Original Article 1, Issue 9.3
Comparison of Three Mandibular Advancement Device Designs in the Management of Obstructive Sleep Apnea: A Retrospective Study
http://dx.doi.org/10.15331/jdsm.7250Linda Sangalli, DDS, MS, PhD; Fernanda Yanez-Regonesi, DDS, MS; Diego Fernandez-Vial, DDS; Andrés Martinez-Porras, DDS; Isabel Moreno-Hay, DDS, PhD
Department of Oral Health Science, Division of Orofacial Pain, University of Kentucky, College of Dentistry, Lexington, Kentucky, USA
ABSTRACT
 |
Study Objectives:
To evaluate the efficacy of three mandibular advancement device (MAD) designs in terms of apnea-hypopnea index (AHI), minimum blood oxygen saturation (min SpO2), and Epworth Sleepiness Scale (ESS) between pretreatment and posttreatment sleep studies for the management of obstructive sleep apnea (OSA). The protrusive range at the time of the second sleep study was correlated with the effectiveness of MAD designs.
Methods:
Retrospective data from 49 patients with OSA referred to the Orofacial Pain Clinic at University of Kentucky (March 2016-March 2021) treated with MAD, with a post-treatment sleep study, were included. Treatment success was defined as 50% improvement in AHI, or as 50% improvement with residual AHI < 10/h.
Results:
Posttreatment AHI improved with Herbst and SomnoDent-Classic (P =.003 and P =.000, respectively). Posttreatment ESS score improved with Herbst, SomnoDent-Classic, and D-SAD designs (P =.004, P = .000, and P =.018, respectively). No differences were found between the three MADs in terms of change in AHI, min SpO2, and ESS (all P >.050). Treatment success was achieved in 59.18% and 48.97%, according to the criteria, with no difference between the appliances and no correlation with the range of protrusion.
Conclusions:
The three MADs were efficacious in improving AHI and ESS, but not min SpO2, in patients with OSA, with no differences between MAD designs. Because some patients showed a worsening in AHI, a posttreatment sleep study is of great importance.
Clinical Implications:
MAD should be selected on an individual basis, according to patient preference and trained dentist recommendation, as the design did not affect the effectiveness in terms of AHI improvement.
Keywords:
obstructive sleep apnea, mandibular advancement device, effectiveness, design
Citation:
Sangalli L, Yanez-Regonesi F, Fernandez-Vial D, Martinez-Porras A, Moreno-Hay, I. Comparison of three mandibular advancement device designs in the management of obstructive sleep apnea: A retrospective study. J Dent Sleep Med. 2021;9(3)
INTRODUCTION
Obstructive sleep apnea (OSA) is the most common sleep-related breathing disorder, with a prevalence varying from 10% to 17% in male and from 3% to 9% in female adults.1 Treatment options for OSA include behavioral modification such as weight loss and alcohol avoidance, positional therapy,2 surgical intervention, hypoglossal nerve stimulation,3 pharmacologic regimen,4 continuous positive airway pressure (CPAP), and oral appliances (OAs). CPAP therapy is considered the gold standard for the management of OSA, particularly in severe OSA disease.5,6 Routine CPAP use remains problematic for some patients, due to mask discomfort, claustrophobia, pressure intolerance, noise, nasal congestion, rhinorrhea, eye irritation, sense of suffocation, and lifestyle or social considerations.7 Unfortunately, its effectiveness is highly dependent on patient adherence, which accounts for 4 hours/night on average.8
OAs are recognized as an effective alternative treatment in the management of mild to moderate OSA, primary snoring, or in case of lack of tolerance to the CPAP machine.9 OAs intend to protrude and stabilize the mandible to maintain a patent airway during sleep.9
Among OAs, mandibular advancement devices (MADs) are the most commonly prescribed in the management of OSA. Several studies have shown that despite the inferior efficacy of MAD compared to CPAP in reduction of apnea-hypopnea index (AHI), both treatments are similar in terms of effectiveness, because the suboptimal efficacy of MAD therapy is counterbalanced by the higher compliance of the patients.10 Likewise, MADs are more effective than other types of OAs in managing OSA.11 A systematic review by Ahrens et al. found that all MADs improved polysomnographic indices when compared with inactive appliances,12 and custom-made monobloc MADs were found to be more effective than thermoplastic monobloc MADs.13 This suggests that the characteristics of MAD design can affect effectiveness.
To the best of the authors’ knowledge, only a few studies in the literature assessed the difference in effectiveness between the MAD designs, with conflicting outcomes: Verburg et al. found no significant difference between Somnodent-Flex and Herbst designs14 and two studies found no difference between Herbst and Twin Block designs.15,16 Interestingly, Gauthier et al. found that the Silencer design was more effective than the Klearway design,17 and Rose et al. found that the Karwetzky activator produced a higher reduction in respiratory disturbance index compared to the Silencor design.18
The aim of the study was to evaluate the efficacy of three different MAD designs, by comparing pretreatment and posttreatment sleep study, in terms of AHI, minimum blood oxygen saturation (min SpO2), and Epworth Sleepiness Scale (ESS) score. It was hypothesized that the MAD design would not have a significant effect on the efficacy of OSA management. A secondary aim was to evaluate whether the protrusive range at which MAD was set at the time of the second sleep study was correlated with the efficacy of the different MAD designs.
