Original Article 1, Issue 9.4
Is There a Relationship Between Obstructive Sleep Apnea Severity and Dental Arch Form in Adult Patients? An Observational Retrospective Study
http://dx.doi.org/10.15331/jdsm.7262Daniela Rita Ippolito, DDS1, Serena Incerti Parenti, DDS, PhD1, Laura Laffranchi, DDS, PhD2, Corrado Paganelli, DMD, MD2, Giulio Alessandri-Bonetti, MD, DDS1
1 Department of Biomedical and Neuromotor Sciences (DIBINEM), Section of Orthodontics and Sleep Dentistry, University of Bologna, Bologna, Italy: 2Dental School, University of Brescia, Brescia, Italy
ABSTRACT
 |
Study Objectives:
The purpose of this study was to investigate the relationship between dental arch morphologic characteristics and OSA severity, after controlling potential confounders such as sex, age, and body mass index (BMI).
Methods:
The dental casts of 91 patients with OSA were scanned and reference points of the dental arches were identified. Intertooth distances were determined. Cartesian coordinates of the bracket slot points were used to generate the best-fitting fourth degree polynomial equation and to compare the patient’s arch form with three standard arch forms (square, ovoid, tapered). Hierarchical regressions were run to examine the amount of variability in apnea-hypopnea index (AHI) that dental arch linear parameters, polynomial coefficients, and arch forms explained after controlling for patients’ general characteristics (sex, age, and BMI).
Results:
The increase in AHI variance accounted for by dental parameters (either linear parameters or polynomial coefficients or arch forms) was not statistically significant (P>0.05).
Conclusions:
No relationship was found between OSA severity and dental arch morphologic characteristics after controlling for potential confounders such as sex, age, and BMI.
Keywords:
obstructive sleep apnea; apnea/hypopnea index; dental arch; dental casts.
Citation:
Ippolito DR, Incerti Parenti S, Laffranchi L, Paganelli C, Alessandri-Bonetti G. Is there a relationship between obstructive sleep apnea severity and dental arch form in adult patients? An observational retrospective study. J Dent Sleep Med. 2022;9(4)
INTRODUCTION
Obstructive sleep apnea (OSA) is a common disorder characterized by repetitive episodes of partial or complete obstruction of the upper airway during sleep, resulting in oxygen desaturation, sleep fragmentation, and excessive daytime sleepiness.1 Polysomnography (PSG) is the current gold standard test for the diagnosis of OSA. The severity of the disorder is defined as the number of partial or complete cessations of breathing per hour of sleep (apnea-hypopnea index, AHI), with ≤5 to 15 events per hour classified as mild, 15 to 30 events per hour as moderate, and ≥30 events per hour as severe.2,3 The pathogenesis is multifactorial, with both anatomic and nonanatomic pathophysiologic traits contributing, alone or in combination, to the development of the disorder.4 Nonanatomic pathophysiologic traits include the ability of the upper airway dilator muscles to respond to respiratory challenge during sleep, the propensity to wake from increased respiratory drive during sleep (arousal threshold), and the stability of the respiratory control system (loop gain).4,5 Anatomically, an imbalance between the volume of the upper airway soft tissue and the bony enclosure size may result in pharyngeal airway obstruction during sleep.6 Obstruction may occur at multisegmental sections of the upper airway: nasopharynx, oropharynx, and hypopharynx. Locating the level of upper airway obstruction is a key clinical feature for addressing OSA treatment; however, the assessment of the disease does not require knowing at which point the obstruction is. Drug-induced sleep endoscopy is currently the best technique for direct visualization of the site or sites of obstruction in sleeping patients.7 With regard to the anatomic aspect, several cephalometric studies have investigated the craniofacial characteristics in adult patients with OSA and, also, the relationship between cephalometric parameters and AHI.8-17 A recent systematic review concluded that there is strong evidence for reduced pharyngeal airway space, inferiorly placed hyoid bone, and increased vertical growth pattern in adult patients with OSA in comparison with healthy patients.18 Conversely, limited data are available on dental arch morphology, with narrower dental arches being generally observed in patients with OSA.19-23 This method can be considered more practical because it does not require radiographic examinations and several landmarks identification but, so far, no study has investigated the relationship between dental arch morphology and OSA severity taking into consideration the effect of potential confounders such as sex, age, and body mass index (BMI). Generally, OSA severity increases with age and women are less severely affected than men, but this sex difference narrows with age due to the increased risk of OSA brought by menopause.24 Moreover, obesity is recognized as an important risk factor for OSA and a significant positive correlation exists between BMI and AHI.25,26
Therefore, the aim of this study was to investigate the relationship between dental arch morphologic characteristics and AHI on a sample of adult Caucasian patients with OSA, controlling the effects of sex, age, and BMI.
