Original Article 1, Issue 4.3
Safety and Efficacy of a Novel Oral Appliance in the Treatment of Obstructive Sleep Apnea
http://dx.doi.org/10.15331/jdsm.6678
Damian Lavery, BDSc1 ; Irene Szollosi, PhD2 ; Stefan Czyniewski, BMedSci3 ; Fiona Beer, MSc3 ; Karen McCloy, BDSc, MS, MSMed; Christopher Hart, MPhil2
1National Dental Care, Brisbane, Queensland, Australia; 2Oventus Medical Pty Ltd., Brisbane, Queensland, Australia; 3Mobius Medical Pty Ltd., Sydney, New South Wales, Australia
ABSTRACT
Study Objectives:
To establish the safety and efficacy of a novel oral appliance (O2Vent Mono, Oventus Medical Pty Ltd., Brisbane, Australia), that incorporates a built-in enclosed airway, as an alternative treatment for obstructive sleep apnea (OSA).
Methods:
A prospective, single-arm, single-center study was performed. Participants had mild-moderate OSA or continuous positive airway pressure (CPAP) intolerant severe OSA. Ambulatory polysomnography (PSG), subjective snoring, and subjective nasal obstruction were assessed at baseline and following acclimatization with the device. Baseline mandibular protrusion was set at 50% and was increased to a maximum of 85% if required as determined by questionnaire and PSG. Participants with a ≥ 50% reduction in apnea-hypopnea index (AHI) were classified as responders. Compliance was recorded via a questionnaire.
Results:
In 29 participants (20 males, 9 females), mean ± standard deviation age = 49.3 ± 8.6 years, body mass index = 29.9 ± 6.1 kg/m2 , AHI decreased from 41.8 ± 26.5 to 16.2 ± 15.4 (P < .001) or 62.5 ± 21.1%. Time spent below 90% oxygen saturation as assessed by pulse oximetry improved from 9.3 ± 12.7% to 2.2 ± 3.4% (P = .001). Seventeen participants (59%) had subjective nasal obstruction and 22 (75.9%) were classified as responders. Subgroup analysis between those with nasal obstruction (NO) and without nasal obstruction (NNO) revealed no significant difference in percentage of change in AHI from baseline (NO = 66.3 ± 18.1%, NNO = 57.0 ± 24.6%, P = .280) or response rate (NO = 76.5%, NNO = 75%, chi-square = 0.930). Overall compliance was 82.8%, and three minor transient device-related adverse events occurred.
Conclusions:
This novel device was safe, effective, and well tolerated in a group of participants with relatively severe OSA. There was a clinically and statistically significant reduction in AHI of 62% as well as improvement in oxygen saturation. Importantly, the efficacy and response do not appear to be reduced by the presence of nasal obstruction.
Clinical Trial Registration:
Trial name: A prospective, single arm, single center pilot trial to establish the safety and efficacy of the Oventus device to treat mild to moderate obstructive sleep apnea and snoring. URL: https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=367532. Registration number: ACTRN12615000028505
Keywords:
mandibular advancement device, mandibular advancement splint, obstructive sleep apnea, oral appliance
Citation:
Lavery D, Szollosi I, Czyniewski S, Beer F, McCloy K, Hart C. Safety and efficacy of a novel oral appliance in the treatment of obstructive sleep apnea. Journal of Dental Sleep Medicine. 2017;4(3):57–63.