MATERIALS AND METHODS
Subjects
In this retrospective study, data were analyzed for all consecutive patients between March 2016 and March 2021, referred to the Orofacial Pain Clinic at the University of Kentucky by a sleep physician for the management of OSA with a MAD. The included patients presented with a diagnosis of OSA confirmed by a sleep study (polysomnography [PSG] or home sleep apnea test [HSAT] (mild 5/h ≤ AHI < 15/h, moderate 15/h ≤ AHI < 30/h, severe AHI ≥ 30/h), and had undergone a second posttreatment sleep study (PSG or HSAT prescribed, interpreted, and approved by a certified sleep physician) performed with MAD in situ, after obtaining a maximum subjective improvement or the maximum range of protrusion.
Data Collection
Patients' demographic data, medical records, and sleep parameters were collected.
Primary outcome measures:
- Efficacy of MADs, assessed by comparing AHI and min SpO2 values at pretreatment and at posttreatment study with MAD.
- ESS, recorded at baseline before MAD delivery and on the follow-up visit before the posttreatment study with MAD. Total score ranges from 0 to 24, with higher value indicating greater daytime sleepiness.
Secondary outcome measures:
- Treatment success, established using two different criteria: first criterion was established as 50% reduction in AHI, with residual AHI < 10/h; second criterion was established as 50% reduction in AHI.
- Treatment failure, defined as an increase of AHI after MAD therapy.
- Range of protrusion, percentage of appliance advancement after reaching the maximum subjective improvement, or the maximum range of protrusion.
- Subjective improvement, measured via questionnaire with visual analog scale and expressed as a percentage ranging from “no improvement at all” (0%) to “maximum possible improvement” (100%); it was recorded during the follow-up appointment prior to the posttreatment study.
Appliances
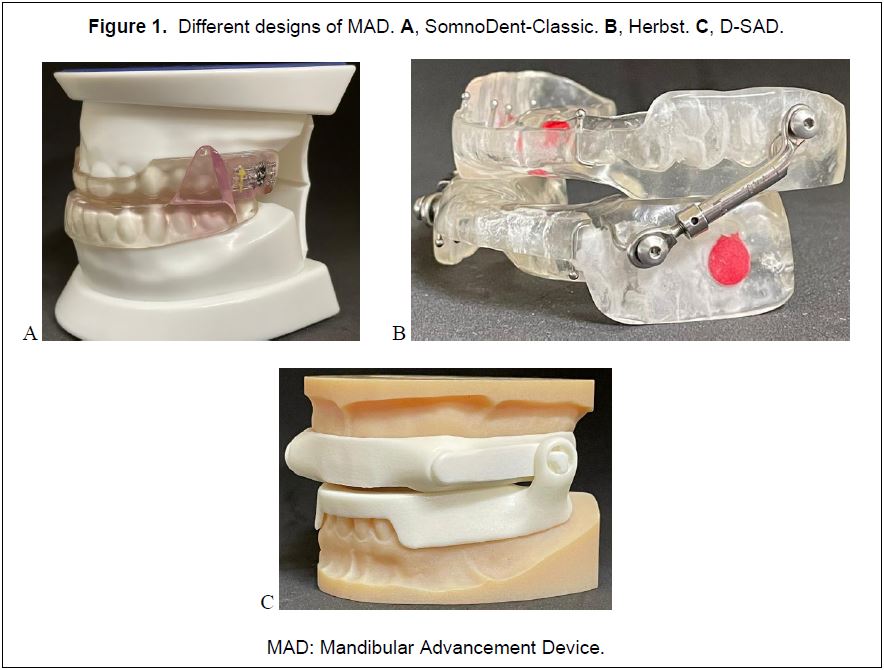
Three US Food and Drug Administration-approved commercially produced MADs were used: Herbst (Great Lakes, Tonawanda, NY, USA), SomnoDent-Classic (SomnoMed, Sydney, Australia) and D-SAD (Panthera Dental, Quebec, QC Canada) appliances (Figure 1). All three designs are duo bloc, customized, titratable OAs that fulfill the criteria of adjustability of mandibular protrusion, and limited lateral and vertical mandibular movement during sleep.19 Each design presents a different attachment and propulsion mechanism. Herbst is characterized by an attached bilateral compression (bilateral push), SomnoDent-Classic by an unattached bilateral interlocking, and D-SAD by an attached bilateral traction (bilateral pull). Appliance selection was determined based on the preference of the clinician and the patient. The initial protrusion was established between 60% and 70% of the maximum protrusion, and subsequent advancements were performed progressively every 2 weeks based on the patient’s tolerance. Once the maximum anatomic protrusion or the maximum therapeutic benefit at 100% subjective improvement were attained, the patient was referred to the sleep physician for reevaluation of the MAD effectiveness.Statistical Analysis
Normality of distribution was tested with the Shapiro-Wilk test. Assumption of homogeneity of variances was verified with the Levene test. Normally distributed continuous variables are presented as mean ± standard deviation.