MATERIALS AND METHODS
Study design and sample
The study was designed as an observational retrospective study. It was approved by the Ethical Committee of the Ausl of Bologna (number of approval: 435/2018/OSS/AUSLBO). Consent was obtained by the study participants prior to study commencement. Participants were retrieved from patients who accessed the Department of Orthodontics of the University of Bologna (Italy) for consultation for treatment with mandibular advancement device between January 2008 and June 2016. Inclusion criteria were: white ancestry, age older than18 years, a diagnosis of OSA based on PSG (i.e. AHI ≥5 events per hour with symptoms/sequelae or AHI ≥15 events per hour regardless of associated symptoms),27 good quality dental casts, presence of at least 10 teeth (excluding third molars) in each dental arch. Exclusion criteria were: previous or ongoing orthodontic treatment, history of reconstructive/orthognathic surgery to the head and neck, history of pharyngeal surgery, craniofacial syndromes, and severe crowding (8 mm or more).
Data Collection
Demographic data, BMI, and AHI were obtained from manual medical record review. Dental casts were digitized using an optical scanner (AGE Solutions SRL, Pisa, Italy) and scans were saved in stereolithography format. The digitized renderings were analyzed using Rhinoceros software (Rhinoceros® Nurbs modeling for Windows, Robert McNeel & Associates, Seattle, Washington, USA). One operator (DRI) identified on each cast of both dental arches the points shown in Figure 1a. A second point, "BS" (or bracket slot), was obtained using the method of Andrews28 as shown in Figure 1b and used only to determine dental arch form. The projections of the points in Figure 1a were used to compute linear measurements (Figure 2). The X and Y coordinates for the BS points projections on the occlusal plane were inputted into the mathematical software MATLAB (MATLAB version 8.5.0.197613 (R2015a), Natick, Massachusetts, USA: The MathWorks Inc., 2015). These projections were used to generate the best-fitting curve that represented the arch, by using the fourth-degree polynomial equation (f(x)=ax4bx3cx2dxe). Using a series of complex mathematical steps (available upon request), each subject's dental arch was classified into one of the three standard arch forms (square, ovoid, tapered; OrthoForm, 3M Unitek, Monrovia, California, USA) (Figure 3).
Statistical Analysis
Method Error and Reliability
To assess the errors associated with the dental casts measurements, 15 casts were randomly selected and their measurements were repeated by the same operator three weeks apart. A second blinded, duly calibrated operator analyzed the same 15 casts and interobserver reliability was tested using the intraclass correlation coefficient.Relationship Between AHI and Dental Arch Characteristics
Hierarchical regressions were run to examine the amount of variability in AHI that dental arch characteristics (expressed as linear parameters, polynomial coefficients, and arch forms) explained after controlling for patients’ general characteristics (sex, age, and BMI). Therefore, during the first step of the hierarchical regression procedure, patients’ general characteristics were block entered, providing the variance accounted for by this group of independent variables. During the second step, dental arch linear parameters/coefficients of the polynomial curve that best fitted the arch/arch forms were entered into the step 1 model, providing their unique contribution to AHI.All statistical analyses were conducted using the Statistical Package for Social Sciences Software (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0. Armonk, New York, USA: IBM Corporation). A value of P<0.05 was set as the level for statistical significance.