INTRODUCTION
Obstructive sleep apnea (OSA) is characterized by repetitive occlusions of the upper airway during sleep, resulting in sleep fragmentation and oxygen desaturations.1 The prevalence of OSA is reported to be 34% in men and 17% in women, whereas OSA accompanied by symptoms of sleepiness is reported to occur in 14% of men and 5% of women between 30–70 years old.2 OSA is an important contributor to cardiovascular disease,3–7 stroke,4,8,9 and depression10 and is a recognized risk factor for motor vehicle accidents,11–13 workplace injuries, and loss of productivity.14,15
Although continuous positive airway pressure (CPAP) remains the treatment of choice for OSA, custom-fit oral appliances that advance the mandible—a mandibular advancement device (MAD)—are emerging as an alternative treatment option. These devices are used primarily in patients with mild to moderate OSA, CPAP intolerant OSA, and primary snorers.16,17 Studies consistently demonstrate that CPAP reduces the apnea-hypopnea index (AHI) further than oral appliances; however, CPAP efficacy is likely to be offset by reductions in usage and adherence.18 In support of this, recent studies have demonstrated that the health outcomes in patients with moderate to severe OSA after treatment with CPAP and MAD are similar.19,20 Patients with high nasal resistance may have difficulty in using both CPAP and traditional oral appliances, with studies reporting high nasal resistance being associated with both CPAP 21 and oral appliance 22 intolerance. High nasal resistance is an indication of reversible or irreversible nasal obstruction and its prevalence is high in OSA.23
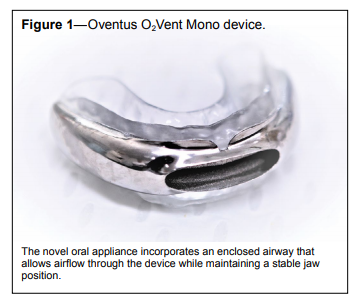
The novel oral appliance studied in the current study (O2Vent Mono, Oventus Medical Pty Ltd., Brisbane, Australia) (Figure 1) incorporates both mandibular advancement to reduce pharyngeal collapsibility and an enclosed airway that allows airflow through the device to circumvent nasopharyngeal obstruction. Titration is achieved by sequential relining of the upper silicone insert, which is changed over to a more retentive dual laminate material after the optimum level of advancement is achieved. Thus, although a monobloc design, it can be considered as a titratable device during the treatment optimization and acclimatization period. The aim of the current study was to evaluate the safety and efficacy of this novel oral appliance for the treatment of OSA. In addition, we wanted to examine whether compliance with or the response rate to the device were influenced by the presence of subjective nasal obstruction.
Figure 1Oventus O2Vent Mono device. |
{kind=link}
METHODS
This was a single-center, prospective pilot study to establish the safety and efficacy of the oral appliance in treating OSA. The study protocol was approved by an independent Human Research Ethics Committee (Bellberry Limited, Australia), and appropriate informed consent was obtained from all participants. Clinical trial and data management was performed by a contract research organization (Mobius Medical Pty Ltd, Australia) to ensure independent oversight of regulatory compliance, monitoring, and reporting.
Participant Selection
Male and female participants aged 18 years and older were recruited from Turbot Street Medical Centre presenting for consideration of oral appliance therapy. Inclusion criteria were grade 2–3 snoring (regular: more than 3 nights/wk or every night) and either mild to moderate sleep apnea (AHI > 5 and < 30 events/h) and recommended for oral appliance therapy, or CPAP-intolerant patients with moderate to severe sleep apnea (AHI ≥ 15 events/h). Additional inclusion criteria were eligibility to receive a MAD with adequate dentition for retention and the ability to provide written informed consent to all study procedures. Diagnosis was based on polysomnography (PSG) within the past 12 months by a qualified sleep physician. Exclusion criteria were pregnancy or lactation, current participation in another clinical trial, periodontal disease, exaggerated gag reflex, medication usage that could influence respiration or sleep (eg, regular use of sedatives, heavy alcohol consumption), OSA with uncontrolled or untreated cardiovascular disease, central sleep apnea ≥ 5 events/h, previous uvulopalatopharyngoplasty (UPPP), and severe somatic or psychiatric disorders. Three-dimensional cone beam computed tomography (CBCT) scans were completed to screen for dental pathology and to assess the temporomandibular joints.
Oral Appliance
The initial jaw position at 50% of maximum mandibular protrusion was recorded by a researcher who is a qualified dentist using a George gauge with a 5-mm bite fork (Great Lakes Orthodontics, Tonawanda, New York, United States) to obtain 5 mm of vertical opening. Maxillary and mandibular impressions were taken using Imprint 4 Preliminary VPS Impression Material (3M ESPE, Landsberg am Lech, Germany). The impressions were poured with dental stone, and the models and bite were scanned using TRIOS 3 Scanner (3Shape, Szczecin, Poland) and converted to a sterolithography file. Computeraided design using proprietary software was used to customize the size and shape of the bimaxillary oral appliance.
