Original Article 1, Issue 9.2
Association of Sleep Disordered Breathing With Oral Health Findings in Children
http://dx.doi.org/10.15331/jdsm.7236Michelle DaRocha, DMD1, 2; Jacy Stauffer, DMD 1, 2; Donna Kritz-Silverstein, PhD 3, 4; Rakesh Bhattacharjee, MD 5
1 San Ysidro Health, Children’s Dental Center at Rady Children’s Hospital, San Diego, California; 2 NYU Langone Dental Medicine – California South, Department of Pediatric Dentistry, San Diego, California; 3 Herbert Wertheim School of Public Health and Longevity Science, University of California San Diego, La Jolla, California, 4 Professor of Epidemiology, Department of Family Medicine, School of Medicine, University of California San Diego, La Jolla, California; 5Associate Professor of Clinical Pediatrics, Division of Respiratory Medicine, Department of Pediatrics, Rady Children's Hospital-San Diego, University of California San Diego, San Diego, California
ABSTRACT
Study Objectives:
This study examines the association of symptoms of sleep disordered breathing (SDB) with specific oral health indicators in children.
Methods:
Between August-December 2018, 151 children aged 1 to 14 years were recruited by a pediatric dental resident during a dental appointment. The Sleep-Related Breathing Disorder scale of the Pediatric Sleep Questionnaire (SRBD-PSQ) was used to screen for SDB. Demographic information, medical history, and clinical parameters (Brodsky score for tonsillar hypertrophy, bruxism, dental malocclusion, mouth breathing, non-nutritive sucking habits, previous tonsillectomy, and dental crowding) were assessed by a dentist blinded to the child’s SRBD-PSQ score.
Results:
Mean age ± standard deviation was 7.8 ± 2.7 years; 53% were female. Based on body mass index percentile, 11% were overweight, 24% had obesity, and 52% were of healthy weight. SRBD-PSQ scores ranged from 0 to 18 (mean ± standard deviation =5.4 ± 3.9). Linear regression analyses adjusted for age, sex, and body mass index showed that Brodsky score I, II, III/IV versus 0 for tonsils was negatively associated with SRBD-PSQ score (P = 0.04, P = 0.01, P = 0.04, respectively), whereas bruxism, mouth breathing, and prior tonsillectomy were positively associated with SRBD-PSQ score (Ps<0.01). The Angle classification of first permanent molar relationship, attention deficit hyperactivity disorder, non-nutritive sucking habits, and dental crowding were not associated with SRBD-PSQ score. Associations were stronger for children older than 7 years.
Conclusions:
Dental clinical parameters including bruxism, mouth breathing, and a history of tonsillectomy were associated with higher SRBD-PSQ scores.
Clinical Implications:
Specific oral health assessment characteristics elicited on a dental examination may be associated with the SRBD-PSQ, placing dentists in an important position to screen for SDB.
Keywords:
obstructive sleep apnea; oral health; pediatric sleep; pediatric sleep questionnaire; sleep disordered breathing; pediatric dentistry
Citation:
DaRocha M, Stauffer J, Kritz-Silverstein D, Bhattacharjee R. Association of sleep disordered breathing with oral health findings in children. J Dent Sleep Med. 2022;9(2)
INTRODUCTION
Sleep disordered breathing (SDB) disorders, characterized by disturbed respiration during sleep, can have an effect on normal child development and well-being. Obstructive sleep apnea (OSA), a severe and common form of SDB, typically presents with frequent snoring and is characterized by prolonged periods of increased upper airway resistance leading to intermittent partial to complete obstruction of the upper airway during sleep.1 Normal breathing can often be disrupted during sleep, resulting in episodic oxyhemoglobin desaturation, hypercapnia, frequent arousals, and subsequent sleep fragmentation.1 Audible snoring, a predictor of OSA, is highly prevalent during childhood, affecting as many as 34% of children. 2,3 Habitual snoring, defined as consistent snoring occurring at least 3 nights per week, affects approximately 3% to 12% of all children and these children have a higher prevalence of OSA.4 Epidemiologic studies estimate a prevalence of polysomnography (PSG) confirmed OSA ranging from 1% to 5% of all children (regardless of snoring status).5
Recent studies emphasize the importance of early detection of SDB in young children due to the potential associated health complications associated with this disorder.6,7 Evidence suggests that SDB is associated with numerous comorbidities in children ranging from cardiovascular abnormalities and difficulty with weight gain for infants, as well as neurocognitive dysfunction including low school grades, low self-esteem, high levels of depression, and worsened overall mood.4, 8 Further, the effect of SDB on neurocognitive ability in children has the potential to lead to long-term permanent effects. 9 For example, in a study of 31 children, those with severe SDB had lower IQ scores, decreased executive function, and lower test scores on memory.9
Predisposing factors to SDB include adenotonsillar hypertrophy, nasal obstruction, cleft palate repair, obesity, and syndromic and nonsyndromic-related craniofacial disorders.10 Because abnormalities such as tonsillar hypertrophy are observed in the oral cavity, a dentist may be one of the first health care professionals to identify children at risk.5,8-10 SDB in children is associated with specific muscular, skeletal, and craniofacial characteristics including a dolichofacial pattern that can lead to upper airway narrowing, ultimately resulting in SDB.5,8 Patients typically visit their dentist every 6 months for recall appointments, placing dentists in a unique position to routinely examine the oral cavity’s hard and soft tissue for evidence of not only plaque-mediated pathology (e.g., caries and early periodontal disease), but also evidence of possible airway-related structural comorbidities, while concurrently probing about sleep and mouth habits. 9,10,11 Thus, pediatric dentists may be able to identify children early who are at increased risk of SDB. 5
Currently, the gold standard for diagnosing SDB is in-laboratory PSG. However, limitations in access to pediatric PSG laboratory studies has led to the development of validated questionnaires including the Sleep-Related Breathing Disorder scale of the Pediatric Sleep Questionnaire (SRBD-PSQ)11 to screen and identify children with signs and symptoms of SDB.