Herbst, SomnoDent-Classic, and D-SAD appliances were categorized as independent variables; AHI, min SpO2, and ESS values were dependent variables. Paired samples t-test was used to compare pretreatment (T0) and posttreatment (T1) dependent variables for each appliance.
Pearson correlation was used to examine the correlation between reported subjective improvement and range of titration, reported subjective improvement and posttreatment AHI, posttreatment ESS and posttreatment AHI, and treatment success and severity of pretreatment AHI.
One-way analysis of variance (normally distributed variables) was performed to compare the appliance designs in terms of change in min SpO2, treatment success, and treatment worsening. The Kruskal-Wallis test (skewed variables) was used to assess the difference between appliance design and efficacy, and change in posttreatment ESS. Significance level was set at α = 0.05. Data were analyzed with SPSS software (IBM SPSS Statistics for Macintosh, Version 27.000, IBM Corp, Armonk, NY).
RESULTS
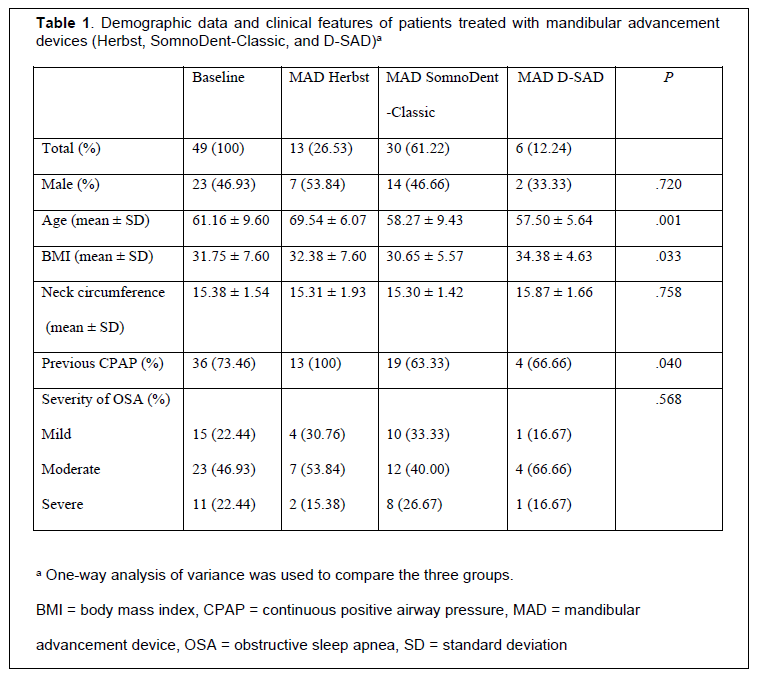
Forty-nine patients met the inclusion criteria and were included in the study. Demographic data and clinical features are presented in Table 1. Thirteen patients (26.53%) received Herbst, 30 (61.22%) SomnoDent-Classic, and 6 (12.25%) the D-SAD appliance. Patients treated with the Herbst appliance were older compared to the other two groups, and none of them could tolerate a previous CPAP therapy (P < 0.05) (Table 1).
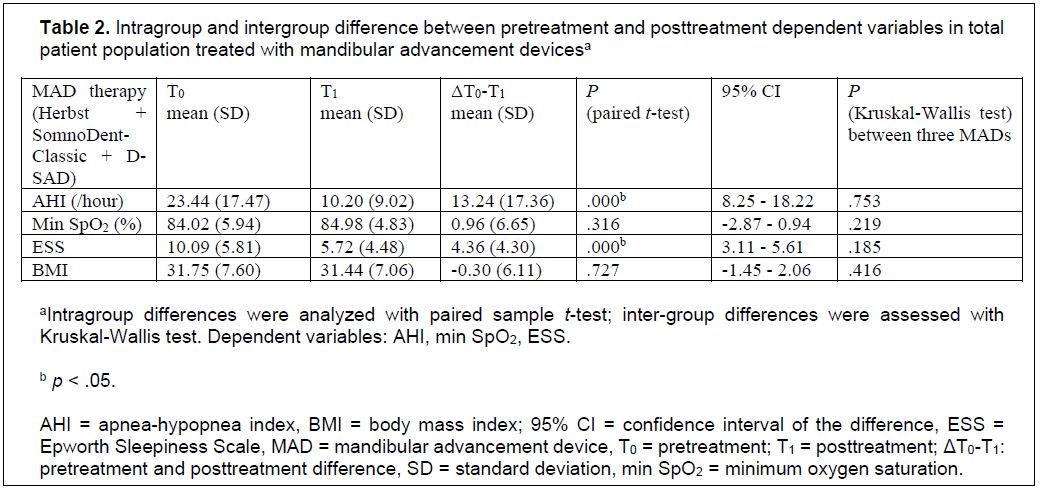
Patients’ body mass index decreased by 0.30 kg/m2 ± 6.11 during the observation period, although it was not statistically significant (P = .727, 95% CI -1.45 - 2.06) (Table 2).