The inner core of the oral appliance (Figure 1) was printed three-dimensionally using Ti6Al4V ELI Titanium Powder Grade 23 (Arcam AB, Mölndal, Sweden). The titanium core has a customized airway, which divides at the level of the canines, and passes posteriorly between the occlusal surfaces of the maxillary and mandibular teeth to deliver air to the oropharynx in the region of the second molars, with the aim of bypassing nasopharyngeal obstruction during sleep and allowing for breathing through the low-resistance device airway when nasal flow is compromised. The cross-sectional area of the bilateral airway is consistent with the average patent nasal airway and a lip seal can be maintained around the anterior opening.
After polishing the titanium core, a silicon primer was applied (NuSil Technology, Carpinteria, California, United States) to allow for bonding of the maxillary silicone inserts, constructed using Bona-Bite Crystal Vision (DMP Ltd, Markopoulo, Greece). The mandibular insert was a dual laminate material (Erkodent, Wembley, Western Australia, Australia) with a hard outer lining and soft inner lining for greater retention and durability. The upper silicone inserts were positioned with the mandibular protrusion as obtained from the bite record and impressions. Further titration during the protocol was performed by sequential relining and replacement of the upper silicone inserts, resulting in the mandible being in a more advanced position.
Study Protocol
During the baseline visit, demographic information was collected and sleep questionnaires administered. Subjective nasal obstruction was assessed at the baseline visit using a 10-point scale where 0 = no obstruction, 5 = moderate obstruction, and 10 = complete obstruction of nasal airflow. Based on the response to this question, nasal obstruction was recorded as a dichotomous variable with 0 being no, and all other responses as yes. A dental examination was performed to ensure dental suitability for oral appliance therapy by an investigator who is a qualified dentist, who then completed records for construction of the device. Baseline physiological parameters were obtained prior to insertion of the device using a Somte PSG Level II device (Compumedics, Abbotsford, Victoria, Australia) measuring: electroencephalogram, electrooculogram, submental electromyogram, electrocardiogram, oronasal flow using nasal cannula, thoracic and abdominal respiratory effort, snore sound, and body position. All PSG was conducted and scored according to The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications Version 2.2. The recommended hypopnea rule was adopted (ie, hypopnea defined as a ≥ 3% oxygen desaturation from pre-event baseline and/or the event is associated with an arousal). Analysis was performed by a single registered polysomnographic technologist (RPSGT) and reported by a qualified sleep physician. Participants who fulfilled the inclusion criteria were fitted with the oral appliance and given care and maintenance instructions before being sent home. Following 1 week to 1 month of acclimatization, participants returned for a follow-up visit where a clinical review for compliance, comfort, and efficacy of the device was conducted via questionnaires. If participants were compliant, defined as using the device for at least 4 h/night for at least 5 d/wk, an additional level II PSG was conducted. If participants were nonresponders to treatment (< 50% reduction of AHI from baseline) as determined by PSG, the oral appliance was titrated to 75% maximum protrusion and another clinical review with PSG was performed after 1 week to 1 month. If the second treatment PSG at 75% protrusion indicated nonresponse, and further advancement was tolerated, a final titration to 85% protrusion was performed with a final clinical review and PSG after 1 week to 1 month.
Based on the Simons II stage design, a sample size of 30 participants would yield 80% power with 95% confidence to rule out a 5% response rate in favor of at least a 20% response rate. Assessment of device-related adverse events occurred at each visit and was reported according to ISO 14155-2011. Events of interest included excessive salivation, temporomandibular joint pain, gum irritation, mouth dryness, jaw discomfort, tooth loosening, tooth wear, and jaw set.
RESULTS
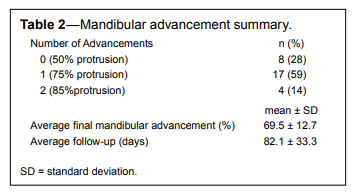
Thirty participants were enrolled into the study, with one withdrawal due to personal reasons prior to a device being issued. Results are presented in Table 1 as mean ± standard deviation for 29 participants (20 males and 9 females) who completed the protocol with age = 49.3 ± 8.6 years, body mass index = 29.9 ± 6.1 kg/m2 . Fifteen participants (51.7%) were initially recommended for CPAP but did not tolerate CPAP prior to inclusion in the study. The study cohort therefore had a greater representation of participants with severe OSA (62%).Seventeen participants (59%) were advanced to 75% maximum protrusion and four (14%) were advanced to 85%, with a mean protrusion of 69.5 ± 12.7% achieved over a mean follow-up period of 82.1 ± 33.3 days (Table 2).
