Original Article 2, Issue 12.1
Knowledge and Awareness of Obstructive Sleep Apnea Among Dental Students
http://dx.doi.org/10.15331/jdsm.7368Melissa Hsu1, Anna Alessandri-Bonetti2, Melisa Alabsy1, John C. Mitchell3, Linda Sangalli1
1 College of Dental Medicine – Illinois, Midwestern University, Downers Grove, IL, USA; 2 Institute of Dental Clinic, A. Gemelli University Hospital IRCCS, Catholic University of Sacred Heart, Rome, Italy; 3 College of Dental Medicine – Arizona, Midwestern University, Glendale, AZ, USA
ABSTRACT
Objectives:
Obstructive sleep apnea (OSA) poses a significant global health burden but remains largely undertreated and underdiagnosed. Its screening relies on acquiring robust multidisciplinary knowledge and clinical application during training. However, its educational presence in predoctoral dental schools is limited. This cross-sectional study evaluated the knowledge of OSA among predoctoral dental students at various stages of education and their awareness of the dentist’s role in managing OSA. Two campuses of the same institution, offering different approaches of educational contents on OSA, were compared.
Methods:
A REDCapTM survey, consisting of the Obstructive Sleep Apnea Knowledge and Attitudes questionnaire, was distributed to all dental students from the two campuses (College of Dental Medicine—Arizona and College of Dental Medicine—Illinois) across all 4 years of dental school. Knowledge percentage and mean score were calculated based on number of correct answers and compared between the two campuses, sex, academic performance, and years of education with independent t-test, chi-square, and analysis of variance.
Results:
The survey was completed by 169 students. Average total knowledge score was 59.1% (10.6 ± 3.7). Third- and fourth-year students scored significantly higher than first- and second-year students. Participants from the campus with more OSA educational content achieved higher overall scores. Self-reported hours of education positively correlated with knowledge scores. As many as 87.0% of the participants were aware of the role of dental providers in managing OSA.
Conclusion:
This study highlighted a moderate knowledge of OSA among dental students. As increased hours of education was associated with greater knowledge in this field, it also emphasized the importance of integrating more educational content on OSA into the predoctoral curriculum.
Keywords:
obstructive sleep apnea, dental students, awareness, OSAKA questionnaire
Citation:
Hsu M, Alessandri-Bonetti A, Alabsy M, Mitchell JC, Sangalli L. Knowledge and awareness of obstructive sleep apnea among dental students. J Dent Sleep Med. 2025;12(1)
INTRODUCTION
Obstructive sleep apnea (OSA) is a widespread sleep-related breathing disorder characterized by recurrent upper airway obstruction, leading to complete cessation of breathing (apnea) or reduced airflow (hypopnea) for 10 seconds or longer.1 To meet the diagnostic criteria, these episodes need to occur five or more times per hour during sleep, to be accompanied by cortical arousals and a 3% to 4% drop in oxygen saturation.2,3 Untreated OSA is considered a systemic life-threatening disease, as repeated oxygen desaturation resulting from apneic events are associated with serious long-term cardiovascular and neurologic damage, and increased mortality.4 OSA poses a significant global health burden, affecting approximately 1 billion individuals worldwide, with projections indicating a rise in prevalence due to population aging and increasing obesity rates.4,5 Unfortunately, OSA is often underreported and undertreated, especially in women or individuals with a lower body mass index.6,7 Prospective studies have shown that clinically significant OSA remains undiagnosed in more than 80% of individuals.8 This underdiagnosis is partly attributed to the nonspecific symptomatology of the condition,9 as only 20% of patients report sleep-related symptoms to their primary care physicians.10 To increase awareness and detect potential disorders, all healthcare providers, including dentists, are recommended to routinely screen patients for OSA. However, studies have shown that many primary care physicians do not routinely screen for OSA,10 and fewer than 15% of dentists perform regular OSA screenings on every patient,11 possibly due to insufficient knowledge and limited training in this field.
