA) as a MAD. It is a custom-fabricated oral device (Figures 1 through 3) used to treat patients with masticatory disorders, snoring, and mild to moderate OSA. Given these approvals, its use could be extended to treating patients with severe cases of OSA if they cannot tolerate CPAP. As a MAD, the device alleviates obstruction in the retropalatal, retroglossal, and hypoglossal pharyngeal space. The device also incorporates a lifting mechanism for the root of the tongue (Figure 1 b) to prevent it from falling back by guiding it toward the palate and front of the mouth.
This preliminary study comprised 91 patients with TMJ disorder (47 men and 44 women) with mild to very severe masticatory and intracapsular symptoms, including advanced TMJ arthritis and condylar resorption unilaterally or bilaterally. A combination of self-reporting, clinical examinations, validated questionnaires, and radiographic analysis assessed the TMJ disorder and the presence of degenerative bone remodeling. Mild to very severe OSA was diagnosed in some patients who were unable to tolerate MAD and CPAP therapy or had a relapse due to previous use of other forms of a MAD. The total sample was subdivided into the following groups: mild (AHI > 5 < 15 events/h), moderate (AHI > 15 < 30 events/h), severe, and very severe (AHI > 30 < 100 events/h). After obtaining informed consent from the patients in this study, a single clinician with board certification from the American Board of Orthodontics and the American Academy of Dental Sleep Medicine custom-fitted each device. All patients received the same custom-fitted HMAD, some in conjunction with invisible retainers, and others with aligners or braces. Study participants were required to demonstrate that they tolerated and complied with using the device for at least 1month. After this assessment, when participants reported subjective improvement in OSA and TMJ disorder symptoms, supported by clinical examination, a titration PSG was performed in an accredited sleep laboratory to evaluate the efficacy of the HMAD in the improvement of OSA and bruxism.15 To determine the most effective setting, data collection from a titration polysomnographic study was performed with a sleep technologist who was present during the patient's habitual sleep period according to standards established by the American Academy of Sleep Medicine (AASM). Parameters include bilateral electrooculographic tracings; electroencephalographic tracings (modified 10:20 electrode configuration, featuring bilateral central and occipital leads); surface electromyography of submental musculature and bilateral anterior tibialis muscles; thoracic and abdominal piezo-crystal respiratory belt recordings; electrocardiography; arterial oxygen hemoglobin saturation via finger pulse oximetry; and snoring intensity via decibel meter recording. Body position and standard audio–video recording were also monitored. The recorded signal tracings, including apneas and hypopneas, were scored using the AASM scoring manual.16
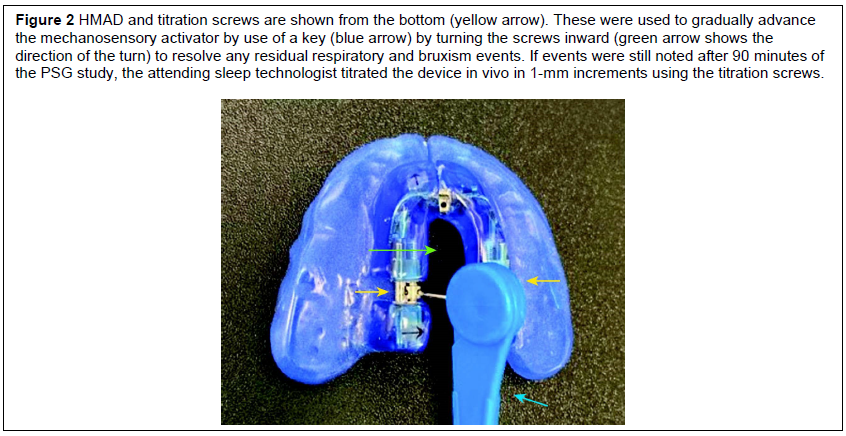
The sleep technologist used the protocol of CPAP titration as per AASM guidelines.16 Titration was performed by gradually adjusting the device to resolve residual snoring, apneas, hypopneas, oxygen desaturations, bruxism, and arousals. If obstructive events were still noted after 90 minutes of the PSG study, the attending sleep technologist titrated the device in vivo in 1-mm increments in a protrusive direction for a maximum of three times or 3 mm, for optimal effect and to minimize sleep disturbance, using titration screws (Figure 2). This procedure ensured that the appliance was effective in various body positions and during the different sleep stages.
Patients similar to those in the case shown in Figure 3 who did not have a previous diagnosis of OSA and decided to reduce costs associated with full overnight PSG had split-night PSG studies (SNPSG), combining diagnostic and HMAD titration testing. The final portion of the study was used for titrating the HMAD. A minimum of 3 hours of sleep was adequately assigned to titrate the HMAD.17 SNPSG acquired recording and analysis of the same parameters as those evaluated in standard diagnostic PSG. If a single SNPSG study did not permit adequate titration of HMAD to control the symptoms, additional full-night PSG for HMAD titration was performed later. An attending dental sleep specialist reviewed the data to determine the most appropriate position for the device. An attending board-certified sleep physician then interpreted the final PSG results and determined the efficacy of the oral appliance according to AASM guidelines.16
The final summary report included the interpreting physician’s assessments and any significant observations, such as bruxism, snoring, rapid eye movement-dominant OSA, or any other events during sleep. In addition, the summary included data from each titration, post-titration AHI, rapid eye movement sleep duration, oxygen saturation, and incremental millimeter advancement, which was provided. The attending physician determined whether the OSA had been adequately treated according to the AASM criteria. If required, recommendations were made regarding supplemental oxygen, central sleep apnea management, and combination therapy with CPAP.
