Original Article 1, Issue 7.1
Adherence and Side Effects Among Patients Treated With Oral Appliance Therapy for Obstructive Sleep Apnea
http://dx.doi.org/10.15331/jdsm.7104
Shaun Murphy DDS, Rachael Maerz DDS, MS, Victoria Sheets, DDS, Victoria McLaughlin DDS, F. Michael Beck, DDS, MS, William M. Johnston, MS, PhD, Allen R. Firestone DDS, MS
The Ohio State University, Division of Orthodontics, Columbus, OH
ABSTRACT
Study Objectives:
Oral appliance therapy (OAT) is a common treatment for obstructive sleep apnea (OSA). The aim of this study was to evaluate the level of patient knowledge and concern for the consequences of untreated OSA, perceived partner satisfaction, and reported adverse effects, and relate these to patient adherence to OAT.
Methods:
Subjects consisted of patients treated for OSA using OAT for at least 1 year. Subjects were administered a telephone survey regarding their adherence to treatment, knowledge and concern about OSA, partner satisfaction, adverse effects, and, where appropriate, reasons for discontinued treatment. Subjects were categorized into adherent (to OAT), and nonadherent to OAT, i.e., CPAP, or no-treatment groups.
Results:
A total of 283 patients were contacted, and 136 responded (48.1%): 104 adherent (76.1%) and 32 non-adherent (23.5%). Of the 32 in the nonadherent group, 13 (40.6%) had returned to CPAP usage, and 18 (56.3%) were using no treatment at all. There was no difference in the level of self-reported knowledge about OSA among the three groups (P>0.05). However, the adherent and CPAP groups had significantly higher levels of self-reported concern about the consequences of untreated OSA when compared to the no-treatment group (P<0.0001, P = 0.0002). Partner satisfaction was reported as significantly higher in the adherent group than in the other groups (P = 0.0213, P = 0.0213). No difference in the severity of snoring was found before or after treatment in any of the three groups (P > 0.05).
Conclusions:
Educating patients on the health consequences of untreated OSA and addressing the concerns of patient partners may increase adherence to treatment with oral appliances and may help reduce the number of patients who discontinue all treatment.
Keywords:
OSA; Oral Appliance Therapy; CPAP; Adherence; Side Effects
Citation:
Murphy S, Maerz R, Sheets V, McLaughlin V, Beck M, Johnston WM, Firestone AR. Adherence and side effects among patients treated with oral appliance therapy for obstructive sleep apnea. J Dent Sleep Med. 2020;7(1)
INTRODUCTION
Obstructive sleep apnea (OSA) is a sleep-related breathing disorder, affecting millions in the United States and worldwide. It has been estimated that one in five adults experiences at least mild OSA.1,2 Untreated OSA is associated with a number of important behavioral, social and medical morbidities including systemic hypertension, cardiovascular disease, stroke, insulin resistance, depression, anxiety, and impaired cognitive function.2 Continuous positive airway pressure (CPAP) is the most commonly prescribed treatment for OSA and is highly effective in reducing the number of apneas and hypopneas per hour of sleep; measured by the apnea-hypopnea index (AHI). However, adherence to treatment with CPAP is low among patients, especially those with moderate to mild OSA.3
Oral appliances are an accepted first-line treatment for those who have mild and moderate sleep apnea, and an alternative for those patients who have severe sleep apnea and cannot tolerate or refuse CPAP therapy. 4 Oral appliances position the mandible forward, resulting in increased airway patency and preventing upper airway obstructions. They have also demonstrated successful improvement of respiratory parameters including reducing oxygen desaturation index, increasing lowest arterial oxygen saturation, and reducing AHI to fewer than 10 events per hour. 5,6 Oral appliances and CPAP have also been shown to achieve similar reductions in systolic and diastolic blood pressure.7 Studies have found the overall success rate, the ability of oral appliances to reduce AHI to fewer than 10 events per hour, to be 54% and a reduction in snoring of 42%.6
Although oral appliances have been shown to effectively decrease symptoms of OSA, there are associated adverse effects including tooth movement, jaw pain, tooth pain, and hypersalivation, which have led patients to discontinue treatment. 6,8 Although adverse effects such as hypersalivation or xerostomia, pain, and discomfort are considered transient, significant occlusal changes including reductions in overjet, overbite, and the number of posterior contacts are progressive in nature and have been found to correlate with long-term OA use, particularly after at least 1 year of use. 8-11 These adverse effects affect patient adherence to treatment.
