Original Article 2, Issue 11.4
Comparing Anterior Protrusive and Speech-Positioned Mandibular Positioning Techniques for Adult Dental Sleep Appliances: A Pilot Crossover Randomized Controlled Trial
http://dx.doi.org/10.15331/jdsm.7358Enoch T. Ng DDS1; Manuel O. Lagravère DDS, MSc, PhD1; Carlos Flores-Mir MSc, PhD1; Ivonne A. Hernandez MSc1; Pedro Mayoral MSc, PhD2; Arnaldo Perez-Garcia MSc, PhD1
1School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada
2University Católica de Murcia UCAM, Faculty of Medicine and Dentistry, School of Dentistry, Madrid, Spain
ABSTRACT
Objective:
This study aimed to determine the feasibility and potential efficacy of the speech positioning technique (SPT) versus the anterior protrusive technique (APT) in oral appliance therapy (OAT) in a crossover randomized controlled trial (RCT).Methods:
A pilot trial was conducted with participants randomized to complete OAT with either the SPT or APT before a washout period, then crossover assignment to complete OAT with the alternative mandibular positioning technique. Feasibility data were collected via administrative tracking and patients’ and clinicians’ feedback. Efficacy data were collected through home sleep testing, measurements of mandibular position using dental landmarks, reported occurrence of adverse effects, differences in sleep quality, and patient experience measured through validated questionnaires.Results:
Eight patients completed participation in this pilot trial. The recruitment rate was 23.91% and the attrition rate was 27.27%. One patient was a nonresponder to OAT with both techniques, one was a responder to the SPT but not the APT, and one was a responder to the APT but not the SPT. Average mandibular protrusion for the SPT was 48.82% and 63.37% for the APT. Adverse effects were reported by several patients using OAT with the positioning techniques. No significant differences in sleep quality and patient experience were reported between the APT and SPT.Conclusion:
Conducting a crossover RCT comparing the SPT and the APT is feasible. Pilot trial data suggest the SPT may provide an alternative therapeutic position to the APT for mandibular positioning in OAT. A properly sampled RCT is necessary to further assess the observed efficacy of the SPT in mandibular target position.Clinical Implications:
The use of the SPT to determine mandibular position in OAT for patients with obstructive sleep apnea may provide patients with an alternative target mandibular position for therapeutic benefit with less mandibular protrusion and decreased risk of adverse effects.Keywords:
Oral appliance therapy, obstructive sleep apnea, dental sleep medicineINTRODUCTION
Obstructive sleep apnea (OSA) is a medical condition defined by upper airway obstruction during sleep, resulting in oxygen desaturation and cortical arousal disruption to normal sleep architecture.1-3 It is estimated that more than 15% of the global population has OSA.4 Direct, indirect, and healthcare-related costs exceed $150 billion annually in the United States alone.5,6 OSA is associated with multiple medical conditions, including cardiovascular disease, cerebrovascular disease, obesity, renal diseases, psychiatric disorders, type 2 diabetes, asthma, chronic obstructive pulmonary disease, and cancer.7-11 Specific to males, OSA is well correlated with an increased risk for erectile dysfunction and an increased risk for all-cause mortality, especially within the middle age range of 40 to 65 years.12-18The primary treatments for adult OSA are positive airway pressure (PAP) therapy and oral appliance therapy (OAT).19,20 PAP therapy consists of a machine delivering positive air pressure from a mask connected to the machine through a hose to maintain upper airway patency by creating a pneumatic splint within the upper airway through the entire respiratory cycle.21-24 OAT devices consist of custom-fit upper and lower dental appliances that can be adjusted to each other and that anchor off the patient’s teeth.19,25 Many variations of OAT exist with differences primarily in material, manufacture, device design, and adjustment methods. Although both treatments have similar effectiveness, greater adherence has been observed in patients treated with OAT.26
OAT involves the fabrication, delivery, adjustment, and regular patient follow-up for a custom-fit adjustable dental appliance designed to hold the mandible in a specific position to the maxillary complex to improve and maintain a patient’s airway patency.19,25 Appliances are generally anchored to teeth on both the maxilla and mandible, with adjustments to mandibular position available through different coupling mechanisms. Adjustments are primarily made to improve patient airway patency with the goal of reaching a therapeutic position, a mandibular position where OSA is fully managed for the individual patient.27-34 The predominant mandibular positioning and titration method in OAT is through the anterior protrusive technique (APT). The mandible is placed in a protrusive position relative to its maximum anterior and posterior positional range, with initial mandibular position traditionally beginning as between 50% to 75% of maximum mandibular protrusion.35-39 If necessary, titration adjustments are done to protrude the mandible further. Recent research, however, has shown that this degree of mandibular protrusion may not be necessary and as little as 25% protrusion may be sufficient for select patients.40,41 Although the parameters for use of the APT have been well studied and well documented for adult OAT, common adverse effects include temporomandibular dysfunction, muscle pain, and occlusal changes.19,42-47 The risk for and occurrence of these adverse effects can significantly affect patient experience, quality of life, and treatment adherence.48-51 Exploring and testing alternative mandibular positioning techniques for OAT is necessary to explore the potential for alternative therapeutic positions, improve position accuracy, reduce adverse effects, and enhance patient adherence.
Since the 1970s, dentistry has used phonetics to obtain and verify a muscularly stable and reproducible mandibular position.52 This technique is known as the sibilant phoneme or speech positioning technique (SPT). In denture prosthodontics, the SPT is used to identify and verify the phonetic neutral zone, a zone in which the placement of denture teeth allows for oropharyngeal muscular stability and, thereby, denture retention and functional stability.53-55 More recently, the SPT has been advocated as an alternative technique for mandibular positioning compared to the anterior protrusive technique, which predominates within OAT.56-58 Previous research supports the potential effectiveness of holding this mandibular position to achieve muscular stability in denture retention obtained through the SPT, which translates to oropharyngeal muscular stability in OAT during sleep.56,57 However, until recently, significant variations existed between experts and their opinions on appropriately adapting the SPT for use in OAT. A recent article has described a consensus-based process for using the SPT in dental sleep medicine, including in OAT.59
The purpose of this study is twofold: to explore the feasibility of a full-scale crossover randomized controlled trial (RCT) comparing the APT and the SPT, and to gather preliminary data on the efficacy of the SPT as an alternative mandibular positioning technique to the APT in adult OAT in a clinical setting. Assessing feasibility would be instrumental in determining the logistical details for running an RCT. Gathering preliminary efficacy data will aid in assessing the need to further demonstrate the efficacy of the SPT through a more robust research design.
MATERIALS AND METHODS
Study Design
A pilot trial design was selected to assess the feasibility of a crossover RCT and to generate preliminary efficacy data for the SPT. This design is useful for assessing the feasibility of a planned RCT and the potential efficacy of the exposure of interest by conducting the future study, or part of it, on a smaller scale.60 Factors of interest in pilot studies can include patient recruitment data, patient attrition rate, patient response to specific measurements or data collection processes (such as surveys and questionnaires), and additional data points of interest that can be measured in an RCT.61,62 Alberta Research Information Services: Human Research Ethics Board approved the study (Pro00097563).Patient Recruitment Criteria
Patients were eligible for the pilot trial if they had been diagnosed with moderate or severe OSA by a sleep physician and they qualified as a candidate for OAT based on the American Academy of Sleep Medicine (AASM) and American Academy of Dental Sleep Medicine (AADSM) treatment guidelines. All patients were screened for OSA and tested with level 3 ambulatory polysomnography (Medibyte Home Sleep Test, Braebon Medical Corp.). Sleep tests were sent to a sleep specialist physician for formal interpretation and diagnosis. Participants were recruited from a single private practice dental clinic in Edmonton. Patients with active temporomandibular degenerative joint disease, known craniofacial, syndromic, or neuromuscular disorders, or uncontrolled/untreated comorbid conditions such as cardiovascular, cerebrovascular, metabolic, and renal diseases were excluded from the pilot trial. Because of technical factors such as the minimum space necessary to fit an intraoral scanner head for digital impressions, patients with a maximum mandibular opening of less than 20 mm were also excluded from participating in the pilot trial. A sample size of N=8 was estimated based on previously published dental sleep medicine pilot studies of similar interventional style.63,64Research Protocol
This protocol applies to both the pilot trial and the planned crossover RCT, as the pilot trial replicates the actual trial on a smaller scale. Following AASM and AADSM treatment guidelines, patients were given custom-fit titratable dental sleep appliances. For the study, the definition of successful treatment for OSA was an apnea-hypopnea index (AHI) reduction of at least 50% and fewer than 10 events per hour. All appliances were of the same make and model type, manufactured by the same laboratory, and patients were blind to which appliance treatment (anterior protrusive or speech positioning technique) they received.Participants were assigned to either the SPT-first or APT-first group based on computer-generated randomization for an equal distribution of eight patients between the two groups. Allocation concealment was achieved with enrolled participants assigned to their group before the treating clinician was made aware of which appliance should be provided to the patient. Dropout replacements were enrolled after all original eight randomizations were assigned.