The purpose of this study is to examine the association of clinical oral health parameters, observed during children’s routine dental appointments, with symptoms associated with SDB.
It is hypothesized that clinical oral health parameters such as elevated Brodsky score, bruxism, dental malocclusion, mouth breathing, non-nutritive sucking habits, absent history of tonsillectomy, and crowding would be associated with a higher SRBD-PSQ score, signifying symptoms of SDB.
METHODS
Participants
Participants were children aged 1 to 14 years who were seen by a pediatric dental resident at a federally qualified health center in San Diego, California, for a standard-of-care dental examination. Children were included in this study if their parent or guardian was aged 18 years or older, could speak or read English or Spanish, were willing to complete a survey distributed by the principal investigator about their child’s sleep (SRBD-PSQ), and have their child clinically assessed. Only patients who completed the entire survey were included.
This study was approved by NYU Langone Hospitals and San Ysidro Health’s institutional review boards; all guardians gave written consent, and children aged 7 to 14 years gave written assent prior to data collection.
Procedures
Participants were recruited at the dental clinic during a 3-month recall, 6-month recall, or initial comprehensive examination. After the study was explained and written consent was obtained, guardians completed the SRBD-PSQ.11 Clinical parameters were assessed during an oral examination performed by a dentist, blinded to the SRBD-PSQ score. Other characteristics such as age, weight, and height were obtained from the child’s dental chart.
Survey
The SRBD-PSQ is a 22-item, validated screening tool used to identify children with SDB.11 Areas addressed in the SRBD-PSQ include sleeping habits (whether the child exhibits daytime sleepiness or hyperactivity), whether the child wakes up unrefreshed, mouth breathing, bedwetting, snoring habits (including cessation in breathing), and child’s weight.11 For all items, response choices were “no,” “yes,” and “don’t know.” One question from the SRBD-PSQ about bedwetting was inadvertently omitted, leaving only 21 items available from the SRBD-PSQ.
Surveys were scored based on the standard SRBD-PSQ scoring system with responses of yes = 1 point; no = 0 points, and do not know = missing. SRBD-PSQ scores were calculated by summing all ‘yes’ responses.1,12 A total of 8 or more ‘yes’ responses is considered a positive screen for children at risk for SDB and is an indicator of when a clinician should consider referring the patient to a medical professional for a sleep evaluation.
Outcomes
After completing the SRBD-PSQ, the dentist obtained information about the child’s age and sex from their chart. Prior to the child being seated in the dental chair, a dental assistant measured each child’s height and weight, which was used to calculate their body mass index (BMI = kg/m2). Based on the Centers for Disease Control and Prevention guidelines, children were categorized as normal weight if their BMI was in the 5th to < 85th percentile, overweight BMI >85th to <95th percentile, and obese if their BMI was greater than or equal to 95th percentile for age and sex.13 In addition, the child’s history was reviewed with the parent or guardian by the dentist to obtain information on the presence of bruxism, mouth breathing, non-nutritive habits, guardian report of a history of tonsillectomy, and guardian report of the presence of attention deficit hyperactivity disorder (ADHD); using no/yes responses. This information was later validated by the child’s dental chart for use in this study.