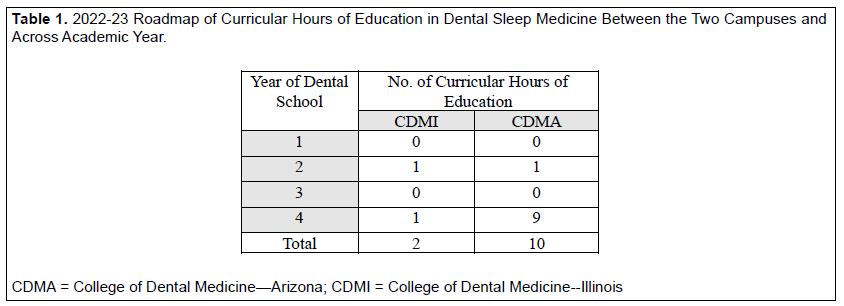
Dental sleep medicine (DSM) is an emerging discipline within dentistry that focuses on studying and managing sleep-related problems, including OSA, using oral appliances and upper airway surgery.12,13 Despite its growing importance over the past 2 decades, DSM has received limited attention in dental school curricula,14 with only approximately one-third of dentists receiving education about OSA during their predoctoral training.15-17 Moreover, many North American dental schools reportedly provide limited or no curriculum in DSM.18 Recently, there have been increasing calls that strongly advocate for inclusion of DSM into all predoctoral dental education.14,19-24 Even when the DSM curriculum is provided, due to the novelty and highly multidisciplinary field, there is significant variability across academic institutions in terms of extent and development of dedicated teaching in DSM.23,25-28 A 2003 survey distributed among 64 US dental schools revealed that among the 43 schools responding to the questionnaire (67% of response rate), 58% did not offer any teaching on the upper airway sleep disorders.29 Of the remaining 18 schools (42%) reportedly offering some teaching, only approximately 12 provided teaching at the predoctoral level with an average of only 2.5 hours (range,1 to 8 hours).29 Almost 10 years later, in 2012, the number of hours dedicated to sleep medicine remained approximately the same, at an average of 2.96 hours, ranging from 0 to 15 the hours.18 At the time of the study, the two campuses at Midwestern University also differed in hours of DSM teaching in the predoctoral curriculum across the 4 years. The Illinois campus provides 2 hours of teaching in the subject, whereas the Arizona campus delivers 10 hours, distributed as outlined in Table 1. However, this limited training may result in insufficient competency and knowledge among future dental providers at the expense of the general patient population.30 Several studies have revealed a relatively poor knowledge on OSA among dental interns31,32 and general dentists;16,17,33 however, very few studies have assessed OSA knowledge among dental students.17,34-36 Yet, understanding the extent of knowledge and awareness of OSA among dental students is crucial to identifying the current education gaps and generating curricular changes to ensure prompt recognition and management of OSA during their training.14
Therefore, given the significant global burden and increasing prevalence of OSA, the current limited dental educational content in DSM within the predoctoral dental schools, and the limited data on the assessment of knowledge of OSA among future dental providers, the aim of the current study was twofold. The primary aim was to assess knowledge regarding OSA of predoctoral dental students at various stages of education using a validated questionnaire. A secondary aim was to explore their awareness of the role dental providers should play in managing OSA. It was hypothesized that participants in higher years of education and schools with more extensive educational contents on OSA will demonstrate greater knowledge in this area.
By investigating the awareness of OSA among dental students, this study seeks to identify potential gaps in their baseline knowledge, which should guide educators in focusing on specific areas for improvement.37 Ultimately, this research aims to contribute to better training of future dental providers to recognize and manage OSA during their dental education.
METHODS
A cross-sectional study was conducted on all the dental students enrolled at Midwestern University across two campuses. The study was approved by the local Institutional Review Board (IRB) (Approval #23011, April 2023).
Study Population
To be invited to partake in the study, the participants had to (1) be enrolled in any of the 4 years (D1, D2, D3, or D4) of dental school at the two campuses (College of Dental Medicine—Illinois (CDMI) or College of Dental Medicine—Arizona (CDMA)); (2) understand English language; (3) possess an Internet connection; and (4) provide a response within 1 month from the first survey invitation.
Study Procedure
All eligible participants were invited to partake in the study through an initial email contact that described the content of the study and survey instrument. The survey was administered during the Spring quarter of 2023 using the web-based software platform REDCapTM, ensuring anonymity of the responses.38 A follow-up email was sent to all the participants after 2 weeks to encourage further participation. Participation in the study and response to individual survey items were entirely voluntary. As incentive for participating, respondents were given the opportunity to enter a raffle for a chance to win one of five $20 gift cards.
Study Instrument
The survey consisted of four sections that assessed demographics, educational content on OSA received during dental school, extent of individual knowledge about OSA, and awareness of the role of dental providers in managing OSA.
Section 1 - Demographics
Participants were asked to self-report their age (in years; categorized as younger than 18, 18 to 24, 25 to 34, and 35 or older), sex (female, male, nonbinary, prefer not to answer), year in training (D1, D2, D3, D4), campus attended (CDMA, CDMI), and current grade point average (GPA) (< 3.0, 3.0-3.5, >3.5, and prefer not to answer).
Section 2 - Educational content on OSA
The extent of educational content in OSA received so far in dental school was ascertained by asking the participants to recall whether they received any teaching on OSA (yes/no).
Section 3 - Extent of knowledge about OSA
An initial question on awareness of OSA was formulated as “Have you ever heard of OSA before?”, which allowed a yes/no answer. Next, the knowledge of OSA was assessed through the use of the Obstructive Sleep Apnea Knowledge and Attitudes (OSAKA) questionnaire, a validated tool consistently used to establish baseline familiarity of OSA among physicians.39 The OSAKA questionnaire consists of 18 true-false statements about OSA, assessing epidemiology, pathophysiology, symptoms, diagnosis, and treatment.39 To increase the accuracy of the responses and decrease the risk of bias derived from guess, “I do not know” was included as a possible answer and scored as an incorrect response. A mean knowledge score was calculated as the sum of all correct answers (from 0 to 18); a percentage knowledge score was computed as percentage of correct answers out of a total of 18 questions (from 0 to 100%). Higher mean values and percentage were deemed as a greater knowledge of the participant.