RESULTS
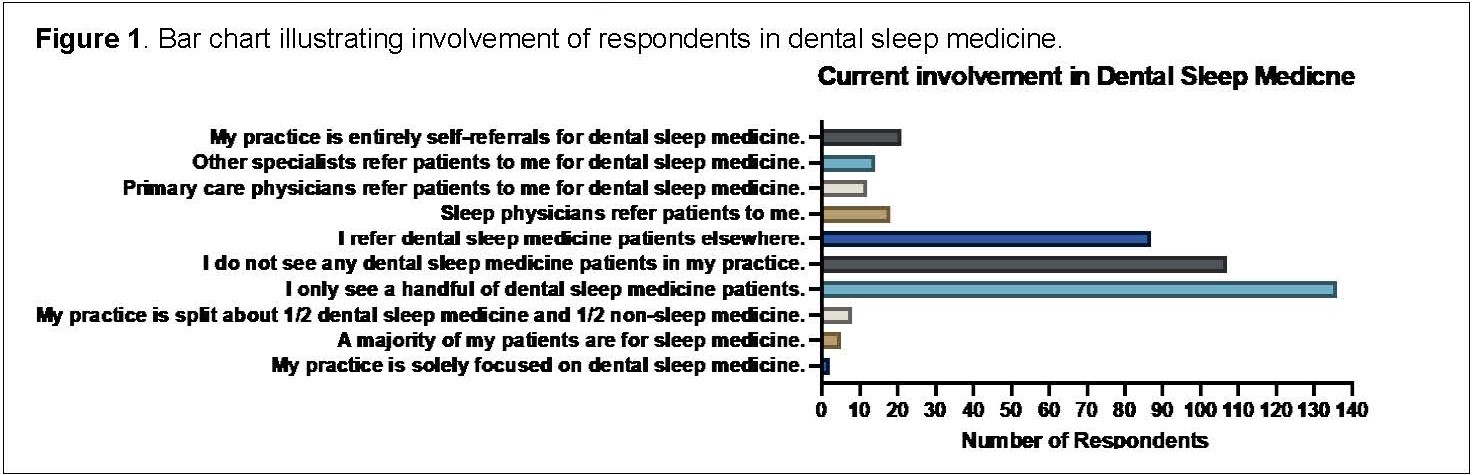
Of a total of 133 patients considered for inclusion, 42 were excluded (n=11: simple snorers, n=24: insufficient number of teeth in either maxillary or mandibular arch, n=7 damaged dental casts). Therefore, the final sample consisted of 91 patients with OSA. The sex distribution was 16 women (17.6%) and 75 men (82.4%). The average age was 53.55 years (95% confidence interval: range 