All appliances were printed nylon-based bilateral traction appliances fabricated by Diamond Orthotic Laboratory. Appliances were titratable in 1-mm increments both for anterior and vertical adjustments. All patients started at the same overjet position based on the initial overjet obtained from the SPT occlusal registration. This was to provide a personalized initial mandibular protrusion percentage for each patient, similar to the protrusion percentage for the patient in SPT, rather than a set percentage equivalent across all patients. This would then allow for a more accurate intrapatient comparison of mandibular protrusion percentages between the two techniques. Vertical opening for APT appliances was set at 5 mm based on the 5-mm George Gauge bite fork used for APT occlusal registration. The vertical opening for SPT appliances was determined to be 4.5 mm based on the minimum material thickness necessary for nylon-printed appliances.
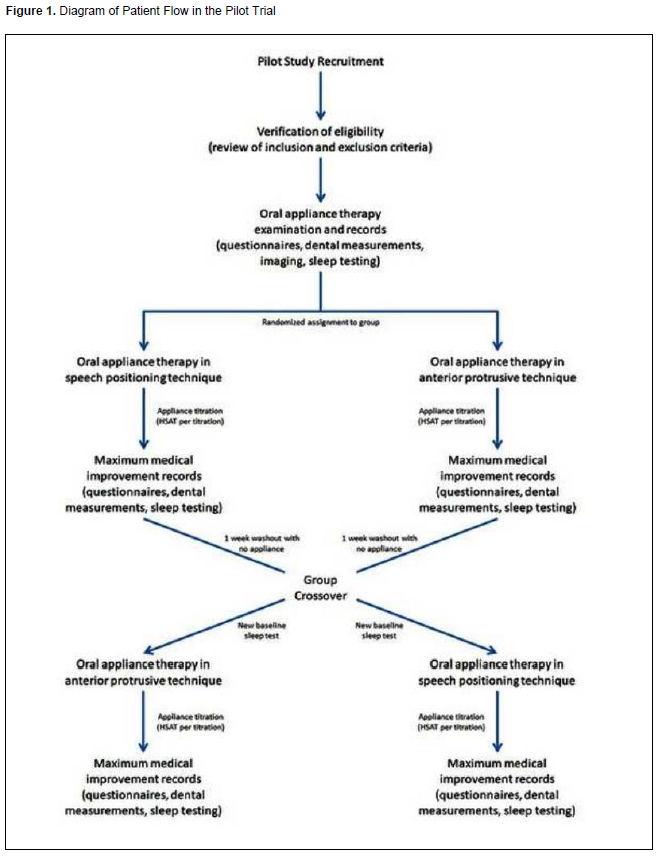
Patients underwent treatment according to standard AADSM treatment recommendations, with the clinician tracking progress and management of the patient’s OSA, including with home sleep apnea testing, until resolution or failure following AASM treatment parameters within a maximum time of 3 months. Posttreatment records included a repeat of the pretreatment questionnaires, confirmation efficacy home sleep apnea testing, patient musculature (masseter, temporalis, temporomandibular joint (TMJ) lateral capsule, TMJ posterior joint space, and sternocleidomastoid) by palpation evaluation, and measurement of the patient’s percentage of mandibular protrusion to maximum mandibular protrusion and retrusion. Patients then underwent a 1-week washout period wearing no appliance before repeating the process, starting with new pretreatment records (excluding cone beam computed tomography based on radiation exposure guidelines). After completion of new pretreatment records, patients were then crossed over to treatment with the other appliance (patients provided with the appliance for adjustments with the APT first were provided with the appliance for adjustments with the SPT, whereas patients provided with the appliance for adjustments with the SPT first were provided with the appliance for adjustments with the APT). Treatment was again repeated similarly under the same criteria (Figure 1).
Figure 1Diagram of Patient Flow in the Pilot Trial. |
{kind=link}
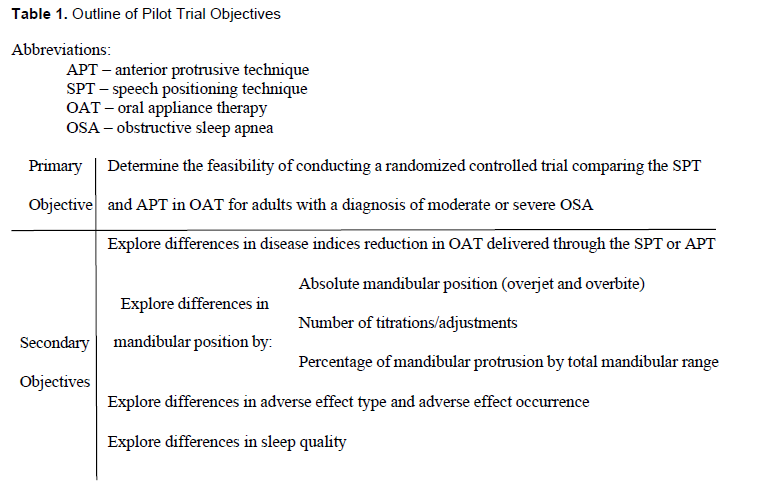
Table 1Outline of Pilot Trial Objectives |
{kind=link}
Data Collection
Feasibility involved an assessment of the practicality and viability of conducting the full-scale RCT with crossover design. Indicators of this feasibility included participant recruitment, participant retention, intervention delivery, and duration of data collection. Data on these indicators were collected through research administrative tracking and clinician feedback. Attrition (dropout) data were collected according to the standard clinical protocol for patient care; administrators contacted the patient to reschedule canceled appointments and recorded the reasoning for the patients not rescheduling their appointments.Initial efficacy data for the pilot trial included disease index reduction data collected through home sleep testing, physical measurements of mandibular position using dental landmarks, occurrence of adverse effects, and differences in sleep quality and patient experience. These are outlined in Table 1. Aside from ambulatory polysomnographic data (AHI, respiratory disturbance index, oxygen desaturation index, etc.) and general dental sleep appliance data (amount of titration, appliance adjustments, signs and symptoms of preexisting TMJ dysfunction and any changes to those conditions, etc.), other data collected included demographic data (age, ethnicity, sex), medical history (including current medications, allergies, supplements, herbals, and complementary medicine therapies), large field of view cone-beam computed tomography (Rayscan S CBCT, Rayscan Canada Ltd.), digital dental impressions (CS3800, Carestream Health Onex Corp.), and questionnaires on sleep quality and quality of life including Sleep Apnea Quality of Life Index, Epworth Sleepiness Scale, Berlin Questionnaire, STOP-BANG questionnaire, and patient experience with OAT. Questionnaires were provided for patients to complete remotely prior to attending clinic appointments. All patients were provided with the OAT patient experience questionnaire after completion of each round of treatment.