Treatment Efficacy
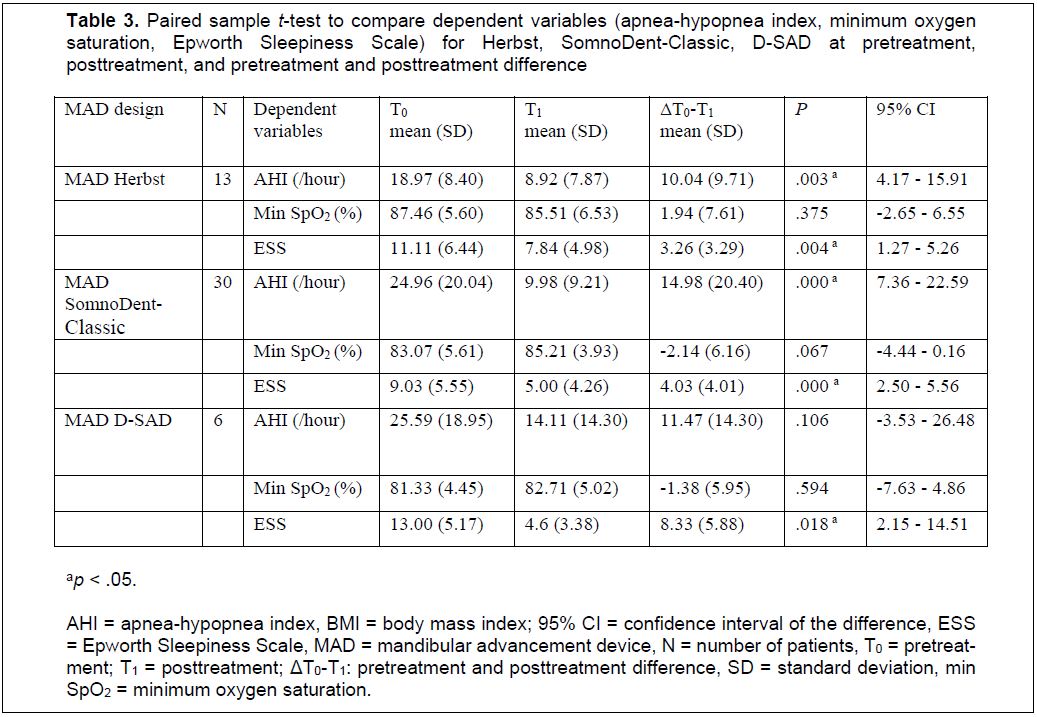
Mean baseline AHI was 23.44 ± 17.47 (range, 6 to 88 events/h) (Table 2). An overall decrease in AHI by 13.24 ± 17.36 was noted, with a residual AHI with MAD of 10.20 ± 9.02 (95% CI 8.25 - 18.22). The difference between AHI at baseline and residual AHI with MAD was statistically significant (P = .000). The Kruskal-Wallis test revealed no statistically significant difference between the three appliance designs (P = .753) (Table 2). AHI improvement was statistically significant for Herbst and SomnoDent-Classic (P = .003, P = .000, respectively), and not statistically significant for D-SAD (P = .106) (Table 3).
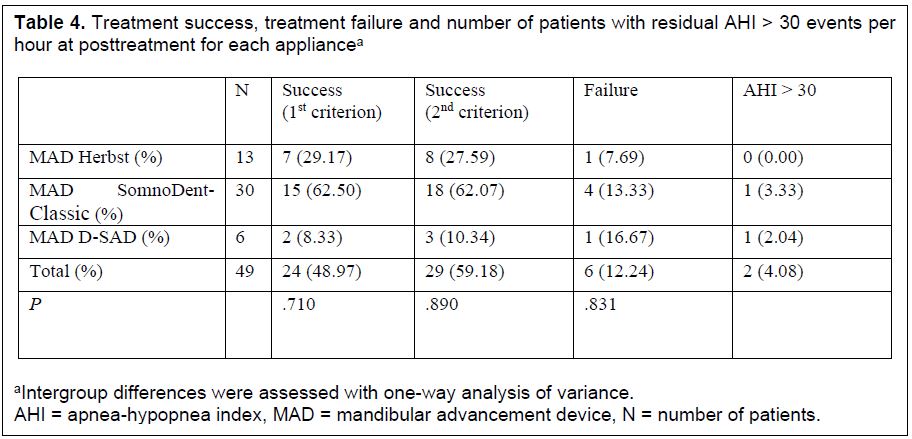
Treatment success, defined as 50% improvement with residual AHI < 10, was achieved in 24 patients (48.97%): 7 with Herbst (29.17%), 15 with SomnoDent-Classic (62.50%), and 2 with D-SAD (8.33%). Treatment success, defined as 50% improvement in AHI, was achieved in 29 patients (59.18%): 8 with Herbst (27.59%), 18 with SomnoDent (62.07%), and 3 with D-SAD (10.34%). No statistically significant difference was found between the three appliance designs, according to both criteria (F(2,46), = .117, P = .890 and F(2,46), = .345, P = .710, respectively). Treatment success was not correlated with baseline severity of OSA (r(48) = -.128, p = .427).