Table 1Sleep and respiratory indices at baseline and following treatment with the oral appliance (n=29). |
{kind=link}
Table 2Mandibular advancement summary. |
{kind=link}
Safety
The device had a favorable safety profile with no serious devicerelated adverse events reported during the trial. Of the four adverse events reported, only three were device related and all events were anticipated. These were jaw pain (on the first night only) for one participant whereas another participant experienced two events, sore tongue and mouth ulcers, all of which resolved and were transient in nature.
Effect on OSA
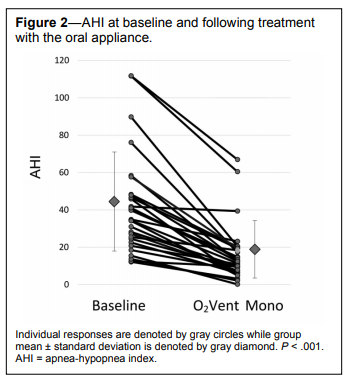
The mean AHI at baseline was 41.8 ± 26.5 (range 12.2 to 111.8) events/h. After the final titration, the group mean AHI was 16.2 ± 15.4 (range 0.2 to 67.0) events/h. The mean reduction in AHI was 24.7 ± 16.8 (range 2.4 to 69.2) events/h, which is statistically and clinically significant (P < .001). This represented a reduction in AHI of 62.5 ± 21.1% from baseline (Figure 2), with improvement observed in supine and nonsupine rapid eye movement and non-rapid eye movement sleep. Arousal index improved from 40.6 ± 16.3 to 22.4 ± 12.4 events/h (P < .001) (Table 1).
Figure 2AHI at baseline and following treatment with the oral appliance. |
{kind=link}
The time spent below 90% oxygen saturation (T90%) improved from 9.3 ± 12.7% to 2.2 ± 3.4% (P = .001) as did the minimum saturation of peripheral oxygen, SpO2, from 82.7 ± 8.9% to 86.3 ± 5.9% (P = .005).
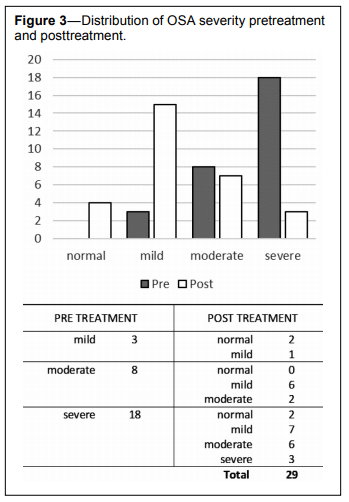
Response rate to treatment according to multiple definitions of AHI reduction were as follows: (1) 22 participants (76%) had a 50% reduction in AHI compared to baseline, (2) 11 participants (38%) obtained a partial response with AHI < 10, and (3) 4 participants (14%) obtained complete normalization with AHI < 5 events/h. In this cohort, 90% of participants were classified as having moderate or severe OSA (28% and 62%, respectively), and we evaluated the changes in OSA severity pretreatment and posttreatment according to the severity of the AHI (Figure 3). Twenty-three participants (79%) obtained a reduction in the classification of OSA severity. Of those with moderate to severe OSA at baseline, 15 of 26 participants (58%) shifted into the normal to mild category.
Figure 3Distribution of OSA severity pretreatment and posttreastment. |
{kind=link}
All participants reported snoring at baseline (Table 1) with 19 (66%) reporting snoring every night and 19 (66%) reporting very loud snoring that can be heard in adjacent rooms. At the conclusion of the study, 24 (82%) reported no snoring, and the remaining 5 (18%) all indicated that the frequency and/or intensity of snoring had improved.
Compliance
The device was well tolerated by participants who indicated good compliance with the device and positive feedback when reporting on comfort. Of the 29 participants who received a device, the average usage of the device was 6 nights/wk. Of the nights the device was used, participants averaged 7 hours of usage (range 4–8 hours). Participants were deemed compliant if they used the device for at least 4 hours for at least 5 days a week. Based on the user comfort survey, compliance was 82.8%.