The orthodontist adjusted the HMAD after titration for proper occlusion. Patients were followed up with periodic examinations every 2 to 4 months to monitor TMJ disorder symptoms and manage OSA, as recommended by the Clinical Practice Guideline for the Treatment of OSA.18 A total of 74 patients, including the patient described in Figure 3, decided to use HMAD for long-term management of TMSD and OSA. The remaining patients proceeded with orthodontic treatment with surgical or nonsurgical procedures for definitive treatment of their TMJ disorder and OSA. Statistical analysis was performed on the PSG data using matched, paired t-tests (SAS University Edition).
{kind=link}
Figure 2. HMAD and titration screws are shown from the bottom (yellow arrow). These were used to gradually advance
the mechanosensory activator by use of a key (blue arrow) by turning the screws inward (green arrow shows the
direction of the turn) to resolve any residual respiratory and bruxism events. If events were still noted after 90 minutes of
the PSG study, the attending sleep technologist titrated the device in vivo in 1-mm increments using the titration screws.
{kind=link}
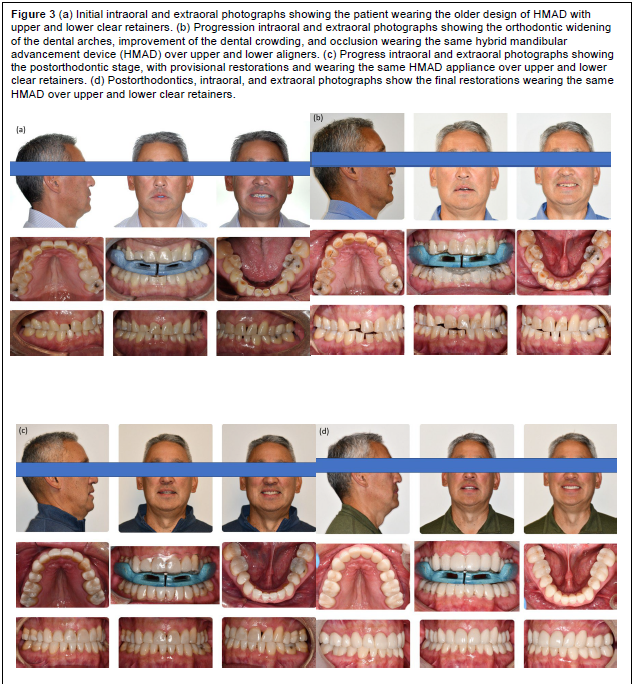
Figure 3. (a) Initial intraoral and extraoral photographs showing the patient wearing the older design of HMAD with
upper and lower clear retainers. (b) Progression intraoral and extraoral photographs showing the orthodontic widening
of the dental arches, improvement of the dental crowding, and occlusion wearing the same hybrid mandibular
advancement device (HMAD) over upper and lower aligners. (c) Progress intraoral and extraoral photographs showing
the postorthodontic stage, with provisional restorations and wearing the same HMAD appliance over upper and lower
clear retainers. (d) Postorthodontics, intraoral, and extraoral photographs show the final restorations wearing the same
HMAD over upper and lower clear retainers.
{kind=link}
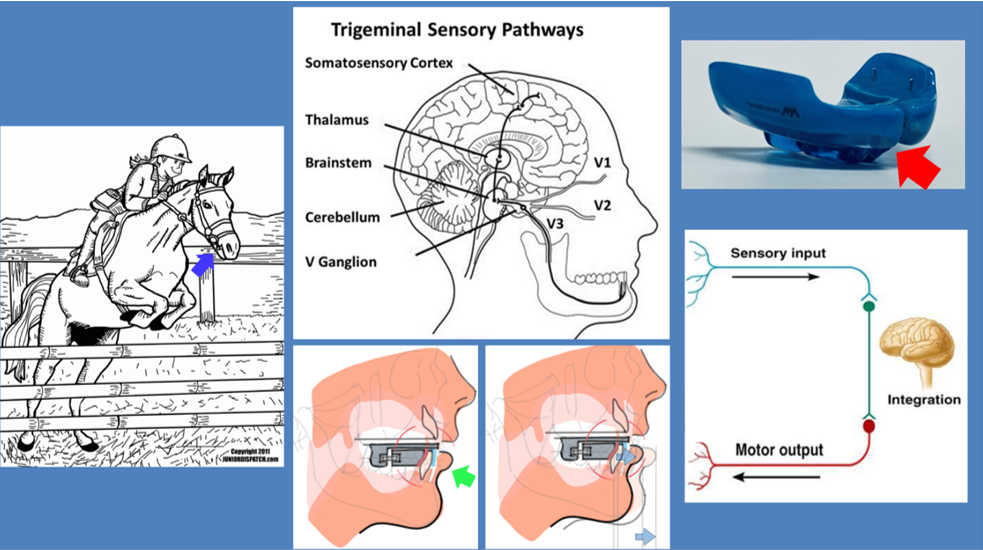
Figure 4. The lingual contact arm of the mechanosensory activator (MSA) in the hybrid mandibular advancement device (HMAD), similar to a bit in a horse's mouth, stimulates mechanosensory reflexes, which activate mandibular forward repositioning through the stimulation of intradental A-beta mechanoreceptors and periodontal A-beta mechanoreceptors and the process of sensory-motor integration. The red arrow points to the MSA in the HMAD, the blue arrow points to the bit in the horse’s mouth, and the green arrow points to the MSA touching the lower anterior teeth.