The mean percentage of protrusion obtained at the end of titration was 91.77% of the maximum anatomic protrusion: 91.65% with Herbst, 90.74% with SomnoDent-Classic, and 93.87% with D-SAD. There was no statistically significant correlation between range of protrusion and treatment success (r(45) = -.049, P = .747), and posttreatment ESS (r(45) = .175, P = .250).
Treatment worsening was noted in 6 patients (12.24%), with no statistically significant difference between the appliances (F(2,46) = .186, P = .831), and no correlation with body mass index change (r(49) = -.009, P = .952) (Table 4).
Minumum Oxygen Saturation
Change in mean min SpO2 was not statistically significant, from a baseline of 84.02 ± 5.94 to a posttreatment value of 84.98 ± 4.83 (P = .316) (Table 2). No significant difference in change of min SpO2 at T1 was found between the three appliances (F(2, 64) = .808, P = .219). Min SpO2 changed by 2.14 ± 6.21 (P = .067) with SomnoDent-Classic, by 1.38 ± 5.95 (P = .594) with D-SAD, and by -1.94 ± 7.61 with Herbst (P = .375) (Table 3).
Epworth Sleepiness Scale
Overall, ESS statistically reduced in all three groups by an average of 4.36 ± 4.48, to a mean value of 5.72 ± 4.48 secondary to MAD therapy (p = .000). No significant difference was found between the different designs (p = .185) (Table 2 and 3).Posttreatment ESS was not statistically significantly correlated with residual AHI (r(48) = -.146, P = .322), nor with subjective improvement (r(45) = -.183, P = .228).
Subjective Improvement
Subjective improvement (81.25% with Herbst, 83.08% with SomnoDent-Classic, and 90.00% with D-SAD) was not statistically significantly correlated with range of protrusion (r(42) = .092, P = .564), nor with residual AHI (r(45) = .083, P = .590).
Figure 1Different designs of MAD. A, SomnoDent-Classic. B, Herbst. C, D-SAD. |
{kind=link}
Table 1Demographic data and clinical features of patients treated with mandibular advancement devices (Herbst, SomnoDent-Classic, and D-SAD). |
{kind=link}
Table 2Intragroup and intergroup difference between pretreatment and posttreatment dependent variables in total patient population treated with mandibular advancement devices. |
{kind=link}
Table 3Paired sample t-test to compare dependent variables (apnea-hypopnea index, minimum oxygen saturation, Epworth Sleepiness Scale) for Herbst, SomnoDent-Classic, D-SAD at pretreatment, posttreatment, and pretreatment and posttreatment difference. |
{kind=link}
Table 4Treatment success, treatment failure and number of patients with residual AHI > 30 events per hour at posttreatment for each appliance. |
{kind=link}
DISCUSSION
The results of this study revealed no difference between the three MAD designs in terms of AHI, min SpO2, and ESS values. All of them were efficacious in improving AHI and ESS posttreatment, whereas the change in min SpO2 was negligible and not statistically significant.
Treatment Efficacy
This study analyzed three custom titratable OAs, reported in the literature to obtain better outcomes in AHI compared to noncustom OAs,20 with a mean reduction of 13.89 events/h compared to a mean reduction of 6.28 events/h.21
In accordance with the findings of 34 randomized controlled trials,10 the current study revealed a statistically significant difference between pretreatment and posttreatment AHI, with a mean AHI reduction by 13.24 ± 17.36 events/h, comparable with studies in the literature (mean reduction by 13.60 events/h).19
Interestingly, the decrease in posttreatment AHI was significant for patients treated with SomnoDent-Classic and Herbst appliances but not with D-SAD. This lack of significant difference can be attributed to the small number of patients treated with D-SAD.