In one 10-year follow-up studying adherence rates among patients using an oral appliance to treat OSA, adherence was found to be 77% in the first year and diminishing to 58% after 10 years. The most common reasons for ceasing treatment were found to be discomfort and inefficiency in reducing snoring. Several patients who stopped use of the oral appliance turned to an alternative treatment such as CPAP.5 Other studies found adherence to oral appliance therapy (OAT) after 30 months to be 56% to 68%.6
In a study focused on African Americans taking medication to treat type 2 diabetes, some reasons the patients reported nonadherence was their lack of knowledge and concern. 12 We hypothesized that in addition to adverse effects, patient adherence may also be associated with the level of knowledge about OSA and the level of concern about the consequences of leaving the condition untreated. We also hypothesized that social factors such as partner satisfaction with the results of treatment and improvement in snoring would affect patient adherence. It is possible that patients with higher levels of knowledge about OSA and concern about the consequences of untreated sleep apnea, or whose partner is satisfied with the results of treatment including snoring cessation, may be more likely to adhere to treatment even in the presence of adverse effects. The aims of this investigation were to evaluate the level of patient knowledge, concern, and perceived partner satisfaction and relate these to patient adherence to treatment.
METHODS
This study was reviewed and approved by The Ohio State Institutional Review Board. Subjects consisted of patients treated for obstructive sleep apnea with OAT for at least 1 year between October 2008 and March 2016 in a private dental practice located in a university medical center. Subjects were administered a telephone survey consisting of a series of questions including, among others, whether or not they were wearing their oral appliance. If they responded that they were not wearing their oral appliance, they were asked if they were managing their OSA some other way. Based on that response, subjects were then categorized into adherent (with OAT) and nonadherent groups. The nonadherent group in turn was subdivided into no-treatment and CPAP groups. Patients who did not respond to two attempts to contact them by phone were mailed a paper copy of the questionnaire with a postage-paid return envelope.
Adherent subjects were asked whether or not they experienced any adverse effects such as jaw pain, tooth pain, bite change, drooling, or other. Nonadherent subjects were asked why they stopped wearing their oral appliance and given a list of reasons: did not work or symptoms worsened, teeth moved or bite changed, uncomfortable/ woke me up/ painful in the morning, inconvenient, does not fit anymore, lost or broken appliance, apnea lessened/ lost weight, started or preferred CPAP usage, or other.
All subjects, Adherent, No Treatment, and CPAP, were asked to rate their concern for the consequences of OSA on a scale of 0 to 10 (0= unconcerned to 10= concerned), along with their knowledge of (0 =no knowledge to 10 = knowledgeable) and partner’s satisfaction with the results of their treatment (‘dissatisfied’= 1 to ‘satisfied’ = 4). All subjects were also asked to rate the severity of their snoring on a scale of 0 to 3 (‘none’= 0 to ‘severe’ = 3) before and after treatment with an oral appliance.
Responses to questions regarding adverse effects, concern, and partner satisfaction in the groups were then summarized and analyzed using a pairwise two-sided multiple comparison analysis (Dwass, Steel, Critchlow-Finger method.) Responses to questions regarding the severity of snoring were summarized and analyzed using non-parametric Wilcoxon rank-sum test and Kruskal-Wallis test. Subject demographics including sex, age, and body mass index (BMI), included in the questionnaire, were analyzed using Pearson chi-square test and Tukey-Kramer analysis.
RESULTS
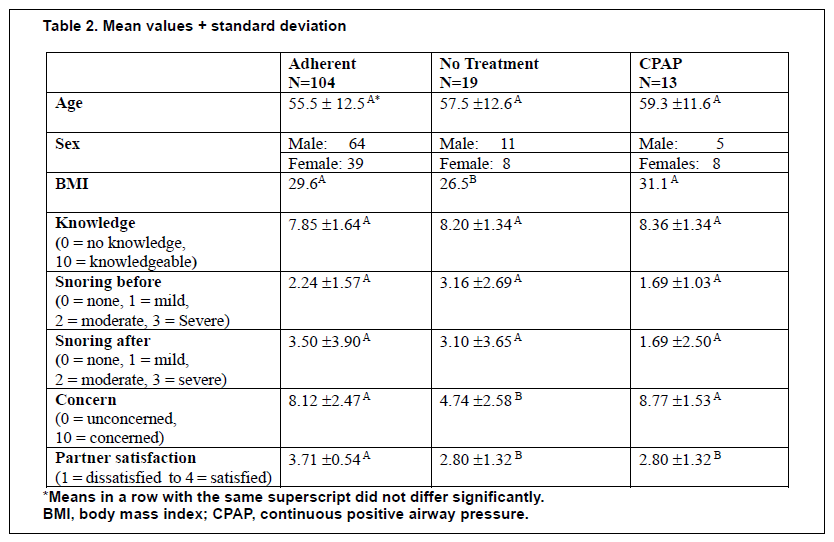
Of the 283 people in whom a contact attempt was made, 136 responded (48.1%): 104 adherent (76.4%), and 32 nonadherent (23.5%). There were no differences in age or sex among groups. However, mean BMI in the no-treatment group was significantly lower than in both CPAP and adherent groups (P = 0.0260 and P = 0.0302, respectively).