Comparative Analyses
Pilot crossover RCT trial data were analyzed using descriptive statistics to generate averages, maximums, minimums, standard deviation, and standard error and to describe differences in patient responses. A paired t-test assuming unequal variances was used to compare groups due to the inability to assume equal variances between groups (for example, between SPT and APT mandibular positioning variables). As a pilot trial, all statistical results were for descriptive purposes and not for statistical significance due to limitations in sample size.RESULTS
Patient Demographics
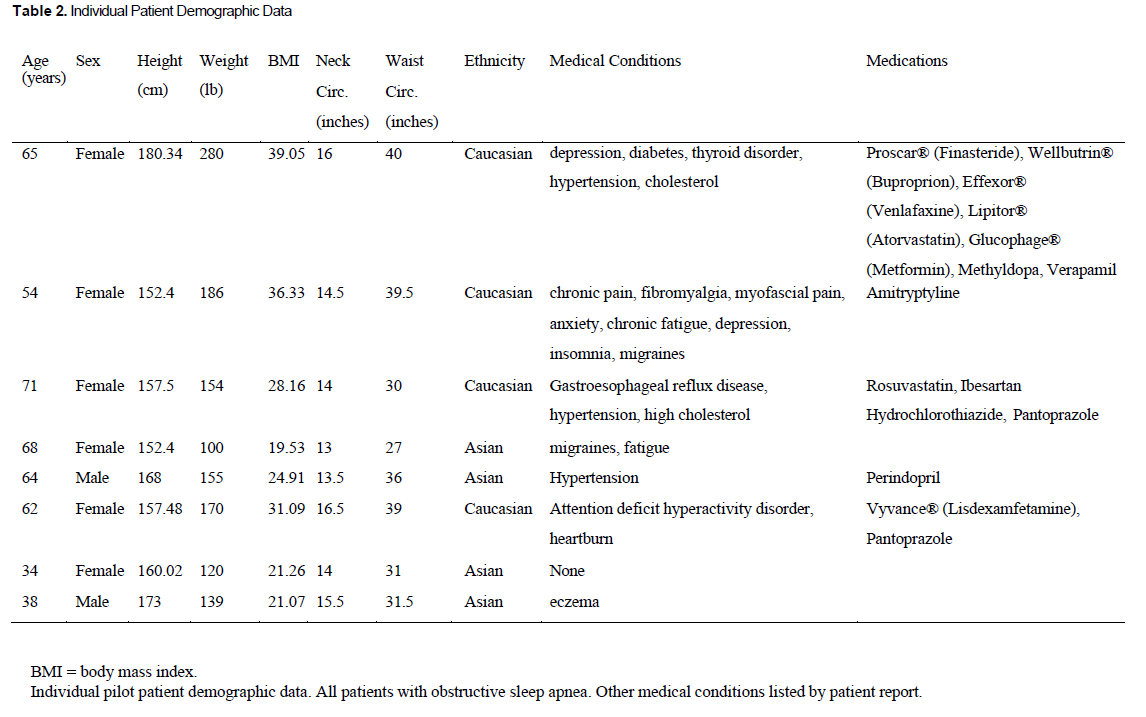
Eight patients between the ages of 34 and 71 years, with an average age of 57 years (standard error [SE] +/- 4.92), completed the study. Patients were recruited between March 2021 and April 2023. Two patients were male, and six were female. Half were Asian and half were Caucasian based on last name and physical appearance. Three patients had previously trialed PAP and were PAP intolerant; the other five were PAP averse. Medical conditions of participants included anxiety, depression, attention deficit hyperactivity disorder, type 2 diabetes, hypertension, high cholesterol, thyroid dysfunction, insomnia, migraine, headache, fibromyalgia, chronic pain, gastroesophageal reflux disease, and eczema. No patient reported changes in their medical conditions or medications throughout the pilot trial. The weight of participants ranged from 100 lb to 280 lb, with an average weight of 163 lb (SE +/- 19.28). Participants' body mass index (BMI) ranged from 19.53 to 39.05, with an average BMI of 27.64 (SE +/- 2.59). Specific per-patient demographic data details are provided in Table 2.Table 2Individual Patient Demographic Data |
{kind=link}
Study Feasibility Data
A total of 46 patients were eligible to participate in the study. A total of 11 patients were recruited to participate in the study, for a recruitment rate of 23.91%. Reasons for nonparticipation included no direct benefit to the patient, extended time of treatment as a research participant, and travel distance to the clinic. A total of eight patients completed participation in the study for an attrition rate of 27.27%. The reasons for dropping out were illness (two patients) and travel distance (one patient).The amount of time associated with patient examination and records for data collection was not significantly longer than nonresearch data collection clinical time. Normal clinical time allotted for examination and records was 2 hours; no research patient required more than an additional 15 minutes for data collection. Adjustments of appliances in both the SPT and the APT took less than 5 minutes.
Changes in Sleep Indices Measurements
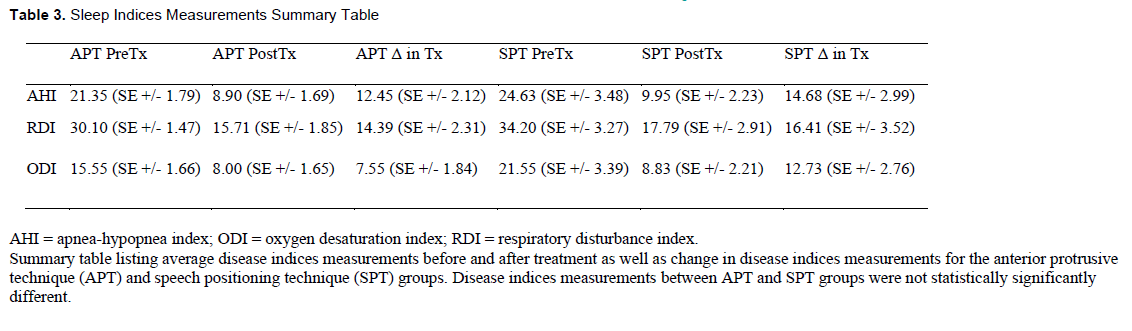
Pretreatment AHI was 21.35 (SE +/- of 1.79) for the APT group and 24.63 (SE +/- 3.48) for the SPT group. Posttreatment AHI was 8.90 (SE +/- 1.69) for the APT group and 9.95 (SE +/- 2.23) for the SPT group.Of the eight patients, one was a nonresponder to OAT, and five were complete responders to both mandibular positioning techniques. One patient was a responder to OAT in the APT but not in the SPT, and one was a responder to OAT in the SPT but not in the APT.
Statistically, there were no significant intergroup differences between pretreatment, posttreatment, or change in disease index numbers. Both groups noted significant changes between their intragroup pretreatment and posttreatment disease index numbers, with significantly lower disease index numbers noted posttreatment than pretreatment. Details of sleep disease indices are summarized in Table 3.
Table 3Sleep Indices Measurements Summary Table |
{kind=link}
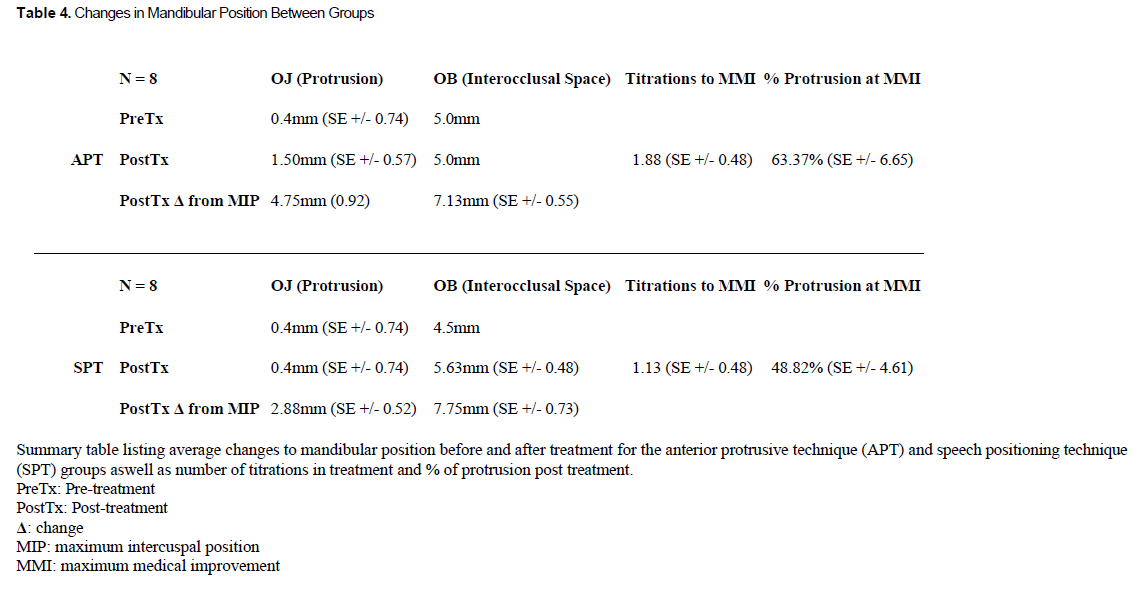
Changes in Mandibular Position
Average habitual occlusion overjet for all patients was 3.25mm (SE +/- 0.49). The average habitual occlusion overbite was 2.13mm (SE +/- 0.55).For the SPT, the initial interocclusal distance was determined to be 4.5 mm of interincisal space based on the minimum material thickness required for structural integrity for the dental sleep appliances. For the APT, the initial interocclusal distance was determined to be 5 mm of interincisal space based on the 5-mm height of the George Gauge bite fork. The average initial overjet for the SPT was 0.4mm (SE +/- 0.74). The initial overjet position for the SPT was used as the initial overjet position for the APT on a per-patient basis to ensure similar starting protrusion for appropriate comparison. Between the two techniques, the SPT averaged 0.75 fewer titrations, 1.87 mm less protrusion, and 14.55% less protrusion. Details of mandibular position are summarized in Table 4.