In comparison with the original OSAKA questionnaire, the additional questions assessing the confidence of the participants to identify and treat patients with OSA were omitted from the current study, as dental students at our institution do not assess nor treat patients with this condition.
Section 4 - Awareness of the role of dental providers in managing OSA
Awareness of the role of dental providers in managing OSA was assessed with an ad-hoc question (“Are you aware that dentists can play a major role in the management of OSA?”), with a dichotomous (yes/no) answer.
Statistical Analysis
Data responses were investigated for missing values and removed from the analysis on a pairwise basis. The Shapiro-Wilk test was used to assess normality of distribution of the data, and the Leven test was used to verify assumption of homogeneity of variances. Because no violation of skewness was found, data were analyzed with parametric tests. Descriptive statistics were used to summarize demographics, extent of educational content and knowledge of OSA, and awareness of the role of the dentist in terms of means, standard deviations, and frequency distribution.
To test the primary aim, the mean knowledge score was computed for each participant by summing all the correct answers. This was achieved by assigning a value of 1 in case of correct answer, and a value of 0 in case of incorrect or “I do not know” answer. The knowledge score was then expressed as a percentage (percentage knowledge score). Next, mean and percentage knowledge scores were compared between the two campuses (CDMI and CDMA) with the independent t-test. Because women and men were the only two options selected for sex, the mean knowledge score was compared between those two categories with the independent t-test. One-way analysis of variance (ANOVA) was used to investigate the difference in mean knowledge scores across years of education and academic performance. Statistically significant ANOVAs were further explored with the Bonferroni post-hoc test (α = 0.05). The Pearson correlation coefficient was used to test the relationship between total knowledge score and self-reported amount of educational content.
To test the secondary aim, the awareness of the role of the dentist was transformed into a dichotomous variable, by assigning a value of 1 when the participant indicated they were aware, and a value of 0 when the participant indicated not to be aware. The chi-square test was used to compare the results across campuses, years of education, and academic performance.
All data analyses were conducted using IBM SPSS v27 (IBM SPSS Statistics Macintosh, Version 27.000, IBM Corp, Armonk, NY). For all analyses, a two-tailed value of P < 0.05 was considered significant.
RESULTS
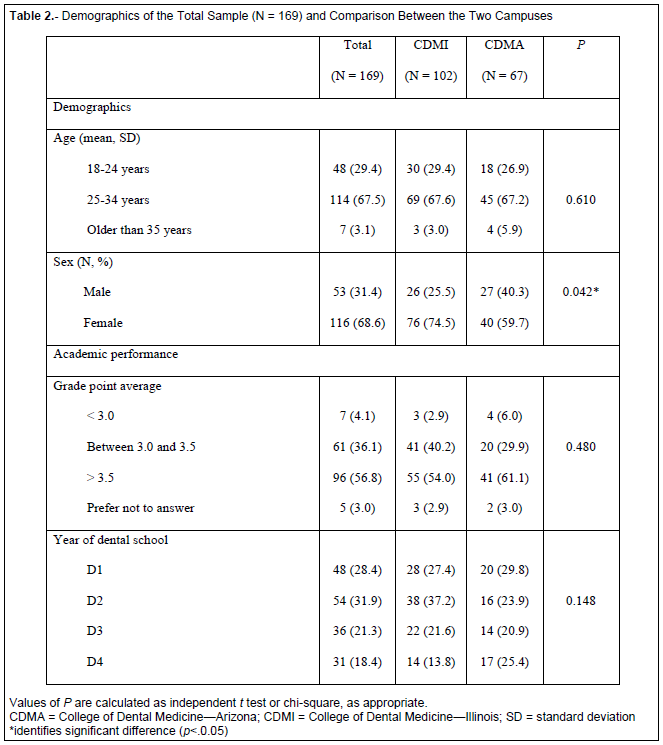
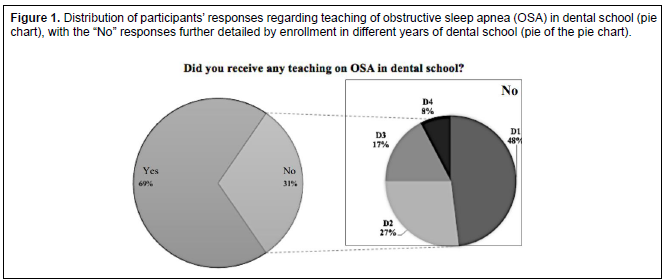
Of 1,110 students enrolled at CDMI and CDMA campuses of Midwestern University, a total of 171 completed the survey (15%). Two of them were removed from the analysis for missing data, which resulted in a total of 169 participants (68.6% females). Demographics of the total sample are reported in Table 2. A total of 30.8% (N=52) of the participants reported to not recall having received any teaching in OSA (Figure 1). Of these, 52.1% were enrolled in D1 year and 25.9% were enrolled in D2 year. Most of them (90.4%, N=47) belonged to the CDMI campus.