An oral examination assessed malocclusion (class I, class II, class III), and crowding (no/yes). Brodsky scores were determined using the Brodsky grading scale where 0 = absent tonsils; Brodsky I = tonsil occupies <25% of oropharynx; Brodsky II = tonsil occupies >25% to 50% of oropharynx; Brodsky III = tonsil occupies >50% to 75% of oropharynx; and Brodsky IV = tonsil occupies >75% of oropharynx.14
Statistical Analysis
Means and standard deviations were calculated for all continuous variables and rates were calculated for all categorical variables. Due to the inadvertent omission of the bedwetting question from the SRBD-PSQ, the SRBD-PSQ score was determined by summing the number of ‘yes’ responses considering the number of ‘do not know’ responses as missing. Comparisons of differences in mean SRBD-PSQ scores by category of each clinical parameter (previous tonsillectomy versus no tonsillectomy, nutritive/non-nutritive habits versus no habits, malocclusion versus no malocclusion, ADHD diagnosis versus no ADHD, and bruxism versus no bruxism) were performed using independent t tests, and by BMI category and Brodsky score (0, I, II, III/IV) using analysis of variance. The association of obesity (BMI category) with PSQ scores was examined using linear regression. The associations of each clinical parameter with SRBD-PSQ scores after adjustment for age, sex, and BMI were examined using linear regression analysis. Sensitivity analyses were performed that examined the associations of each clinical parameter with SRBD-PSQ scores using linear regression analysis after dichotomizing the sample on age (7 years or younger versus older than 7 years).
RESULTS
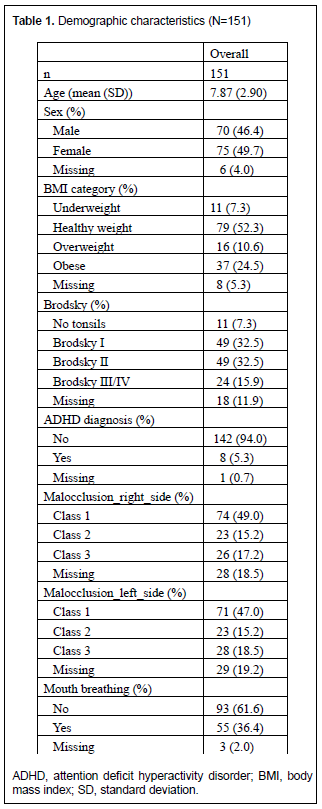
A total of 158 guardian/child pairs who were recruited met the inclusion criteria and agreed to participate. Of these, 151 guardian/child pairs completed the survey and were included in the analyses. Slightly more than half the children were female (53%); average age was 7.8±2.9 years. Based on anthropometric definitions, 10.6% were overweight, 24.5 % were obese, 52.3% were healthy weight, and 7.3% were underweight. Overall, 37% of parents reported mouth breathing in their child, and 9.3% of patients had a previous tonsillectomy (Table 1).
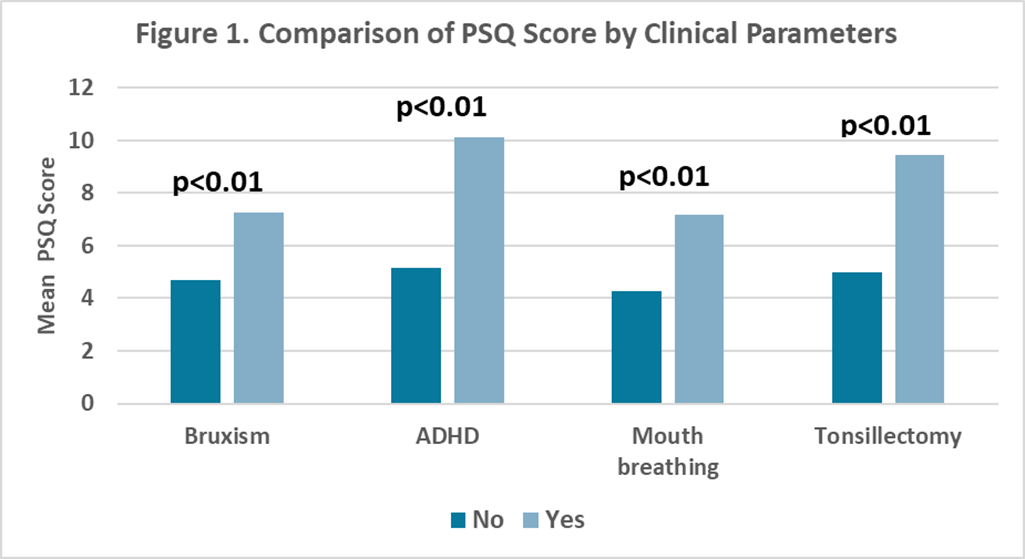