19-77 years). The mean BMI was 27.56 kg/m2 (95% confidence interval: 26.83 to 28.29 kg/m2) with 24 (26.4%) obese patients (BMI≥30 kg/m2) (Table 1).
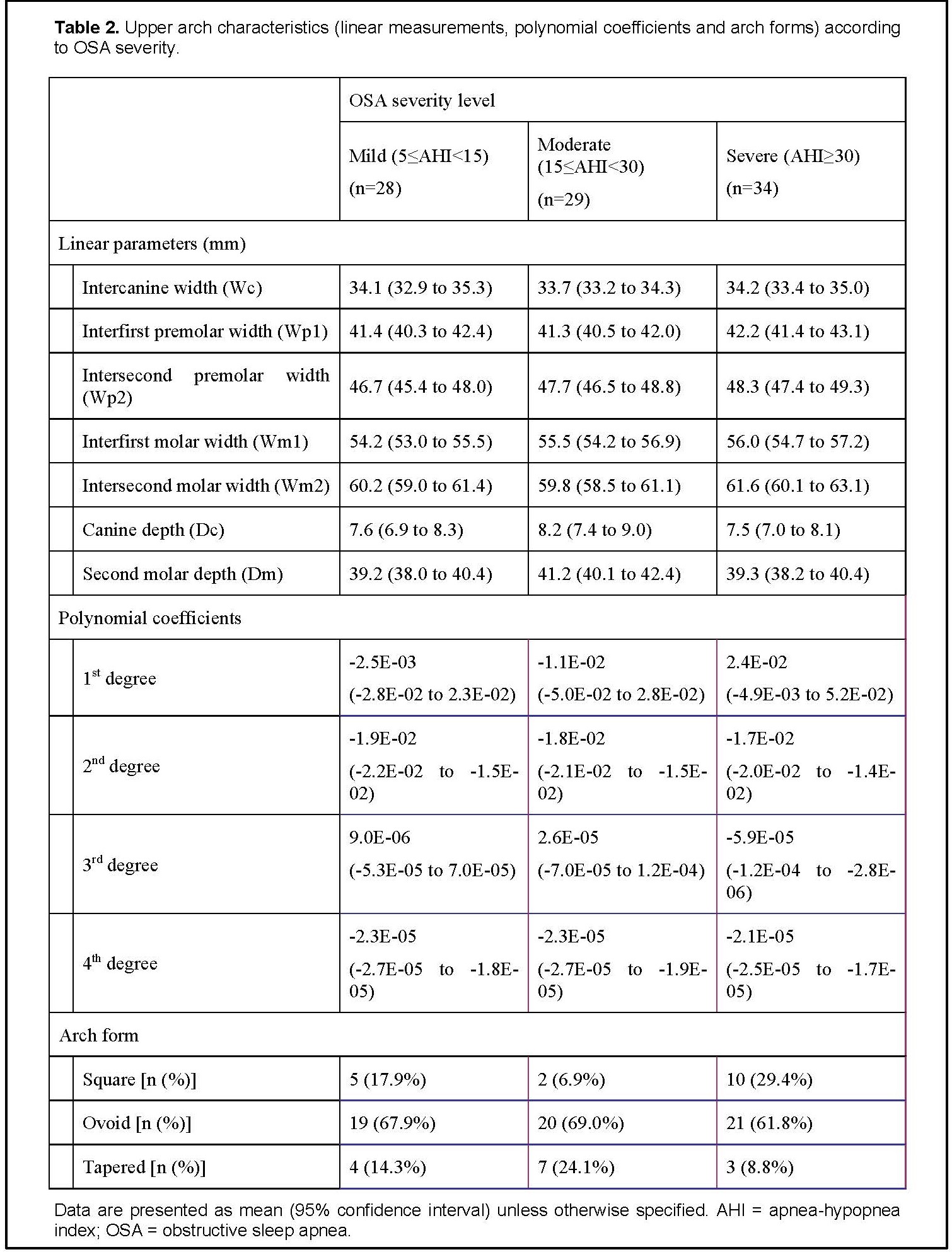
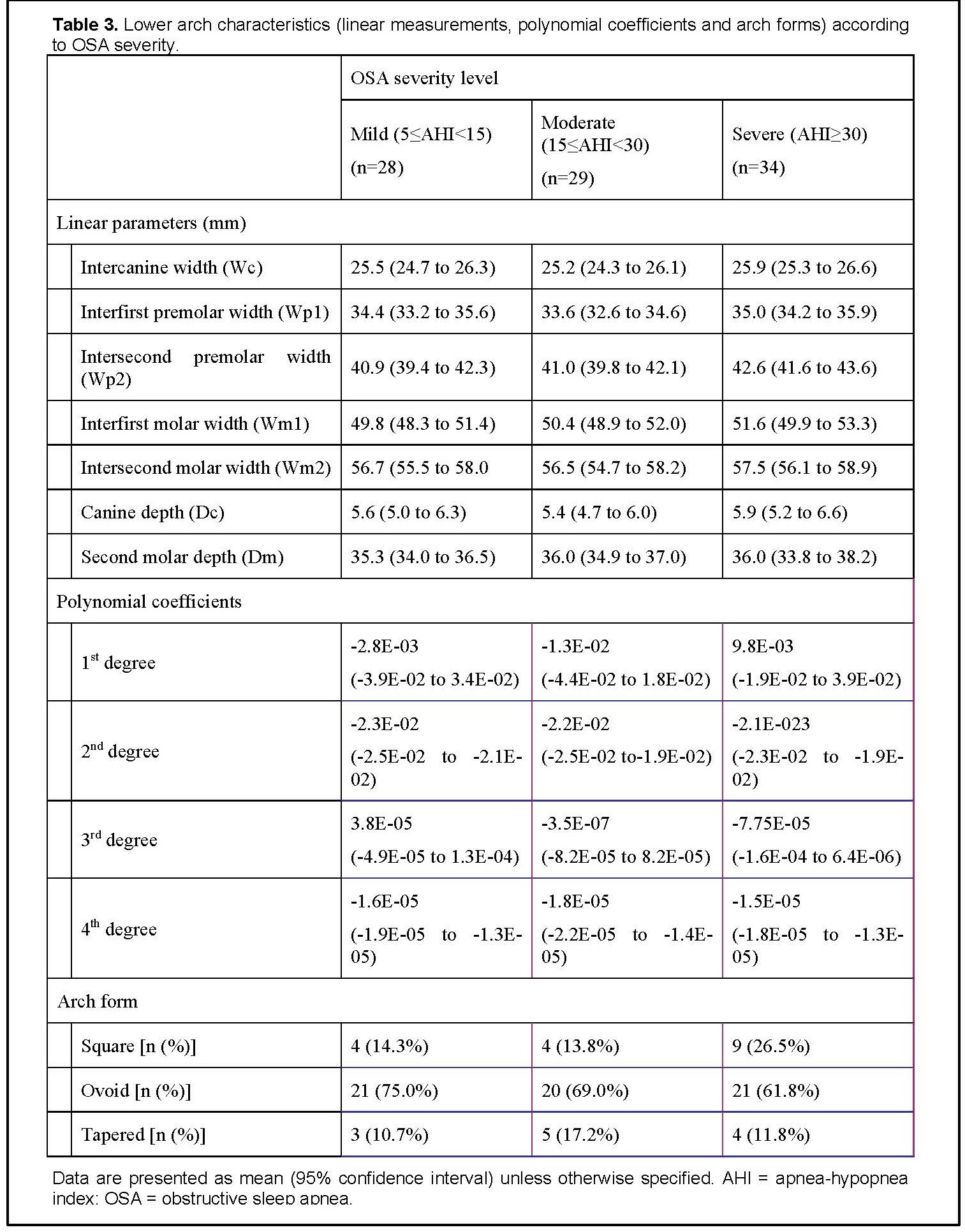
Dental arch characteristics (expressed as linear parameters, polynomial coefficients, and arch forms) according to OSA severity are reported in Table 2 for the upper arch and in Table 3 for the lower arch.