In the 104 adherent subjects, 79 (76.0%) reported one or more adverse effects. Of the 32 nonadherent subjects, 13 (40.6%) were currently managing their OSA using CPAP, and all 32 (100%) reported some sort of adverse effect with the oral appliance.
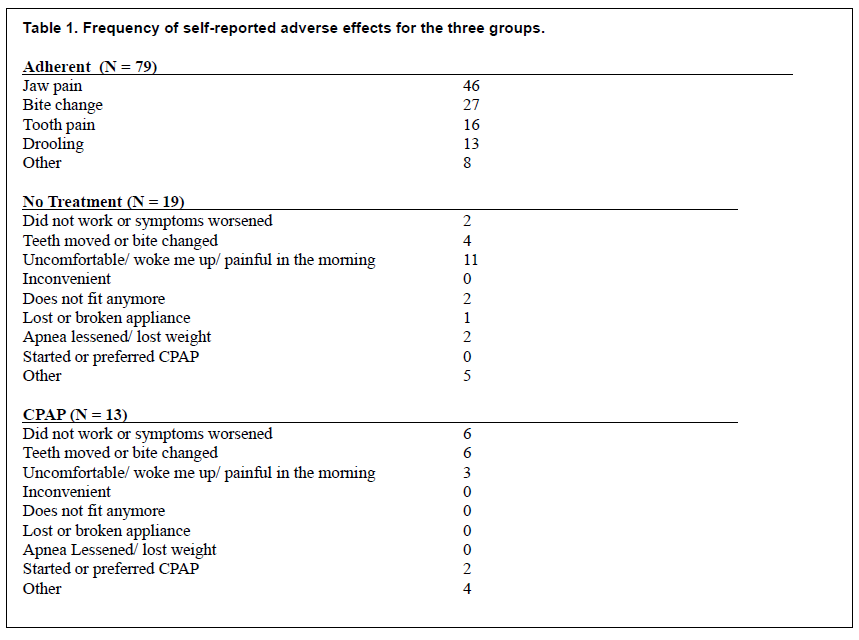
Side effects and reasons for discontinuing use of the oral appliance reported by the three groups are listed in Table 1. The side effects reported most frequently in the adherent and no-treatment groups were jaw pain and discomfort, especially in the morning, followed by a change in occlusion. In the CPAP group the adverse effects reported most frequently were failure to work and teeth moved. Neither the no-treatment nor the CPAP groups found the oral appliance to be inconvenient. Comments under ‘other’ side effects not listed included soft-tissue irritation, sore and bleeding gingiva, xerostomia, and headaches.
There were no differences among the three groups (p>0.05) for knowledge about OSA (0 = no knowledge to 10 = knowledgeable). The mean knowledge reported was 7.9, 8.4, and 8.2 for the adherent, CPAP, and no-treatment groups, respectively. The mean concern (0 = unconcerned to 10 = concerned) with the consequences of untreated OSA, were 8.2, 8.8, and 4.7, for the adherent, CPAP, and no-treatment groups, respectively. Both the adherent and CPAP groups reported significantly higher levels of concern when compared to the no-treatment group (P < 0.0001 and P = 0.0002, respectively). There was no difference in concern between adherent and CPAP groups (p = 0.7067).
Partner satisfaction (‘dissatisfied’ = 1 to ‘satisfied’ = 4) was found to be significantly higher in the adherent group when compared with no-treatment and CPAP groups (p = 0.0213, p = 0.0213 respectively). No difference in partner satisfaction was found between no-treatment and CPAP groups (p = 1.0000). The mean partner satisfaction was 3.71 for adherent and 2.80 in both no-treatment and CPAP groups.