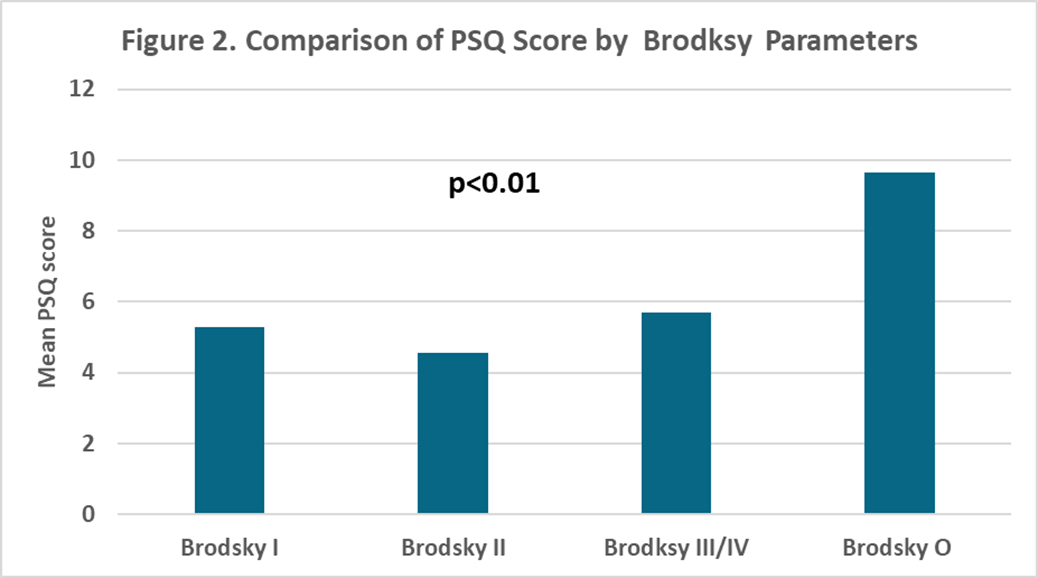
Mean PSQ score was 5.4±3.9 (range = 0-18). There were no significant differences in SRBD-PSQ scores by sex (mean = 6.0±3.8 for boys and 5.1±3.9 for girls, P = 0.19) or by age (mean = 5.2 for children age 7 years or younger and 5.7±3.9 or children older than 7 years, P = 0.42). Comparisons of SRBD-PSQ scores by each clinical parameter (Figure 1) showed that children with bruxism, ADHD, mouth breathing, and previous tonsillectomy had significantly higher mean SRBD-PSQ scores than children without those characteristics (mean = 7.3 versus 4.7 for bruxism (P<0.01); 10.1 versus 5.2 for ADHD (P<0.01); 7.1 versus 4.3 for mouth breathing (P<0.01); and 9.4 versus 5.0 for tonsillectomy (P<0.01)). Comparison of SRBD-PSQ scores by Brodsky score (Figure 2) also showed that children with a Brodsky score of zero had significantly higher SRBD-PSQ scores than those with Brodsky score I, II, or III/VI (mean = 9.6 versus 5.3, 4.6, and 5.7, respectively, P<0.01).
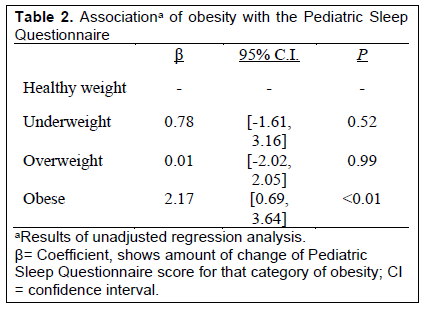
Unadjusted regression analysis revealed that BMI category was significantly and positively associated with SRBD-PSQ scores (Table 2). Relative to healthy weight children, children with obesity had SRBD-PSQ scores that were 2.17 points higher on average (P<0.01), but there were no significant differences in SRBD-PSQ scores between overweight and healthy weight children (P>0.10). Age and sex were not significantly associated with SRBD-PSQ scores (P =0.42 and P =0.19, respectively.
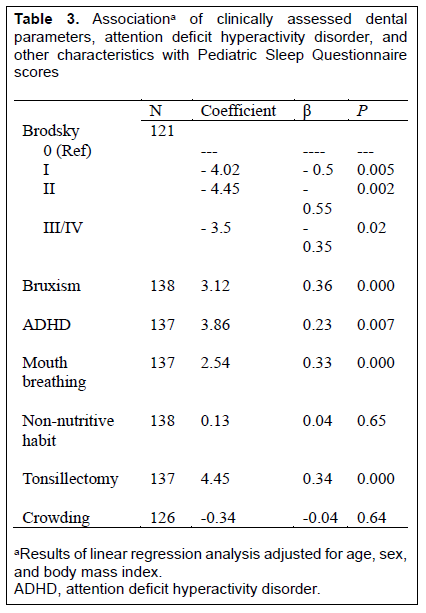
Results of regression analyses evaluating the associations of each clinical parameter with PSQ score after adjustment for age, sex, and BMI are shown in Table 3. Relative to those with Brodsky 0, children with Brodsky scores of I, II, III/IV each had significantly lower PSQ scores (Brodsky I: B = -4.0, P = 0.005; Brodsky II: B =-4.4 , P =0.002; and Brodsky III/IV: B= -3.5, P = 0.01 respectively). After adjustment for covariates, only bruxism, mouth breathing, and prior tonsillectomy history remained significantly associated with SRBD-PSQ score (B s=2.9, 3.0, and 4.1 respectively, all Ps<0.01). Other clinical parameters (malocclusion, ADHD, non-nutritive habits and crowding) were not significantly associated with PSQ scores.