{kind=link}
RESULTS
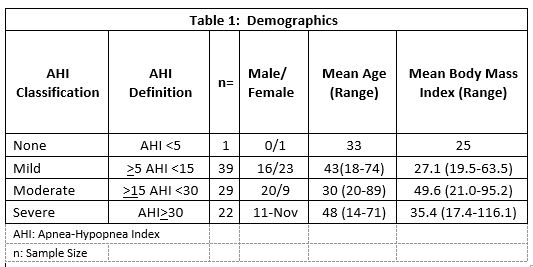
The total sample was subdivided into the following groups: mild (AHI > 5 < 15 events/h; n = 39), moderate (AHI > 15 < 30; n = 29), severe, and very severe (AHI > 30 < 100; n = 22). The average age of the patients in the mild group was 43 years (range, 18 to 74 years), the average age of the moderate group was 30 years (range, 20 to 89 years), and the average age of the severe to very severe group was 48 years (range, 14 to 71 years). The average BMI of the mild group was 27.1 kg/m² (range, 19.5 to 63.5 kg/m²), for the moderate group, 49.6 kg/m² (range, 21.0 to 95.2 kg/m²), and 35.4 kg/m² (range, 17.4 to 116.1 kg/m²) for the severe to very severe group The mild group consisted of 16 males and 23 females, and the moderate and severe groups consisted of 20 females and 9 males and 11 males and females each, respectively. There was one female who had an AHI of 4 events/h, qualifying for the “none” category. Table 1 summarizes these results.
At the outset of treatment, 72.5% of patients demonstrated symptoms of TMJ disorder; this number decreased to 4% after treatment. No correlation was found between the presence or severity of TMJ disorder and the onset or severity of OSA. Treatment success was determined by significant improvement of symptoms of TMJ disorder, including jaw pain, headaches, and joint clicking, as a resolution of OSA symptoms as defined by AASM criteria(American Sleep Disorders Association 1995).19 The clinical data showed a significant adherence to the use of the HMAD at the end of 12 months and resolution of symptoms of TMJ disorder mentioned previously in 95.5% of patients (P<.00001).
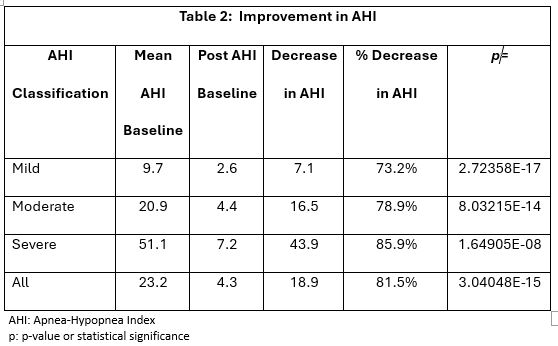
The PSG data showed significant improvements in OSA measures. Overall, patients improved from a mean baseline AHI of 23.2 events/h to a mean AHI of 4.3 events/h, a mean decrease of 18.9 events/h (P<.00001). For the mild cases, the mean baseline AHI was 9.7 events/h (range, 5.7-14.5 events/h); in the moderate cases, the mean baseline AHI was 20.9 events/h (range, 15.4-28.6 events/h), whereas it was 51.1 events/h (range, 31.8-76.7 events/h) in severe to very severe cases (1 teenager age 14 years with a severe score of 17.1 events/h). For the patients with mild-moderate OSA (36 males, 32 females), optimum resolution with an AHI < 5 events/h was achieved for 62 of the 68 patients. A total of 91% of the mild-moderate OSA patient subsample showed optimal resolution. For this subsample, the average AHI in mild cases decreased from 9.7 to 2.6 events/h, whereas in the moderate subsample, the average AHI of 20.9 decreased to 4.4 (Table 2).