Nasal Obstruction
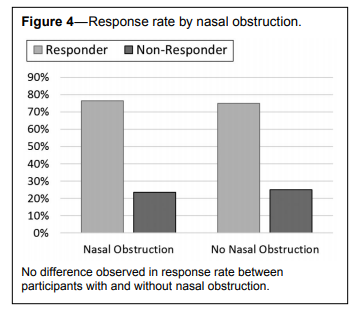
Seventeen of the 29 participants (59%) were documented to have subjective nasal obstruction. Subgroup analysis between those with nasal obstruction (NO) and without nasal obstruction (NNO) revealed no significant difference in the percentage of reduction in AHI (NO = 66.3 ± 18.1%, NNO = 57.0 ± 24.6%, P = .280) or response rate defined as 50% reduction in AHI (NO = 76.5%, NNO = 75%, chi2 = 0.928). Importantly, no differences were observed in compliance between those with and without nasal obstruction (NO = 82.4%, NNO = 83.3%, chi-square = 0.945) (Figure 4).
Figure 4Response rate by nasal obstruction. |
{kind=link}
DISCUSSION
The results of this study demonstrate that the novel oral appliance is safe and effective in treating patients with mild to moderate OSA as well as CPAP-intolerant severe OSA. Importantly, the efficacy, response and compliance with treatment do not appear to be reduced by the presence of nasal obstruction.
Comparisons of different MADs in the treatment of OSA are complicated by many factors including differences in appliance design, level of protrusion and vertical dimension, definition of success, and duration of follow-up. In a review of mandibular advancement therapy, Marklund et al. reported that the mean reduction of AHI from all studies included in the review was 55% (range 28–80),18 whereas Sutherland et al. reported success rates in the range of 30% to 85% for posttreatment AHI < 10 events/h.24 The current study achieved a mean reduction in AHI of 62%, with 38% of the cohort achieving posttreatment AHI < 10 events/h. Although these results are broadly in line with other studies of oral appliance efficacy, it is important to note that the current study included a large proportion of patients (90%) with moderate to severe OSA, making direct comparisons to other studies difficult. However, a recent study by Gjerde et al. reported treatment outcomes for 106 patients with moderate to severe OSA using mixed monobloc and titratable appliances.25 The authors report 75% of patients achieved treatment success as defined by > 50% reduction in AHI, with a reduction in AHI in those with severe apnea from 41.4 to 17.4 events/h. Using this definition of success, our overall cohort had strikingly similar results both for overall success rate (76%) and decrease in mean AHI from 41.8 to 16.2 events/h. However, complete resolution of OSA with AHI < 5 events/h in the current study was 14% compared to 38% reported by Gjerde et al.,25 which may be explained by the higher proportion of individuals with severe apnea in our cohort (62% versus 25%) despite mean AHI being similar between groups. The differences of treatment success rates obtained with various definitions as well as the individual variability in treatment responses is well established. Although complete resolution of OSA was not achieved in most participants, it is important to note that 79% had a reduction in OSA severity classification; 50% of those with severe OSA at baseline moved to the normal to mild category after treatment. This is a clinically important result as a dose-response relationship has been reported between OSA severity and all-cause mortality, cardiovascular mortality,5,7 and incident events26 and those with mild OSA may be at relatively low risk of the development of cardiovascular complications. All of the participants with severe OSA were intolerant to CPAP, and a reduction in OSA severity with the device may offer the opportunity to provide health benefits even if the AHI is not completely normalized. The posttreatment AHI may be an important determinant of when combination therapies may be considered, with recent studies reporting CPAP and oral appliances used in combination may be of benefit.27 Combination therapy using CPAP and MAD may result in lower pressure requirements and improve tolerance and treatment effectiveness in a group that clinically is difficult to treat.
The effect of vertical opening on pharyngeal collapsibility is a topic of current debate and has been evaluated with conflicting results. In one study, increasing the vertical opening was found to have a detrimental effect on pharyngeal collapse as assessed during sleep endoscopy at the base of the tongue28; however, in another study of individuals with apnea, there was no statistically significant difference in sagittal airway at 75% protrusion and 5 or 10 mm vertical dimension.29 In another randomized crossover study, a vertical dimension of 4 or 14 mm did not affect MAD efficacy, although the increase in vertical dimension was associated with a decrease in compliance.30 The required vertical opening for the device used in the current study was 5 mm obtained with a standard 5-mm bite fork. This is within the lower limits of tested vertical dimensions and therefore unlikely to have an adverse effect on either appliance efficacy or compliance.