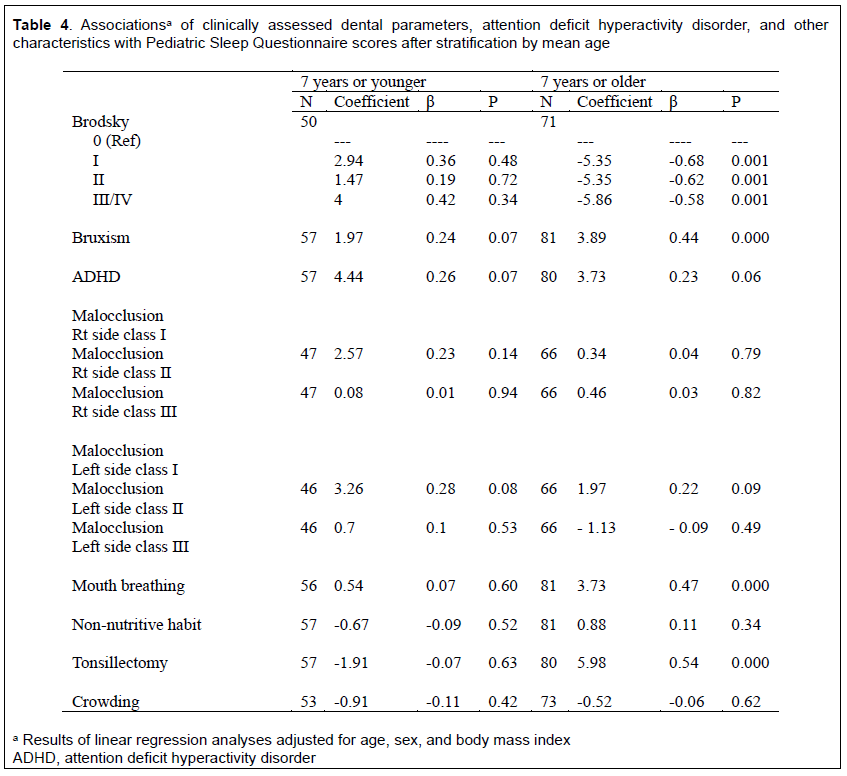
Sensitivity analyses, in which children were stratified by mean age (7 years), were performed to determine whether associations of each clinical parameter and PSQ scores were similar for younger children (age 7 years or younger) with mostly primary dentition, compared to older children (age older than 7 years) with mixed and adult dentition (Table 4). After adjustment for age, sex, and BMI, among children younger than 7 years, ADHD, bruxism, and class 2 malocclusion were not significantly associated with SRBD-PSQ scores. In contrast, among children aged 7 years or older, Brodsky scores I, II, III/IV relative to Brodsky 0 were negatively associated with SRBD-PSQ scores (Ps= 0.0006, 0.0012, 0.0006, respectively), whereas bruxism (P<0.001), mouth breathing (P<0.001) and previous tonsillectomy (P<0.001) all were positively associated with SRBD-PSQ scores.
Table 1Demographic characteristics (N=151) |
{kind=link}
Table 2Associationa of obesity with the Pediatric Sleep Questionnaire |
{kind=link}
Table 3Associationa of clinically assessed dental parameters, attention deficit hyperactivity disorder, and other characteristics with Pediatric Sleep Questionnaire scores |
{kind=link}
Table 4Associationsa of clinically assessed dental parameters, attention deficit hyperactivity disorder, and other characteristics with Pediatric Sleep Questionnaire scores after stratification by mean age |
{kind=link}
Figure 1Comparison of PSQ Score by Clinical Parameters |
{kind=link}
Figure 2Comparison of PSQ Score by Brodsky Parameters |
{kind=link}
DISCUSSION
In this study of children presenting at a pediatric dental clinic, bruxism, ADHD diagnosis, mouth breathing, and history of tonsillectomy were each significantly associated with higher scores on the SRBD-PSQ. These associations were independent of age, obesity and sex, and was were stronger for older children (age older than 7 years). Additionally, obesity was also significantly associated with increased SRBD-PSQ scores. These results suggest that children who present in dental offices as exhibiting these specific clinical parameters may have a higher risk for SDB and may benefit from further medical evaluation.