In step one of hierarchical regression, the variance accounted for (R2) by the patients’ general characteristics equaled 0.10, which was significantly different from zero (F(3,86) = 3.201, P=0.027). Among the patients’ general characteristics, only sex was statistically significant (P=0.012). Next, dental parameters (expressed either as linear parameters, polynomial coefficients, or arch forms) were entered into the regression equation. The increase in variance accounted for (ΔR2) by dental parameters was not significant (linear parameters: ΔR2=0.306, ΔF(14,17)=0.842, P=0.623; polynomial coefficients: ΔR2=0.073, ΔF(8,78)=0.857, P=0.556; arch forms: ΔR2=0.027, ΔF(2,84)=1.306, P=0.276).
Method Error and Reliability
The random error, determined using the Dahlberg formula, ranged between 0.17 and 0.59 mm for linear measurements and between 0.08 and 0.24 mm for the BS points coordinates. No systematic error was detected by the paired t-test for any measurements (P>0.05).Satisfactory values were found for interobserver reliability, with the intraclass correlation coefficient ranging between 0.881 and 0.997 for linear measurements and between 0.727 and 0.997 for the BS points coordinates.
Figure 1Definition of the points. a, Reference points used to compute linear measurements: A, the midincisal point of the incisors; B1, B2, the canines’ cusp tips; C1, C2, the buccal cusp tips of the first premolars; D1, D2, the buccal cusp tips of the first premolars; E1, E2, the distobuccal cusp tips of the first molars; F1, F2, the distobuccal cusp tips of the second molars. b, Reference points used to determine dental arch form: bracket slot points (BS points). |
{kind=link}
Figure 2Arch-dimension variables. Wc, intercanine width: distance between the canine cusp tips; Wp1, interfirst premolar width: distance between the first premolar cusp tips; Wp2, intersecond premolar width: distance between the second premolar cusp tips; Wm1, interfirst molar width: distance between the distobuccal cusp tips of the first molars; Wm2, intersecond molar width: distance between the distobuccal cusp tips of the second molars; Dc: canine depth: distance between the contact of the central incisors and a line that connects the canine cusp tips; Dm, second molar depth: distance between the contact of the central incisors and a line that connects the distobuccal cusp tips of the second molars. |
{kind=link}
Figure 3Comparison between patient’s arch form and standard arch forms by using the method of least squares. The red crosses are the bracket slot points; the blue lines are the standard arch forms (square, ovoid, tapered). |
{kind=link}
Table 1 Patients’ demographic and clinical characteristics. |
{kind=link}
Table 2Upper arch characteristics (linear measurements, polynomial coefficients and arch forms) according to OSA severity. |
{kind=link}
Table 3Lower arch characteristics (linear measurements, polynomial coefficients and arch forms) according to OSA severity. |
{kind=link}
DISCUSSION
Several data are available on the craniofacial characteristics of adult patients with OSA and, also, on the relationship between cephalometric parameters and AHI. The evaluation of dental arch morphologic characteristics in patients with OSA has the advantage that radiographic examination is not required but limited and controversial data are available on this topic.