Exploratory statistics for the pilot sample (N=8) noted significant differences between groups in end overjet position (P < 0.05). However, no significant differences in change in overjet, percentage of protrusion between end overbite position, change in overbite, or number of adjustments/titrations were noted (P > 0.05). These statistical differences did not change in subgroup analysis having removed the single patient who was nonresponsive to both positioning techniques (N=7).
Table 4Changes in Mandibular Position Between Groups |
{kind=link}
Adverse Effects
The pilot crossover RCT data showed that no patients free from TMJ symptoms before OAT experienced TMJ symptoms during OAT. Three patients reported discomfort/pain during palpation of orofacial musculature pretreatment. All three patients with preexisting TMJ symptoms (myalgia, limitations of mandibular range of motion) did not fare significantly differently between both mandibular titration techniques. One patient with preexisting bilateral wrist pain reported worsening wrist pain with the appliance in APT while reporting resolution of wrist pain with the appliance in SPT. The same patient also reported increased jaw clicking when using either dental sleep appliance. One patient experienced changes to occlusion during OAT under both mandibular positioning techniques, which was verified as a change in resting mandibular position as opposed to tooth movement from intraoral scan image overlays. One patient experienced an exacerbation of tinnitus during OAT with the APT for mandibular positioning and no difference in tinnitus during OAT with the SPT for mandibular positioning. Two patients reported generally requiring time to adapt to the dental sleep appliance. One patient reported discomfort on inserting and removing the appliance but no concerns with appliance fit. Adverse effects were generally transient and were primarily dealt with via morning exercises and manual therapy (self-administered massage). Both patients who reported symptomology with one appliance over the other self-selected long-term use of the other appliance after completion of their participation in the pilot trial.Sleep Quality
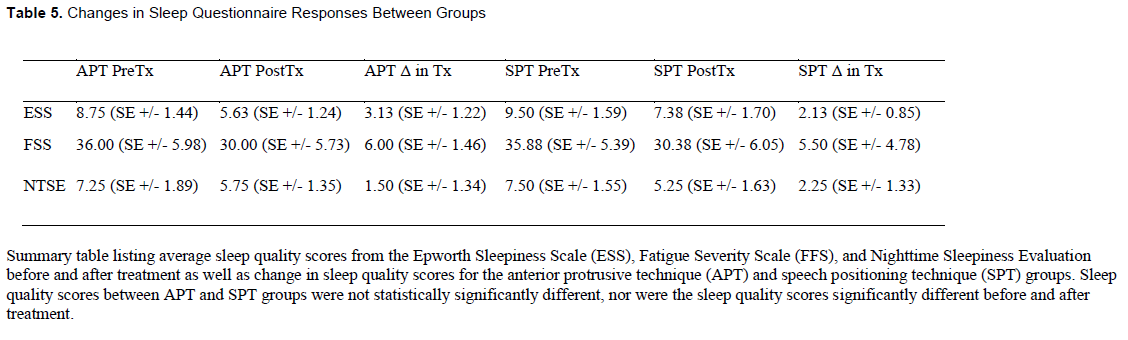
Across all patients, the average pretreatment Epworth Sleepiness Scale score was 9.13 (SE +/- 1.04), the average Fatigue Severity Scale score was 35.94 (SE +/- 3.89), and the average Nighttime Sleepiness Evaluation score was 7.38 (SE +/- 1.18). Exploratory statistics noted no significant differences between groups and before and after treatment for both groups. Details of sleep questionnaires are summarized in Table 5.Patient Experience
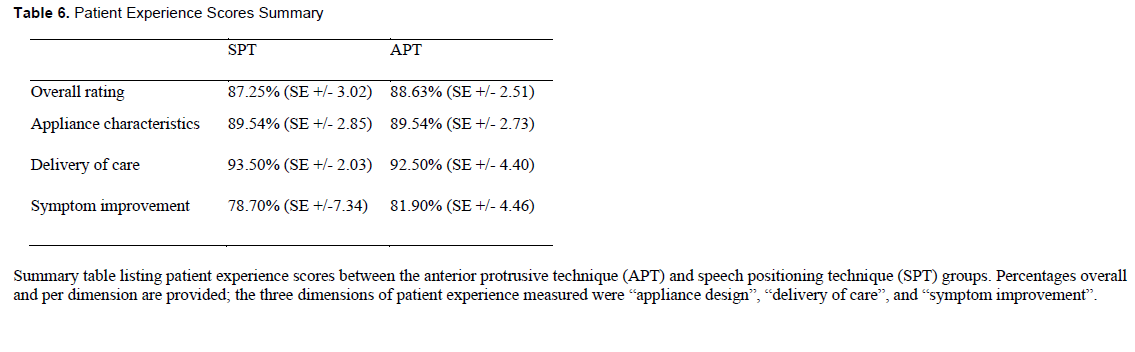
Five patients completed the patient experience questionnaires. Two patients declined to complete the patient experience questionnaire. Patients did not provide reasoning for noncompletion. One patient partially completed the questionnaire and declined to complete it on prompting. The reasoning provided was that the questionnaire was redundant. Four patients reported no preference differences between the two titration techniques. One patient reported a preference for the appliance positioned and adjusted in SPT. The reason for preference was due to fewer office visits (a single adjustment was necessary for the APT, whereas no adjustments were necessary for the SPT for this patient). There were no significant differences in the other dimensions of care delivery or symptom improvement. Patient experience data are summarized in Table 6.Additional Select Patient Information
Additional information posttreatment was collected on three patients: the patient who was a complete nonresponder to OAT for both the APT and SPT and both patients who were responsive to OAT in either the APT or SPT.In an examination of the patient with complete nonresponse to OAT, a tongue tie (grade 3 tongue range of motion ratio [TRMR]), lip seal strength of less than 4 lb, and a first maxillary molar intermolar distance of 34 mm were noted. From previously gathered data the patient had a neck circumference of 16.5 inches, a waist circumference of 39 inches, and a BMI of 31.09.
In examination of the patient who was responsive to OAT in the APT but nonresponsive to OAT in the SPT, a normal range of tongue movement (grade 2 TRMR), lip seal strength of less than 3 lb, and a first maxillary molar intermolar distance of 32 mm were noted. From previously gathered data, the patient had a neck circumference of 14 inches, a waist circumference of 30 inches, and a BMI of 28.16.
In examination of the patient who was responsive to OAT in the SPT but nonresponsive to OAT in the APT, a normal range of tongue movement (grade 2 TRMR), lip seal strength of less than 4 lb, and a first maxillary molar intermolar distance of 31 mm were noted. From previously gathered data, the patient had a neck circumference of 14.5 inches, a waist circumference of 39.5 inches, and a BMI of 36.33.