No significant difference was found between the three appliances with respect to improvement in AHI. This result is in accordance with a wide body of the literature, which supported the findings that MAD effectiveness is generally independent of design features.11 Verburg et al. found no difference between 67 patients treated with Somnodent-Flex and 70 patients treated with Herbst (P = .608).14 Similarly, Bloch et al. compared Monobloc, Herbst, and a control appliance, revealing that treatment with MAD was significantly more effective than a control appliance, and that Monobloc was more effective than Herbst, although the difference was not significant.15 Likewise, Lawton et al. found no significant difference between Herbst and Twin Block (p = .071), with both improving AHI.16 Conversely, a study by Rose et al. reported a higher effectiveness of the Karwetzky activator compared with Silencor (P < .010), although the two appliances differed not only on design but also on vertical and sagittal dimension.18 This confirmation has a direct influence on patient management in an everyday clinical setting. Indeed, if a precise MAD design was found to be more effective than another, the clinical decision would have been driven by this evidence. Instead, the results of the study suggest that the treatment should be tailored based on individual needs and personal preference, also considering the crucial role of the compliance of the patient in the success rate. The adoption of a precise design can take into consideration other clinical conditions, such as the presence of parafunctional activities (grinding), absent or tilted posterior teeth, and crowded anterior teeth.22
Minimum Oxygen Saturation
The literature reported a modest improvement in min SpO2 in patients with OSA treated with OAs, with a mean value of 3.09% in a weighted analysis of 22 randomized controlled trials.19 The values vary across the studies, with the greatest improvement reported by Hoekema et al., with min SpO2 increasing by 13%.11
On the contrary, in accordance with some other reports,7,8 the current study did not show a statistically significant change in min SpO2 with MAD. Interestingly, the Herbst population revealed a decrease in min SpO2 by 1.94 ± 7.61 posttreatment, although this difference was not significant. Similarly, the change achieved with SomnoDent-Classic and D-SAD (2.14 ± 6.16 and 1.38 ± 5.95, respectively) did not reach the significance level. Concordant with the literature,17,23 no significant difference was found by comparing appliance design and min SpO2. The explanation of Lawton et al. suggests that the arterial blood SpO2 level may be influenced by other factors, including supine sleeping position, individual low hematocrit, and heart failure.23
Epworth Sleepiness Scale
The ESS, an 8-item questionnaire assessing daytime sleepiness,24 has been shown to be positively correlated with OSA severity.24 The current study found a statistically significant improvement in daytime sleepiness between pretreatment and posttreatment values, with the greatest change in the group treated with D-SAD. The reduction in ESS by 4.36 was slightly higher than what was reported by a meta-analysis, where the mean reduction was 3.81.19 However, the effect on daytime sleepiness is uncertain, particularly in patients within the mildest spectrum of disease severity and in snorers, as some studies did not observe any significant improvements in daytime sleepiness when compared to placebo.25
The current study corroborates the findings of other reports17,23 in that the improvement in ESS is not influenced by MAD design. This suggests that the crucial factor may be the mandible protrusion rather than the distinctive propulsion mechanism of the different designs.
Treatment Success
The definition of treatment success is variable in the literature and the success rate of OSA treatment with MAD can vary remarkably according to success criteria.26 Hence, two sets of criteria, normally accepted as a cutoff across studies,27 were applied to effectively differentiate between success and failure.
When treatment success was defined as 50% improvement with residual AHI < 10, MAD was successful in treating 24 patients (48.97%), which is in line with the range of 30% to 94% reported by a systematic review.28 When treatment success was defined as 50% reduction in AHI, it was achieved in 29 patients (59.18%), in accordance with a meta-analysis that reported greater than 50% AHI reduction in 23 of the 25 randomized controlled trials included.19 However, the broad variability of effectiveness suggests the lack of good and consistent predictors of successful MAD treatments. In the literature, treatment success has been correlated with degree of protrusion,29 and inversely related to disease severity.26 However, the current study did not find any correlation between range of protrusion and treatment success. Interestingly, the most protruded position was achieved in the D-SAD group (i.e., protrusion of 93.87%), which actually coincided with a nonstatistical improvement in post-treatment AHI. However, a larger sample size is warranted to replicate these results.
The sample of this retrospective analysis showed a heterogeneity disease severity at baseline: most of the patients exhibited moderate OSA (46.93%), for which MAD is recognized as an effective treatment. Nevertheless, MAD therapy obtained promising results also in the group of patients with severe OSA (22.44%), considering that only 2 patients (4.08%) had residual severe AHI in the posttreatment study. Surprisingly, the most relevant improvements in AHI were found in 4 patients with severe OSA. The most impressive case was a patient with a baseline AHI of 88 events/h, which reduced to 5 events/h after treatment.
This study confirmed the unpredictability of treatment success secondary to MAD;30 indeed, not appliance design, range of protrusion, or pretreatment OSA severity could predict treatment success.