Aim 1: Extent of knowledge of OSA
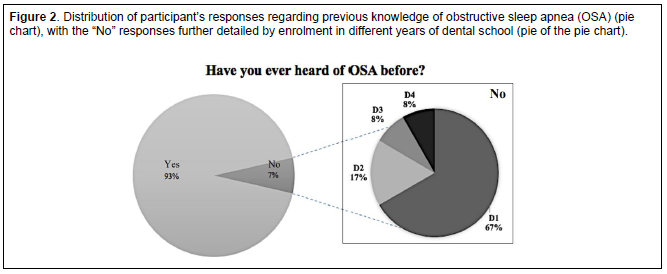
A total of 7.1% (N=12) of the participants indicated to have never heard about OSA before. Of these, 66.7% were enrolled in the D1 year and 16.7% were enrolled in the D2 year (Figure 2). Most of those (75.0%, N=9) belonged to the CDMI campus.
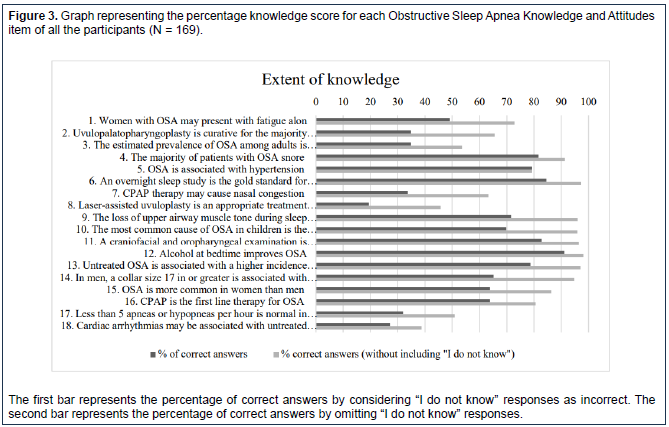
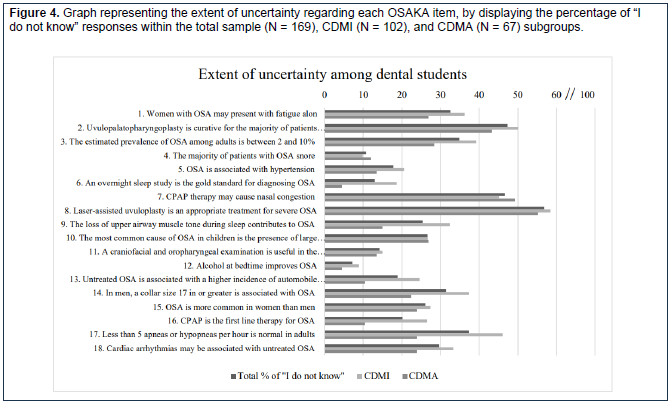
Only one participant (0.6%) achieved 100% of correct answers on the OSAKA questionnaire, whereas two participants (1.2%) did not answer any of the questions correctly. Most of the responders (11.8%) answered 14 questions correctly. The item that was most commonly answered correctly (by 91.1%) was denying that “Alcohol at bedtime improves OSA” (Figure 3). This was followed by agreeing that “A craniofacial and oropharyngeal examination is useful in the assessment of patients of large tonsils and adenoids” (correctly answered by 82.8%), and that “An overnight sleep study is the gold standard for diagnosing OSA” (by 84.6%). Conversely, the item that was most commonly missed referred to laser-assisted uvuloplasty as an appropriate treatment for severe OSA (by 19.5%). This same item was also the one that displayed the greatest percentage of uncertainty (in 56.8% of participants) (Figure 4).
The mean knowledge score for the total sample was 10.6±3.7, which corresponded to a percentage knowledge score of 59.1% (Table 3). As expected, the participants enrolled in the D3 and D4 years of dental school scored significantly better than those enrolled in the D1 and D2 years, despite a lack of statistically significant difference in self-reported GPA across the four years. Specifically, dental students enrolled in the D4 year provided statistically significantly more correct answers compared to those enrolled in the D1 (68.5% vs 52.3%, by 2.9±0.8 answers, P=0.003, 95% confidence interval (CI) 0.71, 5.10) and in D2 years (68.5% vs 56.5%, by 2.2±0.8 answers, P=0.049, 95% CI 0.01, 4.31). Similarly, those enrolled in the D3 year scored significantly better than those enrolled in the D1 year (64.0% vs 52.3%, by 2.1±0.8 answers, P=0.049, 95% CI 0.01, 4.22). This was consistently found on both campuses (data not shown).