Thus far, narrow maxillary dental arches have been thought to diminish the oropharyngeal volume available for the tongue, therefore being considered a predisposing factor for OSA.29 Few studies have been carried out on the correlation between adult patients’ arch parameters and the presence of OSA, with inconclusive results.19-21,30,31 Methodologic limitations include the use of questionnaires for the screening of OSA for the selection of the control group, whereas the diagnosis of OSA absence should be based on PSG criteria.23 Moreover, the measurements were often taken on bidimensional images and limited to the upper arch. The comparison between patients with and without OSA was usually based on linear measurements (intertooth widths and arch depths) or at most on the polynomial coefficients. Regarding the upper arch, patients with OSA showed significantly narrower inter-tooth widths and a shorter maxillary depth than patients who were nonsnoring and without apnea. 19A study on three-dimensional maxillary dental casts found that patients with OSA had significantly narrower maxilla with smaller intermolar and intercanine widths when compared with control patients.21 Conversely, other authors did not report significant differences in any intertooth distances.20 Patients with Marfan syndrome proved to have a significant reduction of intercanine, inter-first premolar, and interfirst molar widths compared with control patients.30 However, it should be acknowledged that Marfan syndrome is associated with a high prevalence of OSA. The mean upper arch width of the OSA group has also been shown to be narrower in the canine region and wider in the premolar and molar regions when compared to the non-OSA group.31 Moreover, mandibular arches of the OSA group were narrower in the canine region and wider in the premolar and molar areas.31 Looking at width and depth independently is not adequate to evaluate arch form because these parameters are affected by arch size as well as by arch form. To overcome this limitation, arch form could be represented by a mathematical equation. However, only one study compared the maxillary arch forms of patients with and without OSA based on the coefficients of the polynomial curve that best fitted the arch.19 Comparison of the polynomial coefficients indicated that the quadratic coefficient was significantly greater in patients with OSA than in control patients, indicative of greater tapering of the maxillary arch. In a study comparing dental arches of patients with and without OSA through finite-element morphometry it was found that patients with OSA showed 7% to 11% narrower upper arches in the transverse plane in the incisor and canine regions and 10% to 11% narrower lower arches in the anteroposterior plane in the premolar and molar regions.29
If several studies have investigated the association between adult patients’ arch parameters and the presence of OSA, only a few of them analysed whether these parameters and disease severity were correlated. A significant correlation between indexes of maxillary constriction and AHI in patients with Marfan syndrome has been found.30 However, in addition to the limitations of the study highlighted previously, this study did not take into account the effect of potential confounders as was done in the current study. A further study found that a significant yet weak correlation (r=−0.158, P=0.044) existed between the upper dental arch width (defined as the distance between the cusps of the right and left first premolars) and AHI.32 However, only Japanese male patients were included in the study, the correlation between lower dental arch width and AHI was not analysed and the arch width was evaluated only at the first premolar level. Moreover, potential confounders were not considered in the analysis.
Therefore, the current study aimed to overcome the limitations that burdened the studies currently available on this issue, providing a comprehensive analysis of the correlation between adult patients’ arch morphologic characteristics and OSA severity by using three-dimensional cast analysis and reliable mathematical methods and taking into account potential confounders such as sex, age, and BMI. Age and BMI did not prove to be significant predictors of AHI in the current study’s sample of patients with OSA. However, they were included in the final model, regardless of their statistical significance, because the correlation between AHI and both age and BMI has been widely described in the literature.24-26
No significant relationships were found between dental arch parameters and AHI after controlling for sex, age, and BMI neither in the upper arch nor in the lower arch. Therefore, in patients with OSA the relationship between arch form characteristics and disease severity is not so evident. This finding is consistent with other studies on anatomic characteristics of patients with OSA, which showed that various anatomic correlates were poor predictors of OSA prevalence or severity.33-35 A possible explanation for this finding is that, although anatomic characteristics can help determine pharyngeal collapsibility, anatomic factors alone do not cause OSA. In the pathogenesis of OSA nonanatomic factors such as the ability of the upper airway dilator muscles to respond to respiratory challenge during sleep, the propensity to wake from increased respiratory drive during sleep (arousal threshold), and the stability of the respiratory control system (loop gain) also must be taken into account.4 Because several factors can contribute to upper airway collapse during sleep, the extent to which craniofacial skeletal restriction (which could result in narrower dental arches) contributes to the phenomenon of repetitive collapse of the upper airway during sleep probably varies from patient to patient.36 Moreover, the onset and the duration of OSA must be considered because it can greatly affect the morphologic features: because OSA occurring in adults does not affect growth and development, the effect of OSA on the morphology of the hard palate (and consequently on arch form) is not obvious.37 Further studies are needed to properly evaluate this issue; a better characterization of OSA anatomic and pathophysiologic phenotypes is an essential step toward tailored approaches to therapy to ensure treatment effectiveness.38,39
Limitations of the Study
Unavailability of information on confounders can potentially bias the results of retrospective studies. Given the retrospective nature of this study, certain confounding variables that have the potential to affect the outcome may not have been considered or recorded at all (lifestyle factors such as dietary habits, alcohol consumption, cigarette use, and physical activity or abnormalities in either function or position of the tongue). Especially tongue function, posture, and size, which could not be evaluated in this study, should be considered in future studies. It is generally assumed that the alveolar bone responds to external influences: the altered position of the tongue may cause imbalance in the forces, which may result in alteration in the dental arch form. However conflicting reports exist in the pertinent literature about variations in tongue size or posture affecting the characteristics of the maxillary and mandibular dental arches, mainly assessed as transverse linear measurements.40,41
Patients with previous or ongoing orthodontic treatment had to be excluded from the sample to avoid misleading results given by the change in morphology arch parameters determined by orthodontic treatment. However, it is not known what effect the exclusion of patients with very narrow or wide dental arches who had undergone orthodontic treatment may have had on the study results. Moreover, the study patients may not be representative of the population and study results from a larger sample size might be more generalizable to the entire population.