Moreover, for those patients who cannot tolerate CPAP therapy (73.46% in this study), MAD may constitute a valuable and encouraging option, beside surgical and pharmacologic treatments. In addition to the objective reduction in AHI with MAD, ultimately the goal of OSA therapy is to improve daytime somnolence, sleep quality, and overall quality of life,30 and at the same time to reduce health risks, including those related to cardiovascular function and neurocognitive behavior.9
Importance of a Second Sleep Study
This study revealed some cases of AHI worsening following MAD therapy, even if the patients reported a subjective improvement. The percentage of treatment worsening AHI was 12.24%, in line with the 14% reported in the literature.30 A 12.24% reported treatment worsening AHI is a noteworthy finding. However, the current analysis did not reveal any significant confounding factors, such as appliance design, body mass index, or OSA severity. Use of drug-induced sleep endoscopy before embarking on a specific OSA treatment might help identifying good responders to OA therapy.31
These results suggest that prescribing a second sleep study is therefore essential, as PSG-based definitions of success and subjective improvement reported by the patient do not always coincide. Thus, if the end of titration is exclusively driven by subjective feedback, the patient may remain sub-optimally treated.
Strengths and Limitations of the Study
The current study is the first to compare three commercially available appliances, which differ in propulsion mechanism, design, and attachment, by comparing polysomnographic parameters at baseline and with MAD in situ.
The current study is not exempt from some limitations:
- Small and heterogeneous sample size, especially in the group treated with the D-SAD appliance due to the recent commercialization of the design.
- No power analysis nor randomization, due to the retrospective design of the study, which resulted in unequal distribution of subjects to different appliance designs.
- Heterogeneous disease severity at baseline.
- Heterogeneity in age distribution among the appliance designs due to insurance coverage. Patients older than 65 years were usually limited to the Herbst design.
- No placebo group; however, MAD effectiveness in reducing apneic events and improving subjective daytime sleepiness is well established in the literature compared to placebo.7
- Because of the retrospective nature of this study, the device used to assess sleep parameters at baseline and with the MAD in situ varied among patients. All sleep studies were prescribed and interpreted by the treating certified sleep physician, as recommended by American Academy of Sleep Medicine.32 However, it should be taken into consideration that HSAT and PSG have different specificity and sensitivity.
CONCLUSIONS
The three MAD designs demonstrated to be similarly efficacious in the improvement of AHI and ESS scores in the management of OSA, and to not differ in terms of change in min SpO2. Based on the results on this study, some patients showed a worsening in AHI with MAD; therefore, a posttreatment sleep study is of great importance to assess MAD efficacy.
ABBREVIATIONS
OSA: obstructive sleep apnea
MAD: mandibular advancement device
AHI: apnea-hypopnea index
ESS: Epworth Sleepiness Scale
Min SpO2: minimum oxygen saturation
CPAP: continuous positive airway pressure
OAs: oral appliances
PSG: polysomnography
HSAT: home sleep apnea test
REFERENCES
- Peppard PE, Young T, Barnet J, Palta M, Hagen EW, Hla KM. Increased prevalence of Sleep-Disordered Breathing in Adults. Am J Epidem.2013;177:1006-1014.
- Shneerson J, Wright J. Lifestyle modification for obstructive sleep apnoea. Cochrane Database Syst Rev.2001;CD002875.
- Surdaram S, Bridgman SA, Lim J, Lasserson TJ. Surgery for obstructive sleep apnea. Cochrane Database System Rev.2005;CD001004.
- Smith I, Lasserson TJ, Wright J. Drug therapy for obstructive sleep apnoea in adults. Cochrane Database System Rev.2006;CD003002.
- Basner RC. Continuous positive airway pressure for obstructive sleep apnea. N Engl J Med.2007;356;1751-1758.
- Genna F, Lopomo NF, Savoldi F. Validation of a numerical model for the mechanical behavior of a continuous positive airway pressure mask. Comp Method Biomechan Biomed Engineer. 2021;1-11.
- Ferguson KA, Ono T, Lowe AA, al-Majed S, Love LL, Fleetham JA. A short-term controlled trial of an adjustable oral appliance for the treatment of mild to moderate obstructive sleep apnoea. Thorax.1997;52:362-368.
- McEvoy RD, Antin NA, Heeley E. et al. CPAP for prevention of cardiovascular events in obstructive sleep apnea. N Engl J Med.2016;375:919-931.
- Scherr SC, Dort LC, Almeida FR, et al. Definition of an effective oral appliance for the treatment of obstructive sleep apnea and snoring: a report of the Amercan Academy of Dental Sleep Medicine. JDSM.2014;1:39-50.
- Sutherland K, Philips CL, Cistulli PA. Efficacy versus effectiveness in the Treatment of Obstructive Sleep Apnea: CPAP and Oral Appliance. JDSM.2015; 2:175-181.
- Hoekema A, Stegenga B, De Bont LG. Efficacy and co-morbidity of oral appliances in the treatment of obstructive sleep apnea-hypopnea: a systematic review. Crit Rev Oral Biol Med.2004;15:137–155.