Table 5Changes in Sleep Questionnaire Responses Between Groups |
{kind=link}
Table 6Patient Experience Scores Summary |
{kind=link}
DISCUSSION
This pilot trial aimed to assess the feasibility of a crossover RCT design comparing the SPT and the APT and to generate preliminary efficacy data for the SPT. This pilot trial suggests that the planned RCT is feasible, with a dropout rate that is less than generally accepted attrition rates of up to 35% in dental clinical trials.65-72 Although the recruitment time for the pilot trial was approximately 2 years, the patient recruitment rate was 23.91%, with a total of 11 patients recruited out of 46 qualified patients in the private practice clinic.The recruitment rate suggests that a dedicated dental sleep medicine clinic can recruit patients within a smaller time window. However, this should be viewed with some caution due to potential differences between patient-clinician relationships in private practice general dental clinics and dental sleep medicine specialty clinics. The attrition rate in the pilot trial may be attributed to the challenges associated with the specific population being studied, public health guidelines related to COVID-19 and other respiratory infections in the local geographic area (Edmonton, Alberta), and the difficulties with randomized crossover trials for exploring novel techniques/interventions. Preliminary efficacy data suggest more positive outcomes for the SPT compared to the APT regarding mandibular position and adverse effects, which may be of clinical relevance. Together, these findings suggest that a crossover RCT comparing the SPT and APT is warranted.
Based on the recruitment rate, attrition rate, and time necessary to recruit sufficient pilot trial participants, strategies to improve recruitment should be considered for a future adequately sampled crossover RCT. These strategies may include increased advertising of the research project, involvement of multiple investigator sites, especially high patient volume dental sleep medicine clinics, and patient incentives for research participation.73,74 An increased budget may be necessary, as financial incentives for increased clinician involvement and patient incentives for participation have been shown to be significantly effective in improving patient recruitment.75-78 Ethical considerations in financial incentives for patient recruitment will need to be considered.75
This pilot crossover RCT suggests that adult patients with OSA being treated with OAT may not have a single target mandibular position for effective treatment. A range of positions may provide therapeutic benefits for OSA in OAT, with the possibility that a patient with no response or incomplete response to a single mandibular positioning technique may benefit from an alternative mandibular positioning technique. Because one patient was a responder to the APT but not the SPT, and one was a responder to the SPT but not the APT, the pilot data suggest that patients in OAT who are not responsive at a specific target position may be responsive at a different target position using different mandibular positioning techniques.
Consistent with previous studies,79-82 the patient with complete nonresponse to OAT had a large neck circumference, large waist circumference, a BMI indicating obesity, limited tongue mobility, acceptable lip seal strength, and lower-than-average maxillary intermolar width. These factors suggest that the patient was a phenotypically poor candidate for OAT.83-85 Additional factors (eg, poor tongue tone and poor tongue jaw dissociation) suggest that the patient also had poor myofunctional coordination of the orofacial musculature and insufficient palatal space for appropriate tongue rest posture.86 The combination of these factors may explain why the patient was nonresponsive to both mandibular positioning techniques in OAT.
Interestingly, the patient who was responsive to OAT in the APT but nonresponsive to OAT in the SPT had a large neck circumference, a normal waist circumference, a BMI indicating overweight, average tongue mobility, limited lip seal strength, and lower-than-average maxillary intermolar width. Additionally, this patient lost lip seal after the second adjustment in the SPT, with significantly worsening disease indices on follow-up sleep testing. The patient did not report losing lip seal with OAT in the APT. This may suggest that patients with poor lip seal strength may not be good candidates for OAT with the SPT due to increased vertical dimension titration.
The patient who was responsive to OAT in the SPT but nonresponsive to OAT in the APT had a large neck circumference, a large waist circumference, a BMI indicating obesity, average tongue mobility, acceptable lip seal strength, and lower-than-average maxillary intermolar width. Although the patient had the typical phenotypic presentation suggestive of poor response to OAT, it may be possible that the use of the SPT in OAT provided a patient-specific mandibular position allowing for myofunctionally neutral tongue resting posture. Because the patient had adequate lip seal strength and average tongue range of motion, maintaining the mandible in the SPT positional range may have aided in maintaining appropriate tongue rest posture in the oral cavity.87-89 Additionally, maintaining the mandible in the SPT orientation may have induced changes in cervical alignment that may have improved airway patency or some other unexplained factors that are not present within a purely mandibular protrusive positioning technique.90-97
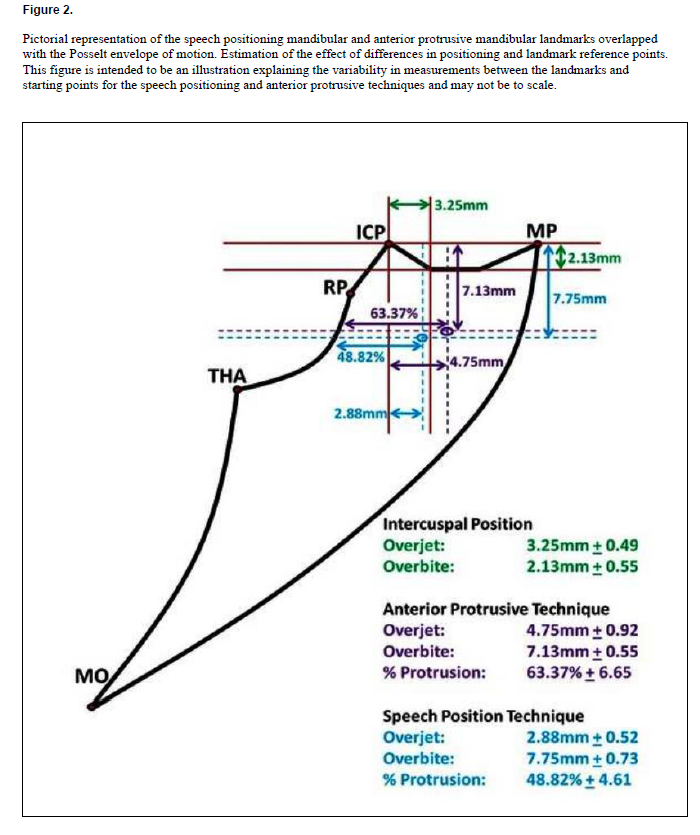
The pilot crossover RCT data support prior research that the SPT allows for less absolute mandibular protrusion than the APT, whereas interocclusal space does not appear to be significantly different.56,57 However, there were no significant differences between the two mandibular positioning techniques regarding protrusion percentage. This may suggest that greater vertical dimension, as measured by incisal edge overbite in the SPT, may position the mandible less anteriorly to the most retruded mandibular position than the APT. A therapeutic position achieved with the SPT may require less mandibular protrusion than one achieved with the APT. A pictorial representation of this can be seen in Figure 2. The clinical significance of these similarities and differences warrants further investigation.
The pilot crossover RCT data suggest that patients using OAT may be at lesser risk of adverse effects if treated with the SPT than with the APT. However, the experienced adverse effects were nontraditional and not commonly associated with OAT. Further research into the occurrence and degree of adverse effects between different mandibular positioning techniques in OAT is warranted.
Early patient experience data suggested a possible preference for the SPT compared with the APT for OAT. Although most patients reported no preference differences, three patients reported a preference for the SPT-positioned appliance, whereas two reported a preference for the APT-positioned appliance. Both patients who experienced nontraditional adverse effects in OAT with the APT noted a preference for the SPT. Two patients noted a preference for the SPT based on the increased speed of treatment. The patient who was not a complete responder to the SPT noted a preference for the APT. One patient noted a preference for the APT based on “comfort” but did not define what that entailed. The decreased rate of completion of patient experience questionnaires suggests greater clinician emphasis on patient experience may be necessary during future studies.
All results from this pilot trial should be viewed with caution. The limited sample size and the nature of pilot studies in design, scope, and limitations bears consideration for any potential insights from the study data. Although limited statistical analyses were provided, these were for descriptive purposes and should not be interpreted as statistically significant.
Future research should evaluate for equivalency in OSA disease indices reduction and sleep quality, differences in therapeutic position, and differences in patient experience between the SPT and APT. An additional collection of data related to lip seal strength, tongue tone, tongue jaw dissociation, and full measurements of tongue range of motion, along with potentially other orofacial myofunctional markers, may be prudent in phenotyping responders to the SPT for OAT. Other studies investigating the effects of changing lip seal strength on vertical range in the SPT, maxillary dentition configuration on tongue resting posture, the adaptation of the SPT to non-English speakers, and the effects of altering nasal patency on patient response to the SPT in OAT may also be of interest.
Figure 2
(more ...)