CONCLUSIONS
No significant relationship was found between dental arch morphologic characteristics and AHI after controlling for potential confounders such as sex, age, and BMI, suggesting that dental arch parameters are poor predictors of OSA severity. Further prospective studies conducted on larger sample size could improve the generalization of the results.
ABBREVIATIONS
AHI: apnea-hypopnea index
BMI: body mass index
BS point: Bracket Slot point
OSA: Obstructive sleep apnea
PSG: Polysomnography
REFERENCES
- American Academy of Sleep Medicine. International Classification of Sleep Disorders. American Academy of Sleep Medicine, ed 3. Darien, IL, 2014.
- Sateia MJ. International classification of sleep disorders-third edition: highlights and modifications. Chest. 2014;146(5):1387-1394.
- Epstein LJ, Kristo D, Strollo PJ Jr, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(3):263-276.
- Bosi M, De Vito A, Kotecha B, et al. Phenotyping the pathophysiology of obstructive sleep apnea using polygraphy/polysomnography: a review of the literature. Sleep Breath. 2018;22(3):579-592.
- Owens RL, Edwards BA, Eckert DJ, et al. An integrative model of physiological traits can be used to predict obstructive sleep apnea and response to non positive airway pressure therapy. Sleep. 2015;38(6):961-970.
- Aihara K, Oga T, Harada Y, et al. Analysis of anatomical and functional determinants of obstructive sleep apnea. Sleep Breath. 2012;16(2):473-481.
- Dijemeni E, D'Amone G, Gbati I. Drug-induced sedation endoscopy (DISE) classification systems: a systematic review and meta-analysis. Sleep Breath. 2017;21(4):983-994.
- Hoekema A, Hovinga B, Stegenga B, De Bont LG. Craniofacial morphology and obstructive sleep apnoea: a cephalometric analysis. J Oral Rehabil. 2003;30(7):690-696.
- Stipa C, Cameli M, Sorrenti G, Ippolito DR, Pelligra I, Alessandri-Bonetti G. Relationship between cephalometric parameters and the apnoea-hypopnoea index in OSA patients: a retrospective cohort study. Eur J Orthod. 2020;42(1):101-106.
- Lowe AA, Fleetham JA, Adachi S, Ryan CF. Cephalometric and computed tomographic predictors of obstructive sleep apnea severity. Am J Orthod Dentofacial Orthop. 1995;107(6):589-595.
- Battagel JM, L'Estrange PR. The cephalometric morphology of patients with obstructive sleep apnoea (OSA). Eur J Orthod. 1996;18(6):557-569.
- Sakakibara H, Tong M, Matsushita K, Hirata M, Konishi Y, Suetsugu S. Cephalometric abnormalities in non-obese and obese patients with obstructive sleep apnoea. Eur Respir J. 1999;13(2):403-410.
- Battagel JM, Johal A, Kotecha B. A cephalometric comparison of subjects with snoring and obstructive sleep apnoea. Eur J Orthod. 2000;22(4):353-365.
- Ito D, Akashiba T, Yamamoto H, Kosaka N, Horie T. Craniofacial abnormalities in Japanese patients with severe obstructive sleep apnoea syndrome. Respirology. 2001;6(2):157-161.
- Hui DS, Ko FW, Chu AS, et al. Cephalometric assessment of craniofacial morphology in Chinese patients with obstructive sleep apnoea. Respir Med. 2003;97(6):640-646.
- Johal A, Patel SI, Battagel JM. The relationship between craniofacial anatomy and obstructive sleep apnoea: a case-controlled study. J Sleep Res. 2007;16(3):319-326.
- Tangugsorn V, Skatvedt O, Krogstad O, Lyberg T. Obstructive sleep apnoea: a cephalometric study. Part I. Cervico-craniofacial skeletal morphology. Eur J Orthod. 1995;17(1):45-56.
- Neelapu BC, Kharbanda OP, Sardana HK, et al. Craniofacial and upper airway morphology in adult obstructive sleep apnea patients: A systematic review and meta-analysis of cephalometric studies. Sleep Med Rev. 2017;31:79-90.
- Seto BH, Gotsopoulos H, Sims MR, Cistulli PA. Maxillary morphology in obstructive sleep apnoea syndrome. Eur J Orthod. 2001;23(6):703-714.
- Johal A, Conaghan C. Maxillary morphology in obstructive sleep apnea: a cephalometric and model study. Angle Orthod. 2004;74(5):648-656.