There were no differences in the severity of snoring found among no-treatment, adherent, or CPAP groups (p = 0.8096, p = 0.2155, p = 0.3332, respectively) before treatment or after treatment (p = 0.9891, p = 0.03980, p = 0.2703). Snoring did not change significantly in any of the groups after treatment. Mean values and results of subject demographics, BMI, knowledge, concern, snoring severity, and partner satisfaction are summarized in Table 2.
Table 1Frequency of self-reported adverse effects for the three groups. |
{kind=link}
Table 2Mean values + standard deviation |
{kind=link}
DISCUSSION
The purpose of this study was to evaluate patient adherence to OAT for OSA, side effects of OAT, patient knowledge, and concern about the effects of OSA and partner satisfaction with treatment. A further aim was to evaluate whether adverse effects contributed to the discontinuation of treatment.
The results of this study indicated that adherence in subjects who responded was high: 76.4% were still using oral appliances, 10.3% were using CPAP, and only 13.2% discontinued treatment altogether. No-treatment subjects reported reasons for discontinuation of OAT as discomfort and jaw pain (61.1%), change in occlusion (22.2%), or they believed the oral appliance did not work (11.1%). The no-treatment subjects reported that they discontinued treatment more frequently due to side effects rather than perceived lack of effect. Pain and discomfort were the most common reasons for subjects to discontinue treatment altogether. For subjects who reported turning to CPAP use, the most common reasons for discontinuing oral appliance use were either that they experienced a change in occlusion (42.6%) or that they believed the oral appliance did not work (42.6%). Subjects who were using their oral appliances reported jaw pain as the most frequent adverse effect (58%), followed by bite change (34%).
Though OAT is generally well tolerated, these results are comparable to other studies that also found reasons for noncompliance among patients to be directly related to the presence of adverse effects including discomfort, occlusal changes, and hypersalivation, or a perceived lack of efficacy. 6,8,9,13 Almeida et al., categorizing patients into ‘users’ and ‘nonusers,’ reported that 46% of users and 59.1% of nonusers experienced one or more adverse effects and that nonusers who experienced more adverse effects tended to discontinue OAT use sooner, whereas patients who were able to use it for longer periods experienced milder problems.8 Among the nonusers, the most common reasons for discontinued use of OAT were discomfort (44.9%), had little or no effect (36.0%), or switched to CPAP (23.6%).8 The most common adverse effects among the OAT users were reported as tooth discomfort and difficulty chewing in the morning, followed by tooth movement. 8
As occlusal changes are progressive in nature, studies have found this to be significant reason for discontinuing treatment and have shown a positive correlation with the length of OA use, with significant changes occurring after 1 year of appliance use. 8,9 Studies that quantified the progression of occlusal changes with long-term use of an oral appliance observed changes including decreased overbite and overjet, development of a posterior open bite, and anterior-posterior changes with a movement tendency toward a mesiocclusion. 9,14 In this study, occlusal changes were reported as the second most common adverse effect among adherent, no-treatment and CPAP groups. Because the subjects had worn the oral appliance for at least 1 year, they likely experienced the dental changes associated with wearing the oral appliance. However, although a significant number of subjects in the adherent group reported the adverse effect, ‘tooth movement or bite change’ (34%), it is likely that other factors or benefits from treatment outweighed the dental side effects reported by adherent subjects.
Although self-reported knowledge about OSA did not differ among the groups, the reported levels of concern for the consequences of untreated OSA were significantly higher in the adherent and CPAP groups than in the no-treatment group. Adherent subjects also reported a higher level of partner satisfaction with treatment than the CPAP and no-treatment groups. Other investigators have also reported higher partner satisfaction among those adhering to OAT. 8 Although no group reported significant differences in snoring before or after treatment, it is likely that it contributes to partner satisfaction. Although this study did not inquire about the effects of CPAP on the patient’s partner, anecdotal evidence suggests that bed partners can be negatively affected by CPAP. The significantly higher partner satisfaction and level of concern in adherent subjects suggests that these factors contribute to patients’ adherence to treatment even in the presence of significant adverse effects such as discomfort and occlusal changes.