Results of this study are in accordance with others that reported children with bruxism, ADHD, obesity, and mouth breathing have higher rates of SDB. 2,4-8,10 Tan et al7 noted that obesity has been identified as a significant risk factor for SDB in children. Multiple studies have also described how chronic mouth breathing, a marker for orofacial muscle dysfunction, along with other various oral habits, may place the child at risk for SDB. 4,5,15 Ohayon et al. noted that sleep bruxism typically does not appear by itself but often in conjunction with the presence of SDB, along with other symptoms such as daytime sleepiness.16 Additionally, several studies14,17-23, including a longitudinal study by Perfect et al.,24 reported that SDB in children was associated with a greater number of parent-reported behavioral problems such as ADHD. 17-24 In accordance with others, this study found that guardian report of ADHD was significantly associated with SRBD-PSQ score for the sample as a whole. However, associations were not significant in stratified analyses, most likely due to the attenuated sample sizes.
In this study, tonsil size was assessed using the Brodsky scale, as tonsillar hypertrophy is a known risk factor for SDB in children.25,26 However in the current study, a Brodsky score of zero (likely reflecting a history of tonsillectomy) was associated with a higher SRBD-PSQ score, even following adjustment for obesity. This is in contrast to several previous studies that reported that adenotonsillar hypertrophy is a major risk factor for OSA in children. 2,4,5,27,28 Accordingly, surgical removal of tonsils and/or adenoids or adenotonsillectomy (AT) is considered first-line treatment for pediatric OSA. 15 Several studies report resolution of OSA following AT.5,4,7,29,30 For example, in a prospective randomized controlled trial of AT, parents of children treated with AT reported that quality of life and SDB symptoms were improved after AT compared to children not surgically treated. 15 Greenfeld et al. reported that in infants, clinical symptoms of OSA resolved or significantly improved after AT, but reoccurrence of symptoms was documented in 26% of infants. 31
Regardless, the current study found that absence of tonsils was associated with a higher SRBD-PSQ score. It is possible that there was residual SDB or the persistence of SDB following AT surgery in our cohort. In a multicenter retrospective study, Bhattacharjee et. al reported that residual OSA, as determined by postsurgical PSG, was high, with only 27% of patients having complete resolution of OSA following AT.29 It is also possible that children with a history of previous tonsillectomy (Brodsky 0) are more likely to have a previous and possibly persistent symptoms of sleep disruption. Compared to a general dental population, who by design are not symptomatic with sleep complaints, parents of patients with tonsillectomy history are more likely to endorse sleep disruption resulting in a form of selection bias.
Furthermore, in addition to obesity, older age (older than 7 years) was also associated with residual OSA following AT. In accord with this, stratified analyses in our study showed that only children older than 7 years had higher SRBD-PSQ scores if they did not have tonsils (Brodsky score 0). Additionally, children with obesity had higher SRBD-PSQ scores, which is also in agreement with Bhattacharjee et al.29
It is plausible that other unmeasured risk factors contributed to elevated SRBD-PSQ scores in this pediatric sample. For instance, the presence of comorbidities as often delineated by determining American Society of Anesthesiologists status, and ethnicity may affect SRBD-PSQ score and/or the presence of SDB. De Luca Canto and colleagues2, 32 reported that although adenotonsillar hypertrophy is usually the most common etiology of SDB, other risk factors such as obesity, craniofacial anomalies, asthma, local environment irritants, and preterm birth all can contribute to SDB.30 Although many of these factors cannot be taken into account during a regular dental recall examination, some clinical features such as mouth breathing and bruxism should alert the dentist to the possible presence of SDB and prompt the dentist to adequately screen for this detrimental disease.
Administering a survey, such as the SRBD-PSQ, is relatively quick and inexpensive; positive results can prompt a medical referral to undergo formal diagnostic evaluation for SDB via PSG. Past research has examined whether screening using a physical examination can improve identification of SDB. Results of a systematic review and meta-analysis suggest that questionnaires such as the SRBD-PSQ, in combination with a physical examination, can improve the overall performance of the test in diagnosing SDB.2 Although the gold standard in the diagnosis of SDB relies on PSG, the application of validated questionnaires such as the SRBD-PSQ may facilitate earlier testing and recognition of SDB. 4 Early diagnosis is key in helping pediatric patients with SDB, and guidelines have been established by both the American Academy of Pediatrics and the American Academy of Pediatric Dentistry to help recognize and treat young patients at risk for SDB. 4, 27
Several limitations and strengths of this study should be noted. Results of this study are limited by the inadvertent omission of the bedwetting question on the SRBD-PSQ. However, this omission is likely to have introduced a conservative bias. Information regarding ethnicity and the presence of skeletal peculiarities and comorbidities were not obtained; thus, it cannot be determined whether the observed associations vary by these characteristics. ADHD was based on guardian self-report rather than diagnosis by a physician, which may have also introduced conservative bias. Further, the current study did not specifically identify the presence of outcomes such as neurocognitive dysfunction, reduced quality of life, reduced school performance, etc. Another limitation of the current study was that we only sought parental report of tonsillectomy and did not ask for a previous history of adenoidectomy. Adenoidectomy alone or combined with tonsillectomy is the mainstay for surgical treatment of OSA. In addition, adenoidectomy may be performed to treat children with recurrent otitis media infections. Because dentists are unable to assess the status of adenoidal tissue, unless aided by a lateral cephalometric radiograph or cone beam computed tomography where enlarged adenoid tissue can be clearly visualized, and given the other indications for adenoidectomy, we opted to only explore a history of tonsillectomy. Future studies should probe the presence of comorbidities, neurocognitive dysfunction, skeletal peculiarities and ethnicity in patients presenting specific dental hallmarks.