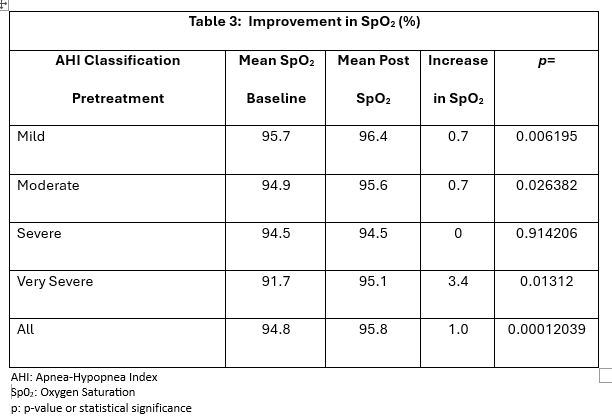
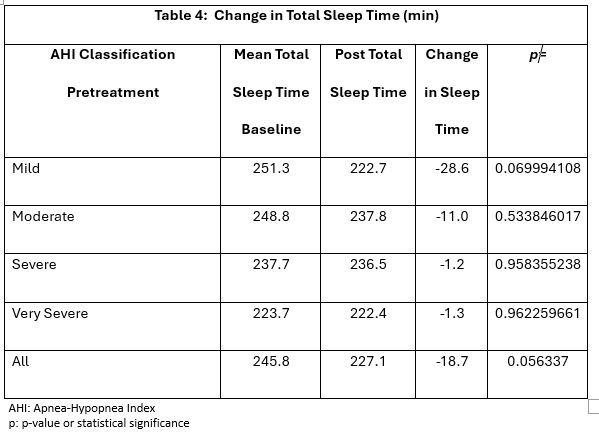
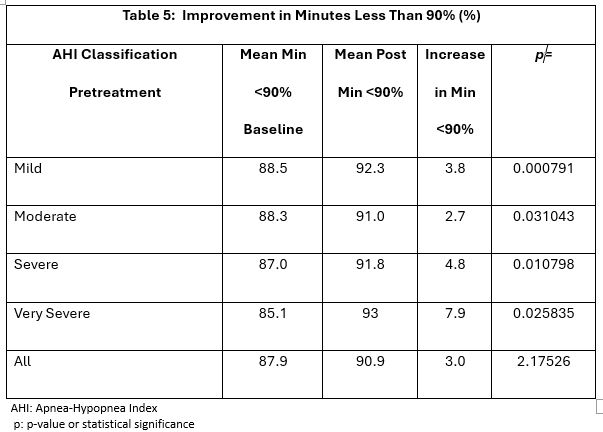
For those with severe OSA (11 males and 11 females), optimum resolution with an AHI less than 5 events/h was achieved for 17 of the 22 patients. Thus, 77% of the severe OSA subsample showed optimal resolution. The average AHI decreased from 51.1 events/h (range, 31.8 to 76.7 events/h) to 7.2 events/h (range, zero to 59.7 events/h) for this subsample, and the oxygen saturation (SpO2 ) nadir improved from 94 to 95.8% (P=.0001). Likewise, the percentage of sleep time with SpO2 saturation less than 90% improved to 21% of the night. Sleep time decreased from 248.9 to 227.1 minutes. These findings are summarized in Tables 3 through 5.
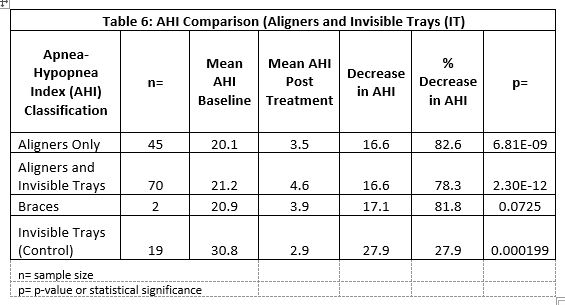
Forty-five of the patients wore aligners and an additional 25 wore aligners followed by retainers. These were compared to 19 patients who also wore retainers. One patient wore aligners and braces and one wore braces alone. Their AHI scores are shown in Table 6. Two patients with large tongues showed a worsening of their results by 30%.
Table 1. Demographics |
{kind=link}
Table 2. Improvement in AHI
{kind=link}
Table 3. Improvement in SpO2 (%)
{kind=link}
Table 4. Change in Total Sleep Time (min)
{kind=link}
Table 5. Improvement in Minute Less Than 90% (%)
{kind=link}
Table 6. AHI Comparison (Aligners and Invisible Trays (IT)
{kind=link}
DISCUSSION
Currently, both CPAP and MAD, which act to improve nasopharyngeal patency during sleep, remain the standard of care for managing sleep apnea.20 In a recent study, the long-term follow-up and comparison regarding the efficacy of these therapies, including patient adherence and satisfaction over a 10-year follow-up period, were reported. CPAP and MAD therapy demonstrated good and stable treatment effects after a 10-year follow-up period. Therefore, when indicated, both therapies are appropriate modalities for the long-term management of OSA.21
As with any medical treatment, there are possible complications or adverse effects to dental sleep therapy or even the use of CPAP22 Despite the advances in treating OSA with MAD, their effectiveness depends on the patient’s compliance. One of the aims of this study was to evaluate the long-term adherence to HMAD therapy and the patient’s treatment experiences with TMJ disorder and OSA. Previously reported by Saglam-Aydinatay et al.23, the most common reasons reported by patients for noncompliance were the inability to adapt to the appliance and pain in the temporomandibular joint. The most common factors associated with continued usage were effectiveness (100%) and ease of use (64%) 23. Doff et al.5 assessed variations in the occurrence of TMJ disorders and the risk of the development of pain and functional impairment of the TMJ complex in OSA patients treated with either MAD or CPAP in a 2-year follow-up study. They reported that oral appliance therapy resulted in more TMJ pain compared to CPAP.