Similarly, in a study exploring reasons for patient adherence and nonadherence to taking prescribed medications for type 2 diabetes in African-American adults, one reason for intentional nonadherence was related to the concern about adverse effects. 12 The same authors reported that patients’ reasons for adherence included concerns about the health consequences of not treating their type 2 diabetes and the social costs of future poor health as a result of their illness, and the belief that the treatment was effective. 12 This is in agreement with our finding that patients who persevered with treatment, either OAT or CPAP, had a higher concern for the consequences of untreated OSA.
There are a number of shortcomings of the study. Although all subjects were surveyed after at least 1 year of treatment, time was not measured for OAT use or adverse effects. Additionally, subjects were not surveyed before beginning treatment on their level of knowledge or concern for OSA. There is also the possibility of the ‘sour grapes’ phenomena, where nonadherent subjects may report a lower level of concern about the consequences of OSA because they stopped treatment for OSA. This could have led them to reason that consequences of OSA are not serious. Additionally, the subjects represented a “convenience sample,” where only subjects in the university medical center private dental practice were administered the survey. Thus, the generalizability of the results is open to question. Furthermore, the administered questionnaires were self-reports, meaning there is potential for recall bias in responses and, with a response rate of 48.1%, the risk of a nonresponse bias.
CONCLUSION
Educating patients, emphasizing the health consequences of untreated OSA, and addressing the concerns of patient partners may increase adherence to treatment with oral appliances. Informed patient education may also help reduce the number of patients who discontinue all treatment for OSA.
REFERENCES
- Ho ML, Brass SD. Obstructive sleep apnea. Neurol Int. 2011;3(3):e15.
- Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002;165(9):1217-1239.
- Yetkin O, Kunter E., Gunen H. CPAP compliance in patients with obstructive sleep apnea syndrome. Sleep Breath. 2008;12(4):365-367.
- Epstein LJ, Kristo D, Strollo PJ, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(03):263–276.
- Wiman Eriksson E, Leissner L, Isacsson G, Fransson A. A prospective 10-year follow-up polygraphic study of patients treated with a mandibular protruding device. Sleep Breath. 2015;19(1):393-401.
- Hoffstein, V. Review of oral appliances for treatment of sleep-disordered breathing. Sleep Breath. 2007;11(1):1-22.
- Bratton DJ, Gaisl T, Wons AM, Kohler M. CPAP vs mandibular advancement devices and blood pressure in patients with obstructive sleep apnea: a systematic review and meta-analysis. JAMA. 2015;314(21):2280-2293.
- Almeida FR, Lowe AA, Tsuiki S, et al. Long-term compliance and side effects of oral appliances used for the treatment of snoring and obstructive sleep apnea syndrome. J Clin Sleep Med. 2005;1(2):143-149.
- Pliska B, Nam H, Chen H, Lowe AA, Almeida FR. Obstructive sleep apnea and mandibular advancement splints: occlusal effects and progression of changes associated with a decade of treatment. J Clin Sleep Med. 2014;10(12):1285-1291.
- Venema JA, Stellingsma C, Do MH, Hoekema A. Dental side effects of long-term obstructive sleep apnea therapy: a comparison of three therapeutic modalities. J Dent Sleep Med. 2018;5(2):39–46.
- Martínez-Gomis, J, Willaert E, Nogues L, Pascual M, Somoza M, Monasterio C. Five years of sleep apnea treatment with a mandibular advancement device: side effects and technical complications. Angle Orthod. 2010;80(1):30-36.
- Shiyanbola OO, Brown CM, Ward EC. “I did not want to take that medicine”: African-Americans’ reasons for diabetes medication nonadherence and perceived solutions for enhancing adherence. Patient Prefer Adherence. 2018;12:409-421.
- McGown AD, Makker HK, Battagel JM, L'Estrange PR, Grant HR, Spiro SG. Long-term use of mandibular advancement splints for snoring and obstructive sleep apnea: a questionnaire survey. Eur Respir J. 2001;17(3):462-466.
- Doff MHJ, Finnema K J, Hoekema A, Wijkstra P J, de Bont LGM, Stegenga B. Long-term oral appliance therapy in obstructive sleep apnea syndrome: a controlled study on dental side effects. Clin Oral Invest. 2013;17(2):475-482.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication January 23, 2019
Submitted in final revised form August 7, 2019
Accepted for publication August 27, 2019
Address correspondence to: Allen Firestone DDS, MS, The Ohio State University, Department of Orthodontics; Email: Firestone.17@osu.edu
DISCLOSURE STATEMENT
The authors have no conflicts of interest to disclose.
PDF