Participants enrolled at CDMA scored significantly better than those enrolled at CDMI, with 65% of correct answers compared to 55% (mean value 11.7±2.9 vs 9.9±4.0, t(167)=3.414, P=0.001, 95% CI 0.763, 2.856)(Table 4). However, when further examined by year of education, only the D1 dental students at CDMA scored significantly higher than the D1 students at CDMI by 2.6±1.0 (10.9±2.5 vs 8.3±4.0, t(46)= 2.575, P=0.013, 95% CI 0.574, 4.683). The correct responses provided by the participants in the remaining years did not differ between the two campuses. Neither self-reported GPA (F(165)=0.986, P=0.401) or sex (t(167)=-0.542, P=0.589, 95% CI -1.549, 0.882) influenced the number of correct answers provided by the participants.
Aim 2: Awareness of the role of dentists in OSA
A total of N=147 (87.0%) of the responders indicated awareness that the dental providers can play a major role in managing OSA. Those that were not aware (13%, N=22) belonged to the CDMI campus, and most of them (36%, N=8) were D1 students. The awareness of the role of the dentist was not related to the GPA of the responders (P=0.806).
Table 1. 2022-23 Roadmap of Curricular Hours of Education in Dental Sleep Medicine Between the Two Campuses and Across Academic Year. |
{kind=link}
Table 2. Demographics of the Total Sample (N = 169) and Comparison Between the Two Campuses |
{kind=link}
Table 3. Answers (“True”, “False”, “I do not know”, %) provided by participants to each Obstructive Sleep Apnea Knowledge and Attitudes (OSAKA) item |
Table 4. Number (%) of correct answers provided by participants to each Obstructive Sleep Apnea Knowledge and Attitudes (OSAKA) item. |
{kind=link}
{kind=link}
Figure 3. Graph representing the percentage knowledge score for each Obstructive Sleep Apnea Knowledge and Attitudes item of all the participants (N = 169). |
{kind=link}
{kind=link}
DISCUSSION
The current study aimed at assessing knowledge of OSA among dental students and their awareness of the role of dentists in managing this condition. The findings revealed that, on average, dental students provided approximately 60% of correct answers. Students enrolled in higher years of education or schools with more comprehensive OSA educational content scored significantly higher in their knowledge of OSA.
Extent of knowledge of OSA among dental students
To evaluate the students’ knowledge, the OSAKA questionnaire was selected;39 it is a validated tool commonly used in the literature to assess knowledge on OSA.33,36,37,40-43 To increase the comparability of our results across other published reports, the knowledge score was expressed both as a mean value and as a percentage. Our study revealed a mean knowledge score of 10.6±3.7 across all participants, ranging from 9.4±3.7 for first-year dental students to 12.3±3.7 for fourth-year students. The mean knowledge score obtained in the current study was slightly higher than that of similar studies that used the OSAKA questionnaire. For instance, a study among fifth-year Iranian dental students reported a mean score of 8.4±3.6, which is even lower than our D1 students’ score.34 However, the authors of this study clarified that there is no specific training on OSA in the predoctoral dental curricula in their country.34 Similarly, other studies reported a lower overall percentage of correct answers compared to our results (59%), such as one study conducted among dental students in Malaysia, which reported 44.4% correct answers.36 The item that was most often correctly answered in the current study referred to “Alcohol at bedtime improves OSA”. This is not consistent with other studies that revealed higher correct scores for “The loss of upper airway muscle tone during sleep contributes to OSA”34 or for “The majority of patients with OSA snore”.36
Conversely, the item that was most commonly missed and that achieved the highest level of uncertainty was “Laser-assisted uvuloplasty is an appropriate treatment for severe OSA”. This observation can be attributed to the lack of discussion on laser-assisted uvuloplasty in the DSM syllabi of either campus. This was also supported by Selvaraj et al;36 however, other authors found that the lowest knowledge score referred to the question “OSA is more common in women than men”.34
Similar to existing reports, the current study showed no difference in knowledge between males and females.34,39 Other studies in the literature used different questionnaires,35 such as the Assessment of Sleep Knowledge in Medical Education (ASKME)44 or nonvalidated questionnaires,17 which makes a direct comparison challenging.