Most dental sleep devices work by moving the lower jaw forward by a different mechanism of pulling or pushing, anchoring the upper and lower teeth to open the throat and a collapsible airway.20 Due to this forward positioning of the lower jaw and teeth and retraction of the upper teeth, there is a risk of changes in bite and occlusion,2 development of TMJ disorder, and muscular discomfort.23,24
In contrast, there is no anchoring of upper or lower teeth in HMAD. The lingual contact arm of the mechanosensory activator (MSA) in HMAD (Figures 1 and 4), similar to a bit in a horse's mouth (Figure 4), stimulates mechanosensory reflexes in the lower anterior teeth and periodontium, which activate mandibular forward repositioning muscles through the stimulation of intradental A-beta mechanoreceptors (IMs) and periodontal A-beta mechanoreceptors (PDLMs) and the process of sensory-motor integration.25 Our study showed that because HMAD is titratable and adjustable for proper occlusion, each device can be adjusted gradually from minimal advancement to more as needed to help enlarge oropharyngeal space with no discomfort; as a result, long-term musculoskeletal pain is rare. Short-term discomfort was usually managed by adjusting the HMAD to a more comfortable setting. On a rare occasion, the device can continue to cause muscle soreness, and in this case, simply adjusting the device for ideal occlusion and bite stability would stop the muscle and intracapsular discomfort. Certain patients with existing TMJ disorder may not be able to wear a MAD.23 In this study, most patients with TMJ disorder saw improvement of their jaw problems and OSA by wearing an HMAD that idealized their bite, bruxism, and TMJ stability, such as the patient described in Figure 3.
MAD therapy has been advocated primarily for patients with mild to moderate OSA, although recent data demonstrate efficacy in some patients with more severe diseases.26 The current treatment of choice in patients in whom moderate to severe OSA has been diagnosed is CPAP. However, this approach is prone to intolerance, and compliance is sometimes less than optimal.18 Even though some cases of OSA are thought to be disorders of craniofacial anatomy, the use of MAD is not typically recommended in patients with a severe or very severe form of the disease unless the patient cannot tolerate CPAP.
In the current study, among 91 patients between ages 14 and 89 years, it was noted that 72.5% of the patients had symptoms of TMJ disorder at the outset of the treatment, and this number was reduced to 4%. The longest duration of usage, 7 years, has been by the oldest patient in this retrospective study, who was 95 years old at the time this information was reported and who initially had symptoms of TMJ disorder and significant bite changes after using a Herbst appliance as a MAD.
Ferreira et al.27 conducted a study on 1,000 patients and found that women were more commonly affected by TMJ disorder. In the current study, 60% of patients with signs and symptoms of TMJ disorder were women.
The effect of myofascial pain on the central control of muscles involved in breathing, chewing, and swallowing as a co-contraction stimulus has been hypothesized to provide a pathophysiologic mechanism relating TMJ disorder to sleep-disordered breathing.28 This prolonged and exaggerated co-contraction of pharyngorofacial and oropharyngeal musculature is an active neuromotor control that provides greater levels of tonus for increased stabilization. One adverse effect of this hyperactivity is pain in the pharyngorofacial complex, causing symptoms of TMJ disorder, dysfunction, and additional pain. One possible interpretation of these findings in the development of SRBD is that upper airway resistance is increased in TMJ disorder. Therefore, sleep-disordered breathing might be a source of sleep disturbance in patients with TMJ disorder. Alternatively, a pain-related decrease in the arousal threshold in patients with TMJ disorder may set the stage for more frequent arousals during minor airway-narrowing episodes that do not necessarily lead to arousals in control patients.12
In this study, 95.5% of patients (P<.00001) with severe to very severe OSA responded well to the use of HMAD in treating symptoms of TMJ disorder, as supported by other studies.26 Therefore, the use of HMAD as an orthopedic and bruxism orthotic and its role in reducing chronic pain conditions could be described as its effective mechanism in increasing the arousal threshold to respiratory stimuli during sleep; this issue needs to be determined in future studies.
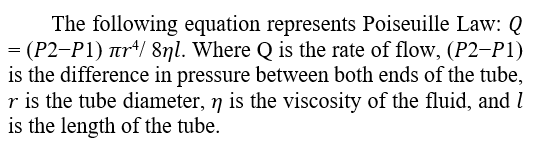
Poiseuille Law is a physical law successfully applied to airflow rates in the respiratory system. It calculates fluid flow rates in cylindrical tubes and accounts for frictional effects between moving fluids and the walls of tubes that contain and inhibit flow rate. The following equation represents Poiseuille Law. The flow rate is shown to be proportional to the tube radius raised to the 4th power.
The importance of Poiseuille Law for the management of sleep-disordered breathing is that the airflow rate is susceptible to the radius of the airway. The Poiseuille equation shows that a 20% increase in a tube's radius can double the fluid flow rate. Current strategies for the management of OSA take advantage of this physical law.
MADs are used to passively stretch the soft tissue walls of the oropharynx to increase the radius of the lumen and enhance airflow. When MADs are introduced between the teeth, they increase tensions within the fascia-tensegrity matrix of the orofacial region. These new passive tensions cause hyoid bone elevation and stretching of the tissues of the oropharynx, widening the lumen of the oropharyngeal opening and enhancing airflow and respiration. HMAD shares this capability through mechanosensory stimulation to advance the mandible instead of forceful forward holding of the lower jaw as with other MAD appliances (Figure 4).
A therapeutic benefit of MADs is thought to be achieved mostly in mild to moderate cases of sleep apnea when the lumen of the oropharyngeal opening is wide enough to allow normal oxygenation and sleep architecture. In the current study, 91% of mild to moderate cases and 77% of cases with severe to very severe OSA demonstrated a positive response to the use of HMAD for proper disease management.