{kind=link}
CONCLUSION
The pilot crossover RCT data suggest that the clinical application of the SPT in a dental sleep medicine practice for OAT is feasible. There were no complications or difficulties in implementing the entirety of the recently published multidisciplinary consensus protocol for the use of speech characteristics in mandibular positioning for dental sleep medicine. From a practical perspective, the clinical application of the SPT did not take longer in application compared to the APT.The pilot trial suggests that an RCT with crossover design to compare the SPT and APT is feasible. However, researchers are encouraged to use several recruitment strategies to increase sample size. Further, pilot crossover RCT data suggest that the SPT may provide an alternative therapeutic position to the APT for mandibular positioning in OAT in patients with OSA.
REFERENCES
- Osman AM, Carter SG, Carberry JC, Eckert DJ. Obstructive sleep apnea: current perspectives. Nat Sci Sleep. 2018;10:21-34. https://doi.org/10.2147/NSS.S124657
- Eckert DJ. Phenotypic approaches to obstructive sleep apnoea - new pathways for targeted therapy. Sleep Med Rev. 2018;37:45-59. https://doi.org/10.1016/j.smrv.2016.12.003
- Kapur VK, Auckley DH, Chowdhuri DC, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2017;13(3)479-504. https://doi.org/10.5664/jcsm.6506
- Franklin KA, Lindberg E. Obstructive sleep apnea is a common disorder in the population-a review on the epidemiology of sleep apnea. J Thorac Dis. 2015;7(8):1311-1322. https://doi.org/10.3978/j.issn.2072-1439.2015.06.11
- American Academy of Sleep Medicine. Frost & Sulliven. In an Age of Constant Activity, the Solution to Improving the Nation’s Health May Lie in Helping it Sleep Better. What Benefits Do Patients Experience in Treating their Obstructive Sleep Apnea? 2016. http://www.aasmnet.org/sleep-apnea-economic-impact.aspx. Accessed December 24, 2019.
- American Academy of Sleep Medicine. Frost & Sulliven. Hidden Health Crisis Costing America Billions. Underdiagnosing and Undertreating Obstructive Sleep Apnea Draining Healthcare System. 2016. http://www.aasmnet.org/sleep-apnea-economic-impact.aspx. Accessed December 24, 2019.
- Memon J, Manganaro SN. Obstructive Sleep-Disordered Breathing. [Updated 2023 Aug 8]. In StatPearls [Internet]. StatPearls Publishing, Treasure Island, Florida, 2023 Jan. https://pubmed.ncbi.nlm.nih.gov/28722938/.
- Young T, Finn L, Peppard PE, et al. Sleep disordered breathing and mortality: eighteen-year follow- up of the Wisconsin sleep cohort. Sleep. 2008;31(8):1071-1078.
- Gami AS, Howard DE, Olson EJ, Somers VK. Day-night pattern of sudden death in obstructive sleep apnea. N Engl J Med. 2005;352(12):1206-1214. https://doi.org/10.1056/NEJMoa041832
- Wang X, Bi Y, Zhang Q, Pan F. Obstructive sleep apnoea and the risk of type 2 diabetes: a meta- analysis of prospective cohort studies. Respirology. 2013;18(1):140-146. https://doi.org/10.1111/j.1440-1843.2012.02267.x
- Anker SD, von Haehling S, Germany R. Sleep-disordered breathing and cardiovascular disease. Indian Heart J. 2016;68 Suppl 1: S69-76. https://doi.org/10.1016/j.ihj.2015.11.018
- Feng C, Yang Y, Chen L, et al. Prevalence and characteristics of erectile dysfunction in obstructive sleep apnea patients. Front Endocrinol (Lausanne). 2022;13:812974. https://doi.org/10.3389/fendo.2022.812974
- Gu Y, Wu C, Qin F, Yuan J. Erectile dysfunction and obstructive sleep apnea: A review. Front Psychiatry. 2022;13:766639. https://doi.org/10.3389/fpsyt.2022.766639
- Pascual M, de Batlle J, Barbé F, et al. Erectile dysfunction in obstructive sleep apnea patients: A randomized trial on the effects of continuous positive airway pressure (CPAP). PLoS One. 2018;13(8):e0201930. https://doi.org/10.1371/journal.pone.0201930
- Marshall NS, Wong KK, Cullen SR, Knuiman MW, Grunstein RR. Sleep apnea and 20-year follow-up for all-cause mortality, stroke, and cancer incidence and mortality in the Busselton Health Study cohort. J Clin Sleep Med. 2014;10(4):355-362. https://doi.org/10.5664/jcsm.3600
- Marshall NS, Wong KK, Liu PY, Cullen SR, Knuiman MW, Grunstein RR. Sleep apnea as an independent risk factor for all-cause mortality: the Busselton Health Study. Sleep. 2008;31(8):1079-1085. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2542953/
- Jennum P, Tønnesen P, Ibsen R, Kjellberg J. All-cause mortality from obstructive sleep apnea in male and female patients with and without continuous positive airway pressure treatment: a registry study with 10 years of follow-up. Nat Sci Sleep. 2015;7:43-50. https://doi.org/10.2147/NSS.S75166
- Lavie P, Lavie L, Herer P. All-cause mortality in males with sleep apnoea syndrome: declining mortality rates with age. Eur Respir J. 2005;25(3):514-520. https://doi:10.1183/09031936.05.00051504
- Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: An update for 2015. J Clin Sleep Med. 2015;11(7):773-827. https://doi.org/10.5664/jcsm.4858
- American Academy of Sleep Medicine. Practice Guidelines. https://aasm.org/clinical-resources/practice-standards/practice-guidelines/. Accessed March 28, 2020
- Weiss P, Kryger M. Positive airway pressure therapy for obstructive sleep apnea. Otolaryngol Clin North Am. 2016;49(6):1331-1341. https://doi.org/10.1016/j.otc.2016.07.004
- MedlinePlus. Positive airway pressure treatment. https://medlineplus.gov/ency/article/001916.htm Accessed December 9, 2023
- Stanford Medicine Health Care. Positive airway pressure (PAP) Therapies. https://stanfordhealthcare.org/medical-treatments/p/positive-airway-pressure-therapies.html Accessed December 9, 2023.
- Kakkar RK, Berry RB. Positive airway pressure treatment for obstructive sleep apnea. Chest. 2007;132(3):1057-1072. https://doi.org/10.1378/chest.06-2432
- Gianoni-Capenakas S, Gomes AC, Mayoral P, Miguez M, Pliska B, Lagravère M. Sleep-disordered breathing: the dentists’ role – a systematic review. J Dent Sleep Med. 2020;7:1. http://dx.doi.org/10.15331/jdsm.7108
- Sutherland K, Phillips CL, Cistulli PA. Efficacy versus effectiveness in the treatment of obstructive sleep apnea: CPAP and oral appliances. J Dent Sleep Med. 2015;2(4):175-181. http://dx.doi.org/10.15331/jdsm.5120.
- Sheats R, Essick G, Grosdidier J, et al. Identifying the appropriate therapeutic position of an oral appliance. J Dent Sleep Med. 2020;7(4).
- Hoekema A, Stegenga B, de Bont LGM. Efficacy and co-morbidity of oral appliances in the treatment of obstructive sleep apnea-hypopnea: a systematic review. Crit Rev Oral Biol Med. 2004;15:137-155. https://doi.org/10.1177/154411130401500303
- Burke P, Knapman F, Tong B, et al. Effects of mandibular advancement splints on upper airway physiology in obstructive sleep apnoea [Abstract]. J Sleep Res. 2018;27:114.
- Brown L, Juge L, Burke P, Sutherland K, Cistulli P, Bilston L. How lateral airway tissues affect upper airway dimensions with mandibular advancement in obstructive sleep apnoea [Abstract]. Eur Respir J. 2018;52(Suppl 62):OA5369.
- Juge L, Knapman F, Eckert D, et al. Tongue deformation during mandibular advancement may help to predict mandibular advancement treatment outcome in obese patients with obstructive sleep apnoea [Abstract]. J Sleep Res. 2018;27:0037.