Of note, students at higher years of education and at the campus where more extensive educational content was provided achieved better scores overall. Although CDMI offers a total of 2 hours of DSM instruction spread across the second and fourth years, CDMA provides a more extensive 10-hour curriculum, with 1 hour in the second year and 9 hours in the fourth year. Interestingly, despite this significant variation in instructional hours, fourth-year students at CDMA, who have received more extensive education, achieved only a slightly higher score compared to their counterparts at CDMI. This suggests that the quantity of instruction alone may not be the sole determinant of students’ performance. The main significant difference between the two campuses lies in the performance of first-year students, who have received no formal DSM instruction at either campus. This indicates the potential effect of early exposure and education in DSM on students’ knowledge and understanding, which warrants further investigation and consideration in dental education curriculum planning. Notably, the Commission on Dental Accreditation (CODA) does not specifically require dental education programs to include instruction and treatment of sleep disorders. Therefore, the decision to include teaching of DSM is left to the discretion of the institution and the faculty. There might be a need to revise and update CODA standards for predoctoral dental schools to incorporate standardized recommendations into the curriculum, ensuring future providers are sufficiently prepared to address the rising prevalence of sleep disorders in the general population. In addition to introducing national requirements for DSM teaching for faculty with sleep training or board certification (e.g. from the American Academy of Sleep Medicine or American Academy of Dental Sleep Medicine), dental schools should also implement brief and cost-effective screening tools (i.e., STOP-Bang questionnaire) during screening intake to improve identification of patients at high risk of sleep disorders and facilitate referrals to sleep specialists. Yet, both faculty and students need to be properly calibrated on the tool’s utilization and incorporation into clinical practice, as studies have shown an insufficient rate of patient referrals despite high-risk scores on the STOP-Bang questionnaire within dental school settings.45 Moreover, the incorporation of clinical experience/rotations in specialized sleep centers into the predoctoral curricula could improve the translational applicability of formal instruction in everyday practice.
Awareness of the role of dental provider
Given the increasing prevalence of OSA worldwide, it is crucial for healthcare providers to suspect, identify, and provide proper treatment for patients with OSA. Although the ultimate diagnosis is made by sleep physicians based on polysomnography results,46 dentists play a crucial role in several other steps for OSA management,47 such as screening patients for risk factors and OSA-related symptoms19,46 with validated screening questionnaires (e.g., STOP-Bang,48 Berlin Questionnaire,49 and Wisconsin Sleep Questionnarie,50 among others). Additionally, dental professionals are essential in referring patients to the appropriate healthcare professionals. Moreover, as further supported by a policy statement released by the American Dental Association, the trained dentist is the only healthcare professional able to provide a mandibular advancement device for managing OSA.19,51 Indeed, although positive airway pressure is still considered the gold standard, mandibular advancement device therapy is recognized as a recommended treatment option for mild-moderate cases and all patients with OSA who are intolerant to positive airway pressure therapy.47
In the current study, awareness of the role of the dental professional in OSA management was assessed with an ad-hoc question. Surprisingly, although most of the dental students responded that they were aware of the dentist’s role in OSA management, 13% of them indicated that they were unaware of this role, and this lack of awareness was not limited to first-year students. Moreover, academic performance did not seem to influence this lack of awareness. This suggests that insufficient educational content or lack of clinical applicability to routine patient management may be contributing to this concerning finding. Although this could be expected for first-year students, it is less clear why some higher-year students, who had already received dedicated lectures on the topic, still lacked awareness of the dental provider’s role in OSA management.
Strengths and limitations
This study has several strengths, including a good sample size and assessment of knowledge among dental students at two different campuses, both with similar sociodemographic characteristics (representation of minorities and private institutions) but differing in the extent of educational content on OSA. Moreover, including the option of “I do not know” as a possible answer improved data accuracy by reducing guesswork. It also provided valuable information on the level of uncertainty regarding specific questions, which could guide a faculty in tailoring their didactic sessions accordingly.
Several limitations also need to be acknowledged. The low response rate may limit the generalizability of the study’s findings to the entire student population of the two universities. The possibility of participation bias, with only those interested in DSM opting to participate, also needs to be considered. Because the survey was distributed through email and administered in an unsupervised setting, it is possible that participants accessed external sources, such as the internet, to provide correct answers. However, if this occurred, it could have led to an overestimation, rather than underestimation, of the knowledge of the dental students. Finally, findings of this study are specific to our institution based on the current curricular content. As highlighted in previous sections and supported by our results, the extent of knowledge is dependent on the number of educational hours dedicated to the topic. Therefore, the results encourage additional training in DSM during predoctoral dental curricula.
CONCLUSION
The results of this study demonstrated that, on average, dental students provided approximately 60% of correct answers, indicating a moderate level of knowledge in this area. Importantly, students enrolled in higher years of education or in schools with more extensive educational content exhibited significantly greater knowledge of OSA, emphasizing the positive effect of dedicated content on this subject.
Studies performed within dental schools are fundamental to assessing the extent of knowledge and awareness of dental students, identifying specific gaps, and implementing the corresponding educational contents accordingly. By doing so, dental schools can better equip future dental providers with the necessary knowledge and skills to identify, manage, and collaborate effectively in the treatment of patients with OSA.
REFERENCES
- Berry RB, Budhiraja R, Gottlieb DJ, et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2012;8:597-619.
- Garvey JF, Pengo MF, Drakatos P, Kent BD. Epidemiological aspects of obstructive sleep apnea. J Thorac Dis. 2015;7(5):920-929.
- Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. Sleep 1999;22:667e689.
- Benjafield AV, Ayas NT, Eastwook PR, Heinzer R, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir Med. 2019;7(8):697-698.
- Lyons MM, Bhatt NY, Pack AI, Magalang UJ. Global burden of sleep-disordered breathing and its implications. Respirol. 2020;25(7):690-702.