Previous studies of oral appliances demonstrate self-reported short-term compliance to be 76% to 95%. Vanderveken et al. conducted a 3-month prospective clinical trial that evaluated oral appliance compliance using an embedded microsensor thermometer to measure adherence. Regular use was defined as > 4 hours per day on > 70% of nights and was achieved in 84% of 43 patients who had a complete dataset in the study.31 With the same definition of compliance assessed subjectively, 83% of participants in the current study were compliant at the conclusion of the study, which is comparable with previous research. However, the duration of follow-up was variable and further research is required to demonstrate long-term objective compliance with this device.
Long-term studies show that adverse effects with MADs are common, but are minor and well tolerated, resulting in good compliance.32 Common short-term side effects include excessive salivation, gum irritation, mouth dryness, and jaw discomfort, with reports that these adverse effects generally last less than 3 weeks.33–35 Only three device-related adverse events were reported by two participants during this study, all of which were anticipated and consistent with known shortterm side effects. These transient events did not affect compliance or the efficacy of the device, with participants continuing to use their device after resolution of the events. Longer term side effects of MAD wear include minor tooth movement, changes in the overbite and overjet relationships, changes in incisal proclination, and an increase in lower facial height.36–40 Although dental changes may be evident after 6 months of treatment40 and are generally well tolerated, there is some evidence that these changes are progressive and continue with ongoing treatment.41 It is anticipated that similar long-term side effects would be seen with the device used in this study; however, a larger cohort with longer follow-up is required to evaluate the long-term changes associated with this device.
As well as demonstrating safety and efficacy of the novel oral appliance, we were able to show that compliance and efficacy, as measured by the response rate (> 50% reduction in AHI), was not different between patients with and without nasal obstruction. This was an interesting finding as increased nasal obstruction is common in OSA23 and has been associated with both CPAP21 and oral appliance intolerance.22 For patients who cannot tolerate CPAP or traditional oral appliances, there are very few treatment options left to consider. We speculate that the similar compliance and response rate of approximately 75% in those with and without subjective nasal obstruction observed in the current study is due to the presence of the builtin device airway, which may improve tolerance and efficacy in patients with increased nasal obstruction who otherwise may find it difficult to breathe exclusively via the nasal route. This, however, needs to be validated in a larger cohort with objective assessment of nasal function.
This was a pilot study that established the safety and efficacy of a novel oral appliance with a built-in enclosed airway in the treatment of mild to moderate OSA and CPAP intolerant OSA. Limitations of the study include small sample size and a relatively short follow-up period. Nasal obstruction was evaluated using subjective symptoms and other health outcomes were not evaluated. Last, the final PSG during the treatment optimization was conducted with silicone as the upper insert material. In clinical practice, this is changed to a more retentive and durable dual laminate material after the optimum position has been identified. An additional sleep study with the change in material at the same level of advancement was not performed and as a consequence it is possible that the final efficacy of this device may have been underestimated. Further investigation is required to determine if treatment effectiveness is affected by the change in material. The results of this study are promising and further research in a larger cohort with objective assessments of nasal obstruction, health outcomes, and compliance are warranted as are studies to evaluate the contribution of the built-in airway to improvements in efficacy and compliance.
CONCLUSIONS
This novel oral appliance was found to be safe and effective in a cohort of patients with relatively severe OSA who experienced very few side effects and demonstrated good compliance. Use of the device was associated with a clinically and statistically significant reduction in AHI in the order of 62%, which is broadly in line with published literature of oral appliance efficacy in the treatment of OSA. According to the frequently used definition of treatment success (> 50% reduction in AHI), 76% of participants were responders to treatment. Although a complete resolution of OSA was achieved in a small number of participants, this is partly explained by the relatively severe OSA seen in the current cohort. Importantly, we observed a reduction in OSA severity classification that is likely to provide health benefits, and the efficacy, response, and compliance with treatment did not appear to be reduced by the presence of subjective nasal obstruction. Larger studies with long-term follow up and objective assessment of nasal obstruction and compliance are required; however, the results of this study provide encouraging data to support the notion that patients with OSA and increased nasal resistance may also benefit from this device.REFERENCES
2. Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177(9):1006–1014.
3. Hla KM, Young T, Hagen EW, et al. Coronary heart disease incidence in sleep disordered breathing: The Wisconsin Sleep Cohort Study. Sleep. 2015;38(5):677–684.
4. Young T, Finn L, Peppard PE, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin Sleep Cohort. Sleep. 2008;31(8):1071–1078.
5. Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342(19):1378–1384.
6. Punjabi NM, Caffo BS, Goodwin JL, et al. Sleep-disordered breathing and mortality: a prospective cohort study. PLoS Med. 2009;6(8):e1000132.
7. Shahar E, Whitney CW, Redline S, et al. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J Respir Crit Care Med. 2001;163(1):19–25.
8. Lipford MC, Flemming KD, Calvin AD, et al. Associations between cardioembolic stroke and obstructive sleep apnea. Sleep. 2015;38(11):1699–1705.
9. Redline S, Yenokyan G, Gottlieb DJ, et al. Obstructive sleep apneahypopnea and incident stroke: the Sleep Heart Health Study. Am J Respir Crit Care Med. 2010;182(2):269–277.
10. Gupta MA, Simpson FC, Lyons DCA. The effect of treating obstructive sleep apnea with positive airway pressure on depression and other subjective symptoms: a systematic review and meta-analysis. Sleep Med Rev. 2016;28:55–68.
11. Ward KL, Hillman DR, James A, et al. Excessive daytime sleepiness increases the risk of motor vehicle crash in obstructive sleep apnea. J Clin Sleep Med. 2013;9(10):1013–1021.
12. Young T, Blustein J, Finn L, Palta M. Sleep-disordered breathing and motor vehicle accidents in a population-based sample of employed adults. Sleep. 1997;20(8):608–613.
13. Sassani A, Findley LJ, Kryger M, Goldlust E, George C, Davidson TM. Reducing motor-vehicle collisions, costs, and fatalities by treating obstructive sleep apnea syndrome. Sleep. 2004;27(3):453–458.
14. AlGhanim N, Comondore VR, Fleetham J, Marra CA, Ayas NT. The economic impact of obstructive sleep apnea. Lung. 2008;186(1):7–12.
15. Deloitte Access Economics. Re-awakening Australia: the economic cost of sleep disorders in Australia, 2010. Sleep Health Foundation website. http://www.sleephealthfoundation.org.au/pdfs/news/ Reawakening%20Australia.pdf. Published October 2011. Accessed October 2016.
16. Epstein L, Kristo D, Strollo P, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(3):263–276.
17. Mansfield D, Antic N, McEvoy R. How to assess, diagnose, refer and treat adult obstructive sleep apnoea: a commentary on the choices. Med J Aust. 2013;199(8):S21–S26.
18. Marklund M, Verbraecken J, Randerath W. Non-CPAP therapies in obstructive sleep apnoea: mandibular advancement device therapy. Eur Respir J. 2012;39(5):1241–1247.
19. Bratton DJ, Gaisl T, Wons AM, Kohler M. CPAP vs mandibular advancement devices and blood pressure in patients with obstructive sleep apnea: a systematic review and meta-analysis. JAMA. 2015;314(21):2280–2293.
20. Phillips CL, Grunstein RR, Darendeliler MA, et al. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea. Am J Respir Crit Care Med. 2013;187(8):879–887.
21. Sugiura T, Noda A, Nakata S, et al. Influence of nasal resistance on initial acceptance of continuous positive airway pressure in treatment for obstructive sleep apnea syndrome. Respiration. 2007;74(1):56–60.
22. Zeng B, Ng AT, Qian J, Petocz P, Darendeliler MA, Cistulli PA. Influence of nasal resistance on oral appliance treatment outcome in obstructive sleep apnea. Sleep. 2008;31(4):543–547.
23. Georgalas C. The role of the nose in snoring and obstructive sleep apnoea: an update. Eur Arch Otorhinolaryngol. 2011;268(9):1365–1373.
24. Sutherland K, Vanderveken OM, Tsuda H, et al. Oral appliance treatment for obstructive sleep apnea: an update. J Clin Sleep Med. 2014;10(2):215–227.
25. Gjerde K, Lehmann S, Berge ME, Johansson AK, Johansson A. Oral appliance treatment in moderate and severe obstructive sleep apnoea patients non-adherent to CPAP. J Oral Rehabil. 2016;43(4):249–258.
26. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046–1053.
27. El-Solh AA, Moitheennazima B, Akinnusi ME, Churder PM, Lafornara AM. Combined oral appliance and positive airway pressure therapy for obstructive sleep apnea: a pilot study. Sleep Breath. 2011;15(2):203–208.