- Chan ASL, Sutherland K, Schwab RJ, et al. The effect of mandibular advancement on upper airway structure in obstructive sleep apnoea. Thorax. 2010;65(8):726-732. https://doi.org/10.1136/thx.2009.131094
- Ferguson KA, Cartwright R, Rogers R, Schmidt-Nowara W. Oral appliances for snoring and obstructive sleep apnea: a review. Sleep. 2006;29(2):244-262. https://doi.org/10.1093/sleep/29.2.244
- Ngiam J, Balasubramaniam R, Darendeliler MA, Cheng AT, Waters K, Sullivan CE. Clinical guidelines for oral appliance therapy in the treatment of snoring and obstructive sleep apnoea. Aust Dent J. 2013;58(4):408-419. https://doi.org/10.1111/adj.12111
- Ippolito DR, Stipa C, Cameli M, Sorrenti G, Pelligra I, Alessandri-Bonetti G. Maximum voluntary retrusion or habitual bite position for mandibular advancement assessment in the treatment of obstructive sleep apnoea patients. J Oral Rehabil. 2020;47(3):301-306. https://doi.org/10.1111/joor.12902
- Gindre L, Gagnadoux F, Meslier N, Gustin JM, Racineux JL. Mandibular advancement for obstructive sleep apnea: dose effect on apnea, long-term use and tolerance. Respiration. 2008;76(4):386-392. https://doi.org/10.1159/000156861
- Gupta A, Tripathi A, Trivedi C, Sharma P, Mishra A. A study to evaluate the effect of different mandibular horizontal and vertical jaw positions on sleep parameters in patients with obstructive sleep apnea. Quintessence Int. 2016;47(8):661-666. https://doi.org/10.3290/j.qi.a36383
- Aarab G, Lobbezoo F, Hamburger HL, Naeije M. Effects of an oral appliance with different mandibular protrusion positions at a constant vertical dimension on obstructive sleep apnea. Clin Oral Investig. 2010;14(3):339-345. https://doi.org/10.1007/s00784-009-0298-9
- Mayoral P, Lagravère MO, Míguez-Contreras M, Garcia M. Antero-posterior mandibular position at different vertical levels for mandibular advancing device design. BCM Oral Health. 2019;19(1):85. https://doi.org/10.1186/s12903-019-0783-8
- Anitua E, Mayoral P, Almeida GZ, Durán-Cantolla J, Alkhraisat MH. A multicenter prospective study on the use of a mandibular advancement device in the treatment of obstructive sleep apnea. Dent J (Basel). 2023 Oct 24;11(11):247. https://doi: 10.3390/dj11110247
- Anitua E, Durán-Cantolla J, Almeida GZ, Alkhraisat MH. Minimizing the mandibular advancement in an oral appliance for the treatment of obstructive sleep apnea. Sleep Med. 2017;34:226-231. https://doi.org/10.1016/j.sleep.2016.12.019
- Marklund M, Franklin KA, Persson M. Orthodontic side-effects of mandibular advancement devices during treatment of snoring and sleep apnoea. Eur J Orthod. 2001;23(2):135-144. https://doi.org/10.1093/ejo/23.2.135
- Giannasi LC, Almeida FR, Magini M, et al. Systematic assessment of the impact of oral appliance therapy on the temporomandibular joint during treatment of obstructive sleep apnea: long-term evaluation. Sleep Breath. 2009;13(4):375-381. https://doi.org/10.1007/s11325-009-0257-3
- Sheats RS, Schell TG, Blanton AO, et al. Management of side effects of oral appliance therapy for sleep-disordered breathing. J Dent Sleep Med. 2017;4(4):111-125. http://dx.doi.org/10.15331/jdsm.6746
- de Almeida FR, Bittencourt LR, de Almeida CIR, Tsuiki S, Lowe AA, Tufik S. Effects of mandibular posture on obstructive sleep apnea severity and the temporomandibular joint in patients fitted with an oral appliance. Sleep. 2002;25(5):507-513.
- Minagi HO, Okuno K, Nohara K, Sakai T. Predictors of side effects with long-term oral appliance therapy for obstructive sleep apnea. J Clin Sleep Med. 2018;14(1):119-125. https://doi.org/10.5664/jcsm.6896
- Pliska BT, Nam H, Chen H, Lowe AA, Almeida FR. Obstructive sleep apnea and mandibular advancement splints: occlusal effects and progression of changes associated with a decade of treatment. J Clin Sleep Med. 2014;10(12):1285-1291. https://doi.org/10.5664/jcsm.4278
- Ng ET, Perez-Garcia A, Lagravère-Vich MO. Development and initial validation of a questionnaire to measure patient experience with oral appliance therapy. J Clin Sleep Med. 2023;19(8):1437- 1445. https://doi.org/10.5664/jcsm.10562
- Cronin C, Essick G, Boone H, Phillips C. Long term patient centered outcomes following treatment with oral appliance therapy for obstructive sleep apnea. J Dent Sleep Med. 2019;6(3). http://dx.doi.org/10.15331/jdsm.7088
- Nordin E, Stenberg M, Tegelberg Å. Obstructive sleep apnoea: Patients' experiences of oral appliance treatment. J Oral Rehabil. 2016;43(6):435-442. https://doi.org/10.1111/joor.12385
- Saglam-Aydinatay B, Taner T. Oral appliance therapy in obstructive sleep apnea: Long-term adherence and patients experiences. Med Oral Patol Oral Cira Bucal. 2018;23(1):e72-e77. https://doi.org/10.4317/medoral.22158
- Pound E. Let /S/ be your guide. J Prosthet Dent. 1977;38(5):482-489. https://doi.org/10.1016/0022-3913(77)90022-1
- Hands On Phonetics approach to denture retention. Dental Abstracts. 2008;53(5):247-249. https://doi.org/10.1016/j.denabs.2008.04.020
- Makzoumé JE. Morphologic comparison of two neutral zone impression techniques: a pilot study. J Prosthet Dent. 2004;92(6):563-568. https://doi.org/10.1016/j.prosdent.2004.09.010
- Bohnenkamp DM, Garcia LT. Phonetics and tongue position to improve mandibular denture retention: a clinical report. J Prosthet Dent. 2007;98(5):344-347. https://doi.org/10.1016/S0022- 3913(07)60117-6
- Viviano J, Klauer D, Olmos S, Viviano JD. Retrospective comparison of the George GaugeTM registration and the sibilant phoneme registration for constructing OSA oral appliances. Cranio. 2022;40(1):5-13. https://doi.org/10.1080/08869634.2019.1694776
- Ng ET, Mayoral P, Hernandez IA, Lagravère MO. Comparing anterior protrusive with sibilant phoneme mandibular positioning techniques for dental sleep appliances in managing obstructive sleep apnea: A retrospective study. J Dent Sleep Med. 2021;8(1).
- Ng ET, Mayoral P, Hernandez I, Lagravère, MO. Comparing a sibilant phoneme denture bite position with an anterior protrusive mandibular positioning device in oral appliance therapy for dental treatment of obstructive sleep apnea: A systematic review. J Dent Sleep Med. 2020;7(4). http://dx.doi.org/10.15331/jdsm.7162
- Ng ET, Lagravere MO, Perez-Garcia A. Delphi consensus on the use of speech for mandibular positioning in dental sleep medicine. J Dent Sleep Med. Published online May 22, 2024
- Eldridge SM, Lancaster GA, Campbell MJ, et al. Defining feasibility and pilot studies in preparation for randomised controlled trials: Development of a conceptual framework. PLoS One. 2016;11(3):e0150205. https://doi.org/10.1371/journal.pone.0150205
- Hassan ZA, Schattner P, Mazza D. Doing a pilot study: Why is it essential? Malays Fam Physician. 2006;1(2-3):70-73.