- Motamedi KK, McClary AC, Amedee RG. Obstructive sleep apnea: a growing problem. Oschler J. 2009;9(3):149-153.
- Kapur V, Strohl KP, Redline S, Iber C, et al. Underdiagnosis of sleep apnea syndrome in U.S. communities. Sleep Breath. 2002;6(2):49-54.
- Saager L, Safer-Zadeh E, Bottros M, Selvidge JA, et al. Prevalence of undiagnosed obstructive sleep apnea among adult surgical patients in an academic medical center. Sleep Med. 2009;10(7):753-8.
- Sangalli L, Yanez-Regonesi F, Fernandez-Vial D, Moreno-Hay I. Self-reported improvement in obstructive sleep apnea symptoms compared to treatment response with mandibular advancement device therapy: a retrospective study. Sleep Breath. 2023;27(4):1577-1588
- US Preventive Services Task Force, Mangione CM, Barry MJ, Nicholson WK, et al. Screening for obstructive sleep apnea in adults: US Preventive Services Task Force Recommendation Statement. JAMA. 2022;328(19):1945-1950.
- Chiang HK, Long A, Carrico CK, Robinson R. The prevalence of general dentists who screen for obstructive sleep apnea. J Dent Sleep Med. 2018;5:55-60.
- Aarab G, Lobbzoo F. Dental sleep medicine redefined. Sleep Breath. 2018;22:1233.
- Lobbezoo F, de Vries N, de Lange J, Aarab G. A further introduction to dental sleep medicine. Nat Sci Sleep. 2020;12:1173-1179.
- Lobbezoo F, Aarab G. Dental sleep medicine in the dental curriculum: What should be the dot on the horizon? Sleep Breath. 2021;25:1171-1172.
- Bian H. Knowledge, opinions, and clinical experience of general practice dentists toward obstructive sleep apnea and oral appliances. Sleep Breath. 2004;8(2):85-90.
- Jokubauskas L, PileičikienÄ G, ?ekonis G, BaltrušaitytÄ A. Lithuanian dentists' knowledge, attitudes, and clinical practices regarding obstructive sleep apnea: A nationwide cross-sectional study. Cranio. 2019;37(4):238-245.
- Swapna LA, Alotaibi NF, Falatah SA, Joaithen MSA, Koppolu P. Knowledge of obstructive sleep apnea among dental fraternity in Riyadh. Open Access Maced J Med Sci. 2019;7(15):2508-2512.
- Simmons MS, Pullinger A. Education in sleep disorders in US dental schools DDS programs. Sleep Breath. 2012;16(2):383-392.
- Herrero Babiloni A, Beetz G, Dal Fabbro C, et al. Dental sleep medicine: Time to incorporate sleep apnoea education in the dental curriculum. Eur J Dent Educ. 2020;24(3):605-610.
- Guneri P, İlhan B, Çal E, Epstein JB, Klasser GD. Obstructive sleep apnoea and the need for its introduction into dental curricula. Eur J Dent Educ. 2017;21(2):121-129.
- Ivanoff CS, Hottel TL, Pancratz F. Is there a place for teaching obstructive sleep apnea and snoring in the predoctoral dental curriculum? J Dent Educ. 2012;76(12):1639-1645.
- Lobbezoo F, Lavigne GJ, Kato T, de Almedia FR, Aarab G. The face of Dental Sleep Medicine in the 21st century. J Oral Rehabil. 2020;47(12):1579-1589.
- Balasubramaniam R, Pullinger A, Simmons M. Sleep medicine education at dental schools in Australia and New Zealand. J Dent Sleep Med. 2014;1:9-16.
- Lobbezoo F, Aarab G, Wetselaar P, Hoekema A, de Lange J, de Vries N. A new definition of dental sleep medicine. J Oral Rehabil. 2016;43(10):786-790.
- Chervin RD, Chesson AL Jr, Benca RM, et al. Organization and structure for sleep medicine programs at academic institutions: Part 1--current challenges. Sleep 2013;36:795-801.
- Tsuda H, Ohmary T, Higuchi Y. Requirement for sleep medicine education in Japanese pre-doctoral dental curriculum. Sleep Biol Rhythms. 2014;12:232-234.
- Karimi N, Mehta N, Pagni SE, Antonellou E, Doherty E, Correa LP. The current state of dental sleep medicine practice in academic institutions: A questionnaire-based study. J Dent Sleep Med. 2019;6(4).
- Moreno-Hay I, Ivonne Hernandez, Mulet M, et al. Sleep medicine education in US and Canadian orofacial pain residency programs: Survey outcomes. J Am Dent Assoc. 2020;151:962-968.
- Ivanhoe JR, Frazier KB, Parr GR, Haywood VB. The teaching and treatment of upper airway sleep disorders in North American dental schools. J Prosthet Dent. 2003;89:292-296.