- Ahrens A, McGrath C, Hagg U. A systematic review of the efficacy of oral appliance design on the management of obstructive sleep apnoea. Eur J Orthod. 2011;33:318-324.
- Vanderveken OM, Devolder A, Marklund M, et al. Comparison of a custom-made and a thermoplastic oral appliance for the treatment of mild sleep apnea. Am J Respir Crit Care Med.2008;1978:197-202.
- Verburg FE, Bollen KHA, Donker HJ, Kramer GJC. The effectiveness of two types of MADS for OSA therapy. Clin Oral Invest.2018;22:1995-2003.
- Bloch KE, Iseli A, Zhang JN, Kaplan V, Stoeckli PW, Russi EW. A randomized, controlled crossover trial of two oral appliances for sleep apnea treatment. Am J Respir Crit Care Med.2000;162:246-251.
- Lawton HM, Battagel JM, Kotecha B. Effect of two types of mandibular advancement splints on snoring and obstructive sleep apnoea. Eur J Orthod. 2005;27:82-90.
- Gauthier L, Laberge L, Beaudry M, Laforte M, Rompré PH, Lavigne GJ. Efficacy of two mandibular advancement appliances in the management of snoring and mild-moderate sleep apnea: a cross-over randomized study. Sleep Med. 2009;10:329-336.
- Rose E, Staats R, Virchow C, Jonas IE. A comparative study of two mandibular advancement appliances for the treatment of obstructive sleep apnoea. Eur J Orthod. 2002;24:191-198.
- Ramar K, Dort LC, Katz SG, et al. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015. J Clin Sleep Med.2015;11:773-827.
- Aarab G, Lobbezoo F, Hamburger HL, Nawjie M. Oral appliance therapy versus nasal contrinuous positive ariway pressure in obstructive sleep apnea: a randomized, placebo-controlled trial. Respiration. 2011;81:411-419.
- Ferguson KA, Ono T, Lowe AA, Keenan SP, Fleetham JA. A randomized crossover study of an oral appliance vs nasal-continuous positive airway pressure in the treatment of mild-moderate obstructive sleep apnea. Chest. 1996;109:1269-1275.
- Bartolucci ML, Bortolotti F, Corazza G, Incerti Parenti S, Paganelli C, Alessandri Bonetti G. Effectiveness of different mandibular advancement device designs in obstructive sleep apoea therapy: a systematic review of randomised controlled trials with meta-analysis. J Oral Rehab.2021;48:469-486.
- Lawton HM, Battagel JM, Kotecha B. A comparison of the Twin Block and Herbst mandibular advancement splints in the treatment of patients with obstructive sleep apnoea: a prospective study. Eur J Orthod. 2005;27:82–90.
- Johns MW. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep.1991;14:540-45.
- Marklund M, Carlberg B, Forsgren L, Olsson T, Stenlund H, Franklin KA. Oral appliance therapy in patients with daytime sleepiness and snoring or mild to moderate sleep apnea: a randomized clinical trial. JAMA Intern Med. 2005;175:1278-1285.
- Fukuda T, Tsuiki S, Kobayashi M, Nakayama H, Inoue Y. Selection of response criteria affects the success rate of oral appliance treatment for obstructive sleep apnea. Sleep Med.2014;15:367-370.
- Sutherland K, Vanderveken OM, Tauda H, et al. Oral appliance treatment for obstructive sleep apnea: an update. J Clin Sleep Med.2014;10:215-227.
- Wenyang L, Lin X, Jing H. The comparison of CPAP and oral appliances in treatment of patients with OSA: a systematic review and meta-analysis. Respir Care. 2013;58:1184-1195.
- Tegelberg A, Wilhelmsson B, Walker-Engstrom ML, et al. Effects and adverse events of a dental appliance for treatment of obstructive sleep apnea. Swed Dent J. 1999;23:117-126.
- Sutherland K, Cistulli PA. Oral appliance therapy for obstructive sleep apnoea: state of the Art. J Clin Med. 2019;8:2121.
- Dijemeni E, D’Amone G, Gbati I. Drug-induced sedation endoscopy (DISE) classification systems: a systematic review and meta-analysis. Sleep Breath. 2017;21:983-994.
- Caples SA, Anderson WM, Calero K, Howell M, Hashmi SD. Use of polysomnography and home sleep apnea tests for the longitudinal management of obstructive sleep apnea in adults: an American Academy of Sleep Medicine clinical guidance statement. J Clin Sleep Med.2021;17:1287-1293.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted June 7, 2021
Submitted in final revised form November 29, 2021
Accepted for publication January 5, 2022
Address correspondence to: Linda Sangalli, DDS, MS, PhD, Department of Oral Health Science, Division of Orofacial Pain, University of Kentucky, College of Dentistry. 740 S. Limestone, Lexington KY 40536, USA Email: lsa276@uky.edu