28. Vroegop AVMT, Vanderveken OM, Van de Heyning PH, Braem MJ. Effects of vertical opening on pharyngeal dimensions in patients with obstructive sleep apnoea. Sleep Med. 2012;13(3):314–316.
29. Piskin B, Karakoc O, Genc H, et al. Effects of varying mandibular protrusion and degrees of vertical opening on upper airway dimensions in apneic dentate subjects. J Orofac Orthop. 2015;76(1):51–65.
30. Pitsis AJ, Darendeliler MA, Gotsopoulos H, Petocz P, Cistulli PA. Effect of vertical dimension on efficacy of oral appliance therapy in obstructive sleep apnea. Am J Respir Crit Care Med. 2002;166(6):860–864.
31. Vanderveken OM, Dieltjens M, Wouters K, De Backer WA, Van de Heyning PH, Braem MJ. Objective measurement of compliance during oral appliance therapy for sleep-disordered breathing. Thorax. 2013;68(1):91–96.
32. Brette C, Ramanantsoa H, Renouardiere J, Renouardiere R, Roisman G, Escourrou P. A mandibular advancement device for the treatment of obstructive sleep apnea: long-term use and tolerance. Int Orthod. 2012;10(4):363–376.
33. Mehta A, Qian JIN, Petocz P, Darendeliler MA, Cistulli P. A randomized, controlled study of a mandibular advancement splint for obstructive sleep apnea. Am J Respir Crit Care Med. 2001;163(6):1457–1461.
34. Schmidt-Nowara W, Lowe A, Wiegand L, Cartwright R, Perez-Guerra F, Menn S. Oral appliances for the treatment of snoring and obstructive sleep apnea: a review. Sleep. 1995;18(6):501–510.
35. Hammond RJ, Gotsopoulos H, Shen G, Petocz P, Cistulli PA, Darendeliler MA. A follow-up study of dental and skeletal changes associated with mandibular advancement splint use in obstructive sleep apnea. Am J Orthod Dentofacial Orthop. 2007;132(6):806–814.
36. Almeida FR, Lowe AA, Otsuka R, Fastlicht S, Farbood M, Tsuiki S. Long-term sequellae of oral appliance therapy in obstructive sleep apnea patients: part 2. study-model analysis. Am J Orthod Dentofacial Orthop. 2006;129(2):205–213.
37. Marklund M. Predictors of long-term orthodontic side effects from mandibular advancement devices in patients with snoring and obstructive sleep apnea. Am J Orthod Dentofacial Orthop. 2006;129(2):214–221.
38. Martinez-Gomis J, Willaert E, Nogues L, Pascual M, Somoza M, Monasterio C. Five years of sleep apnea treatment with a mandibular advancement device. Side effects and technical complications. Angle Orthod. 2010;80(1):30–36.
39. Doff MH, Finnema KJ, Hoekema A, Wijkstra PJ, de Bont LG, Stegenga B. Long-term oral appliance therapy in obstructive sleep apnea syndrome: a controlled study on dental side effects. Clin Oral Investig. 2013;17(2):475–482.
40. Robertson C, Herbison P, Harkness M. Dental and occlusal changes during mandibular advancement splint therapy in sleep disordered patients. Eur J Orthod. 2003;25(4):371–376.
41. Pliska BT, Nam H, Chen H, Lowe AA, Almeida FR. Obstructive sleep apnea and mandibular advancement splints: occlusal effects and progression of changes associated with a decade of treatment. J Clin Sleep Med. 2014;10(12):1285–1291.
ACKNOWLEDGMENTS
The authors acknowledge the contributions of Chris Bunney and Dr. Joseph Janjis in the analysis and reporting of the level 2 sleep studies.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication October 11, 2016
Submitted in final revised form February 8, 2017
Accepted for publication March 31, 2017
DISCLOSURE STATEMENT
Financial support for this study was provided by Oventus Medical Pty Ltd. CH is a Director, shareholder and employee of Oventus. SC is a shareholder of Oventus and Director of Mobius Medical. IS is an employee of Oventus. KMC receives consulting fees from Oventus as a member of the Scientific Advisory Committee. Work for this study was performed at Turbot Street Medical Centre, Spring Hill, QLD, Australia. The device used in this study was for investigation purposes only at the time of the study. Approval for use in the treatment of OSA has since been granted.