Another factor influencing flow capacity is the rigidity of the tube's walls. Fluid flow in a tube can induce pressure changes across the walls, resulting in vibrations or flutter. Flutter in the walls of a floppy tube induces fluid flow turbulence, which reduces the flow rate. Maximum airflow rate may be achieved by widening the lumen and increasing wall rigidity to encourage nonturbulent laminar flow.
The rigidity of the airway can be increased, and airflow can be enhanced by passively stretching oropharyngeal soft tissue walls or by inducing an increased active myofibril tonus within the walls. Whereas most MADs use only passive myofascial forces, the HMAD appliance is unique among MADs in that it uses both active and passive myofascial forces to firm up and widen the walls of the oropharynx. A key aspect of the HMAD appliance is its use of the MSA to regulate mechanosensory stimulation of mandibular incisors to reflexively incite forward posturing of the mandible to open the airway.
One explanation for this issue is that the MSA in HMAD has an adjustable lingual contact arm that rests gently against the lingual surfaces of the mandibular incisors, providing weak mechanosensory stimulation of vital intradental and periodontal mechanoreceptors of these teeth.29 (Figure 4). Vital teeth contain a variety of mechanosensory nerve fibers, including A-delta and C pain fibers and A-beta mechanosensory fibers. Pressure on the teeth by the MSA stimulates slowly adapting A-beta mechanoreceptors located in incisor teeth' pulps and periodontal ligaments. IMs have fast conduction velocities, rapidly adapting characteristics, and are optimized to respond to transient forces and vibrations applied to teeth. PDLMs have fast conduction velocities, lower thresholds, and slowly adapting characteristics. They provide continuous mechanosensory feedback of forces applied to teeth. Cell bodies of IMs and PDLMs are located in the trigeminal ganglion and synapse in the brainstem's central sensory and mesencephalic nuclei, respectively (Figure 4).
Neurologic (Sensory) Signaling and Force Transmission in HMAD Use
The MSA in the HMAD makes contact with the lingual surfaces of the lower anterior teeth (Figure 4), initiating both neurologic and mechanical sensory signaling. This occurs through pressure-induced activation of mechanoreceptors and nociceptors (pain receptors) in the lower anterior teeth, the supporting periodontium, and the gingiva.
{kind=link}
a. Neurologic (Sensory) Signaling
Sensory signaling begins when the MSA exerts pressure on the lower anterior teeth and surrounding structures. This mechanical stimulus activates specialized sensory receptors:
- Mechanoreceptors detect pressure, stretch, and movement.
- Nociceptors respond to potentially harmful stimuli, contributing to pain perception.
- The jaw adapts to a myofascial adaptive position—a functional posture determined by muscle tone, fascia tension, and joint positioning.
- This adaptation is guided by sensory integration, where incoming signals are processed in the brainstem and cortex and integrated with prior motor learning and experience.
- The result is a coordinated motor response, positioning the mandible passively against the lower articulating surface of the HMAD.
Chapter authors’ data suggest that an SNPSG as a follow-up titration PSG is an effective method of demonstrating the efficacy of HMAD in treating OSA, even in the severe to very severe category. An SNPSG as an efficacy study involved titrating the HMAD in vivo to ensure proper resolution of OSA and supported the previously reported data.17
In this study, the attending technologist performed the titration during SNPSG while the patient slept wearing the HMAD. A board-certified sleep physician used the guidelines of AASM to interpret the SNPSG results to establish the efficacy of HMAD and prepared the summary report. The main variables used to determine the efficacy of HMAD were its effectiveness in improving the AHI and SpO2 nadir.
All SNPSG studies were completed consecutively during the study period to minimize the potential selection biases. No patient was excluded from this study, even those who discontinued using HMAD. The same expert sleep technologists were used to complete all of the titration SNPSGs. Finally, all results, such as the AHI and SpO2 nadir, were reviewed and interpreted by board-certified sleep specialists following established AASM guidelines. The AHI and SpO2 nadir are the most accepted measurements at this time to determine effective titration during an SNPSG study.17 Nevertheless, the results of the current study showed significant improvements in both severe and very severe categories of OSA studied, and it was found that most of the study participants showed substantial improvement in AHI and SpO2 nadir. Oxygen saturation SpO2 nadir is an associated marker of oxidative stress that potentiates the detrimental process of atherosclerosis.30 Oxidative stress is another fundamental mechanism contributing to cardiovascular diseases in OSA.30
This study showed that the use of HMAD significantly increased the lowest posttreatment SpO2, regardless of disease severity (P < 0.001: Tables 5 and 6). Furthermore, a review of the desaturation data indicated that treatment significantly reduced the percentage of total oxygen desaturation sleep time by approximately 7% (P < 0.001; Table 5).
More significantly, when the pretreatment, baseline AHI, and SpO2 nadir were compared with the posttreatment period (Tables 5 and 6), the analysis revealed a most notable effect in patients with severe and very severe OSA (Table 1). These findings are significant because they demonstrated that HMAD was effective in managing even severe to very severe OSA. In two patients with moderate and severe sleep apnea, the severity of sleep apnea got worse by wearing the appliance because of narrow arches and large tongues and a high modified Friedman score.31
Data showed little or no correlation between the efficacy of HMAD and a range of other variables, such as sex, age, and BMI. This study demonstrated significant improvement of OSA in both older as well as younger individuals, in contrast to data reported previously, which suggested patients with a good response to MAD were younger.32 Similarly, Otsuka and colleagues33 found that patients with lower BMIs were more likely to respond to MAD, contrasting the findings of this study. Importantly, however, HMAD was found to effectively manage both severe and very severe OSA (Tables 5, 6).