- Equator Network. Enhancing the QUAlity and Transparency of health Research. Consort 2010 statement: extension to randomised pilot and feasibility trials. https://www.equator-network.org/reporting-guidelines/consort-2010-statement-extension-to-randomised-pilot-and-feasibility-trials/ Accessed December 2, 2023
- Hu J, Liptak L. Evaluation of a new oral appliance with objective compliance recording capability: A feasibility study. J Dent Sleep Med 2018;5(2):47-50. http://dx.doi.org/10.15331/jdsm.7024
- Segù M, Campagnoli G, Di Blasio M, Santagostini A, Pollis M, Levrini L. Pilot study of a new mandibular advancement device. Dent J (Basel). 2022;10(6):99. https://doi.org/10.3390/dj10060099
- Cooper CL, Whitehead A, Pottrill E, Julious SA, Walters SJ. Are pilot trials useful for predicting randomisation and attrition rates in definitive studies: A review of publicly funded trials. Clin Trials. 2018;15(2):189-196. https://doi.org/10.1177/1740774517752113
- Moerbeek M. The cluster randomized crossover trial: The effects of attrition in the AB/BA design and how to account for it in sample size calculations. Clin Trials. 2020;17(4):420-429. https://doi.org/10.1177/1740774520913042
- Patient Dropout. However, rates of treatment dropout are high (up to 50% of youth who enter treatment), with the median duration of treatment lasting 6 weeks. From: Encyclopedia of Adolescence, 2011. https://www.sciencedirect.com/topics/medicine-and-dentistry/patient-dropout Accessed December 9, 2023
- Low JL, Lewis SM, Prescott P. Assessing robustness of crossover designs to subjects dropping out. Statistics and Computing. 1999;9:219-227. https://doi.org/10.1023/A:1008974031782
- Macey R, Glenny AM, Brocklehurst P. Feasibility study: Assessing the efficacy and social acceptability of using dental hygienist-therapists as front-line clinicians. Br Dent J. 2016;221(11):717-721. https://doi.org/10.1038/sj.bdj.2016.913
- Patel R, Khan I, Pennington M, Pitts NB, Robertson C, Gallagher JE. Protocol for a randomised feasibility trial comparing fluoride interventions to prevent dental decay in older people in care homes (FInCH trial). BMC Oral Health. 2021;21(1):302. https://doi.org/10.1186/s12903-021- 01650-9
- Al-Nawas B, Domagala P, Fragola G, et al. A prospective noninterventional study to evaluate survival and success of reduced diameter implants made from titanium-zirconium alloy. J Oral Implantol. 2015;41(4):e118-e125. https://doi.org/10.1563/AAID-JOI-D-13-00149
- Palmer RM, Smith BJ, Palmer PJ, Floyd PD. A prospective study of Astra single tooth implants. Clin Oral Implants Res. 1997;8(3):173-179. https://doi.org/10.1034/j.1600-0501.1997.080303.x
- Thoma A, Farrokhyar F, McKnight L, Bhandari M. Practical tips for surgical research: How to optimize patient recruitment. Can J Surg. 2010;53(3):205-210.
- Garnett A, Northwood M. Recruitment of community-based samples: experiences and recommendations for optimizing success. Can J Nurs Res. 2022;54(2):101-111. https://doi.org/10.1177/08445621211060935
- Vellinga A, Devine C, Ho MY, et al. What do patients value as incentives for participation in clinical trials? A pilot discrete choice experiment. Res Ethics. 2020;16(1-2):1-12.
- Wise J. Give doctors financial incentives to take part in clinical trials, review recommends. BMJ. 2023;381:1226. https://doi.org/10.1136/bmj.p1226
- Bickman L, Domenico HJ, Byrne DW, et al. Effects of financial incentives on volunteering for clinical trials: A randomized vignette experiment. Contemp Clin Trials. 2021;110:106584. https://doi.org/10.1016/j.cct.2021.106584
- Abdelazeem B, Abbas KS, Amin MA, et al. The effectiveness of incentives for research participation: A systematic review and meta-analysis of randomized controlled trials. PLoS One. 2022;17(4):e0267534. https://doi.org/10.1371/journal.pone.0267534
- Yoon A, Zaghi S, Weitzman R, et al. Toward a functional definition of ankyloglossia: validating current grading scales for lingual frenulum length and tongue mobility in 1052 subjects. Sleep Breath. 2017;21(3):767-775. https://doi.org/10.1007/s11325-016-1452-7
- Hingorjo MR, Qureshi MA, Mehdi A. Neck circumference as a useful marker of obesity: A comparison with body mass index and waist circumference. J Pak Med Assoc. 2012;62(1):36-40
- Zaghi S, Shamtoob S, Peterson C, et al. Assessment of posterior tongue mobility using lingual- palatal suction: Progress towards a functional definition of ankyloglossia. J Oral Rehabil. 2021;48(6):692-700. https://doi.org/10.1111/joor.13144
- FAirEST.org https://www.fairest.org/tools/ (Tool: Fairest 6) Accessed January 25, 2024
- Camañes-Gonzalvo S, Bellot-Arcís C, Marco-Pitarch R, et al. Comparison of the phenotypic characteristics between responders and non-responders to obstructive sleep apnea treatment using mandibular advancement devices in adult patients: Systematic review and meta-analysis. Sleep Med Rev. 2022;64:101644. https://doi.org/10.1016/j.smrv.2022.101644
- Lee CF, Chen YJ, Huang WC, et al. Prediction of mandibular advancement device response using CPAP pressure in different polysomnographic phenotypes. Nat Sci Sleep. 2022;14:517-529. https://doi.org/10.2147/NSS.S351027
- Chen H, Eckert DJ, van der Stelt PF, et al. Phenotypes of responders to mandibular advancement device therapy in obstructive sleep apnea patients: A systematic review and meta-analysis. Sleep Med Rev. 2020;49:101229. https://doi.org/10.1016/j.smrv.2019.101229
- Dydyk A, Milona M, Janiszewska-Olszowska J, Wyganowska M, Grocholewicz K. Influence of shortened tongue frenulum on tongue mobility, speech and occlusion. J Clin Med. 2023;12(23):7415. https://doi.org/10.3390/jcm12237415
- Alghadir AH, Zafar H, Iqbal ZA. Effect of tongue position on postural stability during quiet standing in healthy young males. Somatosens Mot Res. 2015;32(3):183-186. https://doi.org/10.3109/08990220.2015.1043120
- Fukuda T, Kohzuka Y, Almeida FR, Iijima T, Masuda R, Tsuiki S. Control of tongue position in patients with obstructive sleep apnea: Concept and protocol for a randomized controlled crossover trial. Int J Environ Res Public Health. 2023;20(11):6026. https://doi.org/10.3390/ijerph20116026
- Wang W, Di C, Mona S, Wang L, Hans M. Tongue function: An underrecognized component in the treatment of obstructive sleep apnea with mandibular repositioning appliance. Can Respir J. 2018;2018:2157974. https://doi.org/10.1155/2018/2157974
- Walsh JH, Maddison KJ, Platt PR, Hillman DR, Eastwood PR. Influence of head extension, flexion, and rotation on collapsibility of the passive upper airway. Sleep. 2008;31(10):1440-1447.
- Choi JK, Goldman M, Koyal S, Clark G. Effect of jaw and head position on airway resistance in obstructive sleep apnea. Sleep Breath. 2000;4(4):163-168. https://doi.org/10.1007/s11325-000- 0163-1
- Herzog J, Göttfert F, Maurer-Grubinger C, et al. Improvement of cervical spine mobility and stance stability by wearing a custom-made mandibular splint in male recreational athletes. PLoS One. 2022;17(12):e0278063.https://doi.org/10.1371/journal.pone.0278063
- Armijo-Olivo S, Rappoport K, Fuentes J, et al. Head and cervical posture in patients with temporomandibular disorders. J Orofac Pain. 2011 Summer;25(3):199-209.
- Takigawa T, Matsuoka S, Iida J, Soma K. [Jaw position, head position, body posture: development of an integrated system of examination, Part I]. Kokubyo Gakkai Zasshi. 1995;62(3):441-450. Japanese. https://doi.org/10.5357/koubyou.62.441
- Jan MA, Marshall I, Douglas NJ. Effect of posture on upper airway dimensions in normal human. Am J Respir Crit Care Med. 1994;149(1):145-148. https://doi.org/10.1164/ajrccm.149.1.8111573
- Greenland KB, Edwards MJ, Hutton NJ, Challis VJ, Irwin MG, Sleigh JW. Changes in airway configuration with different head and neck positions using magnetic resonance imaging of normal airways: a new concept with possible clinical applications. Br J Anaesth. 2010;105(5):683-690. https://doi.org/10.1093/bja/aeq239
- Chan C, Chan L, Ng ET. Debilitating lower back pain during menses unexpectedly resolved after treatment of subclinical temporomandibular disorder: a case report. Gen Dent. 2024;72(1):66-70.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication April 13, 2024
Submitted in final revised form April 13, 2024
Accepted for publication May 12, 2024
Address correspondence to: Enoch Ng, DDS, School of Dentistry, Faculty of Medicine and Dentistry; University of Alberta, 11405 - 87th Avenue, Edmonton, Alberta Canada, T6G 1C9; Email: enoch@ualberta.ca