Nevertheless, the current study had a number of strengths including the assessment of a large number of clinical parameters and a relatively large sample size. Additionally, the dentist being blinded to the child’s SRBD-PSQ score when examining the child for clinical parameters and when data on clinical parameters were extracted from the chart are also key strengths in this study.
Clinical parameters such as bruxism, mouth breathing, history of tonsillectomy, ADHD diagnosis, and obesity were associated with higher SRBD-PSQ scores in a pediatric dental population. Because many of these features are routinely identified by pediatric dentists, this study suggests that pediatric dentists and other dentists who provide oral care for children are well positioned for identifying children at risk for SDB. Given the different dental phenotypes of younger versus older children (for example, primary versus permanent dentition), future studies using larger sample sizes that can afford stratification on multiple ages and other clinically significant factors are warranted.
ABBREVIATIONS
ADHD (Attention deficit hyperactivity disorder)
AT (Adenotonsillectomy)
BMI (Body mass index)
OSA (Obstructive sleep apnea)
PSG (Polysomnography)
SDB (Sleep disordered breathing)
SRBD-PSQ (Sleep-Related Breathing Disorder scale of the Pediatric Sleep Questionnaire
ACKNOWLEDGMENTS
The authors thank Yinxinag Wu (Assistant Research Scientist of NYU Langone Health, Division of Biostatistics, Department of Population Health, New York City, New York) for statistical analyses.
REFERENCES
- Tauman R, Gozal D. Obstructive sleep apnea syndrome in children. Expert Review of Respiratory Medicine. 2011; 5(3):425-440.
- De Luca Canto G, Singh V, Major MP, et al. Diagnostic capability of questionnaires and clinical examinations to assess sleep-disordered breathing in children: a systematic review and meta-analysis. J Am Dent Assoc. 2014; 145(2):165-178.
- Ferreira AM, Clemente V, Gozal D, et al. Snoring in Portuguese primary school children. Pediatrics 2000;106(5):E64.
- Ivanoe JR, Lefebvre CA, Stockstill JW. Sleep disordered breathing in infants and children: a review of the literature. Pediatr Dent. 2007; 29:193-200.
- Stauffer J, Okuji D, Lichty G, et al. A review of pediatric obstructive sleep apnea and the role of the dentist. J Dent Sleep Med. 2018; 5(4): 111-130.
- Marcus C, Brooks LJ, Draper K, et al. Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome. Pediatrics. 2012; 130(3):576-584.
- Tan H-L, Gozal D, Kheirandish-Gozal L. Obstructive sleep apnea in children: a critical update. Nat Sci Sleep. 2013; 5:109-123.
- Blechner M, Williamson A. Consequences of Obstructive Sleep Apnea in Children. Curr Probl Pediatr Adolesc Health Care. 2016; 46:19-26.
- Simmons M, Clark G. The potentially harmful medical consequences of untreated sleep-disordered breathing: The evidence supporting brain damage. J Am Dent Assoc 2009;140 (5): 536-542.
- Haviv Y, Benoliel R, Bachar G, Michaeli E. On the edge between medicine and dentistry: Review of the dentist’s role in the diagnosis and treatment of snoring and sleep apnea. Quintessence Intl 2014; 45(4): 345-353.
- Chervin RD, Hedger K, Dillon JE, Pituch KJ. Pediatric sleep questionnaire (PSQ): validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problems. Sleep Med. 2000;1(1):21-32.
- Chervin RD, Weatherly RA, Garetz SL, et al. Pediatric Sleep Questionnaire Prediction of Sleep Apnea and Outcomes. Arch Otolaryngol Head Neck Surg. 2007;133(3):216-222.
- Centers for disease Control and Prevention; https://www.cdc.gov/healthyweight/assessing/bmi/childrens_bmi/about_childrens_bmi.html#HowIsBMICalculated Updated May 9, 2019
- Ramos SD, Mukerji S, Pine HS. Tonsillectomy and adenoidectomy. Pediatr Clin North Am. 2013; 60(4):793-807.