CONCLUSIONS
Based on the current evidence, treatment with MAD successfully resolves moderate to severe OSA in 31% of patients. The results of the current study appear to extend this range into severe and very severe cases of OSA with 77% efficacy.
This study showed that because HMAD is adjustable, each device can be adjusted gradually from minimal advancement to more as needed to help enlarge oropharyngeal space with no discomfort; as a result, long-term musculoskeletal pain is rare.
In the current study, among 91 patients age 14 to 89 years, 72.5% of the patients had symptoms of TMJ disorder at the outset of the treatment, and this number was reduced to 4%.
In this study, 95.5% (P<.00001) of patients with severe to very severe OSA responded well to using HMAD in treating symptoms of TMJ disorder, as supported by other studies. Therefore, the use of HMAD as an orthopedic and bruxism orthotic and its role in reducing chronic pain conditions could be described as its effective mechanism in increasing the arousal threshold to respiratory stimuli during sleep; this issue needs to be determined in future studies.
In the current study, 91% of mild to moderate cases and 77% of cases with severe to very severe OSA demonstrated a positive response to using HMAD for proper disease management.
This study showed that HMAD significantly increased the lowest posttreatment SpO2, regardless of disease severity. Furthermore, a review of the desaturation data indicated that treatment significantly reduced the percentage of total SpO2sleep time by approximately 7%.
More significantly, when the pretreatment baseline AHI, and SpO2 nadir were compared with that in the posttreatment period, the analysis revealed the most notable effect in patients with severe and very severe OSA.
The results of the current study are encouraging and demonstrate that patients with TMJ disorder and mild to very severe OSA may benefit from HMAD as an alternative treatment option.
The study’s modest sample size, retrospective design, and lack of a control group limit the results. There is now a clear need for well-controlled, prospective trials with larger sample sizes and a control group to determine the overall efficacy of HMAD with overnight PSG titration in treating patients with severe to very severe OSA.
REFERENCES
1. Garbarino S. Excessive daytime sleepiness in obstructive sleep apnea: implications for driving licenses. Sleep Breath. 2020;24:37-47. doi:10.1007/s11325-019-01903-6
2. Fransson A, Benavente-Lundahl C, Isacsson G. A prospective 10-year cephalometric follow-up study of patients with obstructive sleep apnea and snoring who used a mandibular protruding device. Am J Orthod Dentofacial Orthop. 2020;157:91-97.
3. Behrents R, Sheigika AV, Conley S. Obstructive sleep apnea and orthodontics: an American Association of Orthodontists White Paper. Am J Orthod Dentofacial Orthop. 2019;156(1):13-28.
4. White DP, Shafazand S. Mandibular advancement device vs CPAP in the treatment of obstructive sleep apnea: are they equally effective in short term health outcomes? J Clin Sleep Med. 2013;9:971-972.
5. Doff MHJ, Hoekema A, Wijkstra. Oral appliance versus continuous positive airway pressure in obstructive sleep apnea syndrome: a 2-year follow-up. Sleep. 2013;36:1289-1296.
6. Ramar K, Dort LC, Katz SG. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: an update for 2015. J Clin Sleep Med. 2015;11:773-827.
7. Anandam A, Patil M, Akinnusi M. Cardiovascular mortality in obstructive sleep apnoea treated with continuous positive airway pressure or oral appliance: an observational study. Respirology. 2013;18:1184-1190.
8. Isacsson G, Nohlert E, Fransson AMC. Use of bibloc and monobloc oral appliances in obstructive sleep apnoea: a multicentre, randomized, blinded, parallel-group equivalence trial. Eur J Orthod. 2019;41:80-88.
9. Taga H, Fukuda T, Katahira H, et al. Consequences and implications of discontinuing oral appliance therapy for obstructive sleep apnea: Be true to the tooth. J Dent Sleep Med. 20025;12(1). doi:10.15331/jdsm.7374
10. Yousefian J, Moghadam B. Orofacial complications associated with forward repositioning of the mandible in snore guard users. Gen Dent. 2003;51(6).
11. Wang X, Gong X, Yu Z. Follow-up study of dental and skeletal changes in patients with obstructive sleep apnea and hypopnea syndrome with long-term treatment with the Silensor appliance. Am J Orthod Dentofacial Orthop. 2015;147:559-565.
12. Dubrovsky B, Lavigne G. Polysomnographic investigation of sleep and respiratory parameters in women with temporomandibular pain disorders. J Clin Sleep Med. 2014;15(10(2)):195-201. doi:10.5664/jcsm.3452
13. Eliassen M, Hjortsjö C, Olsen-Bergem H. Self-exercise programmes and occlusal splints in the treatment of TMD-related myalgia—Evidence-based medicine? J Oral Rehabil. 2019;46:1088-1094. doi:10.1111/joor.12856
14. Babiec D. Temporomandibular pain caused by sleep disorders: a review and case report. Gen Dent. 2017;65(4):30-33.
15. Sivaramakrishnan G, Sridharan K. A systematic review on the effectiveness of titratable over nontitratable mandibular advancement appliances for sleep apnea. J Indian Prosthodont Soc. 2017;17(4):319-324. doi:10.4103/jips.jips_115_17
16. Berry RB, Brooks R, Gamaldo CE, et al. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications. Version 2.4. American Academy of Sleep Medicine. 2017.