- Kecik D. Three-dimensional analyses of palatal morphology and its relation to upper airway area in obstructive sleep apnea. Angle Orthod. 2017;87(2):300-306.
- Kale SS, Kakodkar P, Shetiya SH. Assessment of oral findings of dental patients who screen high and no risk for obstructive sleep apnea (OSA) reporting to a dental college - A cross sectional study. Sleep Sci. 2018;11(2):112-117.
- Irlandese G, De Stefani A, Mezzofranco L, et al. Dental arch form and interdental widths evaluation in adult Caucasian patients with obstructive sleep apnea syndrome. Cranio. 2020;4:1-9.
- Subramanian S, Hesselbacher S, Mattewal A, Surani S. Gender and age influence the effects of slow-wave sleep on respiration in patients with obstructive sleep apnea. Sleep Breath. 2013;17(1):51-56.
- Zammit C, Liddicoat H, Moonsie I, Makker H. Obesity and respiratory diseases. Int J Gen Med. 2010;3:335-343.
- Borges PD, Filho ES, Araújo TM, et al. Correlation of cephalometric and anthropometric measures with obstructive sleep apnea severity. Int Arch Otorhinolaryngol. 2013;17(3):321-328.
- American Academy of Sleep Medicine. ICSD-2 International Classification of Sleep Disorders. Diagnostic and Coding Manual American Academy of Sleep Medicine, ed 2. Westchester, IL, American Acdemy of Sleep Medicine, 2005.
- Andrews LF. Straight-wire, The Concept and Appliance. San Diego, California, LA Wells, 1989.
- Banabilh SM. Orthodontic view in the diagnoses of obstructive sleep apnea. J Orthod Sci. 2017;6(3):81-85.
- Cistulli PA, Richards GN, Palmisano RG, Unger G, Berthon-Jones M, Sullivan CE. Influence of maxillary constriction on nasal resistance and sleep apnea severity in patients with Marfan's syndrome. Chest. 1996;110(5):1184-1188.
- Nainan O, Jayan B, Mitra R, Ghosh S, Chopra SS, Mukherjee M. Dental arch morphology as a predictor of sleep disordered breathing. Sleep Hypn. 2017;19(2):30-37.
- Maeda K, Tsuiki S, Fukuda T, Takise Y, Inoue Y. Is maxillary dental arch constriction common in Japanese male adult patients with obstructive sleep apnoea? Eur J Orthod. 2014;36(4):403-408.
- Schwab RJ. Upper airway imaging. Clin Chest Med. 1998;19(1):33-54.
- Isono S, Remmers JE, Tanaka A, Sho Y, Sato J, Nishino T. Anatomy of pharynx in patients with obstructive sleep apnea and in normal subjects. J Appl Physiol. 1997;82(4):1319-1326.
- Sforza E, Petiau C, Weiss T, Thibault A, Krieger J. Pharyngeal critical pressure in patients with obstructive sleep apnea syndrome. Clinical implications. Am J Respir Crit Care Med. 1999;159(1):149-157.
- Ryan CM, Bradley TD. Pathogenesis of obstructive sleep apnea. J Appl Physiol. 2005;99(6):2440-2450.
- Yu C, Ahn HW, Kim SH. Three-dimensional morphological evaluation of the hard palate in Korean adults with mild-to-moderate obstructive sleep apnea. Korean J Orthod. 2018;48(3):133-142.
- Cistulli PA, Sutherland K. Phenotyping obstructive sleep apnoea-Bringing precision to oral appliance therapy. J Oral Rehabil. 2019;46(12):1185-1191.
- Alessandri-Bonetti G, Ippolito DR, Bartolucci ML, D'Antò V, Incerti-Parenti S. Cephalometric predictors of treatment outcome with mandibular advancement devices in adult patients with obstructive sleep apnea: a systematic review. Korean J Orthod. 2015;45(6):308-321.
- Primozic J, Farcnik F, Perinetti G, Richmond S, Ovsenik M. The association of tongue posture with the dentoalveolar maxillary and mandibular morphology in Class III malocclusion: a controlled study. Eur J Orthod. 2013;35(3):388-393.
- Fatima F, Fida M. The assessment of resting tongue posture in different sagittal skeletal patterns. Dental Press J Orthod. 2019;24(3):55-63.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted April 12, 2021
Submitted in final revised form March 6, 2022
Accepted for publication March 12, 2022
Address correspondence to: Giulio Alessandri-Bonetti, Department of Biomedical and Neuromotor Sciences (DIBINEM), Section of Orthodontics, University of Bologna, Via San Vitale 59, 40125, Bologna, Italy. Email: giulio.alessandri@unibo.it