- Garetz SL, Mitchell RB, Parker PD, et al. Quality of life and obstructive sleep apnea symptoms after pediatric adenotonsillectomy. Pediatrics. 2015; 135(2): e477-e486.
- Ohayon MM , Li KK, Guilleminault C. Risk Factors for Sleep Bruxism in the General Population. Chest. 2001; 119(1):53-61.
- Constantin E, Low NCP, Dugas E, Karp I, O'Loughlin J. Association between childhood sleep-disordered breathing and disruptive behavior disorders in childhood and adolescence. Behav Sleep Med. 2015;13:6, 442-454, DOI: 10.1080/15402002.2014.940106
- Fischman S, Kuffler DP, Bloch C. Disordered sleep as a cause of attention deficit/hyperactivity disorder: recognition and management. Clin Pediatr. 2015; 54(8):713-722. doi:10.1177/0009922814548673
- Halbower AC, Degaonkar M, Barker PB, Earley CJ, et al. Childhood obstructive sleep apnea associates with neuropsychological deficits and neuronal brain injury. PLoS Med 2006; 3(8): e301. DOI: 10.1371/journal.pmed. 0030301
- Beebe DW. Neurobehavioral morbidity associated with disordered breathing during sleep in children: a comprehensive review. Sleep. 2006;29(9):1115-1134. doi:10.1093/sleep/29.9.1115. PMID: 17040000
- Um YH, Hong SC, Jeong JH. Sleep problems as predictors in attention-deficit hyperactivity disorder: causal mechanisms, consequences and treatment. Clin Psychopharmacol Neurosci. 2017; 15(1):9-18. doi:10.9758/cpn.2017.15.1.9
- Won DC, Guilleminault C, Koltai PJ, Quo SD, Stein MT, Loe IM. It is just attention-deficit hyperactivity disorder…or is it?. J Dev Behav Pediatr. 2017; 38(2):169-172. doi:10.1097/DBP.0000000000000386
- Calhoun SL, Fernandez-Mendoza J, Vgontzas AN, et al. Learning, attention/hyperactivity, and conduct problems as sequelae of excessive daytime sleepiness in a general population study of young children. Sleep. 2012; 35(5):627-632. Published 2012 May 1. doi:10.5665/sleep.1818
- Perfect MM, Archbold K, Goodwin JL, Levine-Donnerstein D, Quan SF. Risk of behavioral and adaptive functioning difficulties in youth with previous and current sleep disordered breathing. Sleep 2013; 36(4):517–525B.
- Kumar DS, Valenzuela D, Kozak FK, et al. The Reliability of Clinical Tonsil Size Grading in Children. JAMA Otolaryngol Head Neck Surg. 2014; 140(11); 1034-1037.
- Ng SK, Lee DLY, Li AM, Wing YK, Tong MCF . Reproducibility of clinical grading of tonsillar size. Arch Otolaryngol Head Neck Surg. 2010; 136(2):159-162.
- American Academy of Pediatric Dentistry. Policy on obstructive sleep apnea (OSA). The Reference Manual of Pediatric Dentistry. Chicago, Ill.: American Academy of Pediatric Dentistry; 2021:123-126.
- Supriyatno B, Said M, Hermani B, Sjarir DR, Sastroasmoro S. Risk factors of obstructive sleep apnea syndrome in obese early adolescents: a prediction model using scoring system. Acta Medica Indonesiana. 2010;42(3):152-157.
- Bhattacharjee R, Kheirandish-Gozal L, Spruyt K, et al. Adenotonsillectomy outcomes in treatment of obstructive sleep apnea in children: a multicenter retrospective study. Am J Respir Crit Care Med. 2010;182(5):676-683.
- Marcus CL, Moore RH, Rosen CL, et al. A randomized trial of adenotonsillectomy for childhood sleep apnea. N Engl J Med. 2013;368(25):2366-2376.
- Greenfeld M, Tauman R, DeRowe A, Sivan Y. Obstructive sleep apnea syndrome due to adenotonsillar hypertrophy in infants. Intl J Pediatr Otorhinolaryngol. 2003;67(10):1055-1060.
- De Luca Canto G, Singh V, Gozal D, Major PW, Flores-Mir C. Sleep bruxism and sleep-disordered breathing: a systematic review. J Oral Facial Pain Headache. 2014;28(4):299-305.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted February 2, 2021
Submitted in final revised form September 24, 2021
Accepted for publication October 19, 2021
Address correspondence to: Michelle DaRocha, DMD, San Ysidro Health, Children’s Dental Center at Rady Children’s Hospital, 8110 Birmingham Way, Building 28, San Diego, CA 92123; Email: darocham87@gmail.com