17. Wahba N, Sayeeduddin S, Diaz-Abad M. The utility of current criteria for split-night polysomnography for predicting CPAP eligibility. Sleep Breath. 2019;3:729-734. doi:10.1007/s11325-018-1747-y
18. Ramar K, Dort LC, Katz SG. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: an update for 2015. J Dent Sleep Med. 2015;2(3):71-125.
19. American Sleep Disorders Association. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances. Sleep. 1995;18:511-513.
20. Lavigne GJ, Herrero Babiloni A, Beetz G. Critical issues in dental and medical management of obstructive sleep apnea. J Dent Res. 2020;99(1). doi:10.1177/0022034519885644
21. Uniken Venema JAM, Doff MHJ, Joffe-Sokolova D. Long-term obstructive sleep apnea therapy: a 10-year follow-up of mandibular advancement device and continuous positive airway pressure. J Clin Sleep Med. 2020;15(16):353-359. doi:10.5664/jcsm.8204
22. Nikolopoulou M, Aarab G, Ahlberg J. Oral appliance therapy versus nasal continuous positive airway pressure in obstructive sleep apnea: a randomized, placebo-controlled trial on temporomandibular side-effects. Clin Exp Dent Res. 2020;6(4):400-406. doi:10.1002/cre2.288
23. Saglam-Aydinatay B, Taner T. Oral appliance therapy in obstructive sleep apnea: long-term adherence and patients’ experiences. Med Oral Patol Oral Cir Bucal. 2018;1(23):e72-e77. doi:10.4317/medoral.22158
24 Ettlin DA, Mishra SS. Temporomandibular disorders in relation to mandibular advancement devices for treating obstructive sleep apnea. Dent Clin North Am. 2024;268(3):533-540. doi:10.1016/j.cden.2024.02.003
25. Yousefian J. New approaches in adult orthodontics for the treatment of OSA with the Teledontic – ApnoTX and Telegnathic surgical assisted approaches beyond the MARPE and DOME procedures. Sleep Education Consortium, Houston TX. 2023.
26. Byun JI, Kim D, Ahn SJ. Efficacy of oral appliance therapy as a first-line treatment for moderate or severe obstructive sleep apnea: a Korean prospective multicenter observational study. J Clin Neurol. 2020;16(2):215-221. doi:10.3988/jcn.2020.16.2.215
27. Ferreira CL, Silva MA, Felício CM. Signs and symptoms of temporomandibular disorders in women and men. Codas. 2016;28(1):17-21. doi:10.1590/2317-1782/20162014218
28. Cowley A, Bradley D, Dubner R, et al. Cardiovascular and sleep-related consequences of temporomandibular disorders. Bethesda, MD: NHLBI workshop report; 2001.
29. Levy JH, Dong WK. Vibration perception thresholds of human vital and nonvital maxillary incisors. Arch Oral Biol. 2022;139:105426. doi:10.1016/j.archoralbio.2022.105426
30. Chen J, Lin S, Zeng Y. An update on obstructive sleep apnea for atherosclerosis: mechanism, diagnosis, and treatment. Front Cardiovasc Med. 2021;8. doi:10.3389/fcvm.2021.647071
31. Lin HC, Lai CC, Friedman M. Clinical prediction model for obstructive sleep apnea among adult patients with habitual snoring. Otolaryngol Head Neck Surg. 2019;161(1):178-185. doi:10.1177/0194599819839999
32. Liu Y, Lowe A. Factors related to the efficacy of an adjustable oral appliance for the treatment of obstructive sleep apnea. Chin J Dent Res. 2000;3:15-23.
33. Otsuka R, Almeida FR, Lowe AA. A comparison of responders and nonresponders to oral appliance therapy for the treatment of obstructive sleep apnea. Am J Orthod Dentofacial Orthop. 2006;129(2):222-229. doi:10.1016/j.ajodo.2004.06.035
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted February 22, 2025
Submitted in final revised form May 16, 2025
Accepted for publication June 13, 2025
Address correspondence to: Joseph Yousefian DMD, MS, MA. Email: joseph@dryousefian.com
DISCLOSURE STATEMENT
Joseph Yousefian is the inventor of the device.
This study did not receive any intramural or extramural financial support. No conflict of interest, off-label, or investigational use of any product or service is discussed in this article.
This article draws substantially on material from Chapter 18 of the book Pediatric Treatment of Sleep Apnea with Teledontics/Telegnathics, edited by Joseph Yousefian (ISBN 9780429263156), published in 2025 by CRC Press, Boca Raton and London. Permission to use this material has been granted in accordance with the terms of the editor contract, which allows the editor to reference and utilize content from the Work for the purposes of scholarly publication, teaching, and professional presentation, provided appropriate credit is given to the Publisher and the Work.
Yousefian J, ed. Pediatric Treatment of Sleep Apnea with Teledontics/Telegnathics. Boca Raton, FL: CRC Press; 2025.