- Alrejaye NS, Alfayez KM, Al Ali HH, et al. Awareness and attitude of physicians on the role of dentists in the management of obstructive sleep apnea. Int J Environ Res Public Health. 2022;19:16126.
- Alansari RA, Kaki A. Knowledge of signs, symptoms, risk factors, and complications of obstructive sleep apnea among dental interns. J Contemp Dent Pract. 2020;21:558-561.
- Alkhader M, Saadeh R. The knowledge of sleep medicine among dental interns in Northern Jordan. Eur J Dent. 2021;15:193-196.
- Alzahrani MM, Alghamdi AA, Alghamdi SA, Alotaibi RK. Knowledge and attitude of dentists towards obstructive sleep apnea. Int Dent J. 2022;72(3):315-321.
- Shafiee S, Sofi-Mahmudi A, Behnaz M, Safiaghdam H, Sadir S. Iranian dental students and specialists’ knowledge and attitude about obstructive sleep apnea. MedRxiv. 2020. doi: 10.1101/2020.08.07.20170605.
- Talaat W, AlRozzi B, Al Kawas S. Sleep medicine education and knowledge among undergraduate dental students in Middle East universities. CRANIO. 2016;34:163-168.
- Selvaraj S, Eusufzai SZ, Asif JA, Bin Jamayet N, Ahmad WMAW, Alam MK. Comparison of knowledge level and attitude towards obstructive sleep apnoea amongst dental and medical undergraduate students of Universiti Sains Malaysia. Work. 2021;69(1):173-180.
- Cherrez-Ojeda I, Calderon JC, Garcia AF, et al. Obstructive sleep apnea knowledge and attitudes among recent medical graduates training in Ecuador. Multidiscip Respir Med. 2018;13(5).
- Harris PA, Taylor R, Thielke R, Payne J, Gonzales N, Conde JG. Research electronic data capture (REDCap) – A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377-381.
- Schotland HM, Jeffe DB. Development of the obstructive sleep apnea knowledge and attitudes (OSAKA) questionnaire. Sleep Med. 2003;4:443-450.
- Ozoh OB, Iwuala SO, Desalu OO, Ojo OO, Okubadejo NU. An assessment of the knowledge and attitudes of graduating medical students in Lagos, Nigeria, regarding obstructive sleep apnea. Ann Am Thorac Soc. 2015;12(9):1358-1363.
- Ozoh OB, Ojo OO, Iwuala SO, Akinkugbe AO, Desalu OO, Okubadejo NU. Is the knowledge and attitude of physicians in Nigeria adequate for the diagnosis and management of obstructive sleep apnea? Sleep Breath. 2017;21(2):521-527.
- Zaidi GA, Rehman ST, Shafiq MM, Zehra T, Israar M, Hussain SM. Knowledge of obstructive sleep apnoea in final year medical students and junior doctors-a multi-centre cross-sectional study. Clin Respir J. 2021;15(3):345-350.
- Cherrez Ojeda I, Jeffe DB, Guerrero T, et al. Attitudes and knowledge about obstructive sleep apnea among Latin American primary care physicians. Sleep Med. 2013;14(10):973-977.
- Zozula R, Bodow M, Yatcilla D, Cody R, Rosen RC. Development of a brief, self-administered instrument for assessing sleep knowledge in medical education: ‘‘The ASKME Survey’’. Sleep 2001;24:227-233.
- Guess NW, Fischbach H, Ni AA, Firestone AR. Referral rate for obstructive sleep apnea in a pre-doctoral dental clinic using the STOP-Bang Questionnaire. J Dent Educ 2022;86:456-462.
- Levine M, Bennett K, Cantwell M, Postol K, Schwartz D. Dental sleep medicine standards for screening, treating, and managing adults with sleep-related breathing disorders. J Dent Sleep Med. 2018;5:61-68.
- Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: An update for 2015. J Clin Sleep Med. 2015;11(7):773-827.
- Pagappa M, Liao P, Wong J, et al. Validation of the STOP-Bang Questionnaire as a screening tool for obstructive sleep apnea among different populations: A systematic review and meta-analysis. PLoS One. 2015;10(12):e0143697.
- Netzer NC?, Stoohs RA, Netzer CM?, Clark K, Strohl KP. Using the Berlin Questionnaire to identify patients at risk for the sleep apnea syndrome. ?Ann Intern Med. 1999;131:485-491.
- Young T?, Palta M, Dempsey J?, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. ?N Engl J Med. 1993;328:1230-1235.
- Sangalli L, Yanez-Regonesi F, Fernandez-Vial D, Martinez-Porras A, Moreno-Hay I. Comparison of three mandibular advancement device designs in the management of obstructive sleep apnea: A retrospective study. J Dent Sleep Med. 2021;9(3).
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted November 29, 2023
Submitted in final revised form July 12, 2024
Accepted for publication September 18, 2024
Address correspondence to: Linda Sangalli, College of Dental Medicine – Illinois, Midwestern University, 555 31st Street, Downers Grove, IL, 60515. Email: lsanga